w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Analysis
of
the
psychometric
properties
of
the
American
Orthopaedic
Foot
and
Ankle
Society
Score
(AOFAS)
in
rheumatoid
arthritis
patients:
application
of
the
Rasch
model
Cristiano
Sena
da
Conceic¸ão
a,b,∗,
Mansueto
Gomes
Neto
a,c,
Anolino
Costa
Neto
a,
Selena
M.D.
Mendes
b,
Abrahão
Fontes
Baptista
d,
Kátia
Nunes
Sá
baBiofunctionDepartment,PhysicalTherapy,UniversidadeFederaldaBahia,Salvador,BA,Brazil
bMedicineandHealthProgram,EscolaBahianadeMedicinaeSaúdePública,Salvador,BA,Brazil
cMedicineandHealthProgram,UniversidadeFederaldaBahia,Salvador,Bahia,Brazil
dBiointeractionDepartment,UniversidadeFederaldaBahia,Salvador,BA,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received26August2014 Accepted1December2014 Availableonline10March2015
Keywords:
Rheumatoidarthritis Disability
Scale Evaluation Raschanalysis
a
b
s
t
r
a
c
t
Objective:TotestedthereliabilityandvalidityofAofasinasampleofrheumatoidarthritis
patients.
Methods:Thescalewasapplicabletorheumatoidarthritispatients,twicebytheinterviewer
1andoncebytheinterviewer2.TheAofaswassubjectedtotest–retestreliability analy-sis(with20Rheumatoidarthritissubjects).Thepsychometricpropertieswereinvestigated usingRaschanalysison33Rheumatoidarthritispatients.
Results:Intra-ClassCorrelationCoefficient(ICC)were(0.90<ICC<0.95;p<0.001)for
intra-observerreliability and (0.75<ICC<0.91; p<0.001) forinter-observerreliability. Subjects separationrateswere1.9and4.75fortheitems,showingthatpatientsfellintothreeability levels,andtheitemsweredividedintosixdifficultieslevels.TheRaschanalysisshowedthat eightitemswassatisfactory.Oneerroneousitemhavebeenidentified,showingpercentages abovethe5%allowedbythestatisticalmodel.FurtherRaschmodelingsuggestedrevising theoriginalitem8.
Conclusions:TheresultssuggestthattheBrazilianversionsofAofasexhibitadequate
reliabil-ity,constructvalidity,responsestability.ThesefindingsindicatethatAofasAnkle-Hindfoot scalepresentsasignificantpotentialforclinicalapplicabilityinindividualswithrheumatoid arthritis.Otherstudiesinpopulationswithothercharacteristicsarenowunderway.
©2015ElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthor.
E-mail:[email protected](C.S.Conceic¸ão). http://dx.doi.org/10.1016/j.rbre.2014.12.003
Análise
das
propriedades
psicométricas
do
American
Orthopaedic
Foot
and
Ankle
Society
Score
(Aofas)
em
pacientes
com
artrite
reumatoide:
aplicac¸ão
do
modelo
Rasch
Palavras-chave:
Artritereumatoide Incapacidade Escala Avaliac¸ão AnáliseRasch
r
e
s
u
m
o
Objetivo:TestaraconfiabilidadeeavalidadedoescoreAofasemumaamostradepacientes
comartritereumatoide.
Métodos: Aescalafoiaplicadaapacientescomartritereumatoide,duasvezespelo
entre-vistador1eumavezpeloentrevistador2.OAofasfoisubmetidoaexamedeconfiabilidade teste-reteste(com20indivíduoscomartritereumatoide).Aspropriedadespsicométricas foraminvestigadaspelaanáliseRaschem33pacientescomartritereumatoide.
Resultados:Ocoeficientedecorrelac¸ãointraclasse(CCI)foide0,90<CCI<0,95(p<0,001)para
aconfiabilidadeintraexaminadore0,75<CCI<0,91(p<0,001)paraaconfiabilidade interex-aminador.Oíndicedeseparac¸ãodosindivíduosfoide1,9e4,75paraositens.Issodemonstra queospacientessedividiamemtrêsníveisdehabilidadeeositensforamdivididosemseis níveisdedificuldades.AanáliseRaschmostrouqueoitoitensforamsatisfatórios.Foi iden-tificadoumitemerrôneo,quemostroupercentuaisacimados5%permitidospelomodelo estatístico.Alémdisso,omodeloRaschsugeriuarevisãodoitem8original.
Conclusões:OsresultadossugeremqueaversãobrasileiradoAofasapresentaconfiabilidade
adequada,validadedeconstructoeestabilidadederesposta.Essesresultadosindicamque aescaladetornozelo-retropéAofasapresentaumpotencialsignificativodeaplicabilidade clínicaemindivíduoscomartritereumatoide.Outrosestudosempopulac¸õescomoutras característicasjáestãoemandamento.
©2015ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
RheumatoidArthritisisachronicdisablingconditionandmay resultinimpairmentsinfunctionsincludingmusculoskeletal pain,jointstiffness,lossofrangeofmotion,muscular weak-ness,andjointdamage.Thedisabilitycauseslimitationsof activitiesandrestrictionsinparticipation.1
Thenumberofclinicalstudiesaddressingfunctioningas astudyendpointinpatientswithRheumatoidArthritishas steadilyincreasedduringthepastdecade.2Itisalso impor-tanttorecognizethatmeasuresinRheumatoidArthritishave beendevelopedtomeasurethediseaseconsequencesbutwith little attentionto functional aspects.3 Most trialsinvolving RheumatoidArthritishaveusedtheHealthAssessment Ques-tionnaire(HAQ). Thisquestionnaire isinfluenced by social factorssuchaseducationlevelandrequiresamajorchange inscoretorepresentasignificantfunctioningchangeinthe patient.4,5 The HAQ has lower consistency compared with other measures suchas C-Reactive Protein (CRP), Erythro-cyteSedimentationRate(ESR),numberoftenderjointsand patient/physicianglobalassessment.6Furthermore,HAQisa toolwithconsiderable“celling-effect”andthusareunableto detectworseningafterreachingamaximumscore.7
Footimpairmentoccursin85–100%ofRheumatoid Arthri-tis patients and erosive synovitis is the primary reason for high levels of pain and/or disability.8,9 Others stan-dardized method more specifically to assess the disability causedbythedysfunctionofthefeet andgait in Rheuma-toid Arthritis patients is necessary for practice clinical. In 1994, the American Orthopaedic Foot and Ankle Soci-ety(AOFAS)developedratingscales fortheankle-hindfoot,
midfoot, hallux metatarsophalangeal–interphalangeal, and lesser metatarsophalangeal–interphalangeal sites allowing them to be applied to different kinds of injuries and treatments.10AOFASclinicaldomainsweredesignedtoassess foot or ankle problems and are very widely used for this purposed despitethe limited evidence,until now, fortheir reliabilityandvalidityinothercircumstances.11
Rehabilitation programspriorities willbebased increas-inglyon evidenceofthe cost-effectivenessofinterventions on functioning.Thereliabilityofsuchevidenceis substan-tiallydependentonthevalidityofthemethodsusedtoassess healthandfunctioningstatus.InstudyofRodriguesetal.,12 theAOFASwastranslatedandculturallyadaptforBrazilian Portugueseanditsreproducibilityandvalidityweretestedfor patientswithclinicaldiagnosticofankleorhindfootinjuries. Uptothisdate,wedonotknowoftheirvalidationforpatients withRheumatoidArthritisinBrazil.Inthecurrentstudy,we havetestedthereliabilityandvalidityofAOFASinasample ofRheumatoidArthritispatients.
Materials
and
methods
Participants
walking with or without assistive devices. Patients were excludedifhadneurologicdysfunction,cognitivedeficitson theMiniMentalStateExamination,14skinlesions,surgeryin thelowerlimb,pregnantsorinrheumatoidarthritisremission stage(≤2.6onDAS-28).15Inabout25%ofcasesRheumatoid Arthritisisintermittentwith periodsofremissionand this stagemaygenerateaconfoundingeffectandoverestimatethe results.
ThestudywasapprovedbytheResearchEthicsCommittee oftheEstacioofBahiaUniversityCenter,n.657.528andthe participantssignedinformedconsentforms.
Proceduresandinstrumentofmeasure
The questionnaireAOFAS is composed ofnine items, dis-tributedover threecategories:pain,functional aspectsand alignment.Patientswere asked toratethe painon ascale of0–40points.Functionwascalculatedasthetotalscoreof activitylimitations(0–10),maximumwalkingdistance(0–5), walkingsurface(0–5),gaitabnormality(0–8),sagittalmotion (0–8),hindfootmotion(0–6),andankle-hindfootstability(0–8). Alignmentwas ratedfrom 0to10points (good,fair, poor), givingatotalscoreof100points.10,12 Sagittaland hindfoot motionwerephysicalexaminationofjointmotionmeasured bytrainedprofessionalwithgoniometer.
In stage one, the AOFAS were submitted to test–retest reliabilityanalysis by two trained professionals to use the instrument.Totesttheirreliability, theAOFASwas applied twicewithathreetofive-daysintervaltothefirst20 individ-ualswithRheumatoidArthritisincludedinthestudy.Instage two,theBrazilianversionofAOFASwasmeasuredusingRasch
analysis.
Statisticalanalysis
Descriptivestatisticswereutilizedtocharacterizethesample. Intra-classcorrelationcoefficients(ICCs)wereusedtoassess theintra-andinter-raterreliabilities.TheICCwaschosenin preferencetothePearsoncorrelationwhichmayoverestimate reliability.16AllanalyseswereperformedwithSPSSfor Win-dows(SPSSInc.,Chicago,IL,USA)andthesignificancelevel weresetat0.05.
Raschtechniqueshavebeenshowntosuccessfullyreduce
thenumberofitemsonquestionnaires,aparticularly impor-tant issue when developing questionnaires for disabled populations.17Raschanalysisisaprobabilisticmodelwidely usedinthefieldofrehabilitationtoevaluatethepsychometric propertiesofscales.18Isbasedonaprobabilisticrelationship betweenitemdifficultyandpersonability,withthedifference knownasthefunctionalreserveorfunctionalability.19
Itemfitstatisticsareemployedintheassessmentof unidi-mensionality,whichdemonstrateswhetherthequestionnaire or subscale is measuringa single concept. Values such as MnSqandt intwoformats:infit andoutfitwasperformed usingsoftwareWinsteps.20 Theinfitstatistic issensitiveto the variation of scores representing the subject’s abilities, andtheoutfitstatisticreflectstheoccurrenceofunexpected responses.Thesevaluesareusedtodeterminewhetherthe itemsfitwiththeunidimensionalityconcept,withvaluesof MnSq=1±0.4associated with t=±2 being acceptable. The
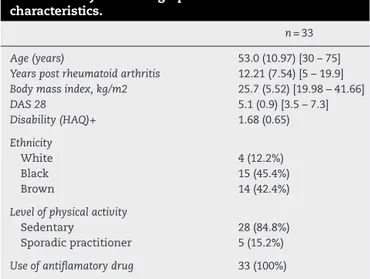
Table1–Subjectsdemographicandclinical characteristics.
n=33
Age(years) 53.0(10.97)[30–75]
Yearspostrheumatoidarthritis 12.21(7.54)[5–19.9]
Bodymassindex,kg/m2 25.7(5.52)[19.98–41.66]
DAS28 5.1(0.9)[3.5–7.3]
Disability(HAQ)+ 1.68(0.65)
Ethnicity
White 4(12.2%)
Black 15(45.4%)
Brown 14(42.4%)
Levelofphysicalactivity
Sedentary 28(84.8%)
Sporadicpractitioner 5(15.2%)
Useofantiflamatorydrug 33(100%)
Values are mean (standard deviation) [range] or frequency (percentage)
conditioninwhichmorethan5%oftheitemsofascaleexhibit erraticscoresindicatethatthecorrespondingcombinationof itemsisnotabletomeasureaunidimensionalconstruct.21,22
TheRaschmodelfurtherincludesthepersonanditem
sep-arationindicesandthesatisfactorytestdividesthesubjects intoatleastthreeabilitylevels:low,medium,andhigh.23The estimatedvaluesofreliabilitytocalibratethemeasuresmust be>0.80.24
Results
Samplecharacterization
Thirty-three femaleswithrheumatoid arthritiswere evalu-atedwithameanageof53±10.9years(rangingfrom30to 75).Demographicandclinicalcharacteristicsofthesubjects arereportedinTable1.
Test–retestreliability
Table 2 gives the ICC values for the intra- and inter-raterreliabilities.Ascanbenoted,significantandadequate values of intra- (0.90<ICC<0.95; p<0.001) and inter-rater (0.77<ICC<0.91;p<0.001)reliabilities wereobtained. Inthe
Table2–Intraclasscoefficients(ICC)Valuesfortheintra andinterraterreliabilityofdomainandtotalscore AOFAS.
AOFAS ICC
Intra Inter
AOFAS–pain 0.90* 0.77*
AOFAS–function 0.92* 0.81*
AOFAS–total 0.95* 0.91*
Table3–CalibrationofAOFASitems.
Calibration Infit Outfit
Item MnSq t MnSq t
9.Alignment 57.11 0.96 0.0 0.61 −0.9
1.Pain** 55.96 0.35 −3.0 0.48 −1.6
4.Walkingsurfaces 54.07 0.79 −0.8 0.94 −0.1
8.Ankle-hindfootstability* 50.05 1.62 2.4 1.49 2.0
3.Maxcontinuouswalkingdistance 48.98 0.61 −2.0 0.64 −1.8
7.Hindfootmotion 48.77 0.92 −0.3 0.91 −0.4
2.Activitylimitations 46.50 1.02 0.2 1.03 0.2
6.Sagittalmotion 46.06 1.30 1.3 1.17 0.7
5.Gaitabnormality 42.48 1.31 1.2 1.34 1.4
∗ Erraticitem:MnSq>1.4andt>2.
∗∗ Predictableitem:MnSq<0.6.
presentstudy,theapplicationoftheAOFASlasted5.5minon average,rangingfrom4to7min.
Raschanalysis
IntheAOFAS,thecalibrationstabilityoftheitemsand individ-ualswas0.96and0.80,respectively.ResultsofRasch’sanalysis arepresentedinTable3,inwhichthevaluesofthecalibration ordifficultyofitems,MnSqandt(infitandoutfit)are individ-uallyreported.Theitemsarecontainedindecreasingorderof difficulty.Item9“Alignment”wasthemostdifficult,anditem 5,“Gaitabnormality”,wastheeasiestone.
Outofthe9itemsofthequestionnaire,1(11.1%)didnot ful-filltheexpectationsofthemodel:numbers8(ankle-hindfoot stability[anteriordrawer,varus-valgusstress])demonstrated MnSq>1.4andt>2.
Theindividualseparationindexwas1.9,whichindicates thattheitemsdistributedthesubjectsamongthreeability lev-els.Theitemseparationindexwas4.75,whichcorrespondsto approximatelysixlevelsofdifficulties.
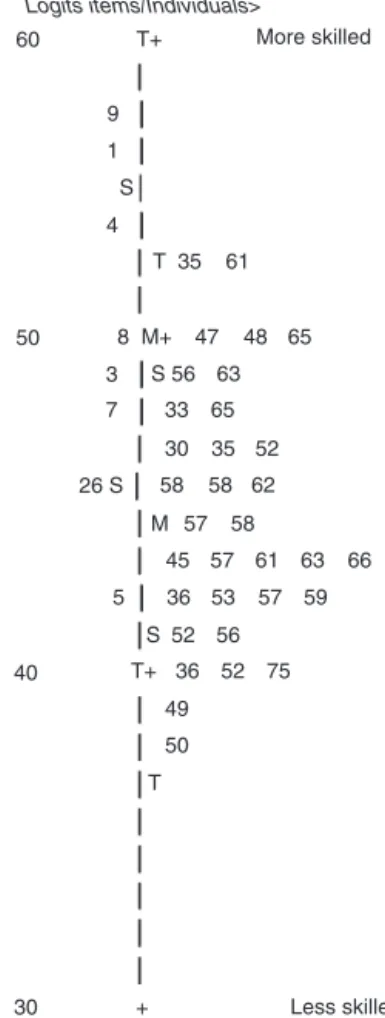
Fig.1displaysamapthatdepictsthecontinuumofthe diffi-cultyoftheitemsontheleftandthesampleabilitycontinuum ontheright.Mostitemshadmediumdifficulty,whereasitems allowingtheassessmentofindividualswithveryhighorvery lowabilitywerelacking.
Discussion
TheAOFASclinicalratingsystemconsistsoffoursite-specific scalesthatenableafocusontargetsitesordiseases.10,12Since theAOFASwasdevelopedinEnglish,itwasnecessarytocarry outatransculturaladaptationofthequestionnaire(i.e.,a lit-eraltranslation isnotenough), aswellas anevaluationof thepsychometricpropertiesofthepopulationwhereitwas supposedtobeused.24
TheRaschanalysisperformedinthepresentstudyshowed
acalibration stability ofthe items and individuals in both investigatedtests,indicatingthatthemeasureswere stable andreproducible.Thevaluefoundfortheindexof separa-tionofthesample’sindividuals(1.9)indicatesthattheywere dividedintothreelevelsofability:low,intermediate,andhigh.
TheRaschanalysisdetectedoneitem(11.1%)witherratic
behaviors (number 8) which was superior to what is
9
1
S
4
50 60
T 35 61
8 M+ 47 48 65
3
7 33
30
26 S 58 58 62
M 57
45 57 61 63 66
5 36 53 57 59
T+ T+
36 52 75
49
50 40
30
T 52 56
58 35 52 65 S 56 63
S Logits items/Individuals>
More skilled
Less skilled +
Fig.1–Maprepresentingthedistributionofsubjectsand itemsfromequilibriummeasuredbytheAOFAS.The numbersontheleftrepresentthetestitems,andthe subjectsareontheright(thenumberidentifiestheage).
Arthritisisadiseasethataffectsthefeetofpatientsin85a 100%ofcases;recurrentsynovitisdamagesthetissuesand thestabilityoftheankle-hindfoot,thatworsenswith advanc-ingdisease.8Thusitprovedpossibletonotethatindividuals withlongerdiseaseclaimedhisankleunstableandthosewith shorterdiseasequalifiedasyouranklesstable.
The results of the present study show that the AOFAS exhibitasatisfactoryabilitytodetectsubtledisabilitydeficits, thus makingthe distinction amongpersonswith Rheuma-toid Arthritis disability. Thepresence of very easy or very difficultitemsconstitutesanadvantagefortheinstrument. Fig.1items/mapshowsthecontinuousofdisabilityby ques-tionnaireitems.Thisisarepresentationofthe relationship betweenexaminedindividualsRheumatoidArthritisseverity withdisabilitylevelsdiscriminatedbyscalesitems.Wecansee someitemsatthetop,withnoalignmenttoanyindividual, whichmeansthattheseitemsmeasureaveryhighdisability degreeandnoindividualsexistedinthissamplewithahigh levelofdisability,the lackofindividuals withhigh levelof disabilitymustbeduetotheestablishedcriterionofpatients walkindependently.
Inthispaper,wehavebeenabletodemonstrategoodand excellentvaluesofinterandintra-raterreliabilitiesand valid-ityoftheAOFAS.Thesefindingsprovidestrongsupportforthe reliabilityandvalidityoftheAOFASmeasures,suggestingthat theyperformwellinpatientsundergoingRheumatoid Arthri-tis.TheICCsareshownasthepreferredandmostadequate indices for reliability analyses ofinterval ratio data, since theyrepresentbothcorrelationsandlevelsofagreement.23,24 AccordingtoPortneyandWatkins,25ICCvaluesof≥0.75are indicativeofacceptablereliabilityandthose below0.75are consideredpoortomoderate.
As found in the present results, for both intra- and inter-raterreliabilities,theICCvalueswereconsideredtobe acceptable. These results are consistent with those of the studybyRodriguesetal.,12whichassessedthevaluesofintra andinter-raterreliabilitiesoftheAOFASinpatientswith clin-icaldiagnosticofankleorhindfootinjuriesandfoundvalues ofICCgreaterthan0.9.
Althoughour sample shows ability to read, since most ofthevolunteershadcompletedhighschooleducation,we believethatbecausethesubjectivecomponentofthe Brazil-ianversionoftheAOFASankle-hindfootscaleisadministered asinterviews,potentialinterpretationerrorsareminimized.26 For further studies, it is important that the AOFAS be appliedwithothersamples,sothatthevalidityofthe instru-ment can be more broadly examined. If in other kinds of samplesfromanumber oferratic itemsabove5%persists, modificationstotheAOFASscaleinitem8arewarranted,for exampleincreasingthenumberofpossibleanswersfollowed bystudiesonthemodifiedversion.
Conclusion
The instrument was shown to be clinically useful for the Rheumatoidarthritissampleassessedinthisstudy.However cautionmustbeexercisedwheninterpretingtheresults,and theanswerspatternmustbeobserved,especiallyforitems8 regardedaserraticitem.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterests.
r
e
f
e
r
e
n
c
e
s
1.StuckiG,CiezaA,GeyhS,BattistellaL,LloydJ,SymmonsD, etal.ICFCoreSetsforrheumatoidarthritis.JRehabilMed. 2004;44Suppl.:87–90.
2.CiezaA,StuckiG.Understandingfunctioning,disability,and healthinrheumatoidarthritis:thebasisforrehabilitation care.CurrOpinRheumatol.2005;17:183–9.
3.StuckiG,EwertT,CiezaA.ValueandapplicationoftheICFin rehabilitationmedicine.DisabilRehabil.2002;24:
932–8.
4.CorbachoMI,DapuetoJJ.Avaliac¸ãodacapacidadefuncionale daqualidadedevidadepacientescomartritereumatoide. RevBrasReumatol.2010;50:31–43.
5.LeebBF,AndelI,LederS,LeebBA,RintelenB.Thepatient’s perspectiveandrheumatoidarthritisdiseaseactivityindexes. Rheumatology.2005;44:360–5.
6.AletahaD,MacholdKP,NellVPK,SmolenJS.Theperception ofrheumatoidarthritiscoresetmeasuresby
rheumatologists.Resultsofasurvey.Rheumatology.2006;45: 1133–9.
7.GreenwoodMC,DoyleDV,EnsorM.DoestheStanfordHealth AssessmentQuestionnaireshavepotentialasamonitoring toolforsubjectswithrheumatoidarthritis?AnnRheumDis. 2001;60:344–8.
8.BalA,AydogE,AydogST,CakciA.Footdeformitiesin rheumatoidarthritisandrelevanceoffootfuncyionindex. ClinRheumatol.2006;25:671–5.
9.NovakP,BurgerH,TomsicM,MarincekC,VidmarG.Influence offootorthosesonplantarpressures,footpainandwalking abilityofrheumatoidarthritispatients:arandomized controlledstudy.DisabilRehabil.2009;31:638–45.
10.KitaokaHB,AlexanderIJ,AdelaarRS,NunleyJA,MyersonMS, SandersM.Clinicalratingsystemsfortheankle-hindfoot, midfoot,hallux,andlessertoes.FootAnkleInt.
1994;15:349–53.
11.ButtonG,PinneyS.Ameta-analysisofoutcomeratingscales infootandanklesurgery:isthereavalid,reliable,and responsivesystem?FootAnkleInt.2004;25:521e5.
12.RodriguesRC,MasieroD,MizusakiJM,ImotoAM,PeccinMS, CohenM,etal.Translation,culturaladaptation,andvalidity oftheAmericanOrthopaedicFootandAnkleSociety(Aofas) Ankle-HindfootScale.ActaOrtopBras[SerialontheInternet]. 2008;16:107–11.
13.ArnettFC,EdworthySM,BlochDA,MCshaneDJ,FriesJF, CooperNS,etal.TheAmericanRheumatismAssociation 1987revisedcriteriaforclassificationorrheumatoidarthritis. ArthritisRheum.1988;31:315–24.
14.BruckiS,NitriniR,CaramelliP,BertolucciPHF,OkamotoIH. SugestõesparaousodoMiniexamedoestadomentalno Brasil.ArqNeuropsiquiatr.2003;61:777–81.
15.ScottDL,HuskissonEC.Thecourseofrheumatoidarthritis. BaillièresClinRheumatol.1992;6:1–21.
16.StreinerDL,NormanGR.Healthmeasurementscales.A practicalguidetotheirdevelopmentanduse.Oxford:Oxford UniversityPress;2008.
17.MitchellJD,O’BrienMR.Qualityoflifeinmotorneurone disease–towardsamorepracticalassessmenttool?JNeurol NeurosurgPsychiatry.2003;74:287–8.
19.AndrichD.Aratingscaleformulationfororderedresponse categories.Psychometrika.1978;43:561–73.
20.LinacreJM.WinstepsRaschMeasurementVersion3.72.3 [Software];2011.Availablefrom:http://www.winsteps.com 21.BondTG,FoxCM.ApplyingtheRaschmodel:fundamental measurementinthehumansciences.Mahwal:Lawrence ErlbaumAssociates;2001.p.288.
22.SilversteinBF,FisherWP,KilgoreKM,HarleyJP,HarveyRF. Applyingpsychometriccriteriatofunctionalassessmentin medicalrehabilitation:definingintervalmeasures.ArchPhys MedRehabil.1992;73:507–18.
23.LexellJE,DownhamDY.Howtoassessthereliabilityof measurementsinrehabilitation.AmJPhysMedRehabil. 2005;84:719–23.
24.BeatonDE,BombardierC,GuilleminF,FerrazMB.Guidelines fortheprocessofcross-culturaladaptationofself-report measures.Spine.2000;25:3186–91.
25.PortneyLG,WatkinsMP.Foundationsofclinicalresearch: applicationstopractice.2nded.NewJersey:Prentice-Hall; 2000.