rev bras ortop.2014;49(1):82–85
w w w . r b o . o r g . b r
Case
Report
Osteoid
osteoma
of
the
acromion
simulating
acromioclavicular
pain
夽
,
夽夽
Alberto
Naoki
Miyazaki
∗,
Marcelo
Fregoneze,
Pedro
Doneux
Santos,
Luciana
Andrade
da
Silva,
Guilherme
do
Val
Sella,
Douglas
Lobato
Lopes
Neto,
Melvis
Muchiuti
Junior,
Sergio
Luiz
Checchia
DepartamentodeOrtopediaeTraumatologia,FaculdadedeCiênciasMédicasdaSantaCasadeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received17March2013 Accepted9April2013
Keywords:
Osteoidosteoma Boneneoplasms Acromion
a
b
s
t
r
a
c
t
Theosteoidosteomaisabenignbonetumourthatusuallypresentswithnocturnalpainin youngadults,relievedbyrestandanti-inflammatories.Itcanaffectanybone;however,their occurrenceisrareintheacromion.Theauthorsdescribeacaseofosteoidosteomalocatedin theacromion,withsymptomsthatsimulatedacromionclaviculararthrosis.Thediagnosis wasmadebyCTscanandtreatmentwasexcisionofthenidusthrougharthroscopy.The diagnosiswasconfirmedbyhistopathology.Intheoutpatientsegment,thepatientremained asymptomatic,withcompleterecoveryoffunctionoftheaffectedlimb.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Osteoma
osteóide
de
acrômio
que
simula
dor
acrômio-clavicular
Palavras-chave:
Osteomaosteóide Neoplasiasósseas Acrômio
r
e
s
u
m
o
Oosteomaosteóideéumtumorósseobenignoqueseapresentageralmenteemadultos jovenscomdornoturna,aliviadaporrepousoeanti-inflamatórios.Podeacometer qual-querosso.Entretanto,suaocorrêncianoacrômioérara.Osautoresdescrevemumcasode osteomaosteóidelocalizadonoacrômio,comsintomasquesimulavamartrose acrômio--clavicular.Odiagnósticofoifeitopormeiodetomografiacomputadorizadaeotratamento propostofoiaexéresedoniduspormeiodeartroscopia.Odiagnósticodefinitivofoi con-firmadoporexamehistopatológico.Nosegmentoambulatorial,a pacientepermaneceu assintomáticaecomrecuperac¸ãocompletadafunc¸ãodomembroacometido.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevierEditora Ltda.Todososdireitosreservados.
夽Pleasecitethisarticleas:MiyazakiAN,FregonezeM,SantosPD,daSilvaLA,doValSellaG,NetoDLL,MuchiutiJuniorM,ChecchiaSL.
Osteomaosteóidedeacrômioquesimuladoracrômio-clavicular.RevBrasOrtop.2014;49:82–85. 夽夽
WorkconductedatShoulderandElbowGroup,DepartmentdeOrthopaedicsandTraumatology,MedicalSciencesSchool,SantaCasa deSãoPaulo,SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](A.N.Miyazaki).
2255-4971/$–seefrontmatter©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
rev bras ortop.2014;49(1):82–85
83
Introduction
Osteoid osteoma is a benign osteoblastic lesion, and con-stitutesapproximately11%ofallbenignbonetumoursthat usuallyoccurinyoungmen.Thisneoplasmisfoundinthe secondorthirddecadeoflife.However,itcanbeseeninother agegroups.1 Anybonecanbeinvolved.However,thereisa predilectionforlower extremities:halfofthecasesinvolve thefemurortibia.2Thescapulaisabonerarelyaffectedand fewcaseshavebeenreportedintheliterature.Mosheiffetal.,3 inareviewoftheliterature,reportedtheinvolvementof12 scapulaein1236casesofosteoidosteoma.
Case
report
Afemalepatient,aged46years,right-handed,complainedof rightshoulderpainforthreemonths,especiallyatnight,with worseningduringphysicalactivities,andimprovedwiththe useofNSAIDs. Shedeniedany historyoftrauma or previ-ousdiseaseinthejoint.Shehasbeendiagnosedpreviously ashavingimpingementsyndromeandtreatedwithtwo sub-acromialcorticosteroidinjectionsandphysicaltherapy,with partialimprovementofsymptoms.
On physical examination, her shoulders had no defor-mities, tumours or skin lesions, and muscle tropism was preserved. The range of active movement of the affected limbwasslightlylimitedbypainandthepassivemovement wasnormal. Provocative manoeuvresfor acromioclavicular joint(O’Brien,forcedadductionandpainonpalpation)were stronglypositiveandtheotherteststoevaluatetherotator cuffandinstabilityoftheshoulderjointresultednegative.
The Zanca view radiographs revealed changes in the acromioclavicularjoint(Fig.1).Amagneticresonance imag-ingstudyshowedanacromioclaviculararthrosiswithintense inflammatory process in the joint region with a cyst on theacromion,initiallyinterpretedasageode.However,our attentionwas drawnbythefact thattherewas anintense inflammatory process around the lesion, which was very regular and larger than usual; in addition, the images
Fig.1–Radiographoftherightshoulder,Zancaview, showingarthrosisofacromioclavicularjoint.
suggestedtheexistenceofsomesolidcontentinsideit(Fig.2A andB).
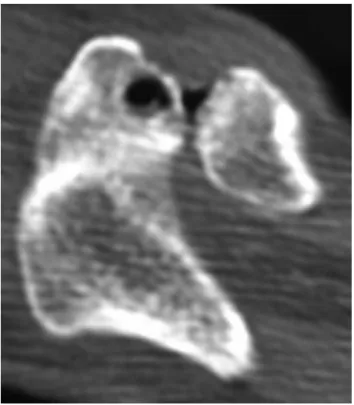
Thediagnosishypothesisofosteoidosteomawasproposed andthenwerequestedaCTscanforconfirmation;thenidus insidethecystcouldbeeasilyevidenced(Fig.3).
Allthecomplementarylaboratorytestswerenormal. Wechosearthroscopicsurgeryandresectionofthenidus (Fig.4),complementedwithabroaderthan usual acromio-plasty,untiltheremovaloftheentiretumour,andresection ofthedistalendoftheclavicle(Mumfordprocedure)wastaken (Fig.5).Thediagnosiswasconfirmedbypathologicalstudy.
Thepatienthadrapidregressionofsymptoms,with com-pleterecoveryofthefunctionalrangeofmotionoftheaffected limb,and remained asymptomatic untilherlast return,by occasionofthepostoperativeexaminationofsevenyears.
Discussion
Thescapulaisarare siteofosteoidosteoma locationand, therefore, is often failed to be included in the differential
84
rev bras ortop.2014;49(1):82–85Fig.3–AxialCTimageoftherightshouldershowing osteoidosteomaintheacromion,nexttothe
acromioclavicularjoint.
Fig.4–Surgicalarthroscopicimage,subacromialview, showingtheresectionofthetumourwithacurette.
diagnosis of chronic shoulder pain.4 The patient with an osteoidosteomaischaracterizedbypainthatoccurs predomi-nantlyatnightandisrelievedbyaspirinoranti-inflammatory drugs.5Oftenthenocturnalpainisattributedtorotatorcuff disease. However, the age range of patients with osteoid osteoma wouldimply inlower probabilityofa rotator cuff disease.
Multipletreatmentoptionsforthistumourareavailable: drugtherapy, percutaneousablationbyradiofrequencyand
Fig.5–Magneticresonanceimaging,rightshoulder, sagittalview,showingcompleteresectionofthelesion (acromioplasty)andresectionofthelateralendofthe clavicle.
surgical procedures involving the complete removalof the nidus, which can be achievedby curettage, en bloc resec-tion and, more recently, by arthroscopic route, with good results.6,7 If the patient’s symptoms are adequately con-trolled,anti-inflammatorymedicationcanbeusedasafinal treatment. Patients treated in this manner usually expe-rience spontaneous healing of the lesion in three to four years.8
Degreefetal.7firstdescribedtheoccurrenceofanosteoid osteomaintheacromioninafemalepatientaged56,whose treatment was open resection of the lesion. Kelly et al.6 described a case of arthroscopic resection of an osteoid osteoma located atthe anterior border ofthe glenoid ofa male patient aged30years,who had undergone two surg-eriesfortreatmentofaSLAPlesion.Theauthorsalsoreported an arthroscopicresection ofan osteoidosteomalocatedat the baseofthe coracoidprocessofamale patientaged12 years.
Ourchoicewasthearthroscopictreatment,asinthecases describedabove,becausethepatient’swasabenignlesionand wehadapossibilitytoresecttheentirelesionwithminimal tissuedamage.Thisoptionprovedtobeeffective,andcanbe appliedinsimilarcases.
Conflicts
of
interest
rev bras ortop.2014;49(1):82–85
85
r
e
f
e
r
e
n
c
e
s
1.LeeBG,ChoNS,RheeYG.Unusualshouldersynovitis secondarytoanosteoidosteomawithoutanidusinthe coracoidprocess:delayedappearanceofanidus.JOrthopSci. 2010;15(6):825–8.
2.MitsuiY,GotohM,YoshidaT,HiraiY,ShinozakiT,NakamaK, etal.Osteoidosteomaoftheproximalhumerus:amisleading case.JShoulderElbowSurg.2008;17(1):e13–5.
3.MosheiffR,LiebergallM,ZivI,AmirG,SegalD.Osteoid osteomaofthescapula.Acasereportandreviewofthe literature.ClinOrthopRelatRes.1991;262:129–31.
4.GlanzmannMC,HinterwimmerS,WoertlerK,ImhoffAB. Osteoidosteomaofthecoracoidmaskedaslocalizedcapsulitis oftheshoulder.JShoulderElbowSurg.2011;20(8):e4–7.
5.GraciaIA,ItarteJI,MajoJB,SaloGB,ProubastaIR.Osteoid osteomaofthecoracoidprocess.JSouthernOrthopAssoc. 2001;10(1):49–52.
6.KellyAM,SelbyRM,LumsdenE,O’BrienSJ,DrakosMC. Arthroscopicremovalofanosteoidosteomaoftheshoulder. Arthroscopy.2002;18(7):801–6.
7.DegreefI,VerduycktJ,DebeerP,DeSmetL.Anunusualcause ofshoulderpain:osteoidosteomaoftheacromion–acase report.JShoulderElbowSurg.2005;14(6):
643–4.
8.HeckJrRK.Bone-formingtumors.In:CanaleT,BeatyJH, editors.Campbell’soperativeorthopaedics.11thed. Philadelphia:SaundersElsevier;2007.p.