w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Inadequate
pain
relief
among
patients
with
primary
knee
osteoarthritis
Pedro
A.
Laires
a,∗,
Jorge
Laíns
b,
Luís
C.
Miranda
c,
Rui
Cernadas
d,e,
Srini
Rajagopalan
f,
Stephanie
D.
Taylor
g,
José
C.
Silva
haMerck,Sharp&Dohme,Oeiras,Portugal
bCentrodeMedicinadeReabilitac¸ãodaRegiãoCentro,Tocha,Portugal
cInstitutoPortuguêsdeReumatologia,Lisbon,Portugal
dAdministrac¸ãodeSaúdedaRegiãoNorte(ARSNorte),Porto,Portugal eCentrodeSaúdedaAguda,Arcozelo,Portugal
fMedDataAnalytics,Inc.,EastBrunswick,UnitedStates gMerck&Co.Inc.,Kenilworth,UnitedStates
hHospitalGarciadeOrta,Almada,Portugal
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received29September2015 Accepted8September2016 Availableonline5December2016
Keywords:
Kneeosteoarthritis Inadequatepainrelief Qualityoflife Disability
Patientreportedoutcomes
a
b
s
t
r
a
c
t
Background:Despitethewidespreadtreatmentsforosteoarthritis(OA),dataontreatment patterns,adequacyofpainrelief,andqualityoflifearelimited.Theprospective multina-tionalSurveyofOsteoarthritisRealWorldTherapies(SORT)wasdesignedtoinvestigate theseaspects.
Objectives: Toanalyze thecharacteristicsandthepatient reportedoutcomesofthe Por-tuguesedatasetofSORTatthestartofobservation.
Methods:Patients ≥50 years with primary kneeOA who werereceiving oral or topical analgesicswereeligible.Patientswereenrolled fromsevenhealthcarecentersin Portu-galbetweenJanuaryandDecember2011.PainandfunctionwereevaluatedusingtheBrief PainInventory(BPI)andWOMAC.Qualityoflifewasassessedusingthe12-ItemShortForm HealthSurvey(SF-12).Inadequatepainrelief(IPR)wasdefinedasascore>4/10onitem5of theBPI.
Results:Overall,197patientswereanalyzed.Themedianagewas67.0yearsand78.2%were female.MeandurationofkneeOAwas6.2years.IPRwasreportedby51.3%ofpatients. Femalegender(adjustedoddsratio–OR2.15[95%CI1.1,4.5]),diabetes(OR3.1[95%CI1.3, 7.7])anddepression(OR2.24[95%CI1.2,4.3])wereassociatedwithhigherriskofIPR.Patients withIPRreportedworstoutcomesinalldimensionsofWOMAC(p<0.001)andinalleight domainsandsummarycomponentsofSF-12(p<0.001).
∗ Correspondingauthor.
E-mail:[email protected](P.A.Laires). http://dx.doi.org/10.1016/j.rbre.2016.11.005
Conclusions: Ourfindingsindicatethatimprovementsareneededinthemanagementof paininkneeOAinordertoachievebetteroutcomesintermsofpainrelief,functionand qualityoflife.
©2016ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Alívio
inadequado
da
dor
em
pacientes
com
osteoartrite
de
joelho
primária
Palavras-chave:
Osteoartritedejoelho Alívioinadequadodador Qualidadedevida Incapacidade
Desfechosrelatadospelo paciente
r
e
s
u
m
o
Antecedentes:Apesardostratamentosmuitodifundidosparaaosteoartrite(OA),dadossobre ospadrõesdetratamento,aadequac¸ãodoalíviodadoreaqualidadedevidasãolimitados. OestudomultinacionalprospectivoSurveyofOsteoarthritisRealWorldTherapies(SORT)foi projetadoparainvestigaressesaspectos.
Objetivos: Analisarascaracterísticaseosdesfechosrelatadospelopacientedoconjuntode dadosportuguêsdoSortnoiníciodaobservac¸ão.
Métodos: Consideraram-seelegíveisospacientescom50anosoumaiscomOAdejoelho primáriaquerecebiamanalgésicosoraisoutópicos.Ospacientesforamrecrutadosdesete centrosdesaúdedePortugalentrejaneiroedezembrode2011.Adoreafunc¸ãoforam avaliadaspeloBriefPainInventory(BPI)epeloWOMAC.Aqualidadedevidafoiavaliadacom o12-itemShortFormHealthSurvey(SF-12).Oalívioinadequadodador(AID)foidefinidocomo umapontuac¸ão>4/10noitem5doBPI.
Resultados: Foramanalisados197pacientes.Aidademédiafoide67anose78,2%eram dosexofeminino.Adurac¸ãomédiadaOAdejoelhofoide6,2anos.OAIDfoirelatadopor 51,3%dospacientes.Osexofeminino(oddsratioajustado-OR2,15[IC95%1,1-4,5]),odiabetes (OR=3,1[IC95%1,3-7,7])eadepressão(OR2,24[IC95%1,2-4,3])estiveramassociadosaum maiorriscodeAID.OspacientescomAIDrelatarampioresdesfechosemtodasasdimensões doWomac(p<0,001)eemtodososoitodomíniosenosdoiscomponentessumáriosdoSF-12 (p<0,001).
Conclusões: Osresultadosdopresenteestudoindicamqueénecessáriomelhoraromanejo dadornaOAdejoelhoafimdealcanc¸armelhoresdesfechosemtermosdealíviodador, func¸ãoequalidadedevida.
©2016ElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCC BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Osteoarthritis(OA)isahighlyprevalentanddebilitating dis-order which seriously limits both health and well-being, particularlyintheelderlypopulation.1,2Theeconomicburden
ofOAonsubjects,theircaregiversandsocietyisconsidered quitehigh.Indevelopedcountriesitmaycostbetween1.0% and2.5%ofgrossdomesticproduct.3
Approximately 13%of womenand 10% ofmenaged60 yearsandolderhavesymptomatickneeOA.Theseproportions arelikelytoincreaseduetotheagingofthepopulationand thegrowingrateofobesityinthegeneralpopulation.4Other
factorsareassociatedwithahigherriskforthedevelopment andprogressionofkneeOAsuchasfemalegender,previous kneetrauma,bonedensity,muscleweakness,joinlaxityand physicallydemandingoccupationsoractivities.2,5
TheEuropeanLeagueAgainstRheumatism(EULAR) recom-mendsthattheclinicaldiagnosisofkneeOAshouldbebased onthree symptoms(persistentknee pain, limitedmorning stiffness and reduced function) and three signs (crepitus, restrictedmovement andboneenlargement).Thepresence
ofallthesesignsandsymptomsincreasestheprobabilityof radiographickneeOAto99%.6
Pain is the most common symptom inknee OA and is the leading cause ofdisability dueto this condition.2 This
symptom has also a diversity of psychological and social implications.
The clinical management of OA aims to relieve pain, maintain or improve joint function and prevent or delay disease progressionand its consequences.7,8 Effective pain
management relies on abroad range combination of non-pharmacologicalandpharmacologicalmodalities.9The
phar-macological approaches and treatment modalities include paracetamol,NSAIDs, opioids,topicalanalgesicsand intra-articularinjectionofcorticosteroid.10,11However,variabilityin
treatmenteffectiveness,aswellastolerability,oftenrequires trialsofdifferenttreatmentmodalitiestoachieve adequate pain control. Treatment should be individualized accord-ing to patient symptoms, preferences,and the therapeutic agent’ssafetyprofile.12Despiteitsseriousconsequences,most
TheStudyofOsteoarthritisRealWorldTherapies(SORT) is a 12-month clinical prospective study conducted in six Europeancountries(UnitedKingdom,France,Germany,Italy, NetherlandsandPortugal)14andisdesignedprimarilyto
eval-uate the impact of inadequate pain relief (IPR) on patient reportedoutcomes(PRO)amongsubjectswithsymptomatic osteoarthritisoftheknee(s)treatedwithoralortopic anal-gesics.
Thepresentworkreportstheclinicalcharacteristics, treat-mentpatternsandPROsofthePortuguesedatasetoftheSORT studyatthestartofobservation.Theadequacyofpainrelief from theuse ofanalgesicsiscomparedwith thesubset of patientswithinadequatepainreliefregardingdemographic andclinicalvariablesofinterest,aswellasseveraldimensions ofotherPROsuchasjointstiffness,generalhealthandquality oflife.
Methods
Participantsandvariablesofinterest
In Portugal, the study was conducted at seven reference healthcare centers, reflecting a wide geographic distribu-tion.Thedatasetincludedmaleorfemalepatientsthatwere enrolledbetweenJanuaryandDecemberof2011.Patientswere eligibleiftheywere50yearsorolderandhadaclinical diag-nosisofprimaryOAoftheknee(s)accordingtothephysician’s clinical judgment. Patients had to beusing oralor topical analgesicsforaperiodnoshorterthantwoweeks.Patients wereexcludediftheyhadother formsofarthritis, subtotal ortotaljointreplacementintheaffectedknee,chronicsevere painduetocausesotherthanarthritisoranyothercondition thatwould require long-term analgesia.Patients were also ineligibleiftheyhadpreviouslyreceiveddisease-modifying antirheumaticdrugsorbiologictherapies,oriftheywere par-ticipatinginaclinicaltrial.Usingthesecriteria,atotalof197 patientswereincludedinthiscross-sectionalanalysis.
Patientswereenrolledinthestudyastheyattendedtheir scheduledconsultation.Duringtheconsultationthe informa-tionwasobtainedfrompatient’sinterview,self-administered questionnairesandthereviewofmedicalcharts.The follow-ingvariableswereconsideredforthisanalysis:gender,age, professionalstatus, self-reportedheightandweight (which allowedthecalculationofbodymassindex–BMI),smoking statusandOAdiagnosis-relatedinformation(duration, num-berofaffectedkneesandotheraffectedjoints).Comorbidities ofinterestincluded:disability(totalorpartial),previouship replacement,gastro-intestinalconditions,diabetes, hyperten-sion, hyperlipidemia, cardiovascular diseases, renal failure anddepression.UseofanalgesicsforkneeOA(byclass)was alsocollected.
Patientreportedoutcomes
ThefollowinginstrumentswereusedtocollectPROs:
• TheBriefPainInventory(BPI)isavalidatedtoolthat meas-urestheintensityofpain(fouritems),scoresrangingfrom 0(nopain)through10(painasbadasyoucanimagine)and
theinterferenceofpainondifferentfacetsofthepatient’s life(sevenitems),rangingfrom0(donotinterfere)and10 (completelyinterferes).15Thisinstrumentalsoqueriesthe
patientabouthowmuchreliefthetreatmentsor medica-tionshaveprovided,thequalityoftheirpainbychoosing wordsamongalistofverbaldescriptorsderivedfromthe
McGillPainQuestionnaire,andthepatient’sperceptionofthe causeofpain.16ApatientwithIPRwasdefinedashavinga
score>4intheitem5ofBPI–“Whatisyourpainon aver-age?”(0=nopainand10=painasbadasyoucanimagine), indicatingmoderatetoseverepain.Therobustnessofthe cut-offof4onBPIwasalreadyexaminedelsewhere.14
• The Western Ontario and McMaster Universities (WOMAC)
OsteoarthritisIndexisaninstrumentthatmeasurespain(5 items),stiffness(2items)andperformanceofdailyactivities (17items)inpatientswithhipand/orkneeosteoarthritis. Theversionusedinthisstudy(WOMAC,VA3.0)consisted of twenty-four 100mm visual analog scales. Responses rangefromnopain/stiffness/difficulty(0)throughextreme pain/stiffness/difficulty(100).16–18
• Thehealthstatusinstrument12-ItemShortFormHealth
Sur-vey (SF-12) (V2.0), measures the quality of liferegarding eighthealthdomainsoffunctionalhealthandwell-being scores aswell as physical(PCS) and mental(MCS) com-ponentsummarymeasures.19Thequestionsreporttothe
previousweekandthescoringrangesfrom0through100. Highervaluesindicatebetterqualityoflife/generalhealth.18
Furthermore,eachpatientratedhis/herlevelof satisfac-tionwiththeprescribedanalgesicstakinginto accounttwo perspectives: (1) relieve of pain and symptoms caused by kneearthritis;(2)side-effects(i.e.stomachupset).Afive-point Likertscalewasusedinbothevaluationswithfivepossible responses:verydissatisfied,dissatisfied,somewhat dissatis-fied,satisfiedandverysatisfied.Eachpatientalsoratedhis/her globalresponsetoanalgesicsusingafive-pointLikertscale(no response,poorresponse,fairresponse,goodresponse, excel-lentresponse).Theseevaluationsreportedtothelastseven days.
Finally, the physician’s impression of patient’s global responsetotheprescribedanalgesicswasassessedusinga five-pointLikertscalewiththesamedescriptorsasthescale administeredtothepatient.
Thestudywasapprovedbyeachsite’sethicscommittee andtheparticipantswereinformedaboutthenatureofthe studybeforesigninganinformedconsent.
Statisticalanalysis
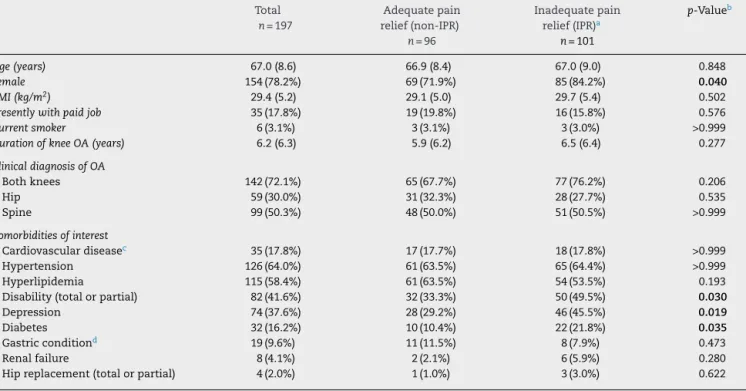
Table1–Socio-demographicandclinicalcharacteristicsofthesample,generalandbrokendownbykneepainrelief status.
Total
n=197
Adequatepain relief(non-IPR)
n=96
Inadequatepain relief(IPR)a
n=101
p-Valueb
Age(years) 67.0(8.6) 66.9(8.4) 67.0(9.0) 0.848
Female 154(78.2%) 69(71.9%) 85(84.2%) 0.040
BMI(kg/m2) 29.4(5.2) 29.1(5.0) 29.7(5.4) 0.502
Presentlywithpaidjob 35(17.8%) 19(19.8%) 16(15.8%) 0.576
Currentsmoker 6(3.1%) 3(3.1%) 3(3.0%) >0.999
DurationofkneeOA(years) 6.2(6.3) 5.9(6.2) 6.5(6.4) 0.277
ClinicaldiagnosisofOA
Bothknees 142(72.1%) 65(67.7%) 77(76.2%) 0.206
Hip 59(30.0%) 31(32.3%) 28(27.7%) 0.535
Spine 99(50.3%) 48(50.0%) 51(50.5%) >0.999
Comorbiditiesofinterest
Cardiovasculardiseasec 35(17.8%) 17(17.7%) 18(17.8%) >0.999
Hypertension 126(64.0%) 61(63.5%) 65(64.4%) >0.999
Hyperlipidemia 115(58.4%) 61(63.5%) 54(53.5%) 0.193
Disability(totalorpartial) 82(41.6%) 32(33.3%) 50(49.5%) 0.030
Depression 74(37.6%) 28(29.2%) 46(45.5%) 0.019
Diabetes 32(16.2%) 10(10.4%) 22(21.8%) 0.035
Gastricconditiond 19(9.6%) 11(11.5%) 8(7.9%) 0.473
Renalfailure 8(4.1%) 2(2.1%) 6(5.9%) 0.280
Hipreplacement(totalorpartial) 4(2.0%) 1(1.0%) 3(3.0%) 0.622
Dataarenumber(%)ormean(standarddeviation). OA,osteoarthritis;BMI,bodymassindex.
a IPRwasdefinedasascore>4(indicatingmoderateorgreaterpain)onthefollowingitemofBriefPainInventory(BPI)scale:“Whatisyour
painonaverage?”(0=nopainand10=painasbadasyoucanimagine).
b Student’sT-testwasusedfornumericalvariablesandChi-squaretestwasusedforcategoricalvariables.Bolddenotesstatisticalsignificance.
c Includedcongestiveheartfailureorestablishedischemicheartdisease,peripheralarterialdiseaseorcerebrovasculardisease.
dIncludedinflammatoryboweldisease,activepepticulcerationorgastrointestinalbleeding,perforationassociatedwithprevioususeof
non-steroidalanti-inflammatorydrugs,recurrentpepticulcerorgastrointestinalhemorrhage.
inthebivariableanalysisandaccordingtoitsinterestforthe research(includingthosetheoreticallyassociatedwithIPR). Thevariables were:age, femalesex, BMI,duration ofknee OA,clinicaldiagnosisofbothknees,co-morbiditiesofinterest (cardiovasculardisease,diabetes,depression,hyperlipidemia, hypertension)andnumberofdifferentclassesofmedication. Statisticaltestswere2-tailedusingasignificancelevelof 5%.AllanalyseswereconductedusingSAS®9.3(SASInstitute, Cary,NC,USA).
Results
Generalcharacteristicsofthesample
Overall,themeanagewas67.0(SD8.6)yearsandmostpatients werefemale(78.2%).Only17.8%ofpatientshadapaidjobat thetimeofassessment–Table1.Theaveragedurationofknee OAwasapproximatelysixyears.Bothkneeswereaffectedin 72.1%ofthepatientsand50.3%alsohadtheirspineaffected. Hypertension (64.0%) and hyperlipidemia (58.4%) were the mostcommoncomorbidities.
Adequacyofpainrelief
Overall,101/197(51.3%[95%CI44.1%,58.4%])ofthepatients reported IPR– Table 1. Womenwere morelikely to report
IPR than non-IPR (p<0.05). Disability, depression and dia-beteswere morefrequentamongpatientswithIPRthanin patients with non-IPR (p<0.05). No statistically significant differences were found between both subgroups regard-ing the mean age (∼67 years), mean duration of knee OA and other socio-demographic and clinical characteris-tics.
Useofanalgesics
Themeannumberofdifferentclassesofmedicationusedby IPRand non-IPRpatients wassimilar(1.76 [SD0.78]versus 1.70[SD0.63];p=0.866).Themostcommonlyusedanalgesics were the non-steroidal anti-inflammatory drugs (NSAIDs) followed by alternative therapies (including glucosamine, chondroitinandhyaluronate)–Fig.1.Therewereno statis-ticallysignificantdifferencesintheuseofthesemedications betweenIPRandnon-IPRgroups.Althoughnon-statistically significant,higherprescriptionofopioid-containing medica-tionswasobservedinpatientswithIPR(18.8%versus10.4%;
p=0.110).
Alternative therapies*
NSAIDs
Meds. containing opioids
Paracetamol
Other
% of patients
Non-IPR (n=96) IPR (n=101) 46.9% 47.5% (P>.999) (P=.494) (p=.110) (p=.874) (P>.999) 80.2% 75.3% 10.4% 18.8% 27.1% 28.7% 5.2% 5.9%
0% 20% 40% 60% 80% 100%
Fig.1–Prescribedanalgesics,brokendownbykneepain reliefstatus.*Alternativetherapiesincludeglucosamine, chondroitinandhyaluronate.NSAIDs,non-steroidal anti-inflammatoryagents;IPR,inadequatepainrelief. Fisherexacttestwasusedforcomparisons.
Otherhealth-relatedoutcomes
Painseverityandinterference(BPI)washigheramongpatients with IPR (p<0.001) – Table 3. Likewise, patients with IPR reportedworstoutcomesinthethreedimensionsofWOMAC (pain, stiffness and physical function) than patients with NON-IPR(p<0.001).
About64%ofpatientswithnon-IPRweresatisfiedorvery satisfiedwiththeeffectsoftheprescribedanalgesicsin reliev-ingthepainandsymptomscausedbykneeOA.Ontheother hand,63.4%ofpatientswithIPRweredissatisfiedorvery dis-satisfiedwiththeeffectsofanalgesics.Ahigherproportionof patientswithIPRreportedafairresponseorworsetothe pre-scribedanalgesicscomparedtopatientswithnon-IPR(79.2% versus55.2%,respectively;p<0.05).Thephysiciansreported patient’sresponsetoanalgesicsasfairorworsein84.2%of patientswithIPRasopposedto55.2%ofthepatientsinthe non-IPRgroup(p<0.05).
A higher proportion of patients in the IPR subgroup reportedfair or poorgeneralhealthin theoverall score of
Table2–Multivariablelogisticregressionanalysis assessingtheadjustedoddsofIPR.
Independentvariables AdjustedOR 95%CI
Age 1.006 0.967 1.047
Female 2.149 1.063 4.480
BMI 1.026 0.965 1.096
DurationofkneeOA(years) 1.007 0.959 1.058 Bothknees 1.342 0.684 2.658
CVD 0.893 0.392 2.022
Diabetes 3.092 1.328 7.655 Depression 2.236 1.194 4.268 Hyperlipidemia 0.457 0.240 0.849 Hypertension 0.924 0.473 1.801 Numberofdifferentclasses
ofmedication
1.081 0.710 1.651
OR,oddsratio;CVD,cardiovasculardisease. Modelp-value(p<0.001).
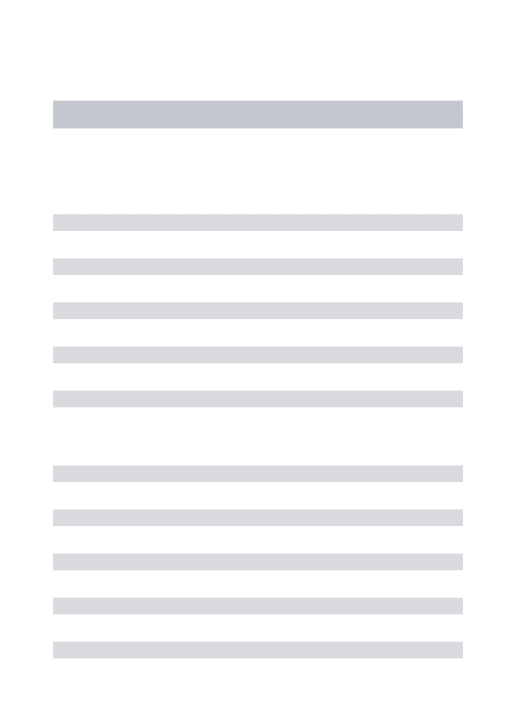
54.2 55.9 32.9 41.0 22.3 19.6 31.6 52.4 43.5 37.3 32.8 65.9 48.9 73.1 80.0 55.5 56.1 36.9 58.6 36.5
Mental component summary Physical component summary Mental health Role emotional Social functioning Vitality Bodily pain Role physical Physical functioning General health perception
90.0 80.0 70.0 60.0 50.0 40.0 30.0 20.0 10.0 0.0 Mean scores SF-12 components Non-IPR IPR
Fig.2–MeanscoreforeachdomainofSF-12,brokendown bykneepainreliefstatus.IPR:inadequatepainrelief. Non-IPR(n=101)andIPR(n=96),unlessotherwise
specified.Thedifferenceswerestatisticallysignificantfor allcomparisons(Mann–Whitney–Wilcoxontest;p<0.001).
SF-12comparedtopatientswithnon-IPR(87.1%versus72.9%, respectively,p<0.001).
ThedistributionsofresponsestoeachoftheSF-12health domainsarepresentedinFig.2.PatientswithIPRhadworst outcomesinalleighthealthdomainsandsummary compo-nentsofSF-12comparedtopatientswithnon-IPR(p<0.001).
Discussion
WefoundthatoverhalfofthePortuguesepatientshad mod-erateor severe pain inspiteofthe use ofanalgesics.This findingsuggestthatthestrategiesadoptedathealthcare cen-tersformanagingpaininkneeOAarebeinginsufficientfor themajorityofpatients.
Currently,theclinicalmanagementofOAissymptomatic and aims to relieve pain and stiffness, and maintain or improve joint function. In addition, the treatment of OA aimstoreducephysicaldisabilityandimprovehealthrelated qualityoflife.9ForpatientswithkneeOA,theimportanceof
pain reliefand functionalimprovementwas evidentinthe resultsofarecentlyreporteddiscretechoiceexperimentthat assessed patient preferences withregard toNSAID-related benefits.20However,thetreatmentofsymptomatickneeOA
posesimportantchallengestothehealthcareprofessionals. In order to be effective the management of OA relies on the appropriate use of a number of non-pharmacological, pharmacologicalandsurgicaltherapies.Despitethefactthat mostcommonlyusedpharmacologicinterventionsforknee OAprovideclinicallysignificantimprovementsinpain,21the
Table3–ScoresofBriefPainInventory,WOMAC,patientandphysicianglobalassessmentofresponsetotherapy,broken downbykneepainreliefstatus.
Adequatepainrelief(non-IPR)
n=96
Inadequatepainrelief(IPR)
n=101
p-Valuea
BPI–painseverity 1.83(1.58) 5.96(1.36) <0.001
BPI–paininterference 2.18(2.35) 5.72(1.98) <0.001
WOMAC–pain 36.31(22.28) 58.03(21.29) <0.001
WOMAC–stiffness 39.35(28.90) 61.34(25.48) <0.001
WOMAC–physicalfunction 40.63(22.15) 61.83(18.44) <0.001
Patientsatisfactionwithprescribedanalgesics
Satisfied/verysatisfied 61(63.5%) 38(37.6%) 0.004
Dissatisfied/verydissatisfied/somewhatsatisfied 35(36.5%) 63(63.4%)
Patientsatisfactionwithtolerabilitytoanalgesics
Satisfied 67(69.8%) 61(60.4%) 0.181
Dissatisfied 29(30.2%) 40(39.6%)
Patientassessmentofresponsetoanalgesics
Excellent/good 43(44.8%) 21(20.8%) 0.004
None/poor/fair 53(55.2%) 80(79.2%)
Physicianassessmentofresponsetoanalgesics
Excellent/good 35(36.5%) 16(15.8%) 0.001
None/poor/fair 61(63.5%) 85(84.2%)
Dataarenumber(%)ormean(standarddeviation).
BPI,BriefPainInventory–higherscoresontheBPIindicateworsepainorgreaterinterferenceofpainwithdailyactivities;WOMAC,Western OntarioMcMasterUniversityOsteoarthritisIndexQuestionnaire–higherscoresontheWOMACindicateworsepain,stiffnessandgreater functionallimitations.
a FisherexacttestwasusedforcategoricalvariablesandMann–Whitney–Wilcoxontestwasusedfornumericalvariables.Allcomparisons
werestatisticallysignificant.
underlyingtheundertreatmentofpainhavebeensuggested. These can include lack of professional medical attention, failuretointroducenon-pharmacologicaltherapiessuchas weight loss and exercise into the management plan, and overrelianceonmonotherapy.25
In our study, the vast majority of patients were using NSAIDs,regardless ofthe reported knee pain relief status. ThisproportionisinlinewiththemultinationalSORTstudy prospectivelongitudinalcohortstudy.14Thisfindingalso
cor-roboratesotherstudieswherehighratesofNSAIDusehave beenreported.Atelephonesurveyof1149patientswithOAin theUKin2003showedthat50%weretakingNSAIDs,while only 15% were taking paracetamol.26 Although the use of
NSAIDwashigheramongpatientswithnon-IPRthanpatients withmoderatetoseverepain,thedifferencesobservedinour studywerenotstatisticallysignificant.
TheAmerican Academyof OrthopedicSurgeons(AAOS) strongly recommends the use of NSAIDs (oral or topic) or TramadolinpatientswithsymptomaticOAoftheknee.The endorsementofNSAIDswasbasedonhighqualityevidence from several studies comparing either the selective, non-selectiveor topicalanalgesicsto placebo.Furthermore,the recommendationon acetaminophenwasdowngradedfrom “moderate”to“inconclusive”,comparingtopreviousguideline publishedbyAAOSin2008.27
Conversely, oral NSAIDs (both non-selective and COX-2 selective)areconditionallyrecommendedbyOARSIguidelines 2013forthemanagementofkneeOA,particularlyin individ-ualswithoutco-morbiditiesorindividualswithmultiple-joint OAwithmoderateco-morbidityrisk.11Regardingtheuseof
acetaminophen,theOARSIguidelinesdifferfromtheAAOS,
butcoincideswiththeACR’s2012guideline,byrecommending itsuseforpatientswithoutrelevantco-morbidities.10,11
A considerable proportion of participants (44%) were using alternative therapies, which included glucosamine, chondroitin andhyaluronate. Theevidenceis controversial regardingthebenefitsofglucosamineandchondrotoininknee andhipOA.Althoughsomestudieshaveshownpositiveeffects oftheseagentsotherstudiesshowednobenefits.9,28TheAAOS
areagainsttheuseofglucosamine,chondroitinandtheACR areagainsttheuseofchondroitinandconditionallyagainst glucosamine.10,27 TheOARSIaremorespecificbyevaluating
thesetreatmentsseparatelyforsymptomaticreliefand dis-easemodification.Recommendationis“uncertain”regarding thesymptomaticefficacyofbothtreatmentsbutconsidered “not appropriate” their use as disease-modifying agents.11
Regardinghyaluronicacid,AAOSrecommendagainstitsuse inkneeOA,citingalackofefficacy,whilstOARSIprovidedan “uncertain”recommendation.11,27
Inourstudy,theuseofopioidswashigheramongpatients whoreportedIPR,althoughthisfindingwasnotstatistically significant.Weakopioidshaveincreasinglybeenusedforthe treatmentofrefractorypaininpatientswithhiporkneeOA. Severalstudieshaveprovidedevidenceregardingthe short-term efficacy and safetyofopioids inchronicpainin OA.9
“uncertain”recommendationfortheuseofopioidsinknee OA.11
Wefoundthattheinadequacyofpainreliefwasmore fre-quentinwomen.Inaddition,theregressionanalysisshowed thatwomenare associatedwithanincreasedriskof expe-riencinginadequatepainreliefwithanalgesics.Womenare moreseverelyaffectedbykneeOA,reportingmorepainand disabilitythan men. Theetiology ofknee OA inwomen is multifactorial and include: anatomic differences compared with men, previous trauma, geneticand hormonal issues. Womenhave increasedincidenceof anterior cruciate liga-mentinjuriesandtheseinjuriesleadtofutureosteoarthritis regardlessof gender. Inaddition, postmenopausalwomen, duetothedecreaseinestrogenhaveanincreasedriskof devel-opingOA.29
The regression analysis also showed that diabetes and depressionwerethecomorbiditiesmostassociatedwithIPR,a findingthatcorroboratestheresultsofthemainSORTstudy.14
Ofnote,hyperlipidemiaisassociatedwithlowerriskofIPR intheregressionmodel,afindingthatisconsistentwiththe resultofthebivariableanalysis.Wefindnoclearexplanation forthisresult,otherthantheexistenceofaconfoundingfactor orduetochance.Still,furtherresearchshouldexaminemore closelythelinksbetweenthesetwovariables.
OuranalysisshowedthatpatientswhoreportedIPRhad moreseverepainandhigherinterferenceofpainwithdaily activities.Moreover,besidespain,thesepatientshadworse outcomesinWOMAC’sdimensionsofstiffnessandphysical functionthanpatientswithnon-IPR.Disabilityisamajor con-sequenceoflowerlimbOA.30Jordanetal.showedthatseverity
ofknee pain correlated with self-reporteddisability inthe community.31Otherauthorsalsoreportedthiscorrelationin
patientsattendingprimarycarewithknee OA32 andinthe
rheumatologysetting.33Itisunclearthemechanismbywhich
paincontributestodisability.Someauthorssuggestthatpain mayleadtoabsenceofphysicalactivity,resultinginacycle ofpain,inactivityandmusclewasting.Psychologicalfactors suchasanxietymayintensifythisnegativecycle.34
Interest-ingly,our resultsshow thatdepression and disabilitywere morefrequentinpatientswithIPR.
TheparticipantswhoreportedIPRhadsignificantlyworse scoresonallphysicalandmentaldomainsofSF-12compared tonon-IPR patients. Quality oflife is a complex construct thatincludesseveral differentdimensionsincluding physi-cal,emotionalandsocialfunctioning.Thebodyofevidence substantiateslower quality of life(QoL) scoresin knee OA patientscomparedtoage-matchednorms.35Desmeulesetal.
observedthat 197participants withknee OA newly sched-uledfor total knee replacement, scored significantly lower inalleightdomainsandonmentalandphysicalcomponent summaryscalesoftheSF-36thanthemean.36Astudywith
Koreaneldersalsoshowedthatkneepainwascorrelatedwith substantialreductioninQoLandphysicalfunction.37Similar
findingswerereportedbyotherauthors.38,39
OurresultssuggestthatpatientswithIPRwere less sat-isfiedwiththeeffectsofprescribedanalgesicsthanpatients withnon-IPR.Thepatientperceivedsatisfactionwith treat-ment is an outcome commonly used to assess treatment success.Thisoutcomecanbeanadequateindicatorofthe qualityofcaregivenondistinctaspectsofthetreatment,such
asitseffectivenessandtolerability.Thisisparticularly impor-tantinpatientswithchronicdiseasessuchasOA,inwhich treatmentsarefrequentlychangedduetolackofeffectiveness oradverseeffects.8
Strengths
and
limitations
Thestrengthsofthisstudyarethatitanalysesreal-worlddata, providingarealisticandvaluable pictureofthePortuguese populationwithkneeOAandtreatmentpatternsunderthe conditionsofnormalclinicalpractice.
Furthermore, we used reliable and validated scales to assesskneeOAsymptoms,particularlypain.TheBPIiswidely usedtomeasurethelevelofpaininseveral chronic condi-tionsandisrecommendedbytheconsensuspanel–Initiative onMethods,Measurement,andPainAssessmentinClinical Trials(IMMPACT).40ThistoolisvalidatedforthePortuguese
populationandrecentstudieshaveshownstrongsupportfor itsreliabilityandvalidity.41,42TheWOMACwasdevelopedto
measuredisabilityinpatientswithlowerlimbOA17andhas
beenextensivelyusedinseveralclinicaltrialsthatassessed paininkneeOA.
Ourstudyhasanumberoflimitations.Weusedarelatively smallsampleandnoprobabilitysamplingmethodswereused. Moreover,wedidnotuseanygeographicstratificationof sam-ple.Therefore,oneshouldbecautiouswhengeneralizingthe findingstothegeneralpopulationwithkneeOA.Nonetheless, whencontrastingthecharacteristicsoftheparticipantsinour studywithpublishedliteratureweobservedsomeoverlapping inthedistributionofgender,ageandcomorbidconditions.
Conclusions
Thepresentworkconstitutesapreliminaryanalysisofthe Por-tuguesesampleincludedinprospectivemultinationalSORT study. Despite the use of analgesics, over half of patients reportedmoderatetoseverekneepain.Thesepatientsalso reportedworseoutcomesregardingothersymptomsofknee OA,generalhealthandqualityoflifethanpatientswithno or mild knee pain. Our findings suggest there isroom for improvement inthe management ofknee pain due to OA inPortugal.FurtherinvestigationontheSORTstudy involv-ing alongitudinalassessmentofthe samplewillprovidea clearerpictureofthecourseofclinicalcareandoutcomesin kneeOA.
Funding
SORTstudywasfundedbyMerckSharp&Dome.
Conflict
of
interest
Acknowledgments
TheauthorswouldliketothankallSORTinvestigators.The authorswould alsoliketoacknowledgeLuísVeloso forhis criticalcontributiontothismanuscript.
r
e
f
e
r
e
n
c
e
s
1. BerenbaumF.Newhorizonsandperspectivesinthe
treatmentofosteoarthritis.ArthritisResTher.2008;10Suppl. 2:S1.
2. HeidariB.Kneeosteoarthritisprevalence,riskfactors, pathogenesisandfeatures:partI.CaspianJInternMed. 2011;2:205–12.
3. Glyn-JonesS,PalmerAJ,AgricolaR,PriceAJ,VincentTL, WeinansH,etal.Osteoarthritis.Lancet.2015;386:376–87. 4. ZhangY,JordanJM.Epidemiologyofosteoarthritis.Clin
GeriatrMed.2010;26:355–69.
5. KlussmannA,GebhardtH,LiebersF,vonEngelhardtLV,Dávid A,BouillonB,etal.Individualandoccupationalriskfactors forkneeosteoarthritis–studyprotocolofacasecontrol study.BMCMusculoskeletDisord.2008;9:26.
6. ZhangW,DohertyM,PeatG,Bierma-ZeinstraMA,ArdenNK,
BresnihanB,etal.EULARevidence-basedrecommendations
forthediagnosisofkneeosteoarthritis.AnnRheumDis. 2010;69:483–9.
7. JordanKM,ArdenNK,DohertyM,BannwarthB,BijlsmaJW, DieppeP,etal.EULARRecommendations2003:anevidence basedapproachtothemanagementofkneeosteoarthritis: ReportofaTaskForceoftheStandingCommitteefor InternationalClinicalStudiesIncludingTherapeuticTrials (ESCISIT).AnnRheumDis.2003;62:1145–55.
8. Oteo-ÁlvaroA,MarínM,Ruiz-IbánM,ArmadaB,RejasJ. Treatmentsatisfactionafterswitchingtoanothertherapyin Spanishorthopaedicclinicoutpatientswithkneeorhip osteoarthritispreviouslyrefractorytoparacetamol.ClinDrug Investig.2012;32:685–95.
9. ZhangW,MoskowitzRW,NukiG,AbramsonS,AltmanRD,
ArdenN,etal.OARSIrecommendationsforthemanagement
ofhipandkneeosteoarthritis,partII:OARSIevidence-based, expertconsensusguidelines.OsteoarthrCartil.
2008;16:137–62.
10.HochbergMC,AltmanRD,AprilKT,BenkhaltiM,GuyattG, McGowanJ,etal.AmericanCollegeofRheumatology2012
recommendationsfortheuseofnonpharmacologicand
pharmacologictherapiesinosteoarthritisofthehand:hip, andknee.ArthritisCareRes(Hoboken).2012;64:465–74.
11.McAlindonTE,BannuruRR,SullivanMC,ArdenNK,
BerenbaumF,Bierma-ZeinstraSM,etal.OARSIguidelinesfor thenon-surgicalmanagementofkneeosteoarthritis. OsteoarthrCartil.2014;22:363–88.
12.KennedyS,MichaelM.Pharmacologicaltreatmentof osteoarthritisofthehipandknee.BCMJ.2010;52:404–9. 13.PeatG,McCarneyR,CroftP.Kneepainandosteoarthritisin
olderadults:areviewofcommunityburdenandcurrentuse ofprimaryhealthcare.AnnRheumDis.2001;60:91–7. 14.ConaghanPG,PelosoPM,EverettSV,RajagopalanS,BlackCM,
MavrosP,etal.Inadequatepainreliefandlargefunctional lossamongpatientswithkneeosteoarthritis:evidencefroma prospectivemultinationallongitudinalstudyofosteoarthritis real-worldtherapies.Rheumatology(Oxford).2015;54:270–7. 15.CaraceniA,ChernyN,FainsingerR,KaasaS,PoulainP,
RadbruchL,etal.Painmeasurementtoolsandmethodsin clinicalresearchinpalliativecare:recommendationsofan ExpertWorkingGroupoftheEuropeanAssociationof PalliativeCare.JPainSymptomManage.2002;23:239–55.
16.CleelandCS,RyanKM.Painassessment:globaluseofthe BriefPainInventory.AnnAcadMedSingap.1994;23:129–38. 17.BellamyN,BuchananWW,GoldsmithCH,CampbellJ,Stitt
LW.ValidationstudyofWOMAC:ahealthstatusinstrument formeasuringclinicallyimportantpatientrelevantoutcomes toantirheumaticdrugtherapyinpatientswithosteoarthritis ofthehiporknee.JRheumatol.1988;15:1833–40.
18.BellamyN.WOMACosteoarthritisindex.Auser’sguide. London,Ontario:VictoriaHospital;1995.
19.WareJJ,KosinskiM,KellerSD.A12-ItemShort-FormHealth Survey:constructionofscalesandpreliminarytestsof reliabilityandvalidity.MedCare.1996;34:220–33.
20.HauberAB,ArdenNK,MohamedAF,JohnsonFR,PelosoPM,
WatsonDJ,etal.Adiscrete-choiceexperimentofUnited Kingdompatients’willingnesstoriskadverseeventsfor improvedfunctionandpaincontrolinosteoarthritis. OsteoarthrCartil.2013;21:289–97.
21.BannuruRR,SchmidCH,KentDM,VaysbrotEE,WongJB,
McAlindonTE.Comparativeeffectivenessofpharmacologic
interventionsforkneeosteoarthritis:asystematicreviewand networkmeta-analysis.AnnInternMed.2015;162:46–54. 22.GebaGP,WeaverAL,PolisAB,DixonME,SchnitzerTJ,VioxxA,
CelecoxibTrial(VACT)Group.Efficacyofrofecoxib,celecoxib, andacetaminopheninosteoarthritisoftheknee:a
randomizedtrial.JAMA.2002;287:64–71.
23.PincusT,SwearingenC,CumminsP,CallahanLF.Preference fornonsteroidalantiinflammatorydrugsversus
acetaminophenandconcomitantuseofbothtypesofdrugs
inpatientswithosteoarthritis.JRheumatol.2000;27:1020–7. 24.SilversteinFE,FaichG,GoldsteinJL,SimonLS,PincusT,
WheltonA,etal.Gastrointestinaltoxicitywithcelecoxibvs nonsteroidalanti-inflammatorydrugsforosteoarthritisand rheumatoidarthritis:theCLASSstudy:Arandomized controlledtrial.CelecoxibLong-termArthritisSafetyStudy. JAMA.2000;284:1247–55.
25.AltmanR.Painreliefinosteoarthritis:therationalefor combinationtherapy.JRheumatol.2004;31:5–7. 26.TNS/arthritiscaresurvey.Availablefrom:
www.arthritiscare.org.uk/OANation.
27.JevsevarDS,BrownGA,JonesDL,MatzkinEG,MannerPA,
MooarP,etal.TheAmericanAcademyofOrthopaedic
Surgeonsevidence-basedguidelineontreatmentof osteoarthritisoftheknee,2ndedition.JBoneJointSurgAm. 2013;95:1885–6.
28.BlockJA,OegemaTR,SandyJD,PlaasA.Theeffectsoforal glucosamineonjointhealth:isachangeinresearchapproach needed?OsteoarthrCartil.2010;18:5–11.
29.SharonL.Kneeosteoarthritisinwomen.CurrRev MusculoskeletMed.2013;6:182–7.
30.YelinE,LubeckD,HolmanH,EpsteinW.Theimpactof rheumatoidarthritisandosteoarthritis:theactivitiesof patientswithrheumatoidarthritisandosteoarthritis comparedtocontrols.JRheumatol.1987;14:710–7. 31.JordanJ,LutaG,RennerJ,DragomirA,HochbergM,FryerJ.
Kneepainandkneeosteoarthritisseverityinself-reported taskspecificdisability:theJohnstonCountyOsteoarthritis Project.JRheumatol.1997;24:1344–9.
32.vanBaarME,DekkerJ,LemmensJA,OostendorpRA,Bijlsma JW.Painanddisabilityinpatientswithosteoarthritisofhipor knee:therelationshipwitharticular,kinesiological,and psychologicalcharacteristics.JRheumatol.1998;25:125–33. 33.CreamerP,Lethbridge-CejkuM,HochbergMC.Factors
associatedwithfunctionalimpairmentinsymptomaticknee
osteoarthritis.Rheumatology.2000;39:490–6.
35.FarrIJ,MillerLE,BlockJE.Qualityoflifeinpatientswithknee osteoarthritis:acommentaryonnonsurgicalandsurgical treatments.OpenOrthopJ.2013;13:619–23.
36.DesmeulesF,DionneCE,BelzileE,BourbonnaisR,FrémontP. Waitingfortotalkneereplacementsurgery:factors
associatedwithpain,stiffness,functionandqualityoflife. BMCMusculoskeletDisord.2009;10:52.
37.KimIJ,KimHA,SeoYI,JungYO,SongYW,JeongJY,etal. PrevalenceofKneePainandItsInfluenceonQualityofLife andPhysicalFunctionintheKoreanElderlyPopulation:A CommunityBasedCross-SectionalStudy.JKoreanMedSci. 2011;26:1140–6.
38.AlkanBM,FidanF,TosunA,Ardıc¸o ˘gluO.Qualityoflifeand self-reporteddisabilityinpatientswithkneeosteoarthritis. ModRheumatol.2014;24:166–71.
39.SalaffiF,CarottiM,StancatiA,GrassiW.Health-related qualityoflifeinolderadultswithsymptomatichipandknee osteoarthritis:acomparisonwithmatchedhealthycontrols. AgingClinExpRes.2005;17:255–63.
40.TurkDC,DworkinRH,AllenRR,BellamyN,BrandenburgN, CarrDB,etal.Coreoutcomedomainsforchronicpainclinical trials:IMMPACTrecommendations.Pain.2003;106:337–45. 41.AzevedoLF,PereiraAC,DiasC,AgualusaL,LemosL,RomãoJ,
etal.Traduc¸ão,adaptac¸ãoculturaleestudomulticêntricode validac¸ãodeinstrumentospararastreioeavaliac¸ãodo impactodadorcrónica.Dor.2007;16:6–37.