w w w . r b o . o r g . b r
Original
article
Trochlear
dysplasia
and
patellar
instability
in
patients
with
Down
syndrome
夽
Tiago
Amaral
Rebouc¸as
Moreira,
Marco
Kawamura
Demange
∗,
Riccardo
Gomes
Gobbi,
Zan
Mustacchi,
José
Ricardo
Pécora,
Luis
Eduardo
Passarelli
Tírico,
Gilberto
Luis
Camanho
InstituteofOrthopedicsandTraumatology,HospitaldasClínicas,SchoolofMedicine,UniversidadedeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received23August2013 Accepted7March2014 Availableonline30March2015
Keywords:
Patellardislocation Downsyndrome Knee
a
b
s
t
r
a
c
t
Objective:ToanalyzeoccurrencesoftrochleardysplasiainpatientswithDownsyndromein thepresenceandabsenceoffemoropatellarinstability.
Methods:Elevenkneeswithstablepatellaeandthirteenwithunstablepatellaeinpatients with Downsyndrome werecompared. Radiographswereproducedto evaluate patellar height,trochlearangleandfemoropatellarcongruenceangle.
Results:Theprevalenceratioforahighpatellabetweentheunstableandthestablepatients was1.01usingtheInsall–Salvatiindexand0.68usingtheCaton–Deschampsindex.Foran abnormalcongruenceangle,theprevalenceratiowas2.04.Anincreasedcongruenceangle wasonlyfoundinfourcases,allpresentinginstability.
Conclusions: Trochleardysplasiawasonlyfoundincasesofinstability.Thetrochleargroove angleandthefemoropatellarcongruenceanglecorrelatedwiththepresenceofpatellar instability.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Displasia
da
tróclea
e
instabilidade
patelar
em
pacientes
com
síndrome
de
Down
Palavras-chave:
Luxac¸ãopatelar SíndromedeDown Joelho
r
e
s
u
m
o
Objetivo:Analisar displasiatroclear em pacientesportadores desíndrome de Down na presenc¸aenaausênciadainstabilidadefemoropatelar.
Métodos:Comparac¸ãode11joelhoscompatelasestáveise13joelhoscompatelasinstáveis emportadoresdesíndromedeDown.Foramfeitasradiografiasemqueforamavaliados alturapatelar,ângulodatrócleaeângulodecongruênciafemoropatelar.
夽
WorkdevelopedintheKneeGroup,InstituteofOrthopedicsandTraumatology,HospitaldasClínicas,SchoolofMedicine,Universidade deSãoPaulo(HC/FMUSP),SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](M.K.Demange). http://dx.doi.org/10.1016/j.rboe.2015.03.005
Resultados: Arazãodeprevalênciadepatelaaltaentreospacientesinstáveiseospacientes estáveis foi de 1,01 para oíndice de Insall-Salvati e de 0,68 parao índice de Caton-Deschamps.Paraoângulodecongruênciaalterado,a razãode prevalênciafoi de2,04. Oângulodecongruênciaaumentadofoiencontradoapenasemquatrocasos,todoscom instabilidade.
Conclusões:Adisplasiadatrócleafoiencontradaapenasemcasosdeinstabilidade,oângulo dosulcodatrócleaeoângulodecongruênciafemoropatelarsecorrelacionaramcoma presenc¸adeinstabilidadepatelar.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Femoropatellarinstabilityisafrequentlyoccurring pathologi-calconditionandislinkedwithpredisposingfactorsinmostof thepatients.Amongthese,dysplasiaofthefemoraltrochlea andtheheightofthepatellaareconsideredtobethemost importantpredisposingfactors.1
Uncertainties remain with regard to understanding the etiopathogenesisofthesefactors,especiallydysplasiaofthe trochlea. There isdoubt concerningwhether the dysplasia isthecauseor theconsequence.Thus,itisaskedwhether a congenital abnormality would lead to femoral dysplasia characterized by a less deep trochlea, which would favor instability,orwhethermuscleabnormalitieswouldcausethe patella to have an abnormalcourse, thereby reducing the femoropatellar pressure andgivingrise to incorrect stimu-lusduringtheanatomicaldevelopmentofthetrochlea,such thatitwouldbecomeflatter,withconsequentprogressionto instability.
Tounderstandthesefactorsbetter,theyneedtobestudied andanalyzedinpatientswithearlyfemoropatellarinstability, i.e.inchildrenwhiletheyaregrowing,whichmakesitpossible toobservethedevelopmentofthefemoraltrochlea.
Among individuals with Down syndrome, there are patientswithseverefemoropatellarinstabilitytogetherwith earlydislocationofthepatella.2Thispeculiarityofthisgroup of patients makes it possible to analyze the development of the femoral trochlea concomitantly with the reduction instimulationresultingfrom thepresenceofthepatellain thefemoropatellarjoint,insituationsofearlydislocationof thepatella.Thismakesitpossibletocomparethis develop-mentwiththat ofpatientswithDown syndromeinwhom femoropatellar instabilityisnotpresent.In additiontothe developmentofthe trochlea, the height ofthe patellacan be studied. This factor relates to the quadriceps muscle, sinceit affects the degree offlexion of the knee towhich thepatellaisjointedwiththetrochlea,andalsoinfluences thestimulationofdevelopmentofgreaterorlessertrochlear depth.
Theaim ofthis study was toanalyze the depth ofthe trochleaand height ofthe patella(predisposing factors) in patientswithDownsyndromewithfemoropatellar instabil-ityandcomparethesewiththeoccurrenceofthesefactorsin patientswithDownsyndromewithoutfemoropatellar insta-bility.
Materials
and
methods
This study was approved by the Research Ethics Commit-teeunderno.175/2010.Allthe patientsreceivedafreeand informedconsentstatement.
Westudied 12 patientswithDown syndrome agedover 12yearswhohadneverundergoneanyinterventionsinthe knees.
Wehadsixmaleandsixfemalepatients.Theirmeanage was16.4years,witharangefromsixto36years(Table1).
Weevaluatedfemoropatellarinstabilityaccordingto clini-calandradiographiccriteria.Theradiographicmeasurements weremadetwice,withaone-weekintervalbetweenthem,by thesameevaluator.
Clinically,weusedtheDugdaleandRenshawclassification systemtodeterminewhether instabilitywaspresent.2This dividesfemoropatellarinstabilityinpatientswithDown syn-dromeintofivegrades,suchthatgradeIisstableandgrades IIandonwardsareunstable,andthehigherthegradeis,the greatertheseverityoftheinstabilityis.
Fromthissample,weobtained11kneeswithstable patel-laeand13withunstablepatellae.
We radiographically studied the knees individually in accordancewiththeradiologicalinstabilitycriteria.Forall24 knees,weusedthefrontalradiographicviewandthe abso-luteandaxiallateralviewsintheMerchantposition,flexedat 45◦.1,3,4
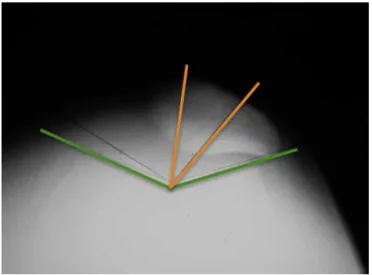
Thefollowingwere measured onall the radiographson thesepatients:theheightofthepatella,inaccordancewith themethodofCatonandDeschamps,5,6thetrochleargroove angle,inaccordancewiththemethoddescribedbyMerchant; andthepatellarcongruenceangle.Thislastmeasurementwas madebetweenthelinebisectingthe trochleargrooveangle andthelinegoingfromthevertexofthetrochlearangleto theeminenceorcrestbetweenthepatellarfacets(Fig.1).
Inevaluatingtheheightofthepatellaonthelateral radio-graphoftheknee,weconsideredthepatellatobehighwhen theratiobetweenthedistancefromtheanteriorborderofthe tibiatothelowercenterofthejointfaceofthepatellaandthe measurementofthejointsurfacewasgreaterthan1.2(Fig.2). Inevaluatingthetrochleargrooveangle,weconsideredthe trochleatobeflatwhentheanglewasgreaterthan150◦.
Inevaluatingthepatellarcongruenceangle,weconsidered thatlateralsubluxationgreaterthan11◦orcomplete
Table1–Anthropometricdescriptionofthesample,includingmeansandstandarddeviations.
Number Sex Dateofbirth Age(a) Weight(kg) Height(m) BMI
1 M 01/10/95 14 52 1.54 21.9
2 F 7/25/00 9 26 1.26 16.4
3 M 5/25/99 10 31 1.4 15.8
4 M 5/9/00 9 44 1.32 25.2
5 M 7/10/92 17 90 1.6 35.2
6 F 4/11/89 21 52 1.52 22.5
7 F 4/8/99 11 45 1.48 20.6
8 M 7/7/87 22 59 1.53 25.2
9 F 9/19/87 22 65 1.4 33.2
10 M 4/29/74 36 74 1.73 24.7
11 F 11/3/03 6 23 1.12 18.3
12 F 5/5/90 20 68 1.4 34.7
Mean 16.4 52.4 1.44 24.5
Standarddeviation 8.4 20.2 0.16 6.75
Minimum 6 23 1.12 15.8
Maximum 36 90 1.73 35.2
Results
FromtheclinicalcriteriaaccordingtotheDugdale classifica-tion,11kneeswerestableand13wereunstable(gradeIIor higher).
Amongthe unstable knees, eight presentedsubluxated patellae,threepresentedreducibledislocatedpatellaeandtwo hadirreduciblepatellae.
Fromtheradiographicevaluation,ahighpatellawas iden-tifiedinthreeknees.Thetrochleargroovewasalteredinfour kneesand the patellarcongruence anglewas alteredin13 knees(Fig.3).
Table2presentstheresultsandcorrelatestheinstability accordingtoclinicalandradiographiccriteria.
Theprevalenceratioisameasurementthatmakesit pos-sible to estimate the strength of association between the exposure(in this case, thepresence ofinstability)and the diseaseorabnormalitystudied(inthiscase,theradiographic alterations).
Theprevalenceratioofhighpatellaebetweenthe unsta-bleandstablepatientswas0.68,usingtheCaton–Deschamps index.Noprevalenceratiocouldbecalculatedforincreased
L
S M
A
O +
–
Fig.1–Diagramshowingaxialincidenceontheknee,with measurementofthepatellarcongruenceangle.
trochlear groove angle, because this only occurred in the unstable patients. The prevalenceratio forthe congruence anglewas2.04.
Trochleardysplasiawasonlyfoundinpatientspresenting instability(fourknees).
Discussion
Downsyndromeisoneofthecommonestdisordersofgenetic origin inhumans. It affects between 1:1000and 1:700 live births.Itconsistsoftrisomyofchromosome21andcanalso occurduetoRobertsoniantranslocation.7
Orthopedicdisordersarefrequentlyobservedinthespine (atlantoaxial instabilityand scoliosis),feet,hips (instability
Table2–Correlationbetweeninstabilityaccordingto clinicalcriteriaandfactorspredisposingtoward instabilityaccordingtoradiographiccriteria.
Radiographiccriterion Clinicalcriterion
Stable Unstable
Highpatella(Caton–Deschamps) 5 4
Trochleargroove>150◦ 0 4
Patellarcongruence>11◦ 4 9
andslidingoftheproximalfemoralepiphysis)andknees (val-gus knee and femoropatellar instability). These alterations areduetomuscledisorders(hypotonia)andligamentlaxity, whicharecommoninthissyndrome.Kneeproblemsareseen in30%to40%ofthesepatients.7
Weconsiderthattheagerangeofourpatientswasa lim-itationofourstudy,inwhichthemeanwas16.4yearsand the range was from six to 36 years.Studying the patients withDownsyndromeisalwaysdifficult,especiallywhenthe individualisasymptomaticorhasfewsymptomsofthe patho-logicalconditioninquestion,giventhatthepatientsandtheir familiesareresistanttoexcessivemedicalattention.We stud-ied12patientswhohadneverhadanymedicalattentionfor theirorthopedicproblems.Initially,welimitedourinclusion criteriontopatientsagedunder14years,butthiswasseento beinsufficientforobtaininganadequatesample.Therefore, wedecidedtoalsoincludepatientsovertheageof14years.
Furthermore, we only used simple radiographs in our evaluation,becausethepatientshadneverundergone tomog-raphy, although the latter is considered to be the best examinationforestimatingtheQangle(bymeansofTA-GT) androtationaldisplacementofthelimb.Sincemanypatients presentedhighfatdistributiontothethighs,wechosenotto includeaclinicalmeasurementoftheQanglebecauseofthe lowreliabilityofthisanalysis.
Inordertodefinethepresenceofinstability,weusedthe DugdaleandRenshawclassification,2becausethisisclassical forpatients with Down syndromepresenting femoropatel-lar instability. In this manner, we selected 13 knees with femoropatellarinstabilitythathadbeendiagnosedclinically
Fig.3–Radiographofthekneeinaxialview.Notethe trochleardysplasiaandlateralizationofthepatella.
in accordance with the Dugdale criteriaand wecompared thesewith11kneesthataccordingtothesamemethodology didnotpresent anyfemoropatellar instability,eventhough they were theknees ofpatients withDown syndrome.We chose to categorize our data analysis between knees with and without instability, sincethis analysisis morereliable thanaclassificationofinstabilityintoseveralgradesandalso strengthensthedataanalysisinasampleofmorerestricted size. The radiographic criteria were chosen and limited to threepositions.Thethreeindicesevaluatedwerebasedonthe studybyDejouretal.,1withtheaimofestablishingthe pres-ence ofobjectivesigns offemoropatellarinstability. During thestudy,weattemptedtoevaluatethedepthofthetrochlea onradiographsinabsolutelateralview,butweonly consid-eredthesemeasurementstobeadequateinthreepatientsand preferredtodisregardthismeasurementofinstabilityinthe presentstudy.IndividualswithDownsyndromeoftendonot cooperateduringexaminationsandseveralradiographsmay needtobeproducedinordertoobtainonethatisgoodenough foranalysis.Increasingthenumberofradiographicviews sig-nificantlycomplicatesthestudyandexposesthepatientsto additionalradiation.Withregardtocomplementary examina-tions,wechosenottoperformcomputedtomographybecause oftheradiationexposure,giventhatthesepatientsare fre-quentlyexposedtomultipleexaminationsovertheirlifetimes. Wechosenottoperformmagneticresonanceexaminations becausealargeproportionofthepatientswouldneedtobe sedated.
In our results, we observed that the patellar height (a femoropatellarinstabilityindexthatisconsideredtobevery importantamongpatientswithoutDownsyndrome)wasnot usefulasacriterionforinstabilityhere,giventhatamongthe nine kneeswithabnormalpatellarheight, fivewerestable. Thepatellarheightevaluationmethodusingthejointsurface (Caton–Deschamps)waschosenbecausethispresentsresults thataremorereliableandhavebettercorrelationbetweenthe evaluators.8Initially,weimaginedthatthismighthavebeen aproblemconsequenttothemeasurementmethodchosen (Caton–Deschamps) and therefore werepeated the patellar heightmeasurementsusingtheInsall-Salvatimethod.9Inthis second measurement, wefoundthat 22knees presenteda patellathatwasconsideredhigh,andtenwereinpatientsin thegroupthatwasconsideredtobestable.Thiscorroborated thefindingthatthepatellarheightisnotanappropriate mea-surementforindicatingfemoropatellarinstabilityinpatients withDownsyndrome.Theprevalenceratioforhighpatella betweentheunstableandstablepatientswasonly1.01 accord-ingtotheInsall–Salvatiindex.
Barnettetal.10analyzedpatellarheightinmagnetic reso-nanceimagingexaminationsoncompletelyextendedknees, among29patientswithtrochleardysplasiainassociationwith patellarinstability.Theyobservedthattherewasno relation-ship between high patella and instability. We believe that musclealterationsrelatingtoDownsyndromemaybe respon-sible forretractionofthequadriceps,whichwould causea highpatellainmostpatients,eveninindividualswhodonot presentfemoropatellarinstability.
ahigherprevalenceratio(2.04)insituationsoffemoropatellar instability.
The measurements defining the depth of the trochlea were clearly positive for femoropatellar instability in the patientswhosepatellaehadbecomedislocatedand sublux-ated.Amongthefourkneeswithalterationsofthefemoral trochlearangle,allofthemwereunstable.
The prevalence ratio calculations in the present study demonstrated that the prevalence of altered congruence angles in patients with patellar instability was 2.04 times greaterthaninstablepatients.Theprevalenceratioisamore conservativemeasurementthantheoddsratio.11 Sincethis wasacross-sectionalstudyandnotaprospectivecase-control study,wechosetouseprevalenceratios.Oddsratio calcula-tionson oursamplewould resultinvaluesof1.2and 0.53 for the patellar height according to the Insall-Salvati and Caton–Deschampsindicesand6.75foralterationsofthe con-gruenceangle.Thesedatareinforceourunderstandingthat theheightofthe patella isnotareliable indexfor assess-ingpatellarinstabilityamongpatientswithDownsyndrome, whereas the patellar congruence angle is relevant among thesepatients,asisthegrooveangle,whichwasfoundtobe alteredonlyinunstableknees.
We believe that absence of the patella in the femoral trochleaimpededformationofthetrochleargroove.Thisis suggestedfromtheobservationthatpatientswithout insta-bilitywhopresentedDownsyndromeshadnormaltrochlear depths. Studies using magnetic resonance imaging have demonstratedthatpatientswithnon-traumaticpatellar insta-bilityhavehighprevalenceoftrochleaewithlateralcondyle inclinationslessthan 11◦.12,13 Inourview,this meansthat
thetrochleaisshallowerwhenthereislessdemandforthe presenceofthe patella,therebygivingrisetolargerangles. Thepresenceofthepatellaalignedonthetrochleargrooveis whatdeterminesitsdepthandnormalshape.
Dejouretal.14believedthattrochleardysplasiawasa con-genitalalterationthatwouldbeapredisposingfactorfavoring femoropatellar instability.If this were so, trochlear dyspla-siamightbefoundinyoungpatientswhohadnotdeveloped instability,whichwasnotseeninthesamplestudiedhere.In ourview,trochleardysplasiacannotbetakentobecongenital, atleastinpatientswithDownsyndrome.
Finally,itneedstobeborneinmindthatthe osteoarticu-laralterationsseeninDownsyndromearegenerallymultiple andthatcareisrequiredintransposingtheseobservationsto patientswithoutDownsyndrome.
Conclusion
Fromthesamplestudied,thefindingssuggestthattrochlear dysplasiaisnotcongenital,butdevelopsasaresultofpatellar instability.
Theradiographicmeasurementsonthefemoraltrochlear depthshowedthatthetrochleawasatmorethan150◦(flat)
onlyincasesofinstability.
Basicradiographicmeasurements,suchasmeasurements ofthetrochleargrooveangle,correlatedwiththe femoropatel-larinstability.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.DejourH,WalchG,Nove-JosserandL,GuierC.Factorsof patellarinstability:ananatomicradiographicstudy.Knee SurgSportsTraumatolArthrosc.1994;2(1):19–26.
2.DugdaleTW,RenshawTS.Instabilityofthepatellofemoral jointinDown’ssyndrome.JBoneJointSurgAm.
1986;68(3):405–13.
3.MerchantAC.Femoralsulcusanglemeasurements.AmJ Orthop[BelleMead,NJ].1997;26(12):820–2.
4.MerchantAC,MercerRL,JacobsenRH,CoolCR.
Roentgenographicanalysisofpatellofemoralcongruence.J BoneJointSurgAm.1974;56(7):1391–6.
5.CatonJ.Methodofmeasuringtheheightofthepatella.Acta OrthopBelg.1989;55(3):385–6.
6.CatonJ,DeschampsG,ChambatP,LeratJL,DejourH.Patella infera.Aproposof128cases.RevChirOrthopReparatrice ApparMot.1982;68(5):317–25.
7.DiamondLS,LynneD,SigmanB.Orthopedicdisordersin patientswithDown’ssyndrome.OrthopClinNorthAm. 1981;12(1):57–71.
8.SeilR,MullerB,GeorgT,KohnD,RuppS.Reliabilityand interobservervariabilityinradiologicalpatellarheightratios. KneeSurgSportsTraumatolArthrosc.2000;8(4):231–6. 9.InsallJ,SalvatiE.Patellapositioninthenormalkneejoint.
Radiology.1971;101(1):101–4.
10.BarnettAJ,PrenticeM,MandaliaV,WakeleyCJ,EldridgeJD. Patellarheightmeasurementintrochleardysplasia.Knee SurgSportsTraumatolArthrosc.2009;17(12):1412–5. 11.ThompsonML,MyersJE,KriebelD.Prevalenceoddsratioor
prevalenceratiointheanalysisofcrosssectionaldata:what istobedone?OccupEnvironMed.1998;55(4):272–7.
12.CarrillonY,AbidiH,DejourD,FantinoO,MoyenB,Tran-Minh VA.Patellarinstability:assessmentonMRimagesby measuringthelateraltrochlearinclination-initialexperience. Radiology.2000;216(2):582–5.
13.SeilR,MullerB,GeorgT,KohnD,RuppS.Reliabilityand interobservervariabilityinradiologicalpatellarheightratios. KneeSurgSportsTraumatolArthrosc.2000;8(4):231–6. 14.DejourH,WalchG,NeyretP,AdeleineP.Dysplasiaofthe