www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Osteitis
and
mucosal
inflammation
in
a
rabbit
model
of
sinusitis
夽
,
夽夽
Carlos
Augusto
Correia
de
Campos
a,b,∗,
Eduardo
Landini
Lutaif
Dolci
a,b,
Leonardo
da
Silva
a,b,
José
Eduardo
Lutaif
Dolci
a,b,
Carlos
Alberto
Herrerias
de
Campos
b,
Ricardo
Landini
Lutaif
Dolci
a,baFaculdadedeCiênciasMédicas,SantaCasadeSãoPaulo,SãoPaulo,SP,Brazil bDepartmentofOtorhinolaryngology,SantaCasadeSãoPaulo,SãoPaulo,SP,Brazil
Received25June2014;accepted5August2014 Availableonline30March2015
KEYWORDS Sinusitis; Osteitis; Animalmodels
Abstract
Introduction:Severalexperimentalstudieshaveshownosteitisaftertheonsetofsinusitis, sup-portingtheideathatboneinvolvementcouldparticipateinthedisseminationandperpetuation ofthisinflammatorydisease.However,procedurescommonlyperformedfortheinductionof sinusitis,suchasantrostomies,cantriggersinusitisbythemselves.
Objective:Toevaluateosteitisinananimalmodelofsinusitisthatdoesnotviolatethesinus directlyandverifywhetherthisislimitedtotheinductionside,orifitaffectsthecontralateral side.
Methods:Experimentalstudyinwhichsinusitiswasproducedbyinsertinganobstructingsponge intothenasalcavityof20rabbits.Afterdefinedintervals,theanimalswereeuthanizedand maxillarysinussampleswereremovedforsemi-quantitativehistologicalanalysisofmucosaand bone.
Results:Signs ofboneand mucosal inflammationwere observed, affectingboth the induc-tionandcontralateralsides.Statisticalanalysisshowedcorrelationbetweentheintensityof osteitisonbothsides,butnotbetweenmucosalandboneinflammationonthesameside, sup-portingthetheorythatinflammationcanspreadthroughbonestructures,regardlessofmucosal inflammation.
夽 Pleasecitethisarticleas:deCamposCA,DolciEL,daSilvaL,DolciJE,deCamposCA,DolciRL.Osteitisandmucosalinflammationina
rabbitmodelofsinusitis.BrazJOtorhinolaryngol.2015;81:312---20.
夽夽Institution:DepartmentofOtorhinolaryngology,SantaCasadeSãoPaulo,SãoPaulo,SP,Brazil.
∗Correspondingauthor.
E-mail:[email protected](C.A.C.deCampos). http://dx.doi.org/10.1016/j.bjorl.2015.03.003
Conclusion: Thisstudydemonstratedthatinananimalmodelofsinusitisthatdoesnotdisturb thesinusdirectlyosteitisoccursintheaffectedsinusandthatitalsoaffectsthecontralateral side.
© 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE Sinusite;
Osteíte; Modelosanimais
Osteíteeinflamac¸ãomucosaemummodeloexperimentalderinossinusite
Resumo
Introduc¸ão: Diversos estudos experimentais evidenciam osteíte após estabelecimento de sinusite, corroborando para a ideia de que o envolvimento ósseo poderia participar na disseminac¸ãoeperpetuac¸ãodoprocessoinflamatório.Porémprocedimentosrealizadospara induc¸ãodadoenc¸anestesmodelos,comoantrostomias,podem,porsisó,desencadearosteíte.
Objetivo: Avaliarosteíteemummodeloderinossinusiteemquenãoocorremanipulac¸ãosinusal everificarseestaélimitadaaoladodeinduc¸ão,ouseacometeoladocontralateral.
Método: Estudo experimentalem que induziu-se rinossinusite em 20 coelhos, pormeio de obliterac¸ãotemporáriacomesponjadeumadascavidadesnasais.Amostrasdetecidosinusal foramsubmetidasàanálisehistológicasemiquantitativa,apóssacrifíciodosanimaisem inter-valosregulares.
Resultados: Foramobservadossinaisdeinflamac¸ãoósseaemucosa maisintensanoladode induc¸ão,mastambémcontralateral.Testesestatísticosevidenciaramcorrelac¸ãoentreaosteíte deambososlados,porémnãoentreinflamac¸ãoósseaemucosadeummesmolado,apoiando ateoriadequeainflamac¸ãopoderiasedisseminaratravésdotecidoósseo,independenteda inflamac¸ãomucosa.
Conclusão:Opresenteestudo evidenciouaexistênciade osteíte,tanto nolado deinduc¸ão quantonocontralateral,emmodeloexperimentalemquenãoocorremanipulac¸ãosinusal. ©2015Associac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicado por ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Severalfactorsmaycontributetotheonsetandpersistence ofsinonasalinflammation,leadingtochronicrhinosinusitis (CRS).Theserangefromalterationsrelatedtothehost,such as immunodeficiencies and mucociliary disease, to char-acteristics associated withetiological agents, suchas the capacitytoformbiofilmsandbacterialsuperantigens.1
Amongthese,theinvolvementoftheparanasalbonesin
CRSdevelopmentandmaintenancehasbeeninvestigated.
Theclosecontactbetweenboneandmucosainthisregion
and radiological findings in patients withCRS suggest the
involvementofthistissue.2---4
Several studies have disclosed the presence of sinus
bone inflammation in patients with CRS, usually using
tomographic assessment or histological analysis.2,5,6 This
incidence varies from36% to 100%,4,7,8 depending on the
methodchosenforpatientinclusionandtheformof
assess-ment.Apparently,theincidenceisgreaterwhenhistological
evaluation is performed, showing that, depending on the
intensityofosteitis,theremaynotbeevidenceof
inflam-mationontomographicassessment.8,9
In this sense, Lee et al. prospectively evaluated 121
patientswithCRStreatedsurgically.Basedontomography,
they observed signs of osteitis affecting 36% of patients
(82% ethmoid,64% sphenoid, 45%maxillary, without
eval-uationof thefrontalsinus)but observedhistologicalsigns
in 53%.4 Other studies showed that tomographic signs of
osteitis are associated with greater disease intensity in
anatomopathologicalexaminations7,9andworseoutcomein
surgicaltreatments.6
Themostcommonlyreportedsignsindicativeofosteitis
inpatients with CRS areperiosteal thickening, osteoblast
proliferation,boneresorptionandnewboneformation,and
inflammatorycellinfiltration.2,4,5,7---9
Although these studies have provided evidence of the
existenceof bone inflammation in casesof CRS andsome
clinicalimplications,othershave pointedoutthatosteitis
does not occur in all patients. Also, they have indicated
thatitgreatly increasesifthepatienthasbeenpreviously
submittedtosurgery (from6.7% to58%), which may
sug-gest the importance of other factors for its onset, such
as surgical trauma.4 Another important fact is that we
found no clinical studies that evaluated the presence of
boneinflammationinacuteepisodesofrhinosinusitis.That
is because acute rhinosinusitis (ARS) is usually treated
non-surgically,makingitdifficulttocollectsamplesfor
his-tologicalanalysis.Determiningwhether osteitisis present
attheearlystagesorifitarisesonlywiththepersistenceof
sinonasalinflammationwouldaidtofurtherunderstand its
role.
Forthispurpose,experimentalanimalmodelsareused,
usuallyrabbitmodels,inwhichboneandmucosal
withsinusitiscanberuledout,suchasallergicand
inflam-matorydisorders,druguse,previoussurgery,andanatomical
alterations.Thesestudiesshowbone involvementasearly
as two weeks after the rhinosinusitis induction process
has begun and persisting at varying intensities, for up to
13weeks.The most commonly described findingsof bone
inflammation aresimilar tothose reported in clinical
tri-als:periostealthickening,inflammatoryinfiltrate,increased
osteoclasticandosteoblasticactivity,newboneformation,
andeventuallyfibrosis.3,10---13
The problem with these experimental models is the
methodsbywhichthesinusitisisinduced.Normally,
defini-tive obliteration of the maxillary ostium drainage with
glue and sinus inoculation of an infectious agent through
an external sinusotomy are performed. These procedures
injureacertainareaofthesinuswallandalteritsphysiology
and,bythemselves, triggertissueinflammationregardless
oftheinfection.Moreover,thedefinitiveobliterationofthe
sinuscontaininga pathogenleadstoan intenseinfectious
process,that,iflimitedtothesinus cavityoftendoesnot
correspondtothepathophysiologyofthisdisease.14InARS,
infection usually has a nasal origin and maxillary ostium
obstructionisreversible,asitiscausedbymucosaledema.
There are experimental modelswhere rhinosinusitis is
inducedbyproceduresinwhichthereislessmanipulationof
theanimals’nasalcavity.Theyarecalledrhinogenicmodels
andarebasedontheintroduction ofaspongeintooneof
thenasalcavities, thatremains in placefor aset period.
Inthismethod,the sinusesarenotviolated,thus limiting
inflammationcausedbytheprocedure,andtheostial
block-ageisreversible.Therefore,thesemodelsbetterreflectthe
physiopathogenyofthisdiseaseinhumans.14---16
Therefore, the present study aimed to determine
whethersinusboneinflammationoccurs,tocorrelateitwith
mucosalinflammation inanexperimentalmodelof
rhinos-inusitisinwhichthereisnomanipulationof theparanasal
sinusandtoverifywhetherthisinflammation islimitedto
theinductionside,orifitalsoaffectsthecontralateralside.
Methods
Atotalof 22adult, white,maleandfemaleNew Zealand
rabbits were used, weighing approximately 2500g at the
beginningoftheexperiment.Throughoutthestudy,the
ani-malsweremaintained in individualcages suitablefor the
breedandweightandhadfreeaccesstofoodandwater.
Bacterialrhinosinusitiswasinducedin20of22animals,
byplacingasmallpieceofporouspolyvinylsponge
measur-ing3.0cm×0.5cm×0.3cm,previouslysterilizedwith
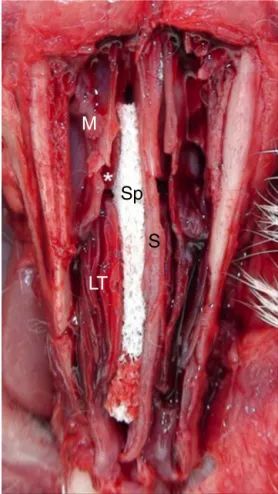
ethy-leneoxide,intotherightnasalcavityoftheanimals(Fig.1).
The sponges were soaked in 1.0mL solution containing
streptococcalandstaphylococcaltoxoid.Noprocedurewas
performedintheleftnasalcavity.Twoanimalsusedas
con-trolswereeuthanizedwithoutundergoinganyintervention.
After10days,thespongeswereremovedandsixanimals
wererandomly euthanized(10th day of the experiment).
After another 7 days, during which the animals did not
undergoanyfurtherintervention,sevenadditionalanimals
wereeuthanized(17thdayoftheexperiment). Finally,on
the30thdayoftheexperiment,thelastsevenanimalswere
euthanized.
M
Sp
S
LT
Figure 1 Anatomicalspecimen showing sponge (Sp)placed inthe nasalcavity ofrabbits.Observe thenasal septum(S), themaxillarysinus(M),themiddleturbinate(*),andthelower turbinateontheright(LT).
All procedures were performed under anesthesia with
spontaneousbreathing,accordingtostandardsestablished
by the Brazilian Society of Laboratory Animal Science
(SociedadeBrasileiradeCiênciaemAnimaisdeLaboratório
---SBCAL)andafterapprovalbytheethicscommitteeofthe
institution,underNo.2011-4.
After euthanization, opening of the outer wall of the
nasalcavityandparanasalsinuseswasperformed.Next,the
entiremedialwallofthemaxillarysinusonboththeinduced
sinusitis sideand the contralateralside wasremoved and
samplescontainingboneandmucosaltissuewereobtained.
Thematerialofeachsamplewasfixedinbufferedformalin,
dehydratedatincreasingconcentrationsofethanol,cleared
inxylene,andembeddedinparaffin.Itwasthenslicedwith
amicrotome into4-mmthicksectionsthatwere mounted
onslides,andstainedwithhematoxylinandeosin(HE).
The slideswere evaluatedusing opticalmicroscopy by
apathologistblindedtoeachanimal experimentprotocol.
Themucosaltissueandbonesamplesweregradedaccording
toinflammatory parameters,semi-quantitatively. The
fol-lowingwasconsideredfor mucosalinflammation:grade0,
absenceofinflammation;grade1,mildinflammation(slight
inflammatorycellinfiltrate inthemucosa);grade2,
mod-erateinflammation(diffuseinflammatoryinfiltrate);grade
3, intense inflammation (diffuse inflammatory infiltrate,
architecture).Forboneinflammationclassification,the
fol-lowingwasconsidered:grade0,absenceofinflammation;
grade 1, mild inflammation (mild periosteal thickening);
grade2,moderateinflammation(moderateperiosteal
thick-eningandosteoblasticrimming---osteoblastlayeralongthe
newly formed bone); grade 3, intenseinflammation
(pro-nouncedperiostealthickening,presenceofnon-mineralized
osteoidmatrixandosteoblasticrimming).
Secretion from the maxillary sinus was also collected
using swabs. These samples were plated on blood agar,
Sabouraudagar,andchocolateagarculturemedia(Probac
doBrasil).Thebloodandchocolateagarplateswere
incu-batedat35±2◦C,whileSabouraudagarplateswerekept
atroomtemperature.Dailyreadingsoftheplateswere
per-formedforupto15days.
Statistical analysis sought to correlate the degree of
inflammationofthemucosalandbonetissueonthedifferent
sides,inordertoverifyhowthisinflammationbehaved
dur-ingfollow-upandwhethertherewasanassociationbetween
the degree of inflammation and identifiedpathogens. For
thatpurpose,themucosalandbonehistologydataaswell
as culture test results were described according to the
sideofinterventionandtimeofeuthanization,using
abso-luteandrelativefrequencies.Thesedatawereanalyzedby
pairedWilcoxon,Kruskal---Wallis,andlikelihoodratiotests.
Finally, Spearman’stest was performed tocorrelate bone
andmucosalinflammationonthedifferentsides. Alltests
wereperformedwithasignificancelevelof5%.
Results
At the time of sponge removal, all animals had purulent
rhinorrheaonthesidewherethespongehadbeenplaced,
whereasnoneofthemhadcontralateralrhinorrhea.Noneof
theanimalsdiedbeforethescheduledtimefor
euthaniza-tion.
Figure2 Sample of right maxillary sinus mucosa, showing epithelial alterations, neovascularization, connective-fibrous proliferation,andinflammatorycellinfiltrate---optical micro-scopy,hematoxylinandeosinstaining,100×magnification.
Histological evaluation of mucosal samples showed a
rangeofoutcomes,fromanimalswithsignificant
inflamma-toryprocesstoanimalswithalmostnormalmaxillarysinus
mucosa. Alterations such as inflammatory cell infiltrate,
neovascularization,subepithelialglandularhyperplasiaand
destruction, andepithelial alterations suchasulcerations
andciliarydestructionwereobserved.Somesignsthat
char-acterizechronicity,suchasconnective-fibrousproliferation
and mucosal hyperplasia, were also identified in animals
euthanizedlaterintheexperiment(Fig.2).Ofthe20rabbits
evaluated,three(15%)hadnosignsofmucosalinflammation
ontheinductionsideandnine(45%)didnotshowthesesigns
on the contralateral side. Therefore, the right maxillary
sinusmucosashowedagreaterdegreeofinflammationthan
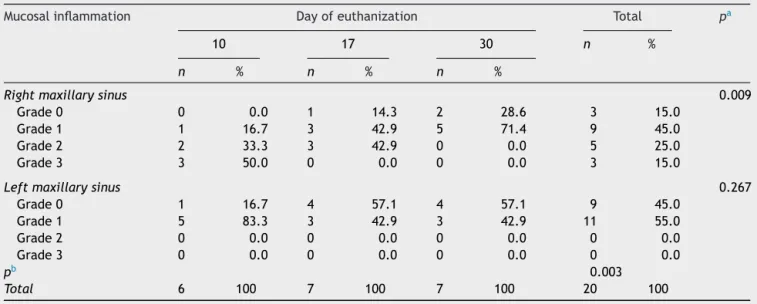
Table1 Descriptionofthesinusmucosahistologyaccordingtosideandtimeofeuthanizationandresultsofthecomparative tests.
Mucosalinflammation Dayofeuthanization Total pa
10 17 30 n %
n % n % n %
Rightmaxillarysinus 0.009
Grade0 0 0.0 1 14.3 2 28.6 3 15.0
Grade1 1 16.7 3 42.9 5 71.4 9 45.0
Grade2 2 33.3 3 42.9 0 0.0 5 25.0
Grade3 3 50.0 0 0.0 0 0.0 3 15.0
Leftmaxillarysinus 0.267
Grade0 1 16.7 4 57.1 4 57.1 9 45.0
Grade1 5 83.3 3 42.9 3 42.9 11 55.0
Grade2 0 0.0 0 0.0 0 0.0 0 0.0
Grade3 0 0.0 0 0.0 0 0.0 0 0.0
pb 0.003
Total 6 100 7 100 7 100 20 100
n,numberofanimals;%,relativepercentageofanimals. a Kruskal---Wallistestresult.
Figure 3 Right maxillary sinus sample showing osteoblast layerover the bonematrix (osteoblastic rimming) and some osteocytes---opticalmicroscopy,hematoxylinandeosin stain-ing,400×magnification.
thatoftheleftmaxillarysinus(p=0.003)andthis
inflamma-tiondecreasedovertimeinastatisticallysignificantmanner
(p=0.009),asshowninTable1.
Themucosalsamplesofthetwocontrolanimals,which
wereeuthanizedbeforerhinosinusitisinduction,showedno
inflammatorysign.Therefore,theywereclassifiedasgrade
0,bothfortheleftandrightmaxillarysinuses.
Histological assessment of bone samples also showed
severalcharacteristicsof inflammation,suchasperiosteal
thickening, osteoblastic proliferation and border,
osteo-clastproliferation,alteredbonearchitecture,presenceof
immaturebonewithdisorganizedcollagenfibers,and
non-mineralizedosteoidmatrixdeposition(Fig.3).Ontheright
side, the animals showed a higher degree of
inflamma-tion than on the left (p=0.004) and this inflammation
Time (days)
10 2.5000
2.0000
1.5000
1.0000
0.5000
0.0000
Right bone
Deg
ree of inflammation
Left bone
17 30
Figure4 Meandegreesofboneinflammationonbothsides overtime.
decreased overtimeonbothsides, withstatistical
signifi-cance(p=0.046andp=0.037).Two(10%)ofthe20assessed
animalsshowednosignsof bone inflammationonthe
rhi-nosinusitisinductionsideandfour(20%)didnotshowsigns
ofinflammation onthecontralateralside(Table2).
Histo-logicalsignsofboneinflammationwerealsonotobservedin
samplestakenfromcontrolanimals.
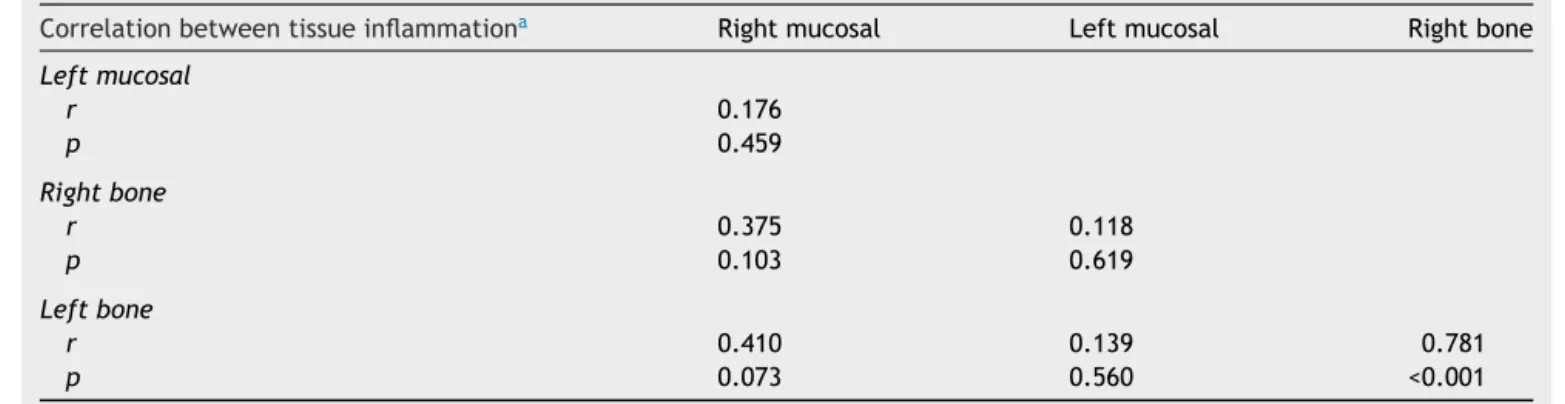
A direct correlation was observed between the
inten-sity of inflammation observed in the right maxillarybone
samplesandthatoftheleftmaxillarybonecollectedover
time(p<0.001). Thatis, asbone inflammation decreased
ontheinductionside,thisalsooccurredonthe
contralat-eral side (Table 3 and Fig. 4). This direct association of
inflammationevolutionovertimewasnotobservedamong
themucosalsamplesobtainedfrombothsidesor between
the mucosal and bone samples collected from the same
side.
Table2 Descriptionofsinusbonehistologyaccordingtosideandtimeofeuthanizationandresultsofthecomparativetests.
Boneinflammation Dayofeuthanization Total pa
10 17 30 n %
n % n % n %
Rightmaxillarysinus 0.046
Grade0 0 0.0 0 0.0 2 28.6 2 10.0
Grade1 2 33.3 1 14.3 3 42.9 6 30.0
Grade2 1 16.7 4 57.1 2 28.6 7 35.0
Grade3 3 50.0 2 28.6 0 0.0 5 25.0
Leftmaxillarysinus 0.037
Grade0 0 0.0 0 0.0 4 57.1 4 20.0
Grade1 3 50.0 3 42.9 2 28.6 8 40.0
Grade2 2 33.3 4 57.1 1 14.3 7 35.0
Grade3 1 16.7 0 0.0 0 0.0 1 5.0
pb 0.004
Total 6 100 7 100 7 100 20 100
n,numberofanimals;%,relativepercentageofanimals. aKruskal---Wallistestresult.
Table3 Correlationbetweenthedegreeofinflammationobservedinsamplesofbonetissueandmucosaltissue.
Correlationbetweentissueinflammationa Rightmucosal Leftmucosal Rightbone
Leftmucosal
r 0.176
p 0.459
Rightbone
r 0.375 0.118
p 0.103 0.619
Leftbone
r 0.410 0.139 0.781
p 0.073 0.560 <0.001
r,correlationvalue(rangingfrom1to−1;whencloserto1,thecorrelationisdirectandwhencloserto−1,thecorrelationisindirect). a Spearman’scorrelationtest.
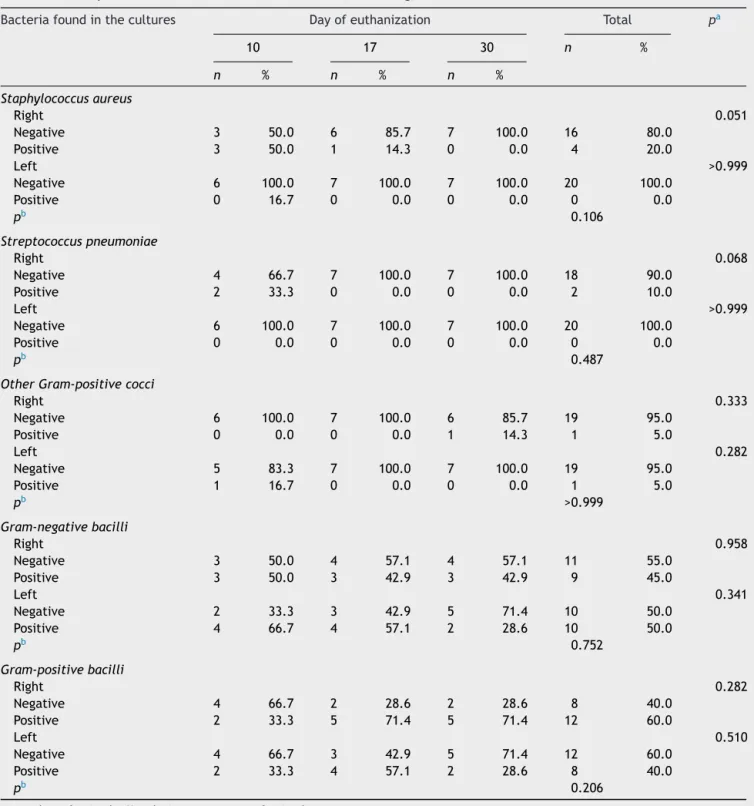
Culturetestresultsshowedhigherpositivityontheside
where rhinosinusitis was induced, compared to the
con-tralateralside,butwithoutstatisticalsignificance.Culture
testsofthetwocontrolanimalswerenegative.
Staphylococcus aureus and Streptococcus pneumoniae,
theagentsusedinrhinosinusitisinduction,werefoundonly
intherightmaxillarysinusof theanimalseuthanized
ear-lier.Other microorganisms,mostlyGram-negative,suchas
Escherichiacoli,Acinetobacterbaumanii,andPseudomonas aeruginosa, were found on both the induction and
con-tralateralsidesandatthedifferenttimesoffollow-up.No
statistically significant differences were observed for the
microorganismsfound onbothsides. Additionally,no
asso-ciation wasobserved between the etiological agents and
sideofinductionortimeofeuthanization,orbetweenthe
etiologicalagentsandinflammationintensity(Table4).
Discussion
Experimental models allow assessments ranging from
aspects related to the pathogenesis of rhinosinusitis to
the effectivenessof different formsof treatment for this
disease.17---22 Among several methodsdescribed for
rhinos-inusitis induction,thisstudy utilizedtheintroductionof a
spongecontainingatoxoidagentintooneofthenasal
cavi-tiesoftheanimals.Inadditiontobeingatechnicallysimple
andefficientproceduretoproducesinusitisin100%of
ani-malsinseveralstudies,22,23itcauseslittleinjurytothenasal
mucosaandnosinusinjury.
Perhapsthisisthemaincharacteristicthatdifferentiates
thepresentinvestigationfromothersdescribedinthe
liter-ature,inthatitassessesboneinflammationinexperimental
models.3,10---13 Proceduresperformedin thesestudies,such
asmaxillaryostiumobliterationwithglueandsinus
inocu-lationofaninfectiousagentperformedthroughsinusotomy,
rupture theosteomucosal wall,alter themucociliaryflow
pattern,damagethevascularnetworkandcause,by
them-selves, an inflammatory process. These procedures also
strip the mucosa from small areas of the sinus bone in
the sinusotomy sites; this bone exposure could facilitate
the involvement of this tissue by pathogenic agents and
theirtoxins.Similarreasonsmightexplain,atleastinpart,
the increased incidence of osteitis in patients with CRS
submittedtoprevious nasalsurgery, comparedwiththose
thatwereneversubmittedtosurgicalprocedures(from6.7%
to58%).4
Moreintensesignsofinflammationwereobserved
affect-ing the mucosal and bone tissue in the early-euthanized
groups and on the induction side. These findings suggest
thatbone inflammation,whichhadalreadybeenobserved
byotherauthors3,11---13eveninexperimentalmodelsinwhich
maxillaryostiumobstructionwastemporary;isprobablydue
to sinus infection rather than the trauma related to the
induction procedures.Still, this inflammation significantly
affectsthemucosaandbone,notonlyontheinductionside,
butalsoonthecontralateralside.
Thepresentstudyusedthehistologicalclassification
pro-posed by Antunes et al., as this method was employed
in an experimental model of rhinosinusitis that assessed
both bone and mucosal tissue.24 This semi-quantitative
assessmentdemonstratedadirectcorrelationbetweenthe
intensityof bone inflammation thatoccurred onthe right
sideandontheleftside.Thatis,althoughlesssevereonthe
leftside,bothsimilarlydecreasedovertime.This
associa-tionwasnotobservedbetween themucosal inflammation
onboth sidesor betweenbone inflammation andmucosal
tissueonthesameside.
Itispossiblethattheinflammationoftenobservedinthe
maxillarysinusontheoppositesideoftheinductioncouldbe
causedbyanopportunisticbacterialinfection,whichwould
spreadthroughthenasalandparanasalsinusestobothsides,
firstaffectingthe mucosaltissueandlater theunderlying
bonetissue.This hypothesis wouldbe consistentwiththe
positiveresultsin culturetestsfromboth sides. However,
inthiscase onewould expecttosee,a directcorrelation
betweentheintensityofinflammationobservedinbone
tis-sueand that observed inthe mucosal tissueonthe same
side,butnotbetweenthebonetissueononesideandthe
contralateralbonetissue.
Perloffetal.observedsignsofboneandmucosal
inflam-mation on the contralateral side, distant from the site
of induction in animals euthanized between seven and
13 weeks after the start of the experiment. They also
described signs of chronicity, and in the bone histology,
theyobserved increased vascularization and expansion of
theHaversiancanalscontaininginflammatorycells.Fibrosis
wasfoundinthesecanalsinsomeanimalseuthanizedata
Table4 Descriptionofthebacteriafoundinthecultures,accordingtosideandtimeofeuthanization.
Bacteriafoundinthecultures Dayofeuthanization Total pa
10 17 30 n %
n % n % n %
Staphylococcusaureus
Right 0.051
Negative 3 50.0 6 85.7 7 100.0 16 80.0
Positive 3 50.0 1 14.3 0 0.0 4 20.0
Left >0.999
Negative 6 100.0 7 100.0 7 100.0 20 100.0
Positive 0 16.7 0 0.0 0 0.0 0 0.0
pb 0.106
Streptococcuspneumoniae
Right 0.068
Negative 4 66.7 7 100.0 7 100.0 18 90.0
Positive 2 33.3 0 0.0 0 0.0 2 10.0
Left >0.999
Negative 6 100.0 7 100.0 7 100.0 20 100.0
Positive 0 0.0 0 0.0 0 0.0 0 0.0
pb 0.487
OtherGram-positivecocci
Right 0.333
Negative 6 100.0 7 100.0 6 85.7 19 95.0
Positive 0 0.0 0 0.0 1 14.3 1 5.0
Left 0.282
Negative 5 83.3 7 100.0 7 100.0 19 95.0
Positive 1 16.7 0 0.0 0 0.0 1 5.0
pb >0.999
Gram-negativebacilli
Right 0.958
Negative 3 50.0 4 57.1 4 57.1 11 55.0
Positive 3 50.0 3 42.9 3 42.9 9 45.0
Left 0.341
Negative 2 33.3 3 42.9 5 71.4 10 50.0
Positive 4 66.7 4 57.1 2 28.6 10 50.0
pb 0.752
Gram-positivebacilli
Right 0.282
Negative 4 66.7 2 28.6 2 28.6 8 40.0
Positive 2 33.3 5 71.4 5 71.4 12 60.0
Left 0.510
Negative 4 66.7 3 42.9 5 71.4 12 60.0
Positive 2 33.3 4 57.1 2 28.6 8 40.0
pb 0.206
n,numberofanimals;%,relativepercentageofanimals. aLikelihoodratiotestresult.
b McNemartestresult.
theHaversiancanal system,implying thatthis couldbea
pathwayfordisseminationofinflammationtodistantsites.
Signsofcontralateralosteitiswereobservedinanimals
euth-anizedbetweensevenandnineweeksafterinfection.They
evensuggestedthefollowingsequenceofeventstoexplain
thedissemination:maxillarysinusmucosaldisease onone
side,entryofinfectiousandinflammatoryagentsinto
adja-centbone, activation of bone remodelingprocess, access
tothevascularnetwork,disseminationthroughbonetothe
contralateralside,andsecondaryinflammationof
contralat-eralmucosa.13
In the present study, inflammatory cell infiltrate,
osteoblast proliferation, and other characteristics of
bone remodeling were observed. However, no alterations
were observed in the Haversian system canals, perhaps
studies andbecause themaxillarysinus clearance limited
the inflammatory process. But even without histological
alterations,thiscanalsystemmayallowinflammatory
medi-atorstospreadtonon-adjacentbonestructures.Thiswould
explain the fact that signs of inflammation were found
in the left maxillary sinus in this study and the finding
thatthe leftosteitisintensity wascorrelated totheright
osteitis intensity rather than the underlying left mucosal
inflammation. The dissemination of inflammation to
dis-tant sites through bone tissue implies that these sites
onlyimproveafterimprovementofthesiteoftheoriginal
inflammation.
AhigherpercentageofS.aureusandS.pneumoniae,the
agentsinoculatedintotherabbits,wasfoundonthe
induc-tionsideandin theanimalsthatwereeuthanizedearlier.
Regardingotherpathogens,themostfrequentlyisolatedwas
E.coli.Severalotherbacilliwerealsoobserved,bothGram
positiveandGramnegative.Manyofthesemicro-organisms
are opportunisticpathogens of the respiratory and
diges-tive system of rabbits, which after the prolonged course
ofrhinosinusitisand theresultingalterationsinthe upper
respiratorytract,acquirethemeanstomultiplyandoften
replacetheoriginalinfection-causingagent,asdescribedby
otherauthors.23,25
Perloffetal.andKhalidetal.isolatedtheagentsusedfor
inductioninallanimalseuthanizedattheendofthe
experi-ment.Thisisperhapsduetothefactthattheseauthorsused
morepathogenicagents(P.aeruginosaandS.aureus),
asso-ciatedwith definitivesinus obliteration.3,13 Westrin et al.
usedS.pneumoniaeandBacteroidesfragilisforthe
induc-tionof experimental bacterial rhinosinusitis andanalyzed
thesubsequentbacteriologicalterations.Onaverage,they
observedthesubstitutionofpneumococcusafter5daysof
culture.However,theyidentifiedB.fragilisonthedayof
euthanizationofallanimalsthatwereinoculated.10
Thepresentstudyfoundnocorrelationbetweenthetests
identifiedinbacterialcultureandthedegreeof
inflamma-tion in the mucosal or bone tissue onboth sides. This is
explainedbythediverseflorafoundatthosesites,mostly
consistingofopportunisticagentsthatarecapableof
pro-liferating in the inflamed sinus, perhaps related to the
inductionmethod.
Thefindingsofthisstudyshowthatthesinusbone
inflam-mationoccursearlyafterrhinosinusitisinduction.Theyalso
demonstratethatprolongedmaintenanceofinfectionor
sur-gical trauma is not necessary for the underlying bone to
beaffected andfor thisinvolvement toextendtodistant
sites. Itcanbe observedthat,despite thisinitial
involve-ment, bone inflammation at the induction site tends to
improvewithsinusclearingandearlyventilation,andthat
thisimprovementis accompaniedbyimprovementinbone
inflammationatdistantsites.Finallythisinflammationdoes
notoccuronlyinthepresenceofaspecificetiologicalagent,
butalsointhepresenceofdiverseflora.
The involvement of bone in the pathogenesis of
rhi-nosinusitis, already addressed in previous clinical and
experimental research, needs to be better understood.
This capacitytotransmitinflammation todistantsites,as
suggestedbytheresultsofthisstudy,couldexplainthe
char-acteristicsobserved intheclinical pictureof thisdisease,
suchdiseasedisseminationfromafrontalorsphenoidsinus
tothe other, throughthe inter-sinus septum,or from the
ethmoidsinustothemiddleturbinate.Itcouldalsoexplain
thereasonforthepersistenceofsymptomsinsomepatients,
evenwithmedicaltreatment,andtheneedtoremovenot
onlythe mucosabut also theunderlying bone, in specific
cases,inordertoobtainclinicalimprovement.
However,caremustbetakenin extrapolatingthe
find-ings of experimental studies into daily clinical practice.
CRSis notonly an infectious disease,but amultifactorial
process,withenvironmental, individual, andhost genetic
predisposingfactors.Eventheinflammatory-infectious
find-ingsofthisstudy,compatiblewiththeARSpicture,needto
betestedinothermodels,indifferentperiods,and
evalu-atingotheragents.However,itisevidentthatthesinonasal
inflammationin thisprocessisnotlimitedtothemucosa,
butalsoexists inthe underlyingbone tissue.Anditshole
needstobebetterunderstood,sothattreatmentsthat
re-establishnormalityinbothtissuescanbeformulated.
Conclusion
Inanexperimentalrhinosinusitismodelinwhichtherewas
nomanipulationof theparanasalsinus,thisstudy
demon-stratedthepresenceofinflammatorysignsinthesinusbone
tissue,whichaffectedboththeinductionandthe
contralat-eralside.
Wedocumenteda correlationbetween bone
inflamma-tion on both sides, but not between bone and mucosal
inflammationonthesameside.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.FokkensW,LundV,MullolJ,BachertC,AlobidI,BaroodyF,etal. Europeanpositionpaperonrhinosinusitisandnasalpolyps2012. Rhinology.2012;50:1---298.
2.KennedyDW,SeniorBA,GannonFH,MontoneKT,HwangP,Lanza DC.Histologyandhistomorphometryofethmoidboneinchronic rhinosinusitis.Laryngoscope.1998;108:502---7.
3.Perloff JR, Gannon FH, Bolger WE, Montone KT, Orlandi R, Kennedy DW. Bone involvement in sinusitis: an apparent pathway for the spreadofdisease. Laryngoscope. 2000;110: 2095---9.
4.Lee JT, Kennedy DW,Palmer JN, Feldman M, Chiu AG.The incidence of concurrent osteitis in patients with chronic rhinosinusitis: a clinicopathological study. Am J Rhinol. 2006;20:278---82.
5.ToviF,BenharrochD,GatotA,HertzanuY.Osteoblasticosteitis ofthemaxillarysinus.Laryngoscope.1992;102:426---30. 6.KimHY,DhongHJ,LeeHJ,ChungYJ,YinYJ,OhJW,etal.
Hyper-ostosis may affect prognosis after primary endoscopic sinus surgeryforchronicrhinosinusitis.OtolaryngolHeadNeckSurg. 2006;135:94---9.
7.Giacchi RJ, Lebowitz RA, Yee HT, Light JP, Jacobs JB. Histopathologic evaluation of the ethmoid bone in chronic sinusitis.AmJRhinol.2001;15:193---7.
9.Cho SH, Min HJ, HanHX, Paik SS, Kim KR. CT analysis and histopathologyofboneremodelinginpatientswithchronic rhi-nosinusitis.OtolaryngolHeadNeckSurg.2006;135:404---8. 10.Westrin KM, Norlander T, Stierna P, Carlsoo B, Nord CE.
Experimentalmaxillary sinusitisinducedbyBacteroides frag-ilis. A bacteriologicaland histological studyin rabbits.Acta Otolaryngol.1992;112:107---14.
11.NorlanderT,ForsgrenK,KumlienJ,StiernaP,CarlsooB. Cellu-lar regenerationand recoveryofthemaxillary sinusmucosa. An experimental study in rabbits. Acta Otolaryngol Suppl. 1992;492:33---7.
12.Bolger WE, Leonard D,Dick EJ Jr,Stierna P. Gramnegative sinusitis:abacteriologicandhistologicstudyinrabbits.AmJ Rhinol.1997;11:15---25.
13.KhalidAN,HuntJ,PerloffJR,KennedyDW.Theroleofbonein chronicrhinosinusitis.Laryngoscope.2002;112:1951---7. 14.MarksSC.Acutesinusitisintherabbit:anewrhinogenicmodel.
Laryngoscope.1997;107:1579---85.
15.MarksSC.Acutesinusitisintherabbitmodel:histologicanalysis. Laryngoscope.1998;108:320---5.
16.KaraCO,CetinCB,DemirkanN,SengulM,TopuzB,PinarHS, et al.Experimental sinusitisin arhinogenicmodel. Laryngo-scope.2004;114:273---8.
17.MinYG,KimYK,ChoiYS,ShinJS,JuhnSK.Mucociliaryactivity andhistopathologyofsinusmucosainexperimentalmaxillary sinusitis:acomparisonofsystemicadministrationofantibiotic and antibiotic delivery bypolylactic acid polymer. Laryngo-scope.1995;105:835---42.
18.BendeM,Fukami M,ArforsKE,MarkJ, StiernaP,Intaglietta M.Effectofoxymetazolinenosedropsonacutesinusitisinthe rabbit.AnnOtolRhinolLaryngol.1996;105:222---5.
19.MaeyamaT.Astudyofexperimentalsinusitisinrabbits.Auris NasusLarynx.1981;8:87---98.
20.CableBB,WassmuthZ,MannEA,HommerD,ConnelyG,Klem C,etal.Theeffectofcorticosteroidsinthetreatmentof exper-imentalsinusitis.AmJRhinol.2000;14:217---22.
21.SutbeyazY,AktanB,YorukO,OzdemirH,GundogduC. Treat-ment of sinusitis with corticosteroids in combination with antibioticsinexperimentallyinducedrhinosinusitis. AnnOtol RhinolLaryngol.2008;117:389---94.
22.ChengY,WeiH, LiZ,XueF,JiangM,ChenW, etal. Effects ofintranasalcorticosteroidsinthetreatmentofexperimental acutebacterialmaxillarysinusitisinrabbits.ORLJ Otorhino-laryngolRelatSpec.2009;71:57---65.
23.CostaHO,LuchiGER,AugustoAG,CastroM,SouzaFC.Estudo comparativoentrediversastécnicasdeconfecc¸ãodemodelo experimentaldesinusiteinflamatóriaemcoelhos.BrazJ Otorhi-nolaryngol.2007;73:627---31.
24.AntunesMB,FeldmanMD,CohenNA,ChiuAG.Dose-dependent effects of topical tobramycin in an animal model of Pseu-domonassinusitis.AmJRhinol.2007;21:423---7.