REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
The
correlation
among
the
Ramsay
sedation
scale,
Richmond
agitation
sedation
scale
and
Riker
sedation
agitation
scale
during
midazolam-remifentanil
sedation
Turgut
Namigar
a,∗,
Karacalar
Serap
a,
Akdas
¸
Tekin
Esra
a,
Odacılar
Özgül
a,
Öztürk
Ali
Can
a,
Ak
Aysel
a,
Ali
Achmet
baOkmeydaniTrainingandResearchHospital,DepartmentofAnesthesiologyandIntensiveCare,Istanbul,Turkey bIstanbulUniversity,IstanbulMedicalFaculty,DepartmentofAnesthesiologyandIntensiveCare,Istanbul,Turkey
Received11June2015;accepted19July2016 Availableonline10August2016
KEYWORDS Criticallyill; Sedationscale; Validity; Reliability
Abstract
Backgroundandobjectives: Sedative and analgesic treatment administered to critically ill patientsneedtoberegularlyassessedtoensurethatpreviouslystatedgoalsarewellachieved astheriskofcomplicationsofoversedationisminimized.Werevisedandprospectivelytested theRamsaySedationscale(RSS)forinterraterreliabilityandcompareditwiththe Sedation-AgitationScale(SAS)andtheRichmondAgitationSedationScale(RASS)totestconstructvalidity duringmidazolam-remifentanilsedation.
Methods:AconveniencesampleofICUpatientswassimultaneouslyandindependently exam-inedbypairs oftrained evaluatorsbyusingtherevisedSAS,RSS, andRASS.Ninety-twoICU patientswereexaminedatotalof276timesbyevaluatorpairs.
Results:Themeanpatientagewas61.32±18.68years,45,7%werefemale(n=42),54.3%male (n=50).TheirAPACHEvaluesvariedbetween3and39withanaverageof13.27±7.86and75%of thecaseswereundermechanicalventilation.WhenclassifiedbyusingRSS(2.70±1.28),10.9% wereanxiousoragitated(RSS1),68.5%werecalm(RSS2---3),and20.6%weresedated(RSS4---6). WhenclassifiedbyusingRASS(−0.64±1.58),20.7%wereanxiousoragitated(RASS+1to+4), 63.0% werecalm(RASS0to−2),and16.3%weresedated(RASS−3to−5).Whenclassified byusingSAS(2.63±1.00),12%wereanxiousoragitated(SAS5---7),57.6%werecalm(SAS4), and30.4%weresedated(SAS1---3).RSSwascorrelatedwiththeSAS(r=−0.656,p<0.001)and RASSwascorrelatedwiththeSAS(r=0.565,p<0.001).RSSwashighlycorrelatedwiththeRASS (r=−0.664,p<0.001).
Conclusions: Ramsayisbothreliableandvalid(highcorrelationwiththeRASSandSASscales) inassessingagitationandsedationinadultICUpatients.
©2016SociedadeBrasileiradeAnestesiologia.Publishedby ElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗Correspondingauthor.
E-mails:[email protected],[email protected](T.Namigar).
http://dx.doi.org/10.1016/j.bjane.2016.07.002
PALAVRAS-CHAVE Estadocrítico; Escaladesedac¸ão; Validade;
Confiabilidade
Correlac¸ãoentreaescaladesedac¸ãodeRamsay,escaladesedac¸ão-agitac¸ão deRichmondeescaladesedac¸ão-agitac¸ãodeRikerdurantesedac¸ão
commidazolam-remifentanil
Resumo
Justificativaeobjetivos: Otratamentodepacientesemestadocríticocomsedativose anal-gésicosdeveserregularmenteavaliadoparagarantirqueasmetaspré-definidasestãosendo atingidas,bemcomominimizaroriscodecomplicac¸õesresultantesdesedac¸ãoem excesso. ConduzimosumarevisãoetestamosprospectivamenteaEscaladeSedac¸ãodeRamsay(Ramsay SedationScale[RSS])paraaconfiabilidadeinteravaliador eacomparamoscomaEscala de Sedac¸ãoeAgitac¸ãodeRiker(RikerSedation-AgitationScale[RRSAS])eaEscaladeSedac¸ãoe Agitac¸ãodeRichmond(RichmondAgitationSedationScale[RASS])paratestaravalidadede construtoduranteasedac¸ãocommidazolam-remifentanil.
Métodos: UmaamostradeconveniênciadepacientesdeUTIfoisimultâneae independente-menteexaminadaporparesdeavaliadorestreinadoscomousodasescalasrevisadasRRSAS, RSSeRASS.Foramexaminados92pacientesdeUTIporparesdeavaliadoresem276momentos.
Resultados: Amédia dospacientesfoide 61,32±18,68 anos;45,7% eramdosexo feminino (n=42)e54,3%domasculino(n=50).Seusescores APACHEvariaramentre3-39,commédia de13,27±7,86,e75%doscasosreceberamventilac¸ãomecânica.QuandoRSSfoiusadapara aclassificac¸ão(2,70±1,28),10,9%dospacientesestavamansiososouagitados(RSS1),68,5% estavamcalmos(RSS2a3)e20,6%estavamsedados(RSS4a6).QuandoRASSfoiusadaparaa classificac¸ão(-0,64±1,58),20,7%dospacientesestavamansiososouagitados(RASS+1a+4), 63,0%estavamcalmos(RASS0a-2)e16,3%estavamsedados(RASS-3a-5).QuandoRSASfoi usadaparaaclassificac¸ão(2,63±1,00),12%dospacientesestavamansiososouagitados(RSAS 5a7),57,6%estavamcalmos(RSAS4)e30,4%estavamsedados(RSAS1a3).Houvecorrelac¸ão deRSScomRSAS(r=-0,656,p<0,001)edeRASScomRSAS(r=0,565,p<0,001).Houveforte correlac¸ãodeRSScomRASS(r=-0,664,p<0,001).
Conclusões:ARSSéconfiáveleválida(fortecorrelac¸ãocomRASSeRSAS)paraavaliarasedac¸ão eagitac¸ãoempacientesadultosinternadosemUTI.
©2016SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigoOpen Accesssobumalicenc¸aCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
AnalgesiaandsedationareusedintheIntensive CareUnit (ICU)forimprovingthecomfortandsafetyofpatients under-going intensive care therapies. Nevertheless, continuous administrationofsedatives prolongsthetimeon mechan-ical ventilation and ICU stay. These adverse effects can be reduced by clear definition of the goals of sedation combinedwitha sedation protocol.1 Because of the mul-tiplicityofpatientsadmittedtoICU,itisdifficulttodefine astandardprocedureforICUsedation.Onemayencounter avarietyof pathologiesofdifferentgrades ofseverity;in addition, the associated morbidity, the circulatory insta-bilityandthepharmacodynamicalterationsincriticallyill patientscanmaketreatmentguidelinedifficulttoestablish and implement.2 Precise control of the depth of seda-tion is often not well managed; patients are frequently over-or-undersedated with an accompanying increase in morbidity,mortalityand,economiccost.3Sedativeand anal-gesictreatmentadministeredtocriticallyillpatientsshould beregularlyassessed toensure thatpredefinite goals are wellachievedastheriskofcomplicationsofoversedationis minimized.4
Interventions that facilitate a total dose reduction in analgesic andsedative medications,e.g. theuse of nurse
controlled protocol guided sedation, the combination of spontaneousawakeningandbreathingtrialsandtheuseof shortactingmedicationsareassociatedwithimproved out-comessuchasdecreasedtimeofmechanicalventilationand ICUlengthofstay.5---7
Recently,eightnewbedsidescoringsystemstomonitor sedationhavebeendevelopedandtestedprimarilyfor reli-abilityandvalidity.Thechoiceofasedationscalemeasuring level of consciousness could be made among the Ram-saySedationScale,theRichmondAgitationSedationScale (RASS) and the Adaptation tothe Intensive Care Environ-ment Scale-ATICE.4In fact,randomizedcontrolled studies areneededtoassessthepotentialsuperiorityofonescale withrespecttoothers’scales,includingevaluationof reli-abilityandcompliancetothescale.
WerevisedandprospectivelytestedtheRamsaySedation Scale(RSS)forinterraterreliabilityandcompareditwiththe RikerSedation-AgitationScale(SAS)andtheRichmond Agi-tationSedationScale(RASS)totestconstructvalidityduring midazolam-remifentanilsedation.
Methods
Thisstudywasaprospectiveandopen-labeltrialapproved by the Research Ethics Committee of Ministry of Health OkmeydanıResearch&TeachingHospitalinIstanbul,Turkey. The trial was conducted in the 19 bed capacity ICU of the above-mentioned hospital. Ninety-two patients were included in the study, carried out over a period of time betweenMarch1standApril30th2015.75%ofthepatients were provided with mechanical ventilation by Pressure Control-PressureSupportventilation(PC/PSV)mode.
Inclusioncriteria
The patients at the age of 18 years or over, requiring mechanicalventilationandsedation.
Exlusioncriteria
The patients under the age of 18 years; patients having neuromuscular disease; patients receiving neuromuscular blockers;patientswithaknownorsuspectedallergyor intol-erance to midazolam, remifentanil; patients died during thestudyperiod;patientsusingtoxicsubstances;alcoholic patients;patientssuspectedofbeingpregnant;patientswho aremoribund(i.e.,classifiedasASAgradeVaccordingtothe AmericanSocietyofAnesthesiologists).
Remifentanil and midazolam were used for analgesia andsedationofmechanicallyventilatedpatientswhowere admittedtotheICUfollowingmajornoncardiacsurgeryor who had tobe ventilated due to respiratory failure. The remifentanil infusion wasstarted with0.15g.kg−1.min−1
andadaptedinstepsof0.05g.kg−1.min−1accordingto
clin-icalneeds.In caseofsufficientpainreliefbutinadequate sedation,patientscouldreceivebolusdosesofmidazolam (1---3mg)oraninfusionofmidazolam(0.1mg.kg−1.h−1).
After admission tothe ICU, the depthof sedation was adjusted to a Ramsay score level of 4 (sleeping patient, immediatelyarousable)andthentargetedatalevelof2---3 (patientawake,co-operativeandtranquilorrespondingto commandonly).Aftertheprotocolwasinitiated,daily inter-ruptionofanalgesiaandsedationwasperformed.Oncethis dailyinterruptionprocedurewascompleted,thedosagesof opioidanalgesicsandsedativewereadjustedinaccordance withthepatients’needs,asdescribedabove.
Measurementsandrecords
We tested each scale (SAS,RSS, and RASS) for interrater reliabilityandforvalidity,bycorrelationsbetweenthem.All scaleswereappliedto92patientsbythreedifferentcritical careteammembers(nurse,seniorcriticalcarephysicianand criticalcareresident).
Atotalof276scoreswereavailablefromeachscale. Thepatients’demographicdataandmedicalhistory,and also details of their physical examination, were recorded beforestarting sedationand analgesia therapy.APACHE II scorewererecordedinordertoassess theseverityof the patients’ condition. Unless specified, the scores of RSS,
RASSandSAS(inordertoassessthesedationquality)were recorded.
Statisticalanalysis
Atotal92patientswererequired.Sample sizecalculation wasbased on the study of Thuong et al.4 The study was estimatedat95%confidenceintervalandp=0.05.
All the variables are expressed as mean±SD. Corre-lation coefficients were calculated using Spearman rank correlationanalysis.A valueof p<0.05wasconsidered as statisticallysignificant.
Results
ThestudywasconductedbetweenMarch1standApril30th 2015 with total 92 cases including 50 men (54.3% of the participats) and 42 women (45.7% of the particitants) at Ministryof Health OkmeydanıResearch& Teaching Hospi-talinIstanbul,Turkey.Theagesofparticipantsrangedfrom 18to89withanaverageageof61.32±18.68years.Their APACHEvalues varied between 3 and 39 withan average of13.27±7.86.75% ofthe caseswere appliedmechanical ventilation(Table1).
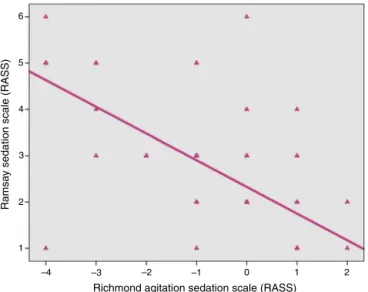
WhenassessingRamsaySedationScore,Richmond Seda-tion Agitation Scale and Sedation-Agitation Scale results of the study participants, their distribution percent is seen (Tables 2 and 3; Figs. 1---3). A negative directional (decreasedRSSvaluebyincreasingRASSvalue)66.4% rela-tionship between Richmond Sedation Agitation Scale and RamsaySedationScoreofthecasesjoinedtothestudywas foundstatisticallysignificant(r=−0.664;p=0.001;p<0.01) (Table4,Fig.4).Apositivedirectional(increasedSASvalue byincreasingRASSvalue)56.5%relationshipbetween Rich-mondSedationAgitationScaleandSedation-AgitationScale results of the cases joined to the study was also statis-tically significant (r=0.565; p=0.001; p<0.01). Lastly, A
Table1 Baselinecharacteristicsofpatients.
Age(years)a 61.32±18.68(18---89)
Sex
Male,n(%) 50(54.3) Female,n(%) 42(45.7)
APACHEa 13.27±7.86(3---39)
Mechanicalventilation,n(%) 75
APACHE,Acutephysiologyandchronichealthevaluation. a Dataareshownasmediansandinterquartileranges.
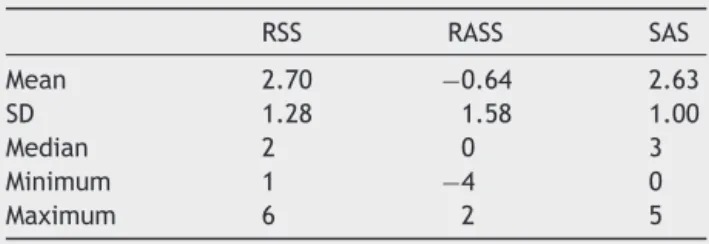
Table 2 The average distribution of RSS, RASS andSAS Scores.
RSS RASS SAS
Mean 2.70 −0.64 2.63
SD 1.28 1.58 1.00
Median 2 0 3
Minimum 1 −4 0
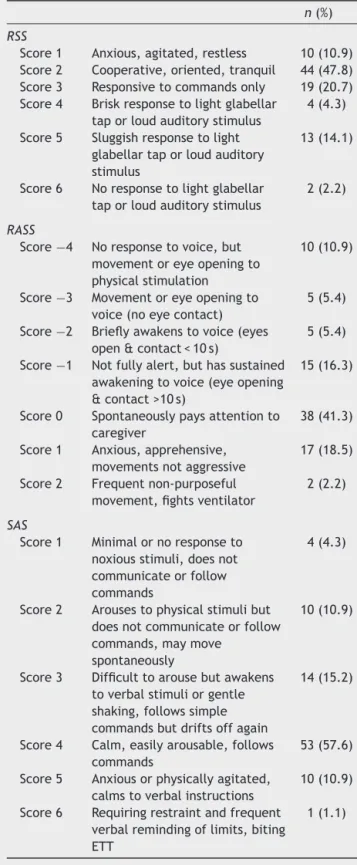
Table3 ThedistributionofRSS,RASSandSASscores.
n(%)
RSS
Score1 Anxious,agitated,restless 10(10.9) Score2 Cooperative,oriented,tranquil 44(47.8) Score3 Responsivetocommandsonly 19(20.7) Score4 Briskresponsetolightglabellar
taporloudauditorystimulus
4(4.3)
Score5 Sluggishresponsetolight glabellartaporloudauditory stimulus
13(14.1)
Score6 Noresponsetolightglabellar taporloudauditorystimulus
2(2.2)
RASS
Score−4 Noresponsetovoice,but movementoreyeopeningto physicalstimulation
10(10.9)
Score−3 Movementoreyeopeningto voice(noeyecontact)
5(5.4)
Score−2 Brieflyawakenstovoice(eyes open&contact<10s)
5(5.4)
Score−1 Notfullyalert,buthassustained awakeningtovoice(eyeopening &contact>10s)
15(16.3)
Score0 Spontaneouslypaysattentionto caregiver
38(41.3)
Score1 Anxious,apprehensive, movementsnotaggressive
17(18.5)
Score2 Frequentnon-purposeful movement,fightsventilator
2(2.2)
SAS
Score1 Minimalornoresponseto noxiousstimuli,doesnot communicateorfollow commands
4(4.3)
Score2 Arousestophysicalstimulibut doesnotcommunicateorfollow commands,maymove
spontaneously
10(10.9)
Score3 Difficulttoarousebutawakens toverbalstimuliorgentle shaking,followssimple commandsbutdriftsoffagain
14(15.2)
Score4 Calm,easilyarousable,follows commands
53(57.6)
Score5 Anxiousorphysicallyagitated, calmstoverbalinstructions
10(10.9)
Score6 Requiringrestraintandfrequent verbalremindingoflimits,biting ETT
1(1.1)
negativedirectional(decreasedSASvaluebyincreasingRASS value)65.6% relationship between Ramsay SedationScore and Sedation Agitation Scale results of the cases joined tothestudywasfoundstatisticallysignificant (r=−0.656; p=0.001; p<0.01) (Table 4, Fig. 5). The distribution of RichmondSedationAgitationScaleScoresandRamsay Seda-tion Scale Scores are shown in Table 5. The distribution
0 5
10.9
Score 1 Score 2Score 3
RSS
P
a
tients
, %
Ramsay sedation scale (RSS)
Score 4Score 5Score 6 47.8 20.7 4.3 14.1 2.2 10 15 20 25 30 35 40 45 50
Figure1 ThedistributionofRamsaySedationScale.
10.9 5.4 5.4 16.3 41.3 18.5 2.2
Score -4Score -3Score -2 Score -1
RASS
P
a
tients
, %
Richmond agitation sedation scale (RASS)
Score 0 Score 1 Score 2 0 10 20 30 40 50
Figure 2 The distribution of Richmond Agitation Sedation Scale. 0 4.3 10.9 15.2 57.6 10.9 1.1 10 20 30 40 50 60
Score 1 Score 2 Score 3
SAS
P
a
tients
, %
Sedation agitation scale (SAS)
Score 4 Score 5 Score 6
Figure3 ThedistributionofSedationAgitationScale.
Table4 ThecorrelationassessmentofRASS,RSSandSASscores.
RASS RSS SAS
r p r p r p
RASS --- --- −0.664 0.001a 0.565 0.001a
RSS −0.664 0.001a --- --- −0.656 0.001a
SAS 0.565 0.001a −0.656 0.001a ---
---r,Spearman’scorrelationcoefficient.
CorrelationasmeasuredbySpearmanrankcorrelationcoefficient. a p<0.01.
6
4 5
3
2
1
–4 –3 –2 –1 0 1 2
Richmond agitation sedation scale (RASS)
Ramsa
y sedation scale (RASS)
Figure4 CorrelationsbetweenRSSandRASS.
Discussion
In assessing agitation and sedation in adult ICU patients, Ramsay is both reliable (high interrater agreement) and valid(highcorrelationwiththeRASSandSASscales).
In orderto provide optimalcomfort and sedative drug therapyforpatientsinIntensiveCareUnit(ICU), establish-ing a goal of therapy often defined by a desired level of consciousness,withtitrationofmedicationstoachievethis targetisimportant.Anassessmentoftheconsciousnesslevel is bestperformed using a simple tool,such asa sedation
6
4 5
3
2
1
1 2 3 4 5 6
Ramsay sedation scale (RSS)
Sedation agitation scale (SAS)
Figure5 CorrelationsbetweenRSSandSAS.
scalethat reliesonobservation ofthe patienttoassigna levelofconsciousthatrangesfromalerttounarousable.8
With its easy titratability and organ-independent metabolism, remifentanil is an ideal agent for analgose-dation. In comparison with sedative-hypnotic regimens, remifentanil-basedregimens were associatedwithshorter duration of mechanical ventilation, more rapid weaning fromtheventilatorand,shorterICUlengthofstay.9
Foroptimalsedoanalgesia,sedationandanalgesiascales playsanimportantrolewithreferencetomechanical venti-lationandICUdischargetime.Bothaetal.demostratedthat
Table5 Cross-tabulationofRASSandRSSscoresinoverallpatientpopulation.
RASS Total
Score−4 Score−3 Score−2 Score−1 Score0 Score1 Score2
RSS
Score1 1 0 0 1 0 7 1 10
Score2 0 0 0 4 32 7 1 44
Score3 0 1 5 8 3 2 0 19
Score4 0 1 0 0 2 1 0 4
Score5 8 3 0 2 0 0 0 13
Score6 1 0 0 0 1 0 0 2
Table6 Cross-tabulationofRASSandSASscoresinoverallpatientpopulation.
RASS Total
Score−4 Score−3 Score−2 Score−1 Score0 Score1 Score2
SAS
Score1 4 0 0 0 0 0 0 4
Score2 5 2 0 1 0 2 0 10
Score3 0 1 2 9 0 1 1 14
Score4 0 1 3 5 37 7 0 53
Score5 0 1 0 0 1 7 1 10
Score6 1 0 0 0 0 0 0 1
Total 10 5 5 15 38 17 2 92
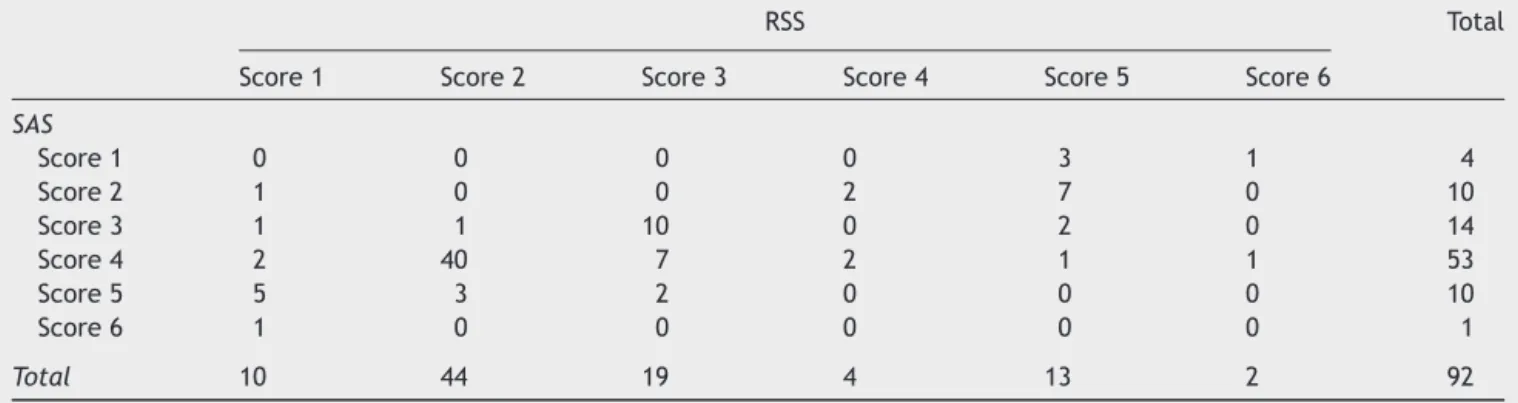
Table7 Cross-tabulationofRSSandSASscoresinoverallpatientpopulation.
RSS Total
Score1 Score2 Score3 Score4 Score5 Score6
SAS
Score1 0 0 0 0 3 1 4
Score2 1 0 0 2 7 0 10
Score3 1 1 10 0 2 0 14
Score4 2 40 7 2 1 1 53
Score5 5 3 2 0 0 0 10
Score6 1 0 0 0 0 0 1
Total 10 44 19 4 13 2 92
theintroductionofasedationscaleledtoareductioninthe durationofmechanicalventilation.6,10Breenetal. demon-stratedadecreaseinthedurationofmechanicalventilation whenusingremifentanil-basedanalgesiaandsedation.11
Implementationof sedation scales hasbeen related to improvedoutcomes,andfrequentassessmentofthelevelof consciousnessusingsedationscaleisstronglyrecommended inclinicalpracticeguidelines.8
Recentstudieshaveshownthat,analgesicsandsedatives medicationscanproduceadversepatientoutcomes. Inter-ventionsthatfacilitateatotaldose reductioninanalgesic andsedativemedications,e.g.,theuseofnursecontrolled protocolguidedsedation, thecombinationof spontaneous awakeningandbreathing trials,and theuse of short act-ingmedicationsarerelatedtoimproved outcomessuchas decreasedtimeofmechanicalventilationandICUlengthof stay.5
Amainobjectiveofeverymedicalsystemis toprovide a high-quality care in the Intensive Care Units (ICUs). In achievingthisgoal, nursesplay acrucialrole.One ofthe mostimportantresponsibilitiesofnursesissedationandpain controlofpatients.12
Usinga validatedobservational sedation-scoring toolis amethodtooptimizepatientsedation.Nevertheless,what theoptimal instrumentavailable isfor use in thisclinical contextisnotclear.Varndelletal.identifiedtotal27 obser-vational sedation-scoring instruments in their systematic literaturereview.TheRichmondAgitationandAssessment Scale was identified as the most suitable to be trialled prospectivelywithinanAustralianEmergencyDepartment.13
Since nurses are constantly in contact with the ICU patients,theirpracticeofasedationprotocolcanresultin bettersedationandpaincontrolinthepatients,thus reduc-ing the administered doses of sedatives and analgesics.12 Rikeretal.suggestedthat,SAS,oneofthesubjectivescales usedforassessmentofagitationandsedationinICUpatients is correlatedwithHarrisandRamsay scales.14 Khan etal. foundthatahighlevelofagreementbetweentheRASSand SASinidentifyingpatientseligiblefor deliriumassessment intheICU.15Inourstudy,RASSscoreof3or4wasnotseen inanypatientsinourtherapyperformedinaccordancewith oursedoanalgesiaprotocol.
Inordertomeasurethelevel ofconsciousness,a seda-tion scale could be chosen among the Ramsay sedation scale,theRichmondAgitationSedationscale(RASS)andthe AdaptationtoTheIntensiveCareEnvironmentscale-ATICE.4 Inourstudy,midazolam-inducedsedationwasassessedby validated RSS, RASS and, SAS. Riker et al. demonstrated goodvalidityandreliabilitywithSASandagoodcorrelation between theSASandtheRSS.Alsoinourstudy,a strong, negativecorrelation between RSSand RASSwas observed (r=−0.664; p=0.001; p<0.01), besides, we found posi-tivecorrelationbetweenRASSandSAS(r=0.565;p=0.001; p<0.01) and negative correlation between RSS and SAS (r=−0.656;p=0.001;p<0.01).
correlation(rs=0.98,p<0.001).NICSisavalidandreliable sedationscaleforuseinamixedpopulationofintensivecare unitpatients.NICSrankedhighestinnursingpreferenceand ease of communication,thus allowing more effective and interactivemanagementofsedation.
All scales demonstrated good interrater reliability and were comparable. RASS and SAS showed the best corre-lations and the bestagreement results in all professional categories.AllthesecharacteristicsmakeRASSandSASgood scalesfromthepointofvalidity,reliabilityandapplicability forbedsideevaluationofsedation-agitationincriticallyill patients.17
Despitenotbeingacommonpractice,sedationis recom-mendedtobeassessedroutinelyamongcriticallyillpatients sincelackofroutineassessmenthaspotentiallyharmful con-sequences.
Although more than two-third of the responding ICUs reported the use of sedation-and-pain-scales, assessment frequency was low, and objective assessment of pain in thenon-communicatingpatientswasextremelyrare. Sim-ilarly, the use of written procedure was low. The use of sedation-analgesia written procedure in an ICU seems stronglyinfluencedbyamoreglobalinvolvementoftheICU intheprotocolisationofcomplexcare.18
The positive effect of systematic evaluation of pain and agitation in ICUs has recently been demonstrated. Therefore,itisveryimportanttoroutinelyassesssedation in critically ill patients, and sedation-agitationscales are instrumentsthatallowtoachieveappropriatesedation.
Itisimportanttoemphasizethatthesescalesareusedto evaluatenotonlysedationlevelsbutalsoagitationlevels. Therefore,theyarecommonlyappliedtopatientswithout intubationin almost allvalidationstudies,and theyserve asscreeningtoolsforevaluatingdelirium.3Inourstudy,75% of thepatientswere intubated.BothSAS andRASSledto similarratesofdeliriumassessmentbyusingtheCAM-ICU.15 Amongsedationscales,theRamsayscaleisthemostused oneinICUpractice.Beingtheoldestscale,itisalsoonethe mostusedinclinicalstudies.Itisascalethatisableto iden-tifysomnolenceandagitationvisually.19Someauthorshave suggestedthatRamsay’ssedationlevelsarenotconclusive, however.Inourstudy,theRSSandRASSscaleshadthebest agreementamongtheobservers.Thesedata indicatethat RASSandSASareeasytoapplyatthebedside.Thesenewer scalesarealsoabletodefineagitationlevels.
ByusingawrittenstepwiseinstructionwiththeRamsay Scale,theinter-observerreliabilityofthelevelofsedation measurements,performedindailyclinicalpracticewithina largeteamofICnurses,provedtobealmostperfect.19Also inourstudy,RamsayScale,SASandRASSwerefoundtobe clinicallyapplicablebythenursesinICU.
Robinson etal.20 described and analyzed the develop-ment and psychometric properties of subjective sedation scales developed for critically ill adult patients. 36 arti-cleswerereviewedand11sedationscaleswereresearched forthestudy.Thescale developmentprocess, psychomet-ricproperties,feasibility, andimplementationof sedation scales wereanalyzed usinga 0---20 scoring system. In the study, Richmond Agitation-Sedation Scale (19.5) and the Sedation-Agitation Scale (19) demonstrated scores indi-cating ‘‘verygood’’ psychometric properties. Scores with ‘‘moderate’’ properties were the Vancouver Interaction
and Calmness Scale (14.3), Adaptation to the Intensive Care Environment (13.7), Ramsay Sedation Scale (13.2), Minnesota Sedation Assessment Tool (13), and the Nurs-ingInstrumentfor the Communicationof Sedation(12.8). Scaleswith‘‘low’’ properties included the MotorActivity Assessment Scale (11.5) and the Sedation Intensive Care Score (10.5). The New Sheffield Sedation Scale (8.5) and theObserver’sAssessmentofAlertness/SedationScale(3.7) demonstrated‘‘verylow’’publishedproperties.Onthe con-trary,inspiteofthreemonthstrainingprogrammeandusing astandardprotocolintheirstudy,Haddadetal.found dif-ferencesinSASscoreswhichwereaimedandthenobtained after.Thentheyemphasizedthatmoredelicateapproaches wererequiredfortitrationofsedation.21
Analgesics and sedatives are commonly prescribed in the ICU environment for patient comfort. Nevertheless, recentstudieshaveshownthatthesemedicationscan them-selvesleadtoadversepatientoutcomes.Interventionssuch as using nurse controlled protocol guided sedation and a specialized ICU team including physicians, nurses and pharmacists facilitate a total dose reduction in analgesic and sedative medications. Therefore, the clinical effect ofmedicinesmaximizesandtheriskoftreatment-induced adverseeventsminimizes.
In our study three different critical care team mem-bers(nurse,senior criticalcarephysicianandcriticalcare resident)assessedthreedifferentsedationscales simulta-neouslyandindependentlyfromeachother.Wetestedeach scalefor interrater reliabilityandfor validity, by correla-tionsbetweenthem.4
Conclusion
A strong correlation between RSS and RASS wasfound in thisstudywhich confirmsthevalueofthesemeasurement criteria.ThesetoolsshouldthereforebeutilizedbytheICU team toensure the patient is comfortable without being oversedated.
Fordailyinterruptionofsedonanalgesiathenadjustingit forpatient’sclinicalneedinICU,avoidingoversedationand minimizing the risk of treatment-induced adverse events, sedation scales should beeasy to use for ICU nurses and criticalcarephysicianandprovideaccuracyandsafety.
Asaresult,randomizedcontrolledstudiesareneededto assessthepotentialsuperiorityofonescalewithregardto otherscales,includingevaluationofthereliabilityandthe compliancetothescale.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.TallgrenM,PettiläV,HynninenM.Qualityassessmentof seda-tioninintensivecare.ActaAnaesthesiolScand.2006;50:942---6.
2.CostaMG,ChiarandiniP,RoccaGD.SedationinthecriticallyIll patient.TransplProc.2006;38:803---4.
4.Thuong M. Sedation and analgesia assessment tools in ICU patients.AnnFrAnesthReanim.2008;27:581---95.
5.McGrane S,PandharipandePP.Sedation intheintensive care unit.MinervaAnestesiol.2012;78:369---80.
6.KollefMH,LevyNT,AhrensTS,SchaiffR,PrenticeD,Sherman G.Theuseofcontinuousi.v.sedationisassociatedwith prolon-gationofmechanicalventilation.Chest.1998;114:541---8.
7.Brook AD, Ahrens TS, Schaiff R, et al. Effect of a nursing-implementedsedationprotocolonthedurationofmechanical ventilation.CritCareMed.1999;27:2609---15.
8.SesslerCN, RikerRR, RamsayMA. Evaluatingand monitoring sedation,arousal,andagitationintheICU.SeminRespirCrit CareMed.2013;34:169---78.
9.DevabhakthuniS,ArmahizerMJ,DastaJF,Kane-GillSL. Anal-gosedation: a paradigm shift inintensive care unit sedation practice.AnnPharmacother.2012;46:530---40.
10.BothaJA,MudholkarP.Theeffectofasedationscaleon ventila-tionhours,sedative,analgesicandinotropicuseinanintensive careunit.CritCareResus.2004;6:253---7.
11.BreenD,KarabinisA,MalnrainM,etal.Decreaseddurationof mechanicalventilationwhencomparinganalgesia-based seda-tionusingremifentanilwithstandarthypnotic-basedsedation forupto10daysinintensivecareunitpatients:arandomised, controlledtrial.CritCare.2005;9:200---10.
12.Abdar ME, Rafiei H, Abbaszade A, et al. Effects of nurses’ practiceofasedationprotocolonsedationandconsciousness levelsofpatientsonmechanicalventilation.IranJNurs Mid-wiferyRes.2013;18:391---5.
13.VarndellW, ElliottD,FryM. Thevalidity,reliability, respon-siveness and applicability of observation sedation-scoring
instruments for use with adult patients in the emergency department:a systematicliteraturereview.Aust EmergNurs J.2015;18:1---23.
14.RikerRR, PicardJT,FraserGL.Prospectiveevaluationofthe Sedation-Agitation Scale for adult critically ill patients. Crit CareMed.1999;27:1325---9.
15.KhanBA,GuzmanO,CampbellNL,etal.Comparisonand agree-mentbetweentheRichmondagitation-sedationscaleandthe Rikersedation-agitationscaleinevaluatingpatients’eligibility fordeliriumassessmentintheICU.Chest.2012;142:48---54.
16.MirskiMA,LeDrouxSN,LewinJJ3rd,ThompsonCB,MirskiKT, GriswoldM.Validityandreliabilityofanintuitiveonscious seda-tionscoringtool:thenursinginstrumentforthecommunication ofsedation.CritCareMed.2010;38:1674---84.
17.NassarJunior AP,Pires Neto RC, de Figueiredo WB, Park M. Validity,reliabilityandapplicabilityofPortugueseversionsof sedation-agitationscalesamongcriticallyillpatients.SaoPaulo MedJ.2008;126:215---9.
18.ConstantinJM,ChanquesG,DeJongheB,et al.Currentuse ofsedationandanalgesia:218resuscitationsinFranceservices practicessurvey.AnnFrAnesthReanim.2010;29:339---46.
19.vanDishoeckAM,vanderHooftT,SimoonsML,vanderEntM, ScholteopReimerWJ.Reliableassessmentofsedationlevelin routineclinicalpracticebyaddinganinstructiontotheRamsay Scale.EurJCardiovascNurs.2009;8:125---8.
20.RobinsonBR,BerubeM,BarrJ,RikerR,GélinasC.Psychometric analysisofsubjectivesedationscalesincriticallyilladults.Crit CareMed.2013;41:S16---29.