Artigo de Revisão Bibliográfica
Mestrado Integrado em Medicina
ENDOTHELIAL DYSFUNCTION AS A COMMON LINK BETWEEN
ERECTILE DYSFUNCTION AND METABOLIC SYNDROME
Blandina Miranda Coelho Gomes
Orientador: Dr. Nuno Louro
Instituto de Ciências Biomédicas de Abel Salazar
Largo Professor Abel Salazar, 2
4099-003 Porto
Endothelial Dysfunction as a Common Link Between Erectile Dysfunction and
Metabolic Syndrome
Blandina Miranda Coelho Gomes
Abstract
Introduction: Due to the increasing prevalence of obesity metabolic syndrome is considered the most important public health threat of the 21th century. Recently it was observed that this syndrome is associated with erectile dysfunction which affects up to 100 million men worldwide and is an important cause of decreased quality of life.
Purpose: The purpose of this review is to synthesize evidence concerning the connection of erectile dysfunction and metabolic syndrome. An overview will be given on the role of endothelium in the pathophysiology of erectile dysfunction and metabolic syndrome as well as the links between them. It will also be highlighted the importance of erectile dysfunction as a sentinel symptom in patients with occult cardiovascular disease.
Evidence synthesis: The basic mediator of penile erection is nitric oxide, so the deficiency of this mediator when there is an endothelial dysfunction can lead to erectile dysfunction. Endothelial dysfunction can be due to various risk factors namely the components of the metabolic syndrome which increase generation of reactive oxygen species then reducing vascular nitric oxide bioavailability. So the common link between erectile dysfunction and the metabolic syndrome is the endothelium dysfunction. Given the smaller diameter and the higher relative percentage of endothelial and smooth muscle cells in the penile arteries compared to other arteries such as the coronaries, erectile dysfunction is now seen as an early sign for cardiovascular diseases.
Conclusion: Pathologies like atherosclerosis, hypertension, diabetes mellitus, and erectile dysfunction are not disparate and require an integral approach. Erectile dysfunction rather than a disease in itself is a manifestation of pathologies of the biological systems involved in erectile function, so it can be looked at as a symptom of underlying disease, which might help diagnose early cardiovascular disease.
________________________________________________________________________
Keywords: erectile dysfunction, metabolic syndrome, endothelial dysfunction, cardiovascular disease,
Introduction
The metabolic syndrome (MS) is considered the most important public health threat of the 21st century (Taskinen, 2007), affecting between 10 to 15% of adult populations worldwide. This syndrome is characterized by a cluster of cardiovascular (CV) risk factors including central abdominal obesity, elevated triglycerides, reduced HDL-cholesterol, high blood pressure, increased fasting glucose and hyper-insulinemia. The higher prevalence of this syndrome in the occidental populations nowadays is mainly due to increasingly sedentary lifestyles and diets higher in saturated fats.
Erectile dysfunction (ED) is also a major concern, epidemiological data suggest that the prevalence of this pathology ranges between 16 and 52% depending on the patient population (Rosen RC et al, 2004) and affects up to 100 million men worldwide (Lue TF, 2000). Additionally it is an important cause of decreased quality of life (Litwin et al, 1998 and Laumann EO et al, 1999).
Recently it was observed that there is an association between ED and MS. Several studies stated a higher prevalence of ED in men with the MS (Esposito K et al, 2005, Demir T, 2006 and Bal K et al, 2007). This association has been target of increasing interest.
Current literature suggests that the common denominator of ED and MS is endothelial dysfunction (Esposito K et al, 2005). This connection may have an important impact in Public Health because erectile dysfunction appears to be one of the
earliest signs of systemic vascular disease and might be considered as an early marker for subclinical CV disease (Le NA, 2004) allowing preventive strategies.
Physiology of penile erection
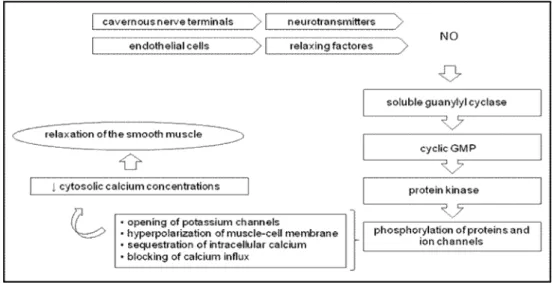
In order to fully understand the pathophysiology of ED as well as its relationship with MS and CV disease it seems useful to remember the basic mechanism of penile erection.Penile erection is a neurovascular event modulated by psychological and hormonal factors (Lue TF, 2000). On sexual stimulation, an increase in parasympathetic activity causes the release of neurotransmitters from the cavernous nerve terminals and of relaxing factors from the endothelial cells in the penis. Nitric Oxide (NO) is both the main neurotransmitter released from neural tissue supplying the corpora cavernosa and the main relaxing factor released from the endothelium. NO has a vasodilator action causing smooth muscle relaxation in the arteries and arterioles supplying the erectile tissue, leading to an increase in the penile blood flow. So NO is the key mediator of penile erection (Ignarro et al, 1990).
NO is synthesized by nitric oxide synthase from the amino acid L-arginine.
The main points of the NO mechanism of action at a molecular level are: NO enters the cavernosal smooth muscle cell and activates soluble guanylate cyclase, which promotes the formation of cyclic
guanosine monophosphate; through a cascade of events, cyclic guanosine monophosphate reduces intracellular calcium levels, causing relaxation of smooth muscle cells of the vasculature (Figure 1).
It is clear that the vascular endothelium of the penis plays a pivotal role in modulating vascular tone and blood flow into the penis. Thus, disturbances in the basic neurovascular event may be responsible for ED.
ED2: Erectile Dysfunction =
Endothelial Dysfunction
Erectile dysfunction was defined by the Consensus Development Panel on Impotence (1993) as the inability to achieve
and maintain an erection sufficient to permit satisfactory sexual intercourse. The etiology of ED is generally classified as psychological, physiological (neurogenic, hormonal, vascular, cavernosal, or drug induced), or mixed.
Vascular ED results from an impairment of endothelial dependent or independent smooth muscle relaxation, occlusion of cavernosal arteries by atherosclerosis or a combination of these.
Because the endothelium plays an important role in the penile arterial dilatation (endothelium dependent vasodilatation), its function is a key factor for erection. Thus the endothelial damage, and subsequent endothelial dysfunction, may cause ED if it
Figure 1 . Physiology of penile erection.
NO is released during a nonadrenergic noncholinergic neurotransmission and from the endothelium. Within the muscle NO activates a soluble guanylyl cyclase, which raises the intracellular concentration of cyclic guanosine monophosphat (GMP). Cyclic GMP in turn activates a specific protein kinase, which phosphorylates certain proteins and ion channels, resulting in the opening of potassium channels and hyperpolarization of muscle-cell membrane, sequestration of intracellular calcium by the endoplasmatic reticulum, and blocking of calcium influx by the inhibition of calcium channels. The consequence is a drop in cytosolic calcium concentrations and relaxation of the smooth muscle.
involves the penile vascular structures. This has led to the often quoted statement: “erectile dysfunction equals endothelial dysfunction (ED2)” (Guay A, 2007). There are various factors that can lead to endothelial damage, like hypertension, diabetes, dyslipidaemia, smoking, MS (Fonseca V,
Jawa A, 2005), etc. The underlying
mechanism of the risk factor-induced endothelial dysfunction is 1) a NO deficiency due to impaired production (Sullivan ME et al, 1999), or increased degradation by reactive oxygen species which interfere with NO pathway and are also toxic for the endothelium (Jones RW et al, 2002); or 2) an increased endothelial thickness climaxing in atherosclerosis and in a symptomatic vascular disease based on vascular stenosis (Creager MA et al, 1990, Panza JA et al, 1990, Meredith IT et al, 1996 and Kloner RA, 2003). So, as Muller A. (2006) pointed out on his review endothelial dysfunction is a central etiologic factor in the development of atherosclerosis and systemic vascular disease, which includes ED.
The small diameter of the cavernosal arteries and the high content of endothelium and smooth muscle (compared with other organs) may make the penis, as a vascular organ, very sensitive to changes in oxidative stress and systemic NO levels. Functional
vascular erectile dysfunction, as an
impairment of endothelial-dependent or
independent smooth muscle relaxation,
occurs before the development of structural, occlusive penile arterial disease. Vascular damages, caused by the above-mentioned risk factors, lead to endothelial dysfunction,
which is the first step for atherosclerotic lesions and the consecutive loss of vascular regulation (Kirby M et al, 2001 and Maas R et al, 2002). Atherosclerotic changes may cause
luminal obstruction leading to erectile
dysfunction, because a certain arterial inflow within the corpora cavernosa is needed to obtain a rigid erection.
Tamler R and Bar-Charma N (2008) successfully compiled in their review the various methods than can be used to access the endothelial function. These include: 1) serum markers like endothelin-1, interleucine 6, both not widely available, and CPR which can be false positive in inflammation and infection; 2) cellular markers like circulating endothelial progenitor cells, active if there is an endothelial damage but also not widely available; 3) intima media thickness of the carotid artery measured by ultrasonography, which has been firmly correlated with ED (Bocchio M et al, 2005) but is operator dependent; and 4) physiological markers as flow mediated dilatation of brachial artery, which is the gold standard but is also
operator dependent. In this last method an
arterial occlusion is made with a blood pressure cuff for 5 minutes and the subsequent release leads to reactive hyperemia and local endothelial activation. When this is performed on the patient’s arm, increased shear stress leads to endothelium-dependent dilation of the brachial artery, which can be measured and quantified by ultrasound. The results can then be contrasted to endothelium independent dilation provoked by administration of nitroglycerin. Chiurlia and colleagues (2005)
demonstrated a worsened flow mediated dilatation in men with ED without CV disease compared to men without ED. The findings of Kaiser et al (2004) are in accordance with these.
Low grade subclinical inflammation also affects endothelial function as it is involved in all stages of the atherosclerotic
process from the initial phase of increased
endothelial permeability up to the formation of the mature atherosclerotic plaque and plaque rupture (Valance P et al 1997, Libby P et al 2002 and Singh U, Jialal I 2006). The normal anti-inflammatory properties of the endothelium are impaired in the presence of inflammatory conditions and increased oxidative stress (Treplers T et al, 2006). Increased production of reactive oxygen species (such as superoxide and peroxynitrite) in subjects with CV risk factors decrease bioavailability of nitric oxide (NO) and may lead to ED. Several studies (Sullivan et al 2001, Giugliano F et al 2004 and Esposito K et al 2005) show that presence and severity of ED are associated with markers and mediators of endothelial dysfunction and subclinical inflammation, like high-sensitivity PCR. Measurement of inflammatory markers may be important given the role of inflammation for the rupture of unstable plaques. In their study Bank et al (2003) wrote that it is possible that CRP may be one mechanism contributing to vascular dysfunction in patients with ED or, alternatively, ED may be the first sign of systemic vascular disease, and PCR is elevated in response.
Metabolic syndrome
The MS, also known as syndrome X or the insulin resistance syndrome, is a common metabolic disorder that results from the increasing prevalence of obesity. As Eckel R and colleagues (2005) said, the metabolic syndrome is the master of disguise since it can present in various ways according to the different components that constitute the syndrome. It includes a cluster of metabolic and CV risk factors: glucose intolerance (type 2 diabetes, impaired glucose intolerance or impaired fasting glucose), insulin resistance, central obesity, dyslipidaemia and hypertension, which help to identify individuals at high risk for type 2 diabetes, CV diseases (Liese AD
,
1998) and ED (Corona G et al, 2006). For that reason Yassin A. et al (2008) stated that the MS is not a disease itself but is rather a pathway to disease. Sattar N and colleagues (2003) concluded that men with MS had a 3.7-fold increased risk of CV events and, more strikingly, a 24.5-fold increased risk of incident diabetes.The MS abnormalities co-occur in an individual more often that might be expected by chance but there is a debate in literature whether combining these components has an added diagnostic or prognostic value.
At least four definitions were proposed for the MS however the most used are the National Cholesterol Education Program’s Adult Treatment Panel III (NCEP-ATP III) definition (Executive summary of the third report of NCEP, 2001) and the International Diabetes Foundation definition (2004). They agree on the essential components – glucose intolerance, obesity, hypertension and dyslipedaemia - but differ in the detail and criteria (Table 1).
Although the IDF criteria identified a higher number of subjects with MS, its effectiveness in detecting individuals at high risk for diabetes, CV disease and ED is still controversial when compared with the NCEP-ATP III criteria (Katzmarzyk PT et al 2006 and Corona G et al, 2007). Eckel and colleagues consider that the NCEP-ATP III definition was simpler for clinical practice.
The most accepted and unifying hypothesis to explain the pathophysiology of MS is insulin resistance. In a few words, abdominal obesity promotes insulin resistance, decreasing peripheral utilization of glucose and fatty acid, thus leading to type 2 diabetes. Insulin resistance, the associated
hyperinsulinemia and hyperglycemia can lead to an abnormal lipid profile, hypertension, and vascular inflammation, all of which promote the development of endothelial dysfunction and atherosclerosis. Eckel and colleagues exposed in detail how each component of the MS can be explained by insulin resistance. They also highlighted that the association of MS and inflammation is well documented and that PCR concentrations increased with increasing obesity.
The role of endothelial
dysfunction in the Metabolic
Syndrome
The MS components dyslipidaemia, hypertension and glucose intolerance or type 2 diabetes are well known CV risk factors and are all associated with impaired endothelial function. The mechanism by which these risk factors induce endothelial dysfunction and lead to events is not entirely defined.
Hyperglycemia may interfere with endothelial function and the NO pathway causing glycation of elastic fibers and failure
Table 1: comparion of MS definitions. FBG – Fasting Blood Glucose; T2DM- Type 2 Diabetes Melittus;
WC – Waist Circunference
MS component NCEP-ATP III (≥ 3 of 5) IDF (criteria number 2 plus 2 of
the other 4)
Hyperglycemia (mg/dL) FBG ≥ 110 or T2DM FBG ≥ 100 or T2DM
Abdominal waist perimeter (cm) WC ≥ 102 in men WC ≥ 88 in women
WC ≥ 94 in men WC ≥ 80 in women
Triglyceride (mg/dL) ≥ 150 ≥ 150
HDL cholesterol (mg/dL) ≤ 40 or medicated ≤ 40 or medicated
in smooth muscle relaxation, decrease in NO production (due to a decreased expression of endothelial NO synthase or reduced bioavailability of its cofactor), increase in NO deactivation, and increase in the NO synthase inhibitor (Matfin G et al, 2005). Hyperglycemia may additionally impair endothelial function by promoting release of free radicals, such as superoxide, which inactivates NO resulting in the production of peroxyinitrite, a potent oxidant that stimulates the production of vasoconstrictor prostanoids. Dyslipidaemia affects the endothelial function in more ways than one; although the
hallmark of the syndrome is
hypertriglyceridemia and low plasma HDL cholesterol concentration, there are qualitative changes in LDL cholesterol. These changes consist in smaller LDL particles that are more susceptible to oxidation and thus potentially more atherogenic. Small dense LDL particles permeate the arterial wall faster and bind more avidly to proteoglycans than larger LDL particles. Oxidized LDL cholesterol impairs endothelial relaxation, and the free radicals that are formed inactivate the most important vasodilator, NO.
It is well known that hypertension is one of the important risk factors for atherosclerosis-induced vascular damage (Feldman et al, 1994).
Given the above, patients with risk factors such as hypertension, insulin resistance and dyslipidaemia appear to have an increased generation of reactive oxygen species which reduces vascular NO bioavailability and promote cellular damage (Tomasian D, 2000). Hence, increased
oxidative stress is considered a major mechanism involved in the pathogenesis of risk factor-induced endothelial dysfunction (Cai H and Harrison DG, 2000). Some studies indicated that the risk to develop endothelial dysfunction increases with the number of risk factors present in an individual (Celermajer DS et al, 1994). The cluster of risk factors of the MS may have a greater impact on endothelial function than other risk factor combinations.
Endothelial dysfunction as a
common
link
between
Erectile
Dysfunction and Metabolic Syndrome
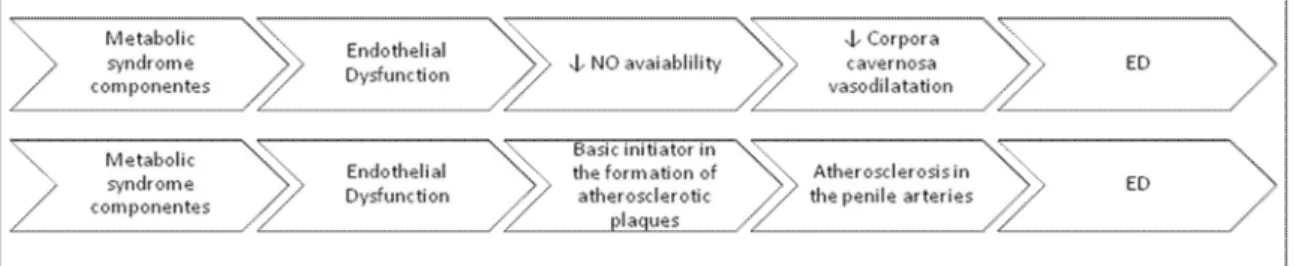
There is strong epidemiological evidence linking the risk of ED to the presence of well-recognized CV risk factors, such as the components of the MS (Sullivan ME et al, 2001). Demir (2006) demonstrated that ED was more prevalent and severe in men with MS, according to the NCEP-ATP III criteria, then in men without the syndrome, and also that the severity of ED is associated with an increasing number of MS components. But it is still not clear whether the risk of ED when all components of the MS are present is greater than the risk associated with each of its components independently.MS has a significant effect on the pathogenesis of ED because it plays a key role in the genesis of endothelial dysfunction, causing vascular deregulation and representing the initial step in the development of atherosclerosis (Heidler S et
al, 2006). This endothelial dysfunction is promoted by oxidative stress from the various risk factors. Hypertension is a known cause of vascular changes such as endothelial dysfunction and decreased NO formation, being a well recognized cause of ED. In the hyperlipidaemia, oxidized LDL impairs endothelial relaxation and the free radicals formed inactivate NO, the most important mediator of penile erection due to its vasodilator actions. In fact Kirby and colleagues (2005) wrote that the relative risk of ED increases 1,5 fold with hypertension and doubles with hyperlipidaemia. Hyperglycemia also interferes in NO pathway, as explained above.
Keeping in mind that vascular ED results from an impairment of vasodilatation, atherosclerosis or a combination of these it might be said that endothelial dysfunction is the initial process of the metabolic risk factor-induced ED (Figure 2).
Esposito and colleagues (2005) postulated an association between ED and MS because the components of the MS are risk factors for ED and are also characterized by abnormal endothelial function. The results of their study show that patients with the MS had an increased prevalence of ED, reduced endothelial function score and higher
circulating concentrations of PCR, compared with the control group.
In their study, Bal K et al (2008) stated that abdominal obesity combined with triglyceride level and HDL cholesterol levels synergistically increase the oxidative stress, which results in endothelial dysfunction and thus ED. They also concluded that, of the MS components, fasting blood glucose level, blood pressure and waist circumference, were the most effective risk factors in predicting the risk of ED. Demir´s results are in accordance with these, he wrote that for every 1 cm increase in waist circumference, the risk of ED increased by 5% and for every 1mg/dL increase in fasting blood glucose, ED risk increased 1%.
Additionally to the traditional risk factors, low grade inflammation might be present in both ED and MS and it can compromise their common denominator; however due to complex interrelationships, it is difficult to define exactly the causal pathway in these disorders.
Because ED is usually the first manifestation of endothelial dysfunction, it may provide a warning sign and, at the same time, an opportunity for early intervention in men otherwise considered at low risk for MS and subsequent CV disease.
Erectile Dysfunction, a sentinel
event for cardiovascular disease
It has been hypothesized that ED represents ‘‘the tip of the iceberg’’ of a systemic vascular disorder thus potentially preceding severe CV events (Montorosi P et al, 2003). ED could therefore serve as a sentinel event for CV diseases, such as coronary heart disease and stroke, both of which being leading causes of morbidity and mortality among adults in industrialized societies. The major advantage of ED as a sentinel event would be the fact that ED, in contrast to other risk factors, is easy to recognize, affects quality of life and therefore potentially drives at least part of patients to medical consultations with the possibility to modify risk factors.
ED and CV disease overlap in risk factors, pathological basis of disease and disease progression. The common underlying factor is endothelial dysfunction. Which is measured as impaired vasodilatation and is prognostic of CV events.
The obvious reason why ED may present before other signs of CVD is because penile artery diameter is smaller (1–2mm) than the coronary artery (3–4mm) or carotid artery (5–7mm), and the relative percentage of endothelial and smooth muscle cells is higher in the penile arteries, meaning that symptoms associated with atherosclerosis occur sooner in the penis (Montorsi F et al, 2003). The plaque size sufficient to cause ED, blocking blood flow through the penile artery, causes only 30–40% stenosis in arteries of greater diameter.
Several studies have demonstrated that CV assessment of men with ED enables early detection of CV disease. Montorsi and colleagues showed that ED presented before symptoms of CAD in 67% of men with a mean time interval of almost 3 years. Another study revealed that 45% of men with ED had previously undiagnosed hyperlipidaemia, 5% had undiagnosed diabetes and 7% had undiagnosed hypertension (Billups K and Friedrich S, 2000).
This provides justification for investigating patients with ED for other CV risk factors, symptoms or occult CV disease, and hence prevents significant morbidity and sometimes mortality. Therefore the ultimate goal is not only to treat the erectile problem but also to diagnose and aggressively treat any cardiac risk factors that may be found. This will not only correct ED in the short term but practice cardiac prevention in the long term. However, for the future, it will be important to perform studies in order to assess the sensitivity, specificity and cost-effectiveness of using ED as a marker for CV disease.
It should be stressed that the penis is not always the most susceptible organ to inflammatory and atherosclerotic changes, so although ED frequently precedes the onset of CV disease, a considerable proportion of patients have CV diseases without concomitant ED, proving that the clinical course of atherosclerosis is multifaceted and not fully predictable (Vlachopoulos C et al, 2007). Given that, if MS is found it should be treated not only to avoid ED but also to avoid the progression of arterial disease.
The stigma associated with ED prevents men for seeking help, so an emphasis in the strong relationship between this pathology and CV diseases could open the door to men to admit more freely having ED.
Baumgartner and colleagues (2008) developed a very interesting prospective study to evaluate the patients’ knowledge about risk factors for ED. They concluded that the knowledge was poor, that patients who had previously turned to their general practitioners were no better informed than those who hadn’t, that the most informed patients learned about the pathology on-line and had a higher educational background. This scenario is worrisome given the importance of ED as an early CV disease marker. Some solutions were proposed in their article such as increase sexual health education in medical school, improve doctors’ communication skills and have available questionnaires in the doctor’s office to help lower the patients threshold to address the issue.
MS is, as said before, a cluster of CV risk factors. So MS and ED are both predictive of CV disease being the common link between all of them the endothelial dysfunction.
Conclusion
Until a decade ago pathologies like atherosclerosis, hypertension, diabetes mellitus and ED were regarded as distinct diagnostic and therapeutic entities but today we know that these entities are not disparate and require an integral approach.
The MS accumulates many risk factors, all of which are implicated in causing endothelial dysfunction (Heidler S et al, 2006). The endothelial dysfunction involves not only central vascular structures, causing CV disease, but also peripheral vascular structures, like the penile artery (Maas R et al, 2002). This compromises the erectogenesis, resulting in erectile dysfunction. So rather than a disease in itself, ED is, particularly in elderly men who have enjoyed normal sexual function earlier in life, a manifestation of pathologies of the biological systems involved in erectile function (Shabsigh et al., 2005). Then, ED can be looked at as a symptom of underlying disease, which might help diagnose early CV disease. Thus the statement that “erectile dysfunction equals endothelial dysfunction (ED2)” may be upgraded to ED3: erectile dysfunction equals endothelial dysfunction equals early detection” (of cardiac disease) (Guay A, 2007).
Given that the MS is defined by a group of CV risk factors and that ED is becoming a more important marker for cardiac disease it might be intriguing to suggest that ED may become a part of the definition of the MS (Bansal T et al, 2005).
References
Bal K (2007). Prevalence of metabolic syndrome and its association with erectile dysfunction among urologic patients: metabolic backgrounds of erectile dysfunction. Urology; 69(2):356-60
Bank AJ, Billups KL, Kaiser DR, Kelly AS, Wetterlimg RA, Tsai MY and Hanson N (2003).Relation of C Reactive Protein nad other cardiovascular risk factors to penile vascular disease in men with erectile dysfunction. International Journal of Impotence Research; 15:231-236.
Bansal T, Guay A, Jacobson J, Woods B, Nesto R (2005). Incidence of metabolic syndrome and insulin resistance in a population with organic erectile dysfunction. J. Sex Medicine; 2: 96-103 Baumgartner MK, Hermanns T, Cohen A et al
(2008). Patients’ knowledge about risk factors for erectile dysfunction is poor. J Sex Med Billups K, Friedrich S (2000). Assessment of fasting
lipid profiles and Doppler ultrasound testing in men presenting with ED and no other medical problems. J Urol; 163: 147.
Bocchio M, Scarpelli P, Necozione S, Pelliccione F, Mhialca R, Spartera C et al (2005). Intima-media thickening of common carotid arteries is a risk factor for severe erectile dysfunction in men with vascular risk factors but no clinical evidence of atherosclerosis. J Urol; 173:526– 529.
Cai H, Harrison DG (2000). Endothelial dysfunction in cardiovascular diseases: the role of oxidant stress. Circ Res; 87:840–844.
Celermajer DS, Sorensen KE, Bull C, Robinson J, Deanfield JE (1994). Endothelium- dependent dilation in the systemic arteries of asymptomatic subjects relates to coronary risk factors and their interaction. J Am Coll Cardiol; 24:1468– 1474.
Chiurlia E, D’Amico R, Ratti C, Granata AR, Romagnoli R, Modena MG (2005). Subclinical coronary artery atherosclerosis in patients with erectile dysfunction. J Am Coll Cardiol; 46:1503–1506
Corona G, Mannucci E, et al (2006). Psyco-biologic correlates of the metabolic syndrome and associated sexual dysfunction. Eur Urol; 50:505-604.
Corona G, Mannucci E, et al (2007) A comparison of NCEP-ATPIII and IDF metabolic syndrome definitions with relation to metabolic syndrome-associated sexual dysfunction. J Sex Med;4:789–796.
Creager MA, Cooke JP, Mendelsohn ME, et al. (1990) Impaired vasodilatation of forearm
resistance vessels in hypercholesterolemic humans. J Clin Invest; 86:228–234.
Demir T (2006). Prevalence of erectile dysfunction in patients with metabolic syndrome. International Journal of Urology; 13: 385–388 Eckel RH, Grundy SM and Zimmet PZ (2005). The
metabolic syndrome. Lancet; 365:1415-28. Esposito K, Giugliano F, Martedi E, et al (2005).
High propotions of erectile dysfunction in men with the metabolic syndrome. Diabetes Care; 28 (5):1201-3.
Executive summary of the third report of National Cholesterol Education Program (NCEP) Expert Panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III) (2001). JAMA; 285:2486-97
Feldman HA, Goldstein I, Hatzichristou DG, Krane RJ, McKinlay JB (1994). Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging Study. J Urol; 151: 54–61.
Fonseca V, Jawa A (2005). Endothelial and erectile
dysfunction, diabetes mellitus, and the
metabolic syndrome: common pathways and treatments? Am J Cardiol; 96:13M–18M.
Giugliano F, Esposito K, Di Palo C, et al (2004). Erectile dysfunction associates with endothelial dysfunction and raised proinflammatory cytokine levels in obese men. J Endocrin Invest; 27:665–9.
Guay A (2007). ED2: erectile
dysfunction=endothelial dysfunction. Endocrinol Metabol Clin N Am; 36: 453-63
Heidler S, Temml C, Broessner C, Mock K, Rauchenwald M, Madersbacher S and Ponholzer A (2006). Is the metabolic syndrome an independent risk factor for erectile dysfunction? The journal of Urology; 177: 651-54
Ignarro LJ, Bush PA, Buga GM, Wood KS, Fukuto JM, Rajfer J. (1990). Nitric oxide and cyclic GMP formation upon electrical field stimulation cause relaxation of corpus cavernosum smooth
muscle. Biochem Biophys Res
Commun;170(2):843-50.
Jones RW, Rees RW, Minhas S, et al (2002). Oxygen free radicals and the penis. Expert Opin Pharmacother; 3:889–897
Kaiser DR, Billups K, Mason C, Wetterling R, Lundberg JL, Bank AJ (2004). Impaired brachial artery endothelium-dependent and -independent vasodilation in men with erectile dysfunction and no other clinical cardiovascular disease. J Am Coll Cardiol; 43:179–184.
Katzmarzyk PT, Janssen I, et al (2006). The importance of waist circumference in the definition of metabolic syndrome: Prospective
analyses of mortality in men. Diabetes Care;29:404–9.
Kirby M, Jackson G, Betteridge J, Friedli K (2001).
Is erectile dysfunction a marker for
cardiovascular disease? Int J Clin Pract; 55:614–618.
Kirby M, Jackson G, Simonsen U (2005).
Endothelial dysfunction links erectile
dysfunction to heart disease. Int J Clin Pract; 59(2):225-29
Kloner RA (2003). Erectile dysfunction in the cardiac patient. Curr Urol Rep; 4:466–471
Laumann EO, Paik A, Rosen RC (1999): Sexual dysfunction in the United States: prevalence and predictors. JAMA; 281:537– 544.
Le NA (2004). Inflammation, oxidative stress, and atherosclerosis. Curr Opin Lipidol;15:227-229.
Libby P, Ridker PM, Maseri (2002) A. Inflammation and atherosclerosis. Circulation; 105:1135–43. Liese AD, Mayer-Davis EJ, Haffner SM (1998).
Development of the multiple metabolic syndrome: an epidemiologic perspective.
Epidemiol Rev; 20:157-172.
Litwin MS, Nied RJ, Dhanani N(1998). Healthrelated quality of life in men with erectile dysfunction J Gen Intern Med; 13:159–166.
Lue, T M (2000), Erectile dysfunction.The New England Journal of Medicine; 342(24):1802-13 Maas R, Schwedhelm E, Albsmeier J, Boger RH
(2002). The pathophysiology of erectile dysfunction related to endothelial dysfunction and mediators of vascular function. Vasc.Med; 7:213–25
Matfin, G., Jawa, A. and Fonseca, V. A (2005). Erectile dysfunction: interrelationship with the metabolic syndrome. Curr Diab Rep; 5: 64,
Meredith IT, Currie KE, Anderson TJ, et al (1996). Postischemic vasodilatation in human forearm is dependent on endothelium-derived nitric oxide. Am J Physiol; 270:H1435–H1440. Montorsi P, Montorsi F, Schulman CC (2003). Is
erectile dysfunction the ‘tip of the iceberg’ of a systemic vascular disorder? Eur Urol; 44:352– 354.
Muller A, Mulhall JP (2006). Cardiovascular disease, metabolic syndrome and erectile dysfunction. Andrology, sexual dysfunction and infertility; 16(6): 435–443
NIH Consensus Development Panel on Impotence (1993). NIH Consensus Conference: impotence. JAMA; 270:83-90
Panza JA, Quyyumi AA, Brush JE, Epstein SE
(1990). Abnormal endothelium-dependent
vascular relaxation in patients with essential hypertension. N Engl J Med; 332:22–27. Rosen RC, Fisher WA, Eardeley I, et al. (2004). The
multinational Mens's Attitudes to Life Events and Sexuality (MALES) Study: I. Prevalence of erectile dysfunction and related health concerns in the general population. Curr Med Res Opin; 20:607–617
Shabsigh R, Perelman MA, Lockhart DC, Lue TF, Broderick GA (2005) Health issues of men: prevalence and correlates of erectile dysfunction. J Urol; 174:662–67.
Singh U, Jialal I (2006). Oxidative stress and atherosclerosis. Pathophysiology; 13:129–42. Sullivan ME, Keoghane SR, and Miller MAV (2001).
Vascular risk factors for ED. BJU Int; 87: 838– 845,.
Sullivan ME, Miller MA, Bell CR, et al (2001). Fibrinogen, lipoprotein (a) and lipids in patients with erectile dysfunction. Int Angiol; 20:195–9. Sullivan ME, Thompson CS, Dashwood MR, et al.
(1999) Nitric oxide and penile erection: is erectile dysfunction another manifestation of vascular disease? Cardiovasc Res; 43:658–665 Tamler R, Bar-Chama N (2008). Assessment of endothelial function in the patient with erectile dysfunction: an opportunity for the urologist. Internationla Journal of Impotence Research; 20:370-377.
Taskinen MR (2007). Is metabolic syndrome the main threat to human health in the twenty-first century? Arterioscler Thromb Vasc Biol; 27: 2275.
Tomasian D, Keaney JF Jr, Vita JA (2000). Antioxidants and the bioactivity of endothelium-derived nitric oxide. Cardiovasc Res; 47:426– 435.
Trepels T, Zeiher A, Fichtlscherer S (2006). The endothelium and inflammation. Endothelium; 13:423–9.
Vallance P, Collier J, Bhagat K (1997). Infection, inflammation, and infarction: does acute endothelial dysfunction provide a link? Lancet; 349:1391–2.
Vlachopoulos C, Rokkas K, Ioakeimidis N and Stefanadis C (2007). Inflammation, Metabolic Syndrome, Erectile Dysfunction, and Coronary Artery Disease: Common Links. European Urology; 52:1590-1600
Yassin A.A, Saad F and Gooren L.J (2008). Metabolic syndrome, testosterone deficiency and erectile dysfunction never come alone. Andrologia; 40:250-64