www.jped.com.br
ORIGINAL
ARTICLE
Practices
related
to
late-onset
sepsis
in
very
low-birth
weight
preterm
infants
夽
Maria
Regina
Bentlin
a,∗,
Ligia
M.S.S.
Rugolo
a,
Ligia
S.L.
Ferrari
b,
on
behalf
of
the
Brazilian
Neonatal
Research
Network
(Rede
Brasileira
de
Pesquisas
Neonatais)
aHospitaldasClínicas,FaculdadedeMedicinadeBotucatu,UniversidadeEstadualPaulista(UNESP),Botucatu,SP,Brazil
bHospitalUniversitáriodeLondrina,UniversidadeEstadualdeLondrina(UEL),Londrina,PR,Brazil
Received6November2013;accepted2July2014 Availableonline6November2014
KEYWORDS Sepsis; Newborn; Premature; Handhygiene; Preventionand control
Abstract
Objective: Tounderstandthepracticesrelatedtolate-onsetsepsis(LOS)inthecentersofthe BrazilianNeonatalResearchNetwork,andtoproposestrategiestoreducetheincidenceofLOS. Methods: This was a cross-sectional descriptive multicenter study approved by the Ethics Committee. Three questionnaires regarding hand hygiene, vascular catheters, and diagno-sis/treatmentofLOSweresenttothecoordinatorofeachcenter.Thecenterwiththelowest incidenceofLOSwascomparedwiththeothers.
Results: All16centersansweredthequestionnaires.Regardinghandhygiene,87%use chlorhex-idine or70%alcohol;alcoholgel isused in100%; 80%use bedsidedispensers(50%hadone dispenserforeverytwobeds);practicaltrainingoccursin100%andtheoreticaltrainingin70% ofthecenters,and37%train onceayear.Catheters:94%haveaprotocol,and75%havea lineinsertion team.Diagnosis/treatment:complete bloodcount andbloodcultureareused in100%,PCRin87%,hematologicalscoresin75%;oxacillinandaminoglycosidesisthe empir-ical therapyin50% ofcenters.Characteristics ofthecenter withlowest incidenceofLOS: stricterhandhygiene;catheterinsertionandmaintenancegroups;useofbloodculture,PCR, andhematologicalscorefordiagnosis;empiricaltherapywithoxacillinandaminoglycoside. Conclusion: Theknowledgeofthepracticesofeachcenterallowedfor theidentificationof aspectstobeimprovedasastrategytoreduceLOS,including:alcoholgeluse,handhygiene training,implementationofcatheterteams,andwiseuseofantibiotictherapy.
©2013SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
夽
Pleasecitethisarticleas:BentlinMR,RugoloLM,FerrariLS,onbehalfoftheBrazilianNeonatalResearchNetwork(RedeBrasileirade PesquisasNeonatais).Practicesrelatedtolate-onsetsepsisinverylow-birthweightpreterminfants.JPediatr(RioJ).2015;91:168---74.
∗Correspondingauthor.
E-mail:[email protected](M.R.Bentlin). http://dx.doi.org/10.1016/j.jped.2014.07.004
PALAVRAS-CHAVE Sepse;
Recém-nascido; Prematuro; Higienedasmãos; Prevenc¸ão&controle
Práticasrelacionadasàsepsetardiaemprematurosdemuitobaixopeso
Resumo
Objetivo: Conheceraspráticasrelacionadasasepsetardia(ST)noscentrosdaRedeBrasileira dePesquisasNeonatais(RBPN)eproporestratégiasparareduc¸ãodaST.
Métodos: Estudotransversal, multicêntricoda RBPN, aprovado peloCEP.Três questionários sobrehigienizac¸ãodasmãos,cateteresvascularesediagnóstico/tratamentodaSTforam elab-oradoseenviadosaoscoordenadoresdecadacentro.OcentrocomamenorincidênciadeST foicomparadoaosdemais.
Resultados: Todosos 16 centrosresponderam aosquestionários. Quanto ahigienizac¸ãodas mãos:87%utilizamchlorhexidineouálcool70%;100%álcoolgel;almotolia/leitoem80%(50% dispõede1dispensadorparacada2leitos);Treinamentopráticoocorreem100%,teóricoem70% doscentrose37%treinam1vez/ano.Cateteres:94%temprotocoloparapassagem,75%grupo deinserc¸ão.Diagnóstico/tratamento:Hemogramaehemoculturasãoutilizadosem100%dos centros;PCRem87%;75%usamescoreshematológicos;oxacilinaeaminoglicosídeosãousados como terapiaempíricaem 50%doscentros.Característicasdocentrocommenorincidência deST:rigorosahigienizac¸ãodasmãos;gruposdeinserc¸ãoemanutenc¸ãodecateteres;usode hemocultura,PCReescoreshematológicosparadiagnósticodaST;tratamentoempíricocom oxacilinaeaminoglicosídeo.
Conclusões: Oconhecimentodaspráticasdecadacentropermitiuidentificaraspectosaserem otimizadoscomoestratégiaparaareduc¸ãodaSTincluindo:usodeálcoolgel,treinamentoem higienizac¸ãodasmãos,implantac¸ãodegruposdecatetereseusoracionaldeantibióticos. ©2013SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
Late-onset sepsis (LOS) is a major cause of neonatal morbidity and mortality. The World Health Organization (WHO) estimates thatof the fourmillion neonatal deaths worldwide per year, more than one-third are caused by severe infections, and one-quarter are due to neonatal sepsis/pneumonia.1,2InBrazil,theneonatalmortalityrate
represents 60% of infant mortality, and sepsis is a major
causeofneonataldeaths.3
Researchnetworksworldwidearededicatedtothestudy
of neonatal sepsis.The National Institute of Child Health
and Human Development (NICHD Neonatal Research
Net-work) documented a 21% incidence of LOS confirmed in
preterm infants weighing<1,500g, ranging from 10-38%
amongcenters.4IntheBrazilianNeonatalResearchNetwork
(BNRN),consistingof16referencecentersinthe
maternal-child health area, the LOS study group showed, in the
years2009-2010,50%incidenceofLOS(range29-72%among
centers)in preterm infants weighing<1,500g,with27.5%
confirmedLOS(unpublisheddata).
LOS is related to the postnatal environment,
charac-teristicsof thenewborn,andcare practices.Among these
practices,theuseofvascularcathetersandparenteral
nutri-tionareimportantriskfactorsforsepsis.5,6Handhygieneis
anotherpracticethatdeservesattention,asthe
transmis-sionof microorganismsthrough thecaregivers’ hands is a
constantconcern.TheCentersforDiseaseControland
Pre-vention(CDC),theWHO,andtheBrazilianNationalHealth
SurveillanceAgency(ANVISA)periodicallypublishguideson
handsanitizing,butwarnthattheadherenceofhealth
pro-fessionalsislow,evenincampaignperiods.7---9
The percentage of professionals’ adherence to hand
washingvariesfrom28%to62%,andgreateradherenceto
handhygienepracticesisassociatedwithreducedratesof
hospitalinfection.10Anotherrelevantaspectisthedifficulty
in the diagnosis of sepsis, as clinical data and laboratory
testsarenonspecificandbloodculture,consideredthegold
standard,haslow positivity.11,12 The difficultyin diagnosis
canleadtotreatmentdelayorexcessiveuseofantibiotics,
allowingtheselection of floraanddevelopmentof
bacte-rialresistance, anotherfrequent problem in the neonatal
intensivecareunit(NICU).
The scarcity of national data regarding LOS, together
withthefact thatNICUsthat arepart ofBNRNreference
units,makesit crucialtoanalyzethe current situationof
theBNRNNICUsanddisseminatedata,tomapthenational
scenario,andtoadviseonpreventivemeasurestobe
insti-tutedaiming toreduce the incidence of LOS in very low
birth weight premature infants. These aspects motivated
thisstudy,which aimedto identifycare practicesrelated
tolate-onset sepsis in16 BNRNcenters,focusingonhand
hygiene,useofvascularcatheters,diagnosis,empiric
treat-ment of sepsis, and identification of aspects that can be
improvedasastrategytoreduceLOS.
Method
presence of clinical and hematological alterations after 72hoursoflife,andLOSisconsideredconfirmedwhenthe bloodcultureispositiveandclinicalwhenthebloodculture isnegative.
In2011,theLOSstudygroupoftheBNRNcreatedandsent threequestionnairestothecoordinatorsofeachofthe16 centers,whichincludedopenandmultiplechoicequestions regardingcarepracticesusedintheirunits.These question-nairesaddressedissuesabouthandhygiene,useofvascular catheters,diagnosis,andempiricaltreatmentofLOS.
Themainissuesaddressedinthequestionnairewere:
Questionnaire1:Handhygiene
Productusedinhandhygiene,specificinformationaboutthe useofalcoholgelandtrainingofhealthstaffthatcaresfor newborns.
Questionnaire2:Vascularcatheters
Presenceofgroupsofcatheterinsertionandmaintenance, catheter insertion protocol, length of stay, sending the cathetertipfor culture,andinformationondressingsand infusionsystemchanges.
Questionnaire3:DiagnosisandtreatmentofLOS
Testsusedforthediagnosis ofLOS:bloodculture (periph-eral and/or central method used for its implementation, interpretation of results taking into account time and growthcurve),useofblood count,acutephasereactants, hematologicalscores,CSFcollectionindicationsandrepeat lumbarpuncture,andinterpretationofgrowthof coagulase-negativestaphylococciin blood culture (contaminationor infection).Mostcommonlyusedantibioticsinantimicrobial therapyanddurationofuse.
Statistical
Analysis
Afterreceivingtheresponses,theyweretabulatedand ana-lyzedusing frequency and association tables,maintaining theconfidentialityofthecenters,whichwereidentifiedonly byletters.ThepracticesoftheBNRNcenterwiththe low-estincidenceofST,includingclinicalandconfirmedsepsis (incidenceof29%-unpublisheddata)werecomparedwith theothers.Basedonthesedata,suggestionsweremadefor LOSreduction.
Results
The16participatingBNRNcentersansweredthethree ques-tionnaires.No question wasexcluded and thepercentage wascalculatedbased onthenumber of answersobtained foreachquestion.
Questionnaire1:Handhygiene(Table1)
Mostcentersusechlorhexidineorandalcohol70%forhand hygiene,andhavealcoholgelbedsidedispensers.However,
regarding the use of dispensers, only seven centershave dispensers at theappropriateproportion(≥ 0.5per bed). The16centerscarryoutpracticaltrainingforhandhygiene; however,only25%conducttrainingmorethantwiceayear.
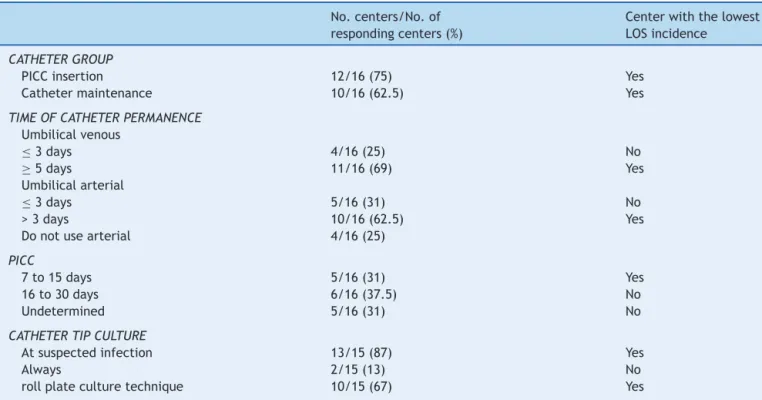
Questionnaire2:Vascularcatheters(Table2)
All centers,except one,use catheterinsertion protocols, but only 12 centershave PICC (peripherally-inserted cen-tralcatheter)insertiongroups,consistingofnurses,andten centershavecathetermaintenancegroups.Inmostcenters, theumbilicalvenouscatheterismaintainedforaperiod≥ fivedays,thearterialcatheterforthreetosixdays,andthe PICCforupto30days.Allcentersusetransparentdressings; 56%changethedressingsonlyiftheyaresoiled.Most cen-ters requestcathetertipcultureifinfection issuspected. Allcenterswithdrawthecatheterimmediatelyinthe pres-enceofbloodculturepositiveforfungi,56%inthepresence of Gram-negative bacteriaor S. aureus, and12.5% in the presenceofcoagulase-negativestaphylococci.
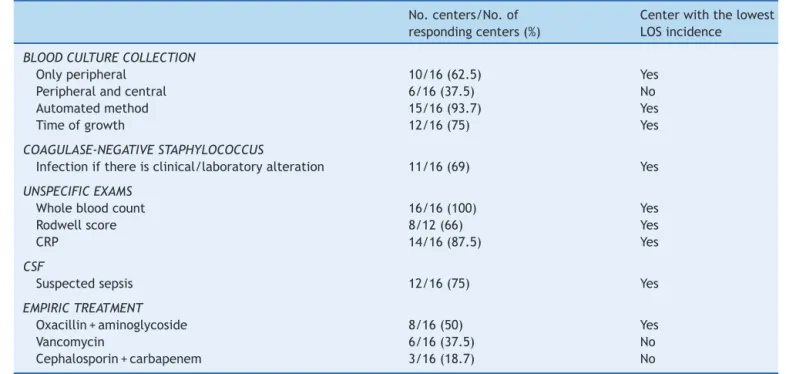
Questionnaire3:Diagnosisandempirictreatment ofLOS(Table3)
All centers collect blood culture samples before starting antibiotictherapy; 15 ofthem usethe automated culture methodandmostcollectperipheralbloodonly.
In 11 centers, coagulase-negative staphylococci are consideredtheetiologicalagentofinfectionifthereis asso-ciatedclinical andlaboratory alteration;12 centers(75%) takeintoaccountthetimeofbacterialgrowthfordiagnosis ofinfection.
Asfornonspecifictests,mostcentersuseC-reactive pro-tein (CRP) asthe acute-phase reactant and consider this markerusefulbothfor excludingthediagnosisofinfection and for infection control.Hematologic scores areused in mostcenters,especiallytheRodwellscore.Fivecentersdid notrepeat thenonspecifictests for suspectedinfectionif theinitialtestwasnormal.ThevastmajorityperformedCSF collectioninsuspectedinfectionandrepeatedthetestifthe resultofthefirstCSFwasabnormal.Onlyhalfofthecenters useoxacillinandaminoglycosideasinitialempiricregimen inLOSand50%oftheservicesmaintainthetreatmentuntil negativeculturesareobtained.
Practicesinthecenterwiththelowestincidence ofLOS
The center withthe lowestincidence of LOS(29%) in the period2009-2010showedthefollowingresults:
- Handhygiene(Table1):useschlorhexidine2%andalcohol
70%; alcohol geldispensers at the bedside and one
dis-penserfortwobeds;trainstheentirehealthteamtwice
ayearthroughpracticalactivitiesandleaflets.
- Vascularcatheters(Table2):hascatheterinsertion
proto-colandcatheterinsertionandmaintenancegroup;keeps
theumbilical venous catheterfor upto fivedays,
arte-rialcatheterforuptosevendays,andPICCforupto15
Table1 Mainquestionnaireanswersonhandhygienein16BrazilianNeonatalResearchNetworkcentersandpracticesinthe centerwiththelowestincidenceoflate-onsetsepsis(LOS).
No.ofcenters/No.of respondingcenters(%)
Centerwiththelowest LOSincidence
PRODUCTUSED
Chlorhexidine 12/15(80) Yes
Alcohol70% 11/14(79) Yes
Iodine-basedantiseptic 2/13(15) No
USEOFGELALCOHOL
Dispenser/bed 13/16(81) Yes
Dispenser/professionals 3/16(19) No
Dispenser/bed≤1:2 7/14(50) Yes
Dispenser/bed1:3to1:7 7/14(50) No
TRAINING
Practical 16/16(100) Yes
Theoretical 11/16(69) No
Leaflets 10/16(62) Yes
HeadofHICC 14/16(87) Yes
FREQUENCYOFTRAINING
Onceayear 6/16(37.5) No
Twotimesayear 5/16(31) Yes
≥3timesayear 4/16(25) No
HICC,HospitalInfectionControlCommission.
every seven days, collects catheter tip culture in sus-pectedinfection,usestherollplateculture,andremoves thecatheterimmediatelyifblood cultureispositivefor fungi.
- DiagnosisandempirictreatmentofLOS(Table3):
col-lects peripheral blood culture, has automated method
available,usesgrowthtimetodifferentiateinfectionand
contamination, considers coagulase-negative
staphylo-cocci as pathogen if there are clinical and laboratory
alterations. Nonspecific tests include blood count and
CRP,takingRodwellscoreintoaccount.Usesoxacillinand
aminoglycosideasempirictherapyforLOS.
Table2 Mainquestionnaireanswersonvascularcatheteruseinthe16BrazilianNetworkonNeonatalResearchcentersand practicesinthecenterwiththelowestincidenceoflate-onsetsepsis(LOS).
No.centers/No.of respondingcenters(%)
Centerwiththelowest LOSincidence
CATHETERGROUP
PICCinsertion 12/16(75) Yes
Cathetermaintenance 10/16(62.5) Yes
TIMEOFCATHETERPERMANENCE Umbilicalvenous
≤3days 4/16(25) No
≥5days 11/16(69) Yes
Umbilicalarterial
≤3days 5/16(31) No
>3days 10/16(62.5) Yes
Donotusearterial 4/16(25)
PICC
7to15days 5/16(31) Yes
16to30days 6/16(37.5) No
Undetermined 5/16(31) No
CATHETERTIPCULTURE
Atsuspectedinfection 13/15(87) Yes
Always 2/15(13) No
rollplateculturetechnique 10/15(67) Yes
Table3 Mainquestionnaireanswersondiagnosisandempiricaltreatmentoflateonsetsepsis(LOS)inthe16BrazilianNetwork onNeonatalResearchcentersandpracticesinthecenterwiththelowestincidenceofLOS.
No.centers/No.of respondingcenters(%)
Centerwiththelowest LOSincidence
BLOODCULTURECOLLECTION
Onlyperipheral 10/16(62.5) Yes
Peripheralandcentral 6/16(37.5) No
Automatedmethod 15/16(93.7) Yes
Timeofgrowth 12/16(75) Yes
COAGULASE-NEGATIVESTAPHYLOCOCCUS
Infectionifthereisclinical/laboratoryalteration 11/16(69) Yes
UNSPECIFICEXAMS
Wholebloodcount 16/16(100) Yes
Rodwellscore 8/12(66) Yes
CRP 14/16(87.5) Yes
CSF
Suspectedsepsis 12/16(75) Yes
EMPIRICTREATMENT
Oxacillin+aminoglycoside 8/16(50) Yes
Vancomycin 6/16(37.5) No
Cephalosporin+carbapenem 3/16(18.7) No
CRP,C-reactiveprotein;CSF,cerebrospinalfluid.
Discussion
Neonatalinfectionsurveillancenetworkshavebeen imple-mented in many countries, aiming to verify the national scenario,comparetheresultswithothernetworks,and pro-posestrategiestoimprovethequalityof careprovidedto newborns. In the centers of the BNRN, all contribute to the maintenance of a database on very low birth weight prematureinfants, which allows monitoring of morbidity, care practices, and mortality rates. One of the priority-monitoringmorbiditiesintheBNRNisLOS.13
LOSiscommoninprematureinfants,isassociatedwith
highmorbidityandmortality,andmayimpairthe
neurode-velopment of survivors.14 A BNRN study showed that 27%
ofverylowbirthweightprematureinfantsdeveloped
con-firmedLOS(range14-51%)and23%(range7.5-41%)clinical
LOS(unpublisheddata).Themortalityinsepticgroupswas
higherwhen compared tothe group without sepsis, even
consideringthevariabilitybetweencenters.Thegreat
vari-ability in infection rates between centers is a common
findingin researchnetworksanddifferencesincare
prac-ticeshavebeenidentifiedintheliteratureasacontributing
factor.15---18 Knowing the care-related practices is critical
in developing strategies to reduce LOS. Interventions to
improvecarepracticescanattenuatethesedifferences.
Hand hygieneis a practice that arouses greatconcern
andshouldalwaysbemonitored.Themainproductsusedfor
handwashingarealcohols(concentrationof70%,no
resid-ualeffect)andchlorhexidine(concentrationsof2%and4%,
witha residual effectof 6hours).10,19 In the BNRN, most
centers use chlorhexidine and alcohol 70%, have alcohol
geldispensers,andhavehandhygienetraining.Thisshows
thatthebasicitemsareavailable;whatprobablymakesthe
differencebetween thecentersis thequalityin practice,
reinforcingthehypothesisthatthemostimportantfactoris
toinvestincontinuingeducationofhealthprofessionalsto
improveadherencetorecommendedprocedures.One
pur-poseofthisstudyistoexpandtheuseofalcoholgel,which
ispreferredbyprofessionalsduetobeingeasytouse,
tak-inglesstimetouseandhavingcomparableefficacytoother
antiseptics,providedthehandsarenotsoiled.10,20
Anotherriskfactor monitoredinthisstudywastheuse
of vascular catheters. Central catheters are widely used
in verylow birth weightprematureinfants for parenteral
nutrition infusion, medication, and antibiotic
administra-tion,andcanbeasourceofinfection:contaminationduring
the insertion, excessive manipulation, interruption in the
closedsystemmaintenanceforadministrationofdrugsand
bloodproducts,useofcontaminatedsolution,thehubitself,
or contaminationbyskin pathogens.5,21,22 Datafromseven
Brazilian NICUsshowedthattheincidenceof bloodstream
infectionassociatedwithvascularcathetervariesby birth
weight:34.9/1,000vascularcatheter(VC)daysinpremature
infantsweighing<1,000g,20.4/1,000VCdaysinpremature
infantsweighingbetween1,001-1,500g,17.3/1,000VCdays
inthoseweighingbetween1,501-2,500gand,18.1/1,000VC
daysininfantsweighing>2,500g.23
These rates are much higher than those found in the
National Healthcare SafetyNetwork (NHSN), which shows
rates of 4.4/1,000 VC days in those weighing<1,000g,
4.8/1,000 VC days between 1,001-1,500g, 4.2/1,000 VC
days between 1,501-2,500g. and 3.1/1,000 VC days in
those weighing>2,500g, and reinforce the importance of
catheter-associated infection in thisenvironment and the
need for preventive measures against this condition of
concern.5,24,25
In the questionnaire on vascular catheters, it was
insertionandmaintenanceteam,withthisrepresentingan
aspecttobeimproved,whichcanbecrucialasaLOS
pre-ventionstrategy.Theothercathetercareprocedureswere
similarbetweencenters.
Inthethirdandlastquestionnaireondiagnosisand
empir-icaltreatmentofsepsis,theanswerswerevariable,showing
greatheterogeneitybetweencenters.Allcentersuseblood
count, CRP, and blood culture, but do not follow a
pro-tocol. Premature newborns are immunocompromised and
exposed to many infectious risk situations that favor the
useofantibiotics.Anotheraspectthatrequiresthefrequent
use of antibiotics is thedifficulty in thediagnosis of
sep-sis, due tothe low specificity of clinical assessment and
laboratorytests,aswellasthelowpositivityofblood
cul-tures,whichhavebeenclassicallyreportedinliterature.14
Antibiotictherapy,inturn,alterstheintestinalflora,which
favorstheemergenceofresistantstrains.26---28Theproposed
strategywastooptimizetheinterpretationofbloodcount,
takinghematologicalscoresintoaccount,suchasthe
Rod-wellscore,andassociatetheuseofserialquantitativePCR
forexclusionandinfectioncontrol.
Empirical antibiotic therapy is among the items with
greatervariabilitybetweencenters.Inordertodefine
pro-tocolsontheempiricaluseofantibiotics,itisnecessaryto
knowtheprevalentagentsineachunit,butitisknownthat
the use of broad-spectrum antibiotics increases
coloniza-tionandinfectionwithmultidrug-resistantorganisms.27The
presenceofcoagulase-negativestaphylococciasoneofthe
mainLOSagentsintheBNRN(60%ofcases)mayhavefavored
theuse of vancomycininthe empirictherapy.The useof
antibiotics,aswellastimeofuse,mustbestrictlymonitored
andreassessed,andempiricaltherapywithbroad-spectrum
antibioticsshouldbeavoided.27,28
Once the diagnosis of infection is ruled out, these
antibioticsshouldbediscontinuedimmediately, andifthe
presenceoftheagentisconfirmedinbloodorothersterile
fluids,gradualantimicrobialdosingdecreaseshouldalways
beperformed.
ThecenterwiththelowestincidenceofLOSshowedno
extraordinary or costly practices to justify its results. In
general,thepracticesbetweencentersweresimilar,which
reinforces the hypothesis that the difference lies in the
qualityof adherencetopractices andthecommitmentof
theentirestaffinvolvedinthecareofthenewbornswhen
applyingthem.
Thedifferencesfoundinthe16BNRNcentersreflectwhat
occursinacountryofcontinentaldimensionssuchasBrazil
anddepictsthecurrentreality.Thefactthatthesecenters
havecometogetherwiththegoalofreducingLOS,making
adiagnosisofthecurrentsituation,identifyingthecenters
withthelowestincidencesandbestpractices,andaimingto
improvetheirperformancejustifiestheworkoftheBNRN’s
studygrouponsepsis.Basedonthesedata,asetofmeasures
hasbeenproposedaimedatreducingLOS:
- Institutethe useof alcohol gel/glycerin dispensers at a
rateofoneforeverybedintheNICU.
- When usingalcoholgel walldispensers, maintaina
pro-portionofatleastonedispenserfortwobeds.
- Perform theoretical and practical training for hand
hygienemorethantwiceayear,fortheentirehealthcare
team.
- Havestandardized procedures forinsertion and
mainte-nanceofPICCs.
- HaveateamassignedtoperformPICCinsertionand
main-tenance.
- Carry outregular(monthly)meetingswiththeInfection
ControlCommitteetomonitorinfectionrates.
- Ensuretheadequacyofhumanresources(physiciansand
nurses) proportionper bed accordingto current
recom-mendations.
- Periodically assess the results attained at the unit in
reducingsepsisandinstituteseveralmeansof
disseminat-ingthisanalysis:meetings,bulletinboards,andelectronic
messages.
Low-costmeasuressuchasthoseproposedbytheBNRN
canhavehighimpactandmakeadifferenceinsepsis
pre-vention, decreasing the length of hospital stay, reducing
thesocialandeconomiccosts,andgeneratinganexpected
improvementinthequalityofcareofverylowbirthweight
prematureinfantsintheBNRNcenters.
Onelimitationofthestudyliesinthefactthatthe
ques-tionnaire was not sent to doctors and nurses that work
shifts,buttothecoordinators ofthecenters,whichwere
responsiblefor the information. Despite the possibilityof
individualizedbehaviors, therewasa commitmentonthe
partofthecoordinatorstoanswerthequestionsaccording
totheserviceprotocolsandaftercheckingtheinformation
withtheirteams.Anotherlimitationwasthelackofdataon
thesensitivitypatternsforsepsisagentsineachunit,sothat
theevaluationoftheempiricaltherapycouldbedetailed.
Onemust also considerthat theaim of this study was
toevaluatecarepracticesrelatedtosepsisandnot
investi-gateriskfactorsforLOS.Therefore,thecharacteristicsof
thepopulationtreatedat eachcenter werenotanalyzed,
whichlimitsdatainterpretation,butdoesnotinterferewith
thestudy’sproposalregardingLOSpreventionmeasures,as
thecharacteristics of thetreated population arenot
pre-ventable, whereasimproving care practicescan minimize
theriskofLOS.
Themajorcontributionofthestudywastodemonstrate
theconductofclinicalpracticeinreferencecentersinBrazil
andshowthat,eveninthesecenters,practicesandroutine
procedurescanbeimproved.
In conclusion, the knowledge of the practices in each
centerallowedfortheidentificationofaspectstobe
opti-mizedasastrategytoreduceLOSincluding:useofalcohol
gel,traininginhand hygiene, implementationof catheter
groups,andtherationaluseofantibiotics.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Appendix
A.
Supplementary
data
References
1.Stoll BJ, Hansen N, Fanaroff AA, Wright LL, Carlo WA, EhrenkranzRA,etal.Late-onsetsepsisinverylowbirthweight neonates:theexperienceoftheNICHDneonatalresearch net-work.Pediatrics.2002;110:285---91.
2.QaziSA,StollBJ.Amajorglobalpublichealthchallenge.Pediatr InfectDisJ.2009;28:S1---2.
3.Brasil (Datasus). Ministério da Saúde Informac¸ões de saúde---Estatísticas vitais. [cited 11 Jun 2012]. Available fromhttp://tabnet.datasus.gov.br
4.Stoll BJ, Hansen N. Infections in VLBW infants: studies fromtheNICHDNeonatalResearchNetwork.SeminPerinatol. 2003;27:293---301.
5.RichtmannR.Prevenc¸ãodeinfecc¸ãorelacionadaàassistênciaa saúde(IRAS).Catetervascularcentraleperiférico.In:APECIH. Diagnósticoeprevenc¸ãodeIRASemNeonatologia,2nded.São Paulo:EditoraAnvisa;2011.p.157---74.
6.Hodge D, Puntis JW. Diagnosis, prevention, and manage-ment of catheter related bloodstream infection during long termparenteral nutrition. Arch DisChild FetalNeonatal Ed. 2002;87:F21---4.
7.Center for Disease Control. Guideline for hand hygiene in health care settings: recommendations of the Healthcare InfectionControl Practices AdvisoryCommittee andthe HIC-PAC/SHEA/APIC/IDSAHandHygieneTaskForce.MMWRRecomm RepAtlanta.2002;51:1---145.
8.World Health Organization The WHO Guidelines on Hand HygieneinHealthCare.Globalpatientsafetychallenge 2005-2006: clean care is safer care. Geneva: WHO Press; 2006 [cited 27 Sep 2012]. Available from: http://www.who.int/ patientsafety/informationcentre/ghhaddownloadlink/en/. 9.Brasil (ANVISA). Higienizac¸ão das mãos em servic¸os de
saúde. Brasília; 2007. [cited 27 Sep 2012]. Available from: http://www.anvisa.gov.br/hotsite/higienizacao maos
10.FerrazS.Higienizac¸ãodasmãos.In:In:APECIH.Diagnósticoe prevenc¸ãodeIRASemNeonatologia.2nded.SãoPaulo:Editora Anvisa;2011.p.225---38.
11.Rodwell R, Leslie Al Tudehope D. Early diagnosis of neona-tal sepsis using a hematologic scoring system. J Pediatr. 1988;112:761---7.
12.Mussi-PinhataM,NascimentoSD.Infecc¸õesneonatais hospita-lares.JPediatr(RioJ).2001;77:S81---96.
13.Rede Brasileira de Pesquisas Neonatais. Infecc¸ão tardia (sepsetardia).Recomendac¸ões.[cited20Jul2013].Available from: http://www.redeneonatal.fiocruz.br/images/stories/ relatorios/infeccaotardia.pdf
14.BentlinMR,RugoloLMSS.Lateonsetsepsis:epidemiology, eval-uationandoutcome.NeoReviews.2010;11:e426---35.
15.AlyH,HersonV,DuncanA,HerrJ,BenderJ,PatelK,etal.Is bloodstreaminfectionpreventableamongprematureinfants.A taleoftwocitiesPediatrics.2005;115:1513---8.
16.AzizK,McMillanDD,AndrewsW, PendrayM,QiuZ,Karuri S, etal.Variationsinratesofnosocomialinfectionamong Cana-dianneonatalintensivecareunitsmaybepractice-related.BMC Pediatr.2005;5:22.
17.VandenHoogenA,GerardsLJ,Verboon-MaciolekMA,FleerA, KredietTG. Longtermtrendsin theepidemiologyof neona-talsepsisandantibioticssusceptibilityofcauseactiveagents. Neonatology.2010;97:22---8.
18.SchulmanJ,StricofR,StevensTP,HorganM,GaseK,Holzman IR,etal.StatewideNICUcentral-line-associatedbloodstream infectionratesdeclineafterbundlesandchecklists.Pediatrics. 2011;127:436---44.
19.KilbrideHW,PowersR,WirtschafterDD,SheehanMB,Charsha DS,LaCorteM,etal.Evaluationanddevelopmentofpotentially betterpracticesto preventneonatalnosocomialbacteremia. Pediatrics.2003;111:e504---18.
20.WorldHealthOrganizationGuidelinesonhandhygieneinhealth care.In:WHO.TheWHOGuidelinesonHandHygieneinHealth Care. WHOPress; 2009[Cited 23Jul 2013]. Available from: http://whqlibdoc.who.int/publications/2009/9789241597906
eng.pdf.
21.DowneyLC,SmithPB,BenjaminDKJr.Riskfactorsand preven-tionoflate-onsetsepsisinprematureinfants.EarlyHumDev. 2010;86:S7---12.
22.Kawagoe JY, Segre CA, Pereira CR, Cardoso MF, Silva CV, FukushimaJ.Riskfactorsfornosocomialinfectionsincritically illnewborns: a 5year prospectivecohortstudy.AmJInfect Control.2001;29:109---14.
23.Pessoa-Silva CL, Richtmann R, Calil R, Santos RM, Costa ML, Frota AC, et al. Healthcare-associated infections among neonates in Brazil. Infect Control Hosp Epidemiol. 2004;25:772---7.
24.National Nosocomial Infections Surveillance (NNIS) System Report.DatasummaryfromJanuary1992through2003,issued August2003.AmJInfectControl.2003;31:481---98.
25.Romanelli RM, Anchieta LM, Mourão MV, Campos FA, Loy-ola FC, Mourão PH, et al. Risk factors and lethality of laboratory-confirmed bloodstream infection caused by non-skin contaminant pathogens in neonates. J Pediatr (RioJ). 2013;89:189---96.
26.Isaacs D. Unnatural selection: reducing antibiotic resis-tance in neonatal units. Arch Dis Child Fetal Neonatal Ed. 2006;91:F72---4.
27.LeJ,NguyenT,OkamotoM,McKamyLiebermanJM.Impactof empiricantibioticuseondevelopmentofinfectionscausedby extended-spectrum-lactamasebacteriainaNeonatalIntensive CareUnit.PediatrInfectDisJ.2008;27:314---8.