www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Correlation
between
presence
of
Leishmania
RNA
virus
1
and
clinical
characteristics
of
nasal
mucosal
leishmaniosis
夽
,
夽夽
Marcos
Massayuki
Ito
a,∗,
Lilian
Motta
Catanhêde
b,
Tony
Hiroshi
Katsuragawa
c,
Cipriano
Ferreira
da
Silva
Junior
a,
Luis
Marcelo
Aranha
Camargo
d,
Ricardo
de
Godoi
Mattos
b,
Juan
Miguel
Vilallobos-Salcedo
b,c,daHealthScience,UniversidadeFederaldeRondônia(UNIR),PortoVelho,RO,Brazil bFundac¸ãoOsvaldoCruz(FIOCRUZ),PortoVelho,RO,Brazil
cUniversidadeFederaldeRondônia(UNIR),PortoVelho,RO,Brazil dUniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil
Received21July2014;accepted23September2014 Availableonline22July2015
KEYWORDS
Leishmaniosis mucocutaneous; Leishmaniosis; Leishmania braziliensis; Leishmania guyanensis; Leishmaniavirus
Abstract
Introduction:Mucosalleishmaniosis(ML)isasevereclinical formofleishmaniosis.Complex factorsrelated to theparasite andthehost areattributed tothedevelopment ofmucosal lesions. LeishmaniaRNA virus1(LRV1)candisruptimmune response,andmay bethe main determinantofseverityofthedisease;itshouldbeinvestigated.
Objective: To study the existence of clinical differences between patients with ML with endosymbiosisbyLRV1and.thosewithoutit.
Methods:A cross-sectional cohortstudy withclinicalevaluation, polymerasechain reaction (PCR)detectionofLeishmania,speciesclassification,andsearchofLRV1wasperformed.Only patientswithconfirmeddiagnosisofMLbypositivePCRandwithnasalmucosainjurieswere includedinthisanalysis.
Results:Outof37patients,30(81.1%)werediagnosedwithLeishmaniabraziliensis,five(13.5%) with Leishmania guyanensis, and two (5.4%) withmixed infection ofL. braziliensis andL. guyanensis.LVR1viruswaspresentin26(70.3%)ofthecases.
夽 Pleasecitethisarticleas:ItoMM,CatanhêdeLM,KatsuragawaTH,daSilvaJuniorCF,AranhaCamargoLM,MattosRG,etal.
Corre-lationbetweenpresenceofLeishmaniaRNAvirus1andclinicalcharacteristicsofnasalmucosalleishmaniosis.BrazJOtorhinolaryngol. 2015;81:533---40.
夽夽Institution:UniversidadeFederaldeRondônia(UNIR),PortoVelho,RO,Brazil. ∗Correspondingauthor.
E-mail:[email protected](M.M.Ito).
http://dx.doi.org/10.1016/j.bjorl.2015.07.014
Conclusion:CorrelationbetweenclinicalphenotypeandpresenceofLRV1wasnotobserved, althoughthefrequencyofthevirusistwo-foldhigherinmucosallesionsthanthatfoundinthe literatureonskinlesionsinthesamegeographicalarea.
© 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Leishmaniose mucocutânea; Leishmaniose; Leishmania braziliensis; Leishmania guyanensis; Leishmaniavírus
Correlac¸ãoentreapresenc¸adeLeishmaniaRNAVírus1eascaracterísticasclínicas daleishmaniosedemucosanasal
Resumo
Introduc¸ão:Aleishmaniosedemucosa(LM)éumaformaclínicagravedaleishmaniose.Fatores complexosligadosaoparasitaeaohospedeirosãoatribuídosao desenvolvimentodaslesões demucosa.Leishmania RNAVírus1(LRV1)podesubverterarespostaimune,podendosero principaldeterminantedagravidadedadoenc¸aedeveserpesquisado.
Objetivo:Estudaraexistênciadediferenc¸asclínicasentrepacientesportadores deLMcom endosimbioseporLRV1easquenãopossuem.
Método: Foi realizado um estudo decoorte históricacom cortetransversal com avaliac¸ão clínica,detecc¸ãodaLeishmania portécnicade PCR,classificac¸ãodaespécieepesquisade LRV1.Foramincluídosnaanálisedapesquisasomenteospacientescomdiagnósticoconfirmado deLMcomPCRpositivo,comlesãodemucosanasal.Resultados:Dos37 pacientes,30 (81,1%) foramdiagnosticadoscomL.braziliensis,5(13,5%)comL.guyanensise2(5,4%)cominfecc¸ão mistadeL.braziliensiseL.guyanensis.OvírusLVR1estavapresenteem26 casos(70,3%).
Conclusão:A correlac¸ão entreofenótipo clínico eapresenc¸a doLRV1 não foi constatada, porémafrequênciadovíruséduasvezesmaioremlesãodemucosadoqueencontrado em trabalho,damesmaregião,sobrelesãocutânea.
©2015Associac¸ãoBrasileira deOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicadopor ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Leishmaniosisisaneglectedtropicaldiseasethatislargely ignored in the discussion of important tropical diseases. Contributing to this neglect are a complex epidemiology, ecology, lack of simple management tools, and a lack of data.1 In2010,theWorldHealthOrganization(WHO)
esti-mated there were1 19,600 cases of American cutaneous
leishmaniosis (ACL) in Brazil; they employed a 2.8---4.6
fold underreporting grade that is considered mild.1 Vega
etal. calculated the actual per capita cost (medical and
non-medical expenditure)of cutaneous leishmaniosis (CL)
treatmentinColombiatobeUS$345.Projectingthesame
costtoBrazil,themeanexpenditureforACLwouldbeUS$
7,586,490 per year for new cases.The estimated cost of
yearsoflifelosttodisease(DALY-WHO)perpatientin
Colom-biawasUS$ 15,000.2Ifonly mucosalleishmaniosis(ML) is
considered,treatmentandDALYcostswouldbemuchhigher.
Mucosal leishmaniosis (ML) is an important and severe
clinicalformofleishmaniosis,duetothedestructive
poten-tial of its injuries. ML is caused by a protozoan of the
genus Leishmania that features an extranuclear DNA and
a mitochondrial organelle, the kinetoplast. ML has two
developmental forms during its life cycle: amastigote,
which is a mandatory intracellular parasite in
verte-brates,andpromastigote, existingin invertebratevectors
(phlebotomines).3
Thereareindications that leishmaniosis maybenative
totheAmazonregion.TheSpanishchroniclerPedroPizarro
reportedthatpeoplelivinginhotvalleysofPeruwere
dec-imatedbyanosediseaseontheAmazonside.TheAndean
theory, formulated by Rabello, has its origin from
Peru-vianhuacos(piecesofpre-Columbianceramics)discovered,
depictingpeoplewithnosedeformities.Basedon
epidemi-ological studies of Leishmania braziliensis, Marzochi and
Marzochi proposed that leishmaniosis hasits origin in the
westernAmazon.4,5
Leishmaniaaredividedintotwosubgenera,Vianniaand
Leishmania. In Brazil, at least seven species that cause
disease arerecognized;cutaneous leishmaniosis iscaused
mainly by L.(V.) braziliensis, Leishmania(V.) guyanensis,
andL.(L.)amazonensis,and,morerarely,byL.(V.)laisoni,
L.(V.) naiffi, L.(V.) shawi,and L.(V.) lindenbergi,all of
interest tothe Amazonregion.The firstthreespeciesare
involved in mucosalleishmaniosis, while L. (L.) chagasi is
the causalagent of visceral disease.3,6---8 L. braziliensis is
themaincauseofML;however,arecentlypublishedstudy
revealed significant prevalence of L. guyanensis, mainly
northoftheAmazonriver.9L.amazonensismayalsocause
ML.3 Nocase of MLby L.(V.)panamensiswasreportedin
Brazil.
MLcanmanifest itselfwithnasalobstruction,epistaxis
associatedwithcrustproduction,rhinorrhea,andmildpain.
mucosa hyperemia, presence of nodules, and subsequent
formation ofa granulomatous lesion,which can evolveto
septalperforation,nasaledemawithskinthickening,nasal
septumcollapse (tapirnose), andbulkynasal pyramid.8,10
Morethan90%ofmucosalinjuriesaffectonlytheanterior
nasalseptum.8,9,11This conditioncanseverelycompromise
thenose,palate,gums,pharynx,andlarynx,causing
defor-mities that impairphonation, breathing, swallowing, and
self-esteem.8,10,11
Factors related to the parasite, host, and magnitude
of the immune response are relevant to mucosal
dam-age.Metastasesoftheparasitetotheupperaerodigestive
tract mucosa can occur through lymphatic or
hematoge-nous routes.3,8,12 The development of mucosal injuries
is attributed to complex and poorly understood factors
(socioeconomic,environmental,andthoseofthehost and
parasite).Mucosallesionsbycontiguitymayalsooccur.3,8
A common pathway for ML development is associated
with a lasting immune response of the host against the
parasite, with increases in inflammatory mediators, such
asTNF-␣,CXCL10,andCCL4,andinT-cell-mediated
cyto-toxicityactivity; higher numbers of CD4+ and CD8+ cells,
increases in IFN␥, IL-2 and IL-5, lower production of
IL-1013-15, and also polymorphism of the genes encoding
inflammatorymediators,suchasTNF-␣andIL-6.3,13,14,15
Type1helper(Th1)Tcellsproducelymphokinesthat
acti-vate macrophages (IL-2, IFN-␥, TNF-␣, and IL-12)tofight
these parasites. Type 2 helper (Th2) T cells produce
IL-4 and IL-10, which inhibit macrophages, leaving the host
susceptible to infection. Leishmania is able to facilitate
the differentiation of T cells into a Th2-type response,
characterized by persistent infection.14,16,17 The parasite
must adapt its metabolism to the intracellular oxidative
stressintothe phagolysosomeof macrophages.16
Paradox-ically,MLischaracterizedbyanexaggerationinresponseto
Leishmaniaantigensandbyascarcityofparasites.The
exag-gerationinTh1responsecausesdestructionof softtissues
wheretheantigenicparticlesarelocated.14,18,19
Recently, Ives et al. demonstratedthat the parasitism
of Leishmania by the Leishmania RNA virus 1 (LRV1), a
double-strandedRNAvirusofTotviridaefamily,increasesthe
concentrationofcytokinesandchemokines(TNF-␣,CXCL10,
CCL5,IL-6)inTLR3/TRIF-mediatedmacrophagesofL.
guya-nensisclones. Inthisstudy therewasahigh potentialfor
metastasisinguineapigs, indicatingthatthenucleicacids
oftheendosymbioticvirusfunctionasstrongimmunogens,
andcausedestructivemucosalinflammation.13,16 Although
research on LRV1 has been conducted since the original
description of the virus 20 yearsago, therole of LRV1in
leishmaniosisremainsunknown.Nomajorstudieswere
pub-lishedontheimpactofthevirusuntilthepublicationofthe
studybyIvesetal.
InthephylogeneticstudyofLRV,withthesoleexception
ofonestrainofL.majorinfectedwithLeishmaniaRNAvirus
2(LRV2)fromaskinlesioninformerSovietUnion,allLRV
strainshavetheirorigininSouthAmerica.Intheassessment
ofthegeneticevolutionamongLRVtypesandamong
Leish-maniaspeciesinfectedwiththeseviruses,thereisevidence
ofaparallelismintheevolutionofLeishmaniaandLRV.19,20
The model suggests that innate recognition of LRV1
occursin the first hoursof infection. Viral dsRNA release
occursfromdeadparasites;then theparticlebindstothe
Toll-like receptor 3 (TLR3) and triggers the inflammatory
cascadethataggravatesthedisease,perhapsrepresenting
themaindeterminantofitsseverity.21Thus,thedetection
of LRVcan have clinical importance, guiding therapy and
prognosis.13,16,19,21
DespitethedetectionofLRV1inlargemetastaticstrains
ofL.braziliensisandL.guyanensis,metastasesmayoccur
in its absence.19,22 LRV discovery as an innate
immuno-gen,changingthecourseofleishmaniosis,shouldmotivate
further research on such viral hyperpathogens in other
infections.19
The methods routinely used in the diagnosis of
cuta-neousleishmaniosis arelimitedfor mucosallesions.8,9,11,12
Montenegro’sreactionisnotsuitablebecausethemucosal
injuriestypicallyoccur secondary tocutaneouslesions.In
theselesions,thelowparasitaemiasignificantlyreducesthe
diagnostic accuracy of biopsy, aswell asthe direct
eval-uation with smears obtained from injuries.8,12,23 The low
level of antibodies reduces the effectiveness of
serologi-caltests.11,23Withmaterialcollectedfrommucosallesions,
identificationunderopticalmicroscopyorbyculturerarely
issuccessful.24 Polymerasechainreaction(PCR)standsout
asan excellent test (i.e. gold standard),12 becauseof its
sensitivity and specificity, especially to establish parasite
species24andalsotodetectLRV1.22,25
GiventherelevantresearchonLRV1conductedbyIves13
onthe definition of the mucosal leishmaniosis phenotype
inmice, and alsoconsidering alsoscarcity of information
on the presence of this virus and clinical manifestations
inpatients,it wasdecidedtostudy theexistence of
clin-icaldifferencesin patients with ML withor without LRV1
endosymbiosis. We hope that this will contribute to the
continuingeducationprocessforhealthprofessionals
work-ingwiththisverychallengingdisease,thatstillrepresents
a majorpublic health problem in Brazil. A better
under-standingofthispathologycanguideamorepragmaticand
workableprotocol,inanattempttoreducethedestructive
effectsofthisdisease.
Methods
The research was a cross sectional study of a historical
cohortof patients seen at the otorhinolaryngology
outpa-tientclinic,referredwithsuspectedMLforevaluationbya
singleotorhinolaryngologistresponsibleforthesecases,in
ordertoobtainastandardizationofclinicalinformationin
aperiodfromDecember2012toDecember2013.
After confirming the clinical suspicion of ML by the
specialist, patients wereinvited toparticipate and,after
signinga written informedconsent, underwentbiopsy for
histopathology with topical instillation of 10% lidocaine
spray into the lesion, with preservation in 10% buffered
formaldehyde.Soonafter,materialfromthebiopsybedwas
collectedwithacervicalbrushforPapsmeartodetermine
PCRintwosamples;toaccomplishthis,thesurgeonmade
aslightrotationonthewoundbiopsywithtwobrushes;one
samplewasallocatedtotheLeishmaniatest and
determi-nation of the species, and the other tothe LVR1 search,
withpreservation inRNALaterTM (Ambion®) untilthe time
ofDNAandRNAextraction.Forthesepurposes,commercial
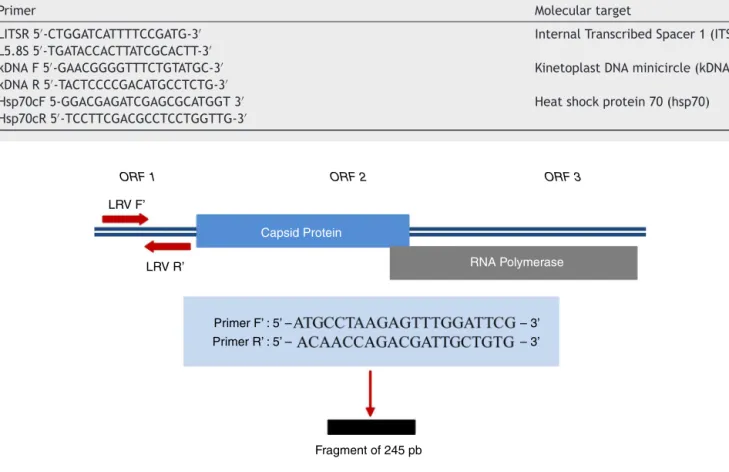
Table1 DescriptionofprimersusedforDNAdetectionofLeishmania.
Primer Moleculartarget
LITSR5′-CTGGATCATTTTCCGATG-3′ L5.8S5′-TGATACCACTTATCGCACTT-3′
InternalTranscribedSpacer1(ITS1)
kDNAF5′-GAACGGGGTTTCTGTATGC-3′ kDNAR5′-TACTCCCCGACATGCCTCTG-3′
KinetoplastDNAminicircle(kDNA)
Hsp70cF5-GGACGAGATCGAGCGCATGGT3′ Hsp70cR5′-TCCTTCGACGCCTCCTGGTTG-3′
Heatshockprotein70(hsp70)
ORF 1 ORF 2 ORF 3
LRV F’
Capsid Protein
RNA Polymerase
Primer F’ : 5’ – Primer R’ : 5’ –
– 3’ – 3’
Fragment of 245 pb LRV R’
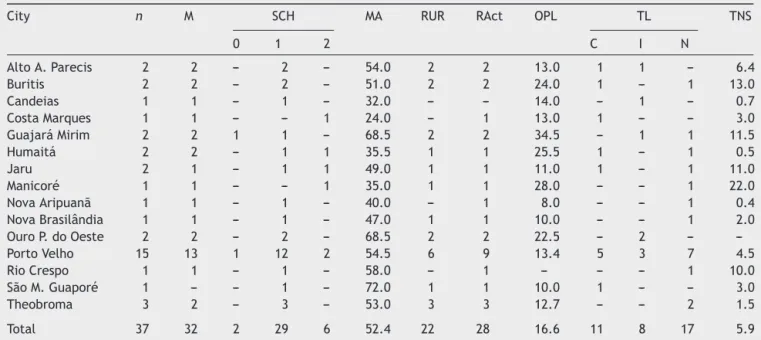
Figure1 RegionamplifiedfordetectionofLRV1andsequencesofprimersused. Source:Cantanhêde.30
biopsied,butsampleswerecollectedformolecularresearch
withanesthetic instillation (as above),and again a brush
rotationwasmadeontheseptalmucosauntilaslightbruise
wasproduced.
For Leishmania DNA detection, three pairs of primers
(ITS1,kDNA,andhsp70)(Table1)wereused;forLRV1,apair
ofprimersthatamplifyasmallregionofORF1(Fig.1)was
used;forallofthem,positivecontrolswereprovided.LVR1
search wasperformed only in samples positive for
Leish-mania,sincethisisanintracellularvirusoftheparasite.
OnlypatientswithconfirmeddiagnosisofMLwitha
pos-itive CPR test and with nasal mucosal injury (in order to
get lesion standardization), and who signed the free and
informedconsent were included. Cases not native tothe
BrazilianNorthRegionwereexcluded.
Tocomparetheseverityoflesionsassociatedwith
pres-enceof virus, the stagingsystem proposed by Lessa10 for
nasalmucosalleishmaniosiswasused.Stage0(noapparent
injury) was included for patients with latent metastases,
with the parasite present in apparently normal mucosa
(Table2).12
StatisticalanalyzeswereconductedwithSPSSsoftware
v.19,EpiData® v.3.1,andEpiDataAnalysisv.1.1.
Descrip-tiveanalyzes ofabsolute andrelative frequencies(with a
95%confidenceinterval)forclinicalsignsdetectedandfor
speciesof Leishmaniawerecarriedout.Relativerisk (RR)
ofpresenceofLRV1inpatientswithmucosalvs.skinlesion,
obtainedinastudybyCatanhêde(2011),wascalculated.
Table2 Stagingofnasalmucosalesions.
Stage Clinicalobservationsofnasalmucosalesion
0 Noapparentlesions
I Nodulationwithoutulceration II Superficialulceration III Deepulceration IV Septalperforation
V Destructionofnasalarchitectureandchanges infacialstructure
StagingsystemproposedbyLessa,10modifiedbyIto.
The collected samples met the criteria of
Resolu-tion CNS 441/2011. The research project was approved
by the Research Ethics Committee under No. CAAE
10215912.1.0000.5300.
Results
This studyevaluated44patients;6wereexcludedfor not
havingadiagnosisconfirmedbyPCR.Thus,37patientsfrom
13 municipalities of Rondoniaand twoof Amazonas were
included(Table3andFig.2).
Twenty-nine (78.3%) patients reported having CL with
Table3 EpidemiologicaldataofstudyparticipantsinPOC,cityofPortoVelho,AC,Brazil.
City n M SCH MA RUR RAct OPL TL TNS
0 1 2 C I N
AltoA.Parecis 2 2 --- 2 --- 54.0 2 2 13.0 1 1 --- 6.4
Buritis 2 2 --- 2 --- 51.0 2 2 24.0 1 --- 1 13.0
Candeias 1 1 --- 1 --- 32.0 --- --- 14.0 --- 1 --- 0.7
CostaMarques 1 1 --- --- 1 24.0 --- 1 13.0 1 --- --- 3.0
GuajaráMirim 2 2 1 1 --- 68.5 2 2 34.5 --- 1 1 11.5
Humaitá 2 2 --- 1 1 35.5 1 1 25.5 1 --- 1 0.5
Jaru 2 1 --- 1 1 49.0 1 1 11.0 1 --- 1 11.0
Manicoré 1 1 --- --- 1 35.0 1 1 28.0 --- --- 1 22.0
NovaAripuanã 1 1 --- 1 --- 40.0 --- 1 8.0 --- --- 1 0.4
NovaBrasilândia 1 1 --- 1 --- 47.0 1 1 10.0 --- --- 1 2.0
OuroP.doOeste 2 2 --- 2 --- 68.5 2 2 22.5 --- 2 ---
---PortoVelho 15 13 1 12 2 54.5 6 9 13.4 5 3 7 4.5
RioCrespo 1 1 --- 1 --- 58.0 --- 1 --- --- --- 1 10.0
SãoM.Guaporé 1 --- --- 1 --- 72.0 1 1 10.0 1 --- --- 3.0
Theobroma 3 2 --- 3 --- 53.0 3 3 12.7 --- --- 2 1.5
Total 37 32 2 29 6 52.4 22 28 16.6 11 8 17 5.9
n,numberofparticipants;M,males;SCH,schooling;0,illiterate;1,primaryeducation;2,highschool;MA,meanage;RUR,livinginrural area;RAct,numberofindividualswithruralactivities;OPL,meanofonsetofprimarylesioninyears;TL,treatmentforleishmaniosis; C,complete;I,incomplete;N,nottreated;TNS,meantimeofonsetofnasalsymptomsinyears.
patientshadahistoryofCLwithoutacompatiblescar;and five(13.5%)patientshadneitherprevioushistorynorCLscar. AccordingtoTable4,themostcommonsymptomswere:
production offetid crusts,chronic fetidrhinorrhea, slight
epistaxisassociated withcrustremoval, nasalobstruction
and, at the time of physical examination, granulomatous
ulcer, presence of crusts, mucosal hyperemia, and septal
perforation.
Ofthisgroupof37patients,30(81.1%)werediagnosed
withL.braziliensis,five(13.5%)withL.guyanensis,andtwo
(5.4%)hadmixedinfectionwithL.braziliensisandL.
guya-nensis.LVR1viruswaspresentin26cases(70.3%),with23of
themassociatedwithL.braziliensis,twowithL.guyanensis,
andonewithamixedinfection.
Themeantimeforonsetoftheprimarylesionwas16.6
years (95% CI 11.1---22.1; SD=16.4), ranging from 0 to 66
5.4%
8.1%
16.2%
32.4%
40.5%
76.7%
81.1%
0 Pharynx injury
Odynophagia
Turbinates
Itching
Nasal pain
Hyperemia mucosa
Epistaxis associated with crusts
Fetid crusts
5 10 15 20 25 30
Patients
Signs
40 35
91.9%
Figure2 Mainsignsandsymptomspresentedbypatients eval-uatedinthesurvey.
years.Whenthegroupswerecomparedwithrespectto
pres-enceor absenceofLRV1, themeantime foronset ofthe
primarylesionwas16.2years(CI95%10.2---22.2;SD=14.9)
for LRV1+ and 17.7 years (95% CI4.0---31.4; SD=20.4) for
LRV1−.TherewasnodifferencebetweenLRV1+andLRV1−
groups(p=0.790).
The mean time for the onset of nasal symptoms was
5.9years(95% CI 3.5---8.3,SD=7.3),ranging from0 to22
years.Inthe comparisonofpresence vs.absence ofLRV1
virus,thefollowingmeantimeswereobtained:LRV1+:5.7
Table4 LeishmaniaspeciesandpresenceofLRV1virus.
Municipality RCP LRV1
Lb Lg Lb+Lg
AltoAlegredosParecis 2 --- --- 2
Buritis 2 --- --- 2
CandeiasdoJamari --- --- 1
---CostaMarques 1 --- --- 1
GuajaráMirim 2 --- ---
---Humaitá 1 --- --- 1
Jaru 2 --- --- 2
Manicoré 2 --- --- 2
NovaBrasilândiaD’Oeste 1 --- --- 1
NovoAripuanã 1 --- --- 1
OuroPretodoOeste 1 1 ---
---PortoVelho 11 3 1 11
RioCrespo --- 1 ---
---SãoMigueldoGuaporé 1 --- --- 1
Theobroma 3 --- --- 2
Total 30 5 2 26
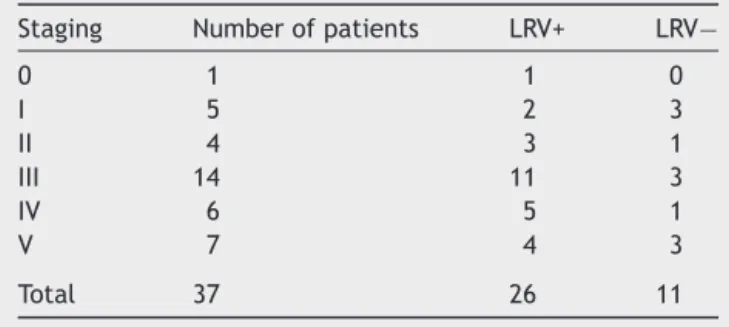
Table5 Clinicalstagingsystemforpatients’nasalmucosa.
Staging Numberofpatients LRV+ LRV−
0 1 1 0
I 5 2 3
II 4 3 1
III 14 11 3
IV 6 5 1
V 7 4 3
Total 37 26 11
years(95%CI2.88---8.50;SD=6.95);LRV1−:4.7years(95%CI 0.04---9.43,SD=6.99).Nodifferencewasobservedbetween LRV1+andLRV1−groups (p=0.351).OnepatientwithHIV developedCLandMLalmostsimultaneously.
TocomparewhetherpatientswithLRV1hadmoresevere injuries vs. patients without the virus, lesion staging was usedinthisanalysis(Table5).
Table5showsthatthemajorityofthelesionspresented
instages III, IV,and V(73%). Of thoseLRV1+patients, 20
(76.9%)wereinmostadvancedstages(III,IV,andV),while
ofthoseLRV−patients,seven(63.6%)wereinthesestages.
However,therewasnosignificantdifferenceinclinical
stag-ingbetweenLRV1+vs.LRV1−patients(p=0.09).
For technical reasons, only 21 of all histopathology
results were received: six diagnosed with leishmaniosis,
sevenwithcompatibility(oneofthesewithPCRnegativefor
leishmaniosis),sixconsiderednonspecific,onewithchronic
rhinitis,andonewithparacoccidioidomycosis.
Discussion
Leishmaniosis is an endemic disease in North Region of
Brazil,whichhasthecountry’slargestdetectionrate.9,26,27
Based on the Sistema de Informac¸ão de Agravos de
Notificac¸ão (SINAN) database28 concerning ACL in Brazil,
until2003---2004, therewasan increasein notifications of
cutaneousleishmaniosis (CL)inBrazil,mainlyintheNorth
Region,witha peakclose to30,000 cases/year, but from
2006onwardstherehasbeenadecreaseandstabilizationto
approximately21,000notificationsperyear.MLfollowsthis
trend,fallingfrom2000to1400casesinthesameperiod.
ThestateofRondoniaexperiencedthesteepestdeclineof
CL,decreasingfrom1981casesreportedin2004to859cases
in2010.MLfollowedasimilarcurve,withapeakof196cases
in2005thatdiminishedto118casesin2010.Forthesame
year,the detectioncoefficientsfor CLandML were46.33
and5.7per10,000inhabitants,respectively.
Theepidemiologicalprofileofthestudiedgroupwasas
follows:men(86%)witha meanageof 52years,living in
aruralarea,withahistory ofCLfor amean of18 years,
withnotreatmentoronlyincompletelytreated,andwitha
meanof5.4yearsofnasalsymptoms.Thisprofileissimilar
tothatofGuerra’s9studyinManauson47patientswithML;
littledifferenceinmeanage(47years)andindurationof
nasallesion(8.3years)wasobserved.Inthisstudy,specific
epidemiologicalprofiles forLRV1+andLRV1−exhibitedno
significantdifference.
ThepredominantspeciesincasesofMLwasL.
brazilien-sis(81%);corroboratingthefindingsofGuerra9andcontrary
tootherpublisheddata,thepresentstudyfoundfive(13.5%)
patientsinfectedwithL.guyanensis.Totheauthors’
knowl-edge,thisisthefirstreportofnasalmucosamixedinfection
withL.braziliensisandL.guyanensis,withtwo(5.6%)cases:
onewiththevirus,andbothcasesinvolvingpalateand
phar-ynxmucosa.ThisfindingincreasedtherateofL.guyanensis
infections to19%, confirmingthesignificant prevalence of
this species. There are few studies on the prevalence of
Leishmania species in the region; it is believed that this
species(i.e.L.guyanensis)hasalwaysbeenpresent,inpart
becauseitwasdetectedinthepresentandalsoinGuerra’s
study.
Thepresenceof mixedinfections highlightsthelack of
cross-protection,whichaparticularspeciescanelicit
rela-tivetoanotherspecies.However,thisdualinfectioncould
constitute a large source of antigens, generating a
Th1-typehyperimmuneresponseandcausinga moreextensive
involvementofaerodigestivemucosa,afindingobservedin
thesetwopatients.
Ofthe37cases,LRV1wasdetectedin26(70.3%).LRV1
was detected in 23/30 cases of L.braziliensis, 2/5 cases
ofL.guyanensis,and1/2casesofmixedinfections.These
findings reveal a high frequency of this virus in mucosal
infections byboth Leishmaniaspecies;however, one-third
of patients had ML and did not harborthe virus,
indicat-ingthatmetastaticlesionsexhibitotherfactorsassociated
withthisclinicalform.Pereiraetal.found LRV1intwoof
fivecases(40%)ofCLfromtheNorthRegionofBrazil,andno
caseswithLRV1in40ACLpatients(ninewithML)inRiode
Janeiro(SoutheasternRegion);Ogg25detected25.5%LRV1+
in47samplesofACL(twoofML).Hartley19reportedthatLRV
maycontributevariablytoML,actinginisolationortogether
withotherfactors.
InPereira’sstudy,theabsenceofLRV1inRiodeJaneiro
supportstheoriesproposingthatLeishmaniaisnativetothe
Amazonregion,whilethespeciesthatpredominateinSouth
and SoutheastRegions of this countrymay have different
origins(Mediterraneantheory).4,5ThepresenceofLRV1can
serve as phylogenetic marker for the origin of parasites.
LeishmaniafromAmazonregionhavehighergenetic
diver-sitythanSoutheastLeishmaniae.29
Cantanhêde,30 in his work on LRV1 detection in ACL
patients, which is part of alarger researchgroup onACL
in the Amazon region (and of which the present work is
alsopart),detected35.9%LRV1positivityin78CLpatients
(RR=0.63; 95% CI0.10---0.55). In the present assessment,
LRV1detectioninMLwas70.3%,showingasignificant
asso-ciation of virus involvement with ML (RR=2.67; 95% CI
1.82---9.81). This association may result from a change in
theimmuneresponsecausedbythisvirus.13,16,19,21
For the first time, a correlation study between
pres-enceofLRV1andclinicalphenotypeofMLwascarriedout.
This study found nosignificant difference between LRV1+
vs.LRV1-groupsbasedonthestagingsystemproposedfor
mucosal lesions,10 withregard tothe severity of injuries.
Similarly,epidemiologicaldifferencesbetweengroupswere
not found, nor differences between signs and symptoms
exhibitedbysuchgroups.
Facedwiththepossibilityofusingthevirustodetermine
moresevere lesionsorlesionswithmorerapidonset,and
consideringthatthiswouldcausethepatienttoseek
intervaltotheonsetofsymptomsofnasalinjury foreach
group(LRV+/LRV−)aftertheonsetof theskin injury,and
alsothetimespentbyeach grouptoseekmedicaladvice
aftertheonsetofnasalsymptoms.Thesetwopiecesof
infor-mation couldrepresent the precocity of the onset of the
injuriesandtheseverityoftheirclinicalsymptoms,
respec-tively. There wasno significance in the time toonset of
symptoms(p=0.13),orintheelapsedtimetoseekmedical
advice(p=0.35)betweengroups.
Tocomparethedegreeofmucosalcompromisebetween
thetwo groups,staging ofseptalinjuries wasperformed,
as proposed by Lessa,10 with the inclusion of stage 0 for
cases where the mucosa shows normal appearance, but
contains parasites.12 This staging was done quite timely,
consideringthatthisstudyonlyincludednasalinjury,which
comprises morethan 90% of mucosal injuries.8,9,11 Among
LRV1+ patients,four (15.38%) werein the most advanced
stage;and amongLRV−patients, three(27.3%) werealso
in this stage. There was no difference in group staging
(p=0.09).
Considering that these patients visit the doctor with
injuriesthatarealreadyveryadvanced,theselesionswould
probablybeatastagewhereadifferentiationbetweenboth
groups, withrespect toclinical phenotype, can nolonger
bemade.Whether therearedifferenceswasnotfoundin
thisstudy;butundoubtedly,itwasascertainedthatstrongly
destructivelesionsarevirus-independent.
Inanidealscenario,CLpatientswithandwithoutLRV1
wouldbefollowed-up,sothatonecouldcomparethe
devel-opmentofmucosallesionsofbothgroups.However,indaily
routinethis appears impractical, becausethe appearance
oftheselesionscantakeaverylongtime;andasFigueroa
etal.12 showedintheirstudy,theparasitemaybepresent
inhealthymucosawithoutindicatingdisease.Theseauthors
point outthat thiscondition is morethe rulerather than
exception.
ML patients arediagnosedlate,and mostpresent with
advanced lesions,withagreat potentialof occurrenceof
sequelaftertreatment. This scenario mayreflectthe
dif-ficultyofaccessingthemedicalcaresystem,9,27 diagnostic
difficulty,8,9,11,12and/orpoorknowledgeofthedisease.
Itiscommonthatinhis/herfirstcontactwithapatient
clinically diagnosedwith ML,the physician (general
prac-titioner, dermatologist, or infectious disease specialist) is
unfamiliarwithclinicalevaluationofnasalmucosa,which
isthemostcommonsiteforthisdisease.Thus,this
profes-sionalendsupreferringthispatienttotheotolaryngologist,
whoalsoisnotusedtomucosalgranulomatousdiseases,due
tothedifficultyforconfirmationofthediagnosisofthis
dis-ease.Thediagnosticmeansavailableinhealthfacilitiesare
insufficientand inadequatetoconfirm anML case, dueto
naturaldifficultiesofthedisease(lowparasitemiainlesions,
previousskin infection).Thus,onewoulddependonmore
complextestssuchasPCRthatarenotavailableinendemic
areas.
LRV1exists inmanyspeciesofLeishmania,intheform
of stableinfection.The virus hasbeen detected
through-outSouthAmericainpatientswithcutaneousleishmaniosis,
often complicated by the presence of infectious
metas-tasis accompanied by an underlying hyperinflammatory
response.13 LRV1detectionmayrepresentclinical benefits
byguidingtreatmentandprognosis,duetoitspotentialin
determiningtheclinicalformsofleishmaniosis.Additionally,
itcanfunction asatarget fordevelopmentof new
treat-ments,for example, the production of vaccines or other
pharmacologicagents.LRV1seemsnottobethelastfrontier
inelucidatingthepathophysiologyofML,butitrepresents
anotherstrongfactorinvolvedinthenaturalhistoryofthis
disease.
Conclusion
Despitethedemonstrationofanassociationbetween
pres-enceofLRV1virus andachangeinimmuneresponse,this
studyfoundnocorrelationamongclinicalfeaturesand
pres-enceof the virus in patients with mucosal leishmaniosis.
Nonetheless,thefrequencyofthevirusinmucosalinjuries
istwicethatinskin lesions,demonstratingtheneed fora
betterunderstanding.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.AlvarJ,VelezID,BernC,HerreroM,DesjeuxF,CanoJ,etal. TheWHOLeishmaniasisControlTeamLeishmaniasisWorldwide andglobalestimatesofitsincidence.PLoSONE.2012;7:e35671.
2.Vega JC, Sanchez BF, MonteroLM, Monta˜na R, Mahecha MP, Due˜nes B, et al. The cost-effectiveness of cutaneous leish-maniasispatientmanagementduringanepidemicinChaparral, Colombiain2004.TropMedIntHealth.2007;12:1540---4.
3.BRASIL---Ministério daSaúde.ManualdeVigilânciada Leish-maniose Tegumentar Americana.Segunda Edic¸ão Atualizada. Brasília:EditoradoMinistériodaSaúde;2010.p.17---31.
4.ValeE,FurtadoT.LeishmaniosetegumentarnoBrasil:revisão históricadaorigem,expansãoeetiologia.AnBrasDermatol. 2005;80:421---8.
5.Altamirano-Enciso AJ, Marzochi MCA, Moreira JS, Schubach AO,MarzochiKBF.Ontheoriginandspreadofcutaneousand mucosalleishmaniasis,basedonpre-andpost-Colombian his-toricalsources.HistCiencSaúde-Manguinhos.2003;10:853---82.
6.LainsonR.TheNeotropicalLeishmaniaspecies:abriefhistorical reviewoftheirdiscovery,ecologyandtaxonomy.RevPan-Amaz Saúde.2010;1:13---32.
7.CupolilloE,GrimaldiGJr, MomenH.Ageneralclassification ofNewWorldLeishmaniausingnumericalzymotaxonomy.AmJ TropMedHyg.1994;50:296---311.
8.Lessa MM, Lessa HA, Castro TWN, Oliveira A, Scheifer A, MachadoP,etal.Mucosalleishmaniasis:epidemiologicaland clinicalaspects.BrazJOtorhinolaryngol.2007;73:843---7.
9.GuerraJAO,PrestesSR,SilveiraH,CoelhoLIARC,GamaP,Moura A,etal.MucosalLeishmaniasiscausedbyLeishmania(Viannia) braziliensisandLeishmania(Viannia)guyanensisintheBrazilian Amazon.PLoSNeglTropDis.2011;8:e980.
10.Lessa HA, Lessa MM, Guimarães LH, Lima CM, Arruda S, MachadoPR,etal.Aproposednewclinicalstagingsystemfor patientswithmucosalleishmaniasis.TransRSocTropMedHyg. 2012;106:376---81.
11.Diniz JLC, Costa MOR, Gonc¸alves DU. Mucocutaneous Leish-maniasis: clinical markers in presumptive diagnosis. Braz J Otorhinolaryngol.2011;77:380---4.
tissues of patients with cutaneous Leishmaniasis caused by Leishmania(Viannia)Species.JInfectDis.2009;200:638---46.
13.IvesA,RonetC,PrevelF,RuzzanteG,Fuertes-MarracoS,Schutz F,etal.LeishmaniaRNAviruscontrolstheseverityof mucocu-taneous.Science.2011;331:775---8.
14.Reis LC, Brito MEF, Souza MA, Pereira MRA. Mecanismos imunológicos na resposta celular ehumoral na leishmaniose tegumentaramericana.RPT.2006;35:103---15.
15.Ronet C,Beverley SM,Fasel1F N. Muco-cutaneous leishman-iasis in the New World: the ultimate subversion.Virulence. 2011;2:547---52.
16.BRASIL--- MinistériodaSaúde.ManualdeVigilânciada Leish-maniose Tegumentar Americana. Segunda Edic¸ãoAtualizada. Brasília:EditoradoMinistériodaSaúde;2010.p.33---41.
17.CarvalhoLP,PassosS,BacellarO,LessaM,AlmeidaRP, Maga-lhãesA,et al.DifferentialImmuneregulationofactivatedT cellsbetweencutaneousandmucosalleishmaniasisasamodel forpathogenesis.ParasiteImmunol.2007;29:251---8.
18.BacellarO,LessaH,SchrieferA,MachadoP,JesusAR,DutraWO, etal.Up-regulationofTh1-typeresponsesinmucosal leishman-iasispatients.InfectImmun.2002;70:6734---40.
19.HartleyMA,RonetC,ZanggerH,BeverleySM,FaselN. Leish-maniaRNAvirus:whenthehostpaysthetoll.FrontCellInfect MicrobiolMicrobiol.2012;2:1---15.
20.WidmerG,DooleyS.PhylogeneticanalysisofLeishmaniaRNA virusandLeishmaniasuggestsancientvirus-p3arasite associa-tion.NucleicAcidsRes.1995;23:2300---4.
21.ZanggerH, RonetC,Desponds C,Kuhlmann FM,Robinson J, HartleyMA,etal.DetectionofLeishmaniaRNAvirusin Leish-mania.ParasitesPLoSNeglTropDis.2013;7:e-2006.
22.Pereira LOR, Maretti-Mira AC, Rodrigues KM, Lima RB, Oliveira-Neto MP,Cupolillo E,et al.Severity oftegumentary leishmaniasis is not exclusively associated with Leishmania
RNA virus 1 infection in Brazil. Mem Inst Oswaldo Cruz. 2013;108:665---7.
23.MedeirosACR,RodriguesSS,RoselinoAMF.Comparac¸ãoentrea especificidadedoPCRedetecc¸ãohistopatológicodeleishmania paraodiagnósticodaleishmaniosecutâneaamericana.BrazJ MedBiolRes.2002;35:421---4.
24.WeiratherJL,JeronimoSMB,GautamS,SundarS,KangM,Kurtz MA,etal.SerialquantitativePCRassayfordetection,species discriminationandquantificationofLeishmaniaspp.inHuman Samples.JClinMicrobiol.2011;49:3892---904.
25.OggMM,CarrionR,BotelhoJRACC,MayrinkW,Correa-Oliveira R,PattersonJL.Shortreport:quantificationofleishmaniavirus RNAinclinicalSamples anditspossibleroleinpathogenesis. AmJTropMedHyg.2003;69:309---13.
26.SilvaN, Muniz V.Epidemiologia da leishmaniosetegumentar americananoEstadodoAcre,Amazôniabrasileira.CadSaude Publica.2009;25:1325---36.
27.BasanoSA,CamargoLMA.Leishmaniosetegumentaramericana: histórico,epidemiologiaeperspectivasde controle.RevBras Epidemiol.2004;7:328---37.
28.Brasil. Sistema de Informac¸ão de Agravos de Notificac¸ão (SINAN).MinistériodaSaúde.Availablefrom:http://dtr2004. saude.gov.br/sinamweb[accessed:07.01.14].
29.CupolilloE,BrahimLR,ToaldoCB,Oliveira-NetoMP,BritoME, FalquetoA.Geneticpolymorphismandmolecularepidemiology ofLeishmania(Viannia) braziliensisfrom differenthostsand geographicareasinBrazil.JClinMicrobiol.2003;41:3126---32.