www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
REVIEW
ARTICLE
Malignant
tumors
of
the
temporal
bone
---
our
experience
夽
Ana
Pereira
da
Silva
a,∗,
Eduardo
Breda
b,
Eurico
Monteiro
baCentroHospitalardoPorto,Porto,Portugal bInstitutoPortuguêsOncologia,Porto,Portugal
Received27May2015;accepted1September2015 Availableonline7January2016
KEYWORDS
Temporalbone; Carcinoma; Surgicaltreatment
Abstract
Introduction:Malignanttumors ofthetemporalbonearerare,withanestimatedincidence ofabout0.8---1.0per1,000,000 inhabitantsperyear.The vastmajorityofthesetumors are squamouscellcarcinomasandtheirtreatmentiseminentlysurgical.
Objective: Thisstudy isanattempt atsystematizingtheforms ofclinical presentation,the therapeuticpossibilities,andoncologicaloutcomesofpatientswithmalignanttumorsofthe temporalboneinatertiaryhospitalinPortugal.
Methods:The authors present a retrospective study of temporal bone tumors treated and followed during otorhinolaryngologyconsultations between 2004and2014. A reviewofthe literatureisalsoincluded.
Results:Ofthe18patientsincludedinthestudy,16hadaprimarytumorofthetemporalbone, inmostcaseswithsquamouscellcarcinomahistology.Ofthese,13patientsweretreatedwith curativeintentthatalwaysincludedthesurgicalapproach.Diseasepersistencewasobserved inonepatientandlocalrecurrenceinfivepatients,onaverage36.8monthsaftertheinitial treatment.
Conclusions: Theanatomicalcomplexityofthetemporalboneandthecloseassociationswith vitalstructuresmakeitdifficulttoperformtumorresectionwithmarginsofsafetyandthus, tumorrelapsesarealmostalwayslocal.Ahighlevelofsuspicioniscrucialforearlydiagnosis, andstringent andprolongedfollow-upafter treatment isessentialfor diagnosis andtimely treatmentofrecurrances.
© 2015 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
夽 Pleasecitethisarticleas:daSilvaAP,BredaE,MonteiroE.Malignanttumorsofthetemporalbone---ourexperience.BrazJ
Otorhino-laryngol.2016;82:479---83.
∗Correspondingauthor.
E-mail:[email protected](A.P.daSilva).
http://dx.doi.org/10.1016/j.bjorl.2015.09.010
PALAVRAS-CHAVE
Ossotemporal; Carcinoma;
Tratamentocirúrgico
Tumoresmalignosdoossotemporal---anossaexperiência
Resumo
Introduc¸ão:Ostumoresmalignosdoossotemporalsãoraros,comumaincidênciaestimadade cercade0,8---1 pormilhãode habitantesporano.A grandemaioriasãocarcinomas espino-celulareseoseutratamentoéeminentementecirúrgico.
Objetivo:Este trabalho tem como objetivo tentar sistematizar as formas de apresentac¸ão clínica, aspossibilidadesterapêuticas e os resultados oncológicosde doentescom tumores malignosdoossotemporalnumhospitalterciárioemPortugal.
Método: Osautoresapresentamumestudoretrospectivodetumoresdoossotemporaltratados eacompanhadosemconsultasdeotorrinolaringologiaentre2004e2014.Étambémapresentada umarevisãodaliteratura.
Resultados: Dos18doentesincluídosnoestudo,16apresentavamumtumorprimáriodoosso temporal,namaioriadoscasoscomhistologiadecarcinomaespinocelular.Destes,13doentes foramsubmetidosatratamentocomintuitocurativoqueincluiusempreumaabordagem cirúr-gica.Verificou-sepersistênciadadoenc¸aem1doenteerecidivalocalem5doentes,emmédia 36,8mesesapósotratamentoinicial.
Conclusões:Acomplexidadeanatómicadoossotemporaleasestreitasrelac¸õescomestruturas deimportânciavitaltornamdifícilaexéresetumoralcommargensdeseguranc¸a,peloqueas recidivastumoraissãoquasesemprelocais.Umníveldesuspeic¸ãoelevadoéfundamentalpara umdiagnósticoprecoceeoseguimentorigorosoeprolongadoapósotratamentoéessencial paraodiagnósticoetratamentooportunodasrecidivas.
© 2015 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Tumors of the temporal bone include skin cancer of the pinnaextending tothe temporalbone, primarytumorsof the external auditory canal (EAC), of the middle ear, of themastoidorpetrousapex,andmetastaticlesionsinthe temporalbone. Primarymalignanttumorsofthetemporal bonehaveanestimatedincidenceof0.8---1.0per1,000,000 inhabitantsperyear,and60---80%ofthemaresquamouscells carcinomas.1
Metastatic lesions in the temporal bone are very rare andusuallyoriginatefromprimarybreast,lung,or kidney tumors.2Althoughtheycanoccuratallages,temporalbone tumorsaremorecommoninthe6thto7thdecadeoflifeand inthemalegender.3Amultifactorialetiologyhasbeen sug-gestedfor thesetumorsandionizingradiation isthemost importantriskfactorfortumorsoriginatingintheskinofthe pinnaandEAC,especiallyinfair-skinnedindividuals.4
The development of temporal bone carcinomas in patientswhohaveundergone radiotherapyfor carcinomas elsewhereintheheadhasalsobeen described.Limetal. presentedaseriesofsevenpatientswithahistoryof radio-therapyforthetreatmentofnasopharyngealcarcinoma.5
Althoughchronic otitismediahasbeen associatedwith thepresenceofthetemporalbone carcinoma,thereis no scientificevidencethatthisentityisinvolvedinitsetiology.6 Agentssuchaschlorinateddisinfectantsorhuman papil-lomavirusincases ofcarcinomas associatedwithinverted papillomashavebeenmentionedaspossiblecarcinogens.7---9 Temporalbone tumorsmanifestwithnonspecific symp-toms, such as otorrhea, ear pain, or hearing loss, that
are often attributed to inflammatory ear diseases. Thus, althoughtheyusuallyhaveasuperficiallocation,diagnosis isoftendelayed.10
TumorsofthepinnaandtheEACareknowntobemore aggressiveandhaveahigherriskofrecurrenceandlymph nodemetastasis,possiblyduetothepresenceofthefusion ofmultipleembryonicplanesinthisregion,whichmay facil-itatetumordissemination.11---13
Inadditiontoacomplete otorhinolaryngological exam-ination and the histolopathological analysis, diagnostic imagingassessmentoftheheadandneckareessentialfor accuratetumordiagnosisandstaging.Computerized tomo-graphy(CT)withcontrastallowsassessingtheboneerosion and the presence of regional adenopathy, whereas mag-neticresonanceimaging(MRI)withcontrastallowsabetter assessmentofitsextensiontotheparotidgland, temporo-mandibular joint,petrousapex,and intracranialinvasion. In locally advancedtumors,positron-emissiontomography (PET)allowstheexclusionofdistantmetastasis.1
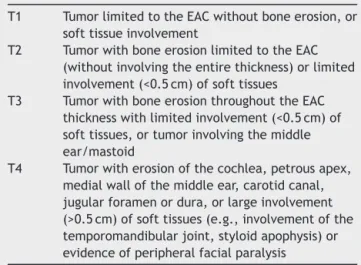
Currently, there is no universally accepted system for the stagingof temporalbone carcinomas. The most com-monly used is the Pittsburgh modified by Moody et al. in 2000(Table1),whichisbasedonphysicalexamination, pre-operativeCT,andthepresenceoffacialparalysis.14
Table1 ModifiedPittsburghstaging systemfor temporal bonecarcinomas.
T1 TumorlimitedtotheEACwithoutboneerosion,or softtissueinvolvement
T2 TumorwithboneerosionlimitedtotheEAC (withoutinvolvingtheentirethickness)orlimited involvement(<0.5cm)ofsofttissues
T3 TumorwithboneerosionthroughouttheEAC thicknesswithlimitedinvolvement(<0.5cm)of softtissues,ortumorinvolvingthemiddle ear/mastoid
T4 Tumorwitherosionofthecochlea,petrousapex, medialwallofthemiddleear,carotidcanal, jugularforamenordura,orlargeinvolvement (>0.5cm)ofsofttissues(e.g.,involvementofthe temporomandibularjoint,styloidapophysis)or evidenceofperipheralfacialparalysis
(TTBR).Thissurgicalapproachmaybecombinedwith cer-vical dissection, witha superficial or total parotidectomy and/orsupplementary radiotherapyand/orchemotherapy, according to thedisease extent, presence of lymphnode metastases,histological subtype,available resources, and surgeon’spreference.11,15,16
Methods
Theauthorsperformed aretrospectivelongitudinal cohort study covering the period between January of 2004 and Augustof2014,whichincluded allpatientswitha diagno-sisofmalignanttumorofthetemporalbonetreatedinthe OtorhinolaryngologyServiceofatertiaryhospitalin Portu-gal.
Demographicdata,clinicalhistory,histologicaldiagnosis, tumor staging, and treatmentsperformed were recorded. Allpatientshadaminimumofsixmonthsoffollow-upafter treatment.
A literature review was also performed through the PubMeddatabase, regardingtumorsof thetemporalbone andtheirtreatment.
Results
and
discussion
Thestudyincluded18patientswithmalignanttumorsofthe temporalbone.Ofthese,16hadprimarymalignanttumors ofthetemporalbone,onepatienthadaunilateralmastoid metastasis of breast carcinoma, and another patient had Langerhanscell histiocytosisthat affected both mastoids. Thelattertwopatientsweresubmittedtomastoidectomy,in thefirstcaseforthesurgicalexcisionofthesecondarylesion and,inthesecondcase,toconfirmthediagnosis.Onlythe dataofpatients withprimarytemporalbone tumorswere consideredfortheanalysisshownherein.
Ofthe16patientswithprimarymalignanttumorsofthe temporalbone,56.25%weremenand43.75%women,and themeanageatdiagnosiswas58.7years.Mostpatientshad squamouscellcarcinomas(68.75%),andtheremainderhad basal cellcarcinomas (25%)and one adenoidcystic carci-noma(6.25%).81.25%ofthetumorsoriginatedfromtheEAC
100%
80%
60%
40%
20%
0%
Otorrhea Hypoacusis Otalgia
Symptoms
% of patients
EAC mass PFP
Figure 1 Symptoms reported by patients (PFP, peripheral facialparalysis).
andtheremaininginvolvedthepinna(12.5%)andthemiddle ear(6.25%).
Themostcommonsymptomsreportedbypatientswere otorrhea,hypoacusis,andotalgia(Fig.1),whichisin accor-dancewiththatdescribedintheliterature.Symptomssuch astrismusandperipheralfacialnerveparalysisarerareand indicativeofadvanced-stagedisease.Symptomdurationhas beenassociatedwithpatientsurvival,soitisveryimportant toconfirmthediagnosiswhensymptomsdonotimprovewith standardtreatment suitable for abenign disease,such as externalotitis.17,18 Thetreatmentofthesepatientsshould includeadetailedexaminationoftheexternalearandskin ofthepre-auricularregion,theEAC,tympanicmembrane, parotidgland,cervicalganglia,andcranialnerves.
Atthetimeofdiagnosis,37.5%ofthetumorswerestaged asT1,18.75%asT2,and43.75%asT4,inaccordancewiththe ModifiedPittsburghSystem.Metastaticlymphnodedisease wasidentifiedinonlyoneofthepatients atpresentation, whohadalocallyadvancedtumor.Theestimatedincidence ofmetastases incervical lymphnodesis 10---23%,4 usually involvinglevelsIandII,andimagingstudiesareconsidered tobesufficientforthediagnosisandsurgicalplanning.19
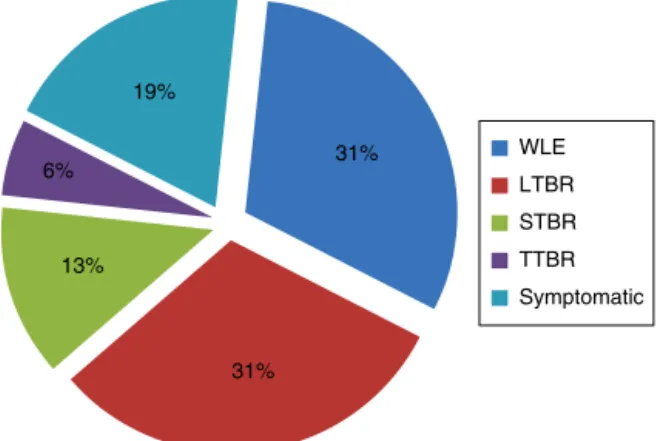
Regardingtheperformedtreatment,symptomatic treat-mentwasperformed in 18.75% of patients,due toof the extentoftheprimarytumorandinvolvementofimportant neurovascularstructures.Incarcinomasoftheexternalear thatdidnotextendmediallybeyondthebony-cartilaginous junctionintheEAC(31.25%),itwaspossibletocarryouta WLE.However,inmostcases(50%)temporalboneresection wasrequired(Fig.2).
Thetemporalboneresectionwasassociatedwitha super-ficial parotidectomy in 18.75% of patients and in 6.25%, with a total parotidectomy. Only one patient underwent ipsilateralcervical lymphnode resection,andthe clinical pathologyanalysisshowednolymphnodemetastasis.
The main surgical complications were associated with STBRandTTBR.OfthepatientssubmittedtoSTBR,complete deafnessand permanentfacialparalysiswereobserved in two patients. TTBR was performed with preservation of theinternalcarotidarteryandnosignificantintraoperative complications.The patienthascompletedeafness, ipsilat-eralperipheral facial palsy, andpersistent dysfunction of thecontralateraltemporomandibularjointassequelae.
31%
31% 13%
6% 19%
WLE LTBR STBR TTBR Symptomatic
Figure 2 Performed treatment (WLE, wide local excision; LTBR,lateraltemporalboneresection;STBR,subtotaltemporal boneresection;TTBR,totaltemporalboneresection).
Table2 Percentagesofoverallanddisease-freesurvival.
Overallsurvival
Total(n=16) 68.75%
PatientswithtumorstageT1/T2(n=9) 88.89% PatientswithtumorstageT4(n=7) 57.14%
Disease-freesurvival
Total(n=16) 62.5%
PatientswithtumorstageT1/T2(n=9) 88.89% PatientswithtumorstageT4(n=7) 28.57%
Themeanfollow-upofpatientsundergoingsurgerywas 67monthsaftertheendoftreatmentandtheoverall sur-vivalwas68.75%(Table2).
In patients at early stage of the disease (T1 and T2), therewaslocalrecurrencein44.44%,onaverage43months aftertreatment.Withtheexceptionofapatientthathadan adenoidcysticcarcinomawhodiedat72months postopera-tively,allpatientsunderwentasecondsurgicalexcision,and weredisease-freeafteramedianfollow-upof66months.
Regarding cancer patients in advanced stage (T3 and T4),42.86%underwentsymptomatictreatment,onepatient haddiseasepersistenceaftersurgery,and28.57%hadlocal recurrence,onaverageninemonthsaftertheinitial treat-ment.Patientsundergoingsymptomatictreatmentdiedon average13monthsafterthediagnosis.
Of the patients with advanced tumors at admission, 28.57% were disease-free at 58.31 months of follow-up, whereasin patients withtumors at early stage, this per-centagewas88.89%(Table2).
Accordingtotheliteratureandinlinewiththeauthors’ experience,treatmentwithcurativeintentalwaysincludes anenblocsurgical resection,whichmustbeaccompanied bytotalparotidectomywhenthereisdirectinvolvementof thegland.1 Performingsuperficialparotidectomyhasbeen advocated when the safety margins arenarrow, or if the diseaseislocallyadvanced,toassessthepresenceof intra-parotidlymphnodemetastases.20,21
Currently,curativesurgicaltreatmentiscontraindicated if there is involvement of the cavernous sinus, massive intracranial extension,unresectable cervical disease, dis-tant metastasis, or poor general status.17 In situations of duralorbraininvolvement,thecurativesurgicaltreatment
can be considered ifit is possible to perform an en bloc
resectionwithdisease-freemargins.1,12
Complementary radiotherapy treatment, such as that performed in the present patients, is indicated in locally advancedtumors(T3---T4)orin thepresenceofaggressive pathologicalfeatures,suchastheperineuralinvasion, mar-gins<5mm,orpositivemarginsorlymphnodemetastasis.20 Regardingthetreatmentwithchemotherapy,thereissome evidence that it may be effective in T4 tumors with postsurgicalresidualormetastaticdisease,butitis contra-indicatedinothersituations.1
Regarding cervical treatment, some authors recom-mend elective ipsilaterallymph node dissectionin locally advanced tumors because of the potential presence of micrometastasesinclinicallynegativenecks.22,23However, asobservedinthepresentstudy,theincidenceofregional lymphnodemetastasisislowandtumorrecurrenceisalmost alwayslocal,sotheperformanceofthisprocedureremains controversial.
Itis generallyaccepted that the prognosis andoverall survival vary considerably depending on the stage of the disease,thetreatmentprotocols,andtheaggressivenessof the surgical resection.24 Considering theanatomical loca-tionoftemporalbonetumors,theprognosisissignificantly influencedbyanydirectinvolvementofnearbystructures, withtheextent ofthe primarytumorrepresentingone of the most important prognostic factors.1 The presence of regionallymphnodemetastasesreflectsthetumor aggres-siveness;itisassociatedwithlocalrecurrence,notregional recurrence.22 Nonetheless, distant metastases, usually in lung,bone,liver,orbrain,areassociatedwithaverypoor prognosis.1,14
Thus,theearlydiagnosisisconsideredofutmost impor-tance,aswellastheperformanceofawidesurgicalexcision oftheprimarytumor.Thisshouldtakeintoaccountthe pos-sibleassociatedconsequences,asitisimportanttoachieve a balance between the radical extent of the surgery and postoperativemorbidity.
Giventhefrequencyoflocalrelapses,aregularand care-fulfollow-upmustbeconductedtotreatrecurrentdisease inatimelymanner.
Conclusions
Malignant tumorsofthetemporalbone arerareandtheir initial presentationis oftenidenticaltothat of inflamma-toryeardiseases.Theotorhinolaryngologistmustmaintain a high level of suspicion when there is no symptomatic improvement after conventional treatment for inflamma-torydiseases.Theimportanceofachievinganearlydiagnosis isreinforcedbythepoorprognosisoftumorspresentingat anadvancedstage.
The surgery, with or without complementary radiothe-rapy, constitutes the basis for the treatment of these tumors. Considering the anatomical complexity and the presence of important neurovascular structures in this region,radicalsurgeriesshouldtaketheassociated morbidi-tiesintoaccount.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Lionello M, Stritoni P, Facciolo MC, Staffieri A, Martini A, Mazzoni A, et al. Temporal bone carcinoma. Current diag-nostic, therapeutic, and prognostic concepts. J Surg Oncol. 2014;110:383---92.
2.CureogluS,TulunayO,FerlitoA,SchachernPA,PaparellaMM, RinaldoA.Otologicmanifestationsofmetastatictumorstothe temporalbone.ActaOtolaryngol.2004;124:1117---23.
3.GidleyPW,ThompsonCR,RobertsDB,DeMonteF,HannaEY.The oncologyofotology.Laryngoscope.2012;122:393---400. 4.Moffat DA, Wagstaff SA. Squamous cell carcinoma of the
temporal bone. Curr Opin Otolaryngol Head Neck Surg. 2003;11:107---11.
5.LimLH,GohYH,ChanYM,ChongVF,LowWK.Malignancyofthe temporalboneandexternalauditorycanal.OtolaryngolHNS. 2000;122:882---6.
6.BarrsDM.Temporalbonecarcinoma.OtolaryngolClinNorthAm. 2001;34:1197---218.
7.MonemSA,MoffatDA,FramptonMC.Carcinomaoftheear:a casereportofapossibleassociationwithchlorinated disinfec-tants.JLaryngolOtol.1999;113:1004---7.
8.GaioE,MarioniG,BlandamuraS,StaffieriA.Invertedpapiloma involvingthetemporalboneanditsassociationwithsquamous cellcarcinoma:criticalanalysisoftheliterature.ExpertRev AnticancerTher.2005;5:391---7.
9.MarioniG, Altavilla G, Busatto G, Blandamura S, DeFilippis C,StaffieriA.Detectionofhumanpapillomavirusintemporal boneinvertedpapilloma bypolymerasechainreaction. Acta Otolaryngol.2003;123:367---71.
10.Al-ShihabiA.Carcinomaoftemporalbonepresentingas malig-nantotitisexterna.JLaryngolOtol.1992;l:908---10.
11.Niparko JK, Swanson NA, Baker SR, Telian SA, Sullivan MJ, KeminkJL.Localcontrolofauricular,periauricular,andexternal canalcutaneousmalignancieswithMohssurgery.Laryngoscope. 1990;100:1047---51.
12.GalTJ,FutranND,BartelsLJ,KlotchDW.Auricularcarcinoma with temporal bone invasion:outcome analysis. Otolaryngol HeadNeckSurg.1999;121:62---5.
13.GaudetJE,WalvekarRR,ArriagaMA,DileoMD,NussDW,Pou AM, et al. Applicability ofthe Pittsburgh stagingsystem for advancedcutaneous malignancy ofthe temporalbone.Skull Base.2010;20:409---14.
14.MoodySA,HirschBE,MyersEN.Squamouscellcarcinomaofthe externalauditorycanal:anevaluationofastagingsystem.Am JOtol.2000;21:582---8.
15.Levine H. Cutaneous carcinoma of the head and neck: management ofmassiveand previously uncontrolled lesions. Laryngoscope.1983;93:87---105.
16.ShottonJC,SergeantRJ,TannerNS,AllenJP.Lateraltemporal boneresectionfor extensivepinnalmalignancy.Hasanything changedinfortyyears?JLaryngolOtol.1993;107:697---702. 17.GidleyPW,DeMonteF.Temporalbonemalignancies.Neurosurg
ClinNAm.2013;24:97---110.
18.GidleyPW,RobertsDB,SturgisEM.Squamouscellcarcinomaof thetemporalbone.Laryngoscope.2010;120:1144---51. 19.Gillespie MB,FrancisHW, CheeN, EiseleDW.Squamous cell
carcinomaofthetemporalbone:aradiographic---pathologic cor-relation.ArchOtolaryngolHeadNeckSurg.2001;127:803---7. 20.ZhangT,LiW, DaiC,ChiF,WangS,WangZ.Evidence-based
surgicalmanagementofT1orT2temporalbonemalignancies. Laryngoscope.2013;123:244---8.
21.Morris LG,Mehra S, Shah JP, Bilsky MH, SelesnickSH, Kraus DH.Predictorsofsurvivalandrecurrenceaftertemporalbone resectionforcancer.HeadNeck.2012;34:1231---9.
22.ZanolettiE,DanesiG.Theproblemofnodaldiseasein squa-mouscellcarcinomaofthetemporalbone.ActaOtolaryngol. 2010;130:913---6.
23.Mazzoni1 A, Danesi G, Zanoletti E. Primary squamous cell carcinoma of the external auditory canal: surgical treat-ment and long-term outcomes. Acta Otorhinolaryngol Ital. 2014;34:129---37.