w w w . r b o . o r g . b r
Original
article
Cubital
compressive
neuropathy
in
the
elbow:
in
situ
neurolysis
versus
anterior
transposition
–
comparative
study
夽
,
夽夽
Marco
Sousa
∗,
Ricardo
Aido,
Miguel
Trigueiros,
Rui
Lemos,
César
Silva
DepartamentodeOrtopediaeTraumatologia,CentroHospitalardoPorto,Porto,Portugal
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received25June2013 Accepted21October2013 Availableonline22October2014
Keywords:
Ulnarnerve Elbow Pain Paresthesia
Ulnartunnelsyndrome
a
b
s
t
r
a
c
t
Objective:Tocomparetheresultsfromtwoofthemostcommonlyusedsurgicaltechniques:
insitudecompressionandsubcutaneoustransposition.Theprocessesofpatientstreated surgicallyinapublicuniversityhospitalbetweenJanuary2004andDecember2011were reviewed.Casesofproximalcompressionofthenerve,angulardeformityoftheelbowand systemicdiseasesassociatedwithnon-compressiveneuropathywereexcluded.
Methods:Ninety-seven cases were included (96 patients). According to the modified
McGowanscore,14.4%ofthepatientspresentedgradeIa,27.8%gradeII,26.8%gradeIIband 30.9%gradeIII.Insituneurolysisofthecubitalwasperformedin64casesandsubcutaneous anteriortranspositionin33.
Results:AccordingtothemodifiedWilsonandKnoutscore,theresultswereexcellentin
49.5%,goodin18.6%,onlysatisfactoryin17.5%andpoorin14.4%.Incomparingthetwo techniques,weobservedsimilarnumbersofexcellentandgoodresults.GradesIIbandIII wereassociatedwithmoreresultsthatwerelesssatisfactoryorpoor,independentofthe surgicaltechnique.
Conclusion: Bothtechniqueswereshowntobeefficientandsafefortreatingcubitaltunnel
syndrome.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Neuropatia
compressiva
cubital
no
cotovelo:
neurólise
in
situ
versus
transposic¸ão
anterior–Estudo
comparativo
Palavras-chave:
Nervoulnar Cotovelo Dor Parestesia
r
e
s
u
m
o
Objetivo:Compararosresultadosdeduasdastécnicascirúrgicasmaisusadas,a
descom-pressãoinsitueatransposic¸ãosubcutânea.Foramrevistososprocessosdosdoentestratados cirurgicamentenumhospitaluniversitáriopúblicoentrejaneirode2004edezembrode2011. Foramexcluídascompressõesproximaisdonervo,deformidadesangularesdocotoveloe doenc¸assistêmicasassociadasaneuropatianãocompressiva.
夽
Pleasecitethisarticleas:SousaM,AidoR,TrigueirosM,LemosR,SilvaC.Neuropatiacompressivacubitalnocotovelo:neuróliseinsitu
versustransposic¸ãoanterior–Estudocomparativo.RevBrasOrtop.2014;49:647–652.
夽夽
WorkdevelopedintheDepartmentofOrthopedicsandTraumatology,PortoHospitalCenter,Porto,Portugal.
∗ Correspondingauthor.
E-mail:[email protected](M.Sousa).
http://dx.doi.org/10.1016/j.rboe.2014.10.005
Síndromedotúnelulnar Metodos: Foramincluídos97casos(96doentes).SegundooescoremodificadodeMcGowan, 14,4%dospacientesencontravam-senoGrauIa,27,8%noII,26,8%noIIbe30,9%noIII.A neuróliseinsitudocubitalfoifeitaem64casoseatransposic¸ãoanteriorsubcutâneaem33.
Resultados: SegundooescoremodificadodeWilsoneKnout,osresultadosforamexcelentes
em49,5%,bonsem18,6%,apenassatisfatóriosem17,5%epobresem14,4%.Nacomparac¸ão dasduastécnicasobservamosvaloressimilaresderesultadosexcelentesoubons.Osgraus IIbeIIIestãoassociadosamaisresultadosmenossatisfatóriosoumausindependentemente datécnicacirúrgica.
Conclusão: Asduastécnicasserevelameficientesesegurasnotratamentodosíndromedo
túnelcubital.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
After observing that the cubital nerve was compressed at the elbow, in a fibro-osseous space defined by a ligament betweenthe medialepicondyle and theolecranon, Feindel andStratford1usedtheterm“cubitaltunnelsyndrome”for thefirsttime.Oneyearearlier,Osborne2haddescribed sim-pledecompressionofthenervebymeansofsectioningthis sameligament.However,thefirstpublishedpapersdatefrom 1878,theyearinwhichPanas3describedtheconditionand Marchand4described aprocedureforreleasingand stretch-ingthecubitalnerve.Theconditionof“toxicneuritisofthe cubitalnerve” wasalsodescribedbyBuzzard5 in1922and, twodecadeslater,Learmonth6alsodescribedtechniquesfor submuscularandintramusculardecompressionand transpo-sition.
Compressionofthecubitalnerveisacommoncondition andmayoccuratseverallevels.Compressionattheelbowis thecommonestformofcubitalcompression7–9andisthe sec-ondcommonestcompressionneuropathyoftheupperlimbs. Thediagnosis isbased on symptoms, signs, orthopedic testsandelectrophysiologicalstudies.
Manycasesofcubitaltunnelsyndromecanbetreated con-servativelywithoutsurgery.Nevertheless,somecasesrequire surgicaltreatmentwithaviewtoavoidingpersistenceofthe symptomsandprogressionoftheneurologicaldeterioration. Thesurgicaltreatmentshouldbeguidedbythefollowing prin-ciples: (1) release of all the possible compression sites; (2) preservationofthevascularizationofthecubitalnerveatthe elbow;and(3)earlymobilizationoftheelbow.
Thecommonestsurgicaloptions includesimple decom-pression, medial epicondylectomy, subcutaneous anterior transposition,intramuscularanteriortranspositionand sub-muscularanteriortransposition.
Theelbowisadynamicjoint.Overthecourseoftheday, it flexes and extends to placethe hand in functional pos-itions.Throughthismobility,changestotheshapeandspace ofthecubitaltunneltakeplace.Whentheelbowisflexed,the tunnelbecomesflatter10andthearcuateligamentbecomes tensioned,11 whichleadstoreductionofthespaceavailable forthenerve11,12andincreasedpressureinsidethetunnel.13
FeindelandStratford1 andOsborne2advocatedthat sec-tioning the fibrotic band that forms the ceiling of this tunnel would be sufficient for relieving the pressure and
consequentlyrelievingthesymptomsinthemajorityofthe cases.
Undernaturalconditions,thenerveisalsosubjectto trac-tionandexcursionduringthenormalmovementoftheelbow. Anteriortranspositionhastheaimoftransferringthenerve toapointanteriortotheaxisofmobilization oftheelbow. Thisdiminishesthetensionandalsoeliminatesthepressure onthecubitaltunnel.
There is no consensus in the literature regarding the bestsurgicaltreatmentforcubitaltunnelsyndrome.Anterior transpositionisperhapstheproceduremostofteneffected.14 Nonetheless, other authors have defendedthe notion that simple decompression is just as effective as transposition and presentsasimilarsuccessrateandlowercomplication rate.15–17
The present study had the aimof expandingthe infor-mation available on comparisons of results between two techniques thatare widelyusedfortreating cubitaltunnel syndrome:insitudecompressionandsubcutaneousanterior transposition.
Material
and
methods
The records of all patients who were treated surgically at our institution between January 2004 and December 2011 were reviewed. The inclusion criterion was taken to be a diagnosis of idiopathic cubital tunnel syndrome based on physicalexaminationandelectromyographicanalysis.Cases of proximalcompression ofthe nerve, angulardeformities of the elbow and systemic diseases associated with non-compressiveneuropathywereexcluded.
Inthismanner,97caseswereobtained,correspondingto 96patients(56menand40women),withameanageof51.91 years(range:15–84).Therightsidewasinvolvedin51patients
andtheleftsidein46(Table1).
Table1–Demographiccharacteristicsofthepatientsincludedinthestudy.
Total Neurolysis Transposition p
No.ofpatients(n) 97 64 33
Sex(n)
Male 56(58.3%) 38(60.3%) 18(54.5%) 0.373
Female 40(41.7%) 25(39.7%) 15(45.5%)
Meanage(SD) 51.9(14.9) 51.2(14.7) 53.3(15.6) 0.535
Follow-up(months) 10.3(4–33) 9.3(4–29) 11.7(6–33)
Reinterventions 2 2 0
Side 50R;47L 28R;37L 22R;10L
Thus,14.4%(14)ofthepatientswereingradeI,27(27.8%) inIIa,26(26.8%)inIIband30(30.9%)inIII(Table2).
Insituneurolysisofthe cubitalnerve wasperformed in 64cases,whilesubcutaneousanteriortranspositionwas per-formed in 33 cases. Among the patients who underwent neurolysis,12.5%were ingradeI,29.7% inIIA, 28.1%inIIB and29.7%inIII.Amongthosewhounderwentanterior trans-position,18.2%wereingradeI,24.2%inIIA,24.2%inIIBand theremaining33.3%inIII(Table3).Nostatisticallysignificant differencesinthe patients’ preoperativestageaccording to surgerygroupwereobserved(p=0.817).
Thepostoperativeevaluationwasstratifiedinaccordance withthesystemofWilsonandKnout,19inwhichanexcellent result corresponded to minimal sensory and motor alter-ations,without tension at the incision site; good signified moderatesensoryandmotoralterations;satisfactorysignified improved,butwithpersistentalterations;andpoorsignified noimprovementorevenworseningofthestate.
In the descriptive analysis, the continuous variables were represented by the mean and standard deviation.
Table2–Characterizationofthesampleinabsoluteand relativefrequencies.
n %
Typeofsurgery
Neurolysis 64 66.0
Transposition 33 34.0
Total 97 100.0
Sex
Male 56 58.3
Female 40 41.7
Total 96 100
Postoperativeresult
Excellent 48 49.5
Good 18 18.6
Satisfactory 17 17.5
Poor 14 14.4
Total 97 100.0
Preoperativegrade
I 14 14.4
IIA 27 27.8
IIB 26 26.8
III 30 30.9
Total 97 100.0
Mean (min–max)
SD
Age 51.91(15–84) 14.9
The categorical variables were represented by the
abso-lute frequency (n) and the relative frequency (%). With
the aim of selecting appropriate statistical tests, the
Kolmogorov–Smirnovtestwasusedtoascertainwhetherthe
study variables followed normal distribution. To compare
means,Student’sttestforindependentsampleswasused.
Thechi-square testorFisher’s exacttest(whenapplicable) wereusedtoanalyzeassociationsbetweenpairsofcategorical variables.
The four grades of the modified McGowan scale were
regroupedintotwolevels:gradeIwithIIA;andgradeIIBwith III.ThepostoperativeevaluationusingtheWilsonandKnout systemwasreclassifiedintotwogroups:excellentand satis-factory,goodandpoor. Thestatisticaltestswereconducted bilaterallywithasignificancelevelof5%.Thestatistical anal-ysisonthedatawasperformedusingtheIBMSPSSStatistics 20.0software.
Results
FromthemodifiedWilsonandKnoutclassification,outofthe
97 operations performed, 48 (49.5%)produced an excellent
result,18(18.6%)good,17(17.5%)satisfactoryand14(14.4%) poor.Anewsurgicalinterventionwasonlynecessaryin rela-tiontotwopatients(Table1).
Nodifferencesrelatingtosexwereobservedwithregardto thesurgicaltechnique.Themeanagewas52(14.9)years.The patientswhounderwenttranspositionsurgeryweretwoyears olderthanthosewhounderwentneurolysis(53.3versus51.2). Comparison between the results from the two surgical techniques showed that there were no statistically sig-nificant differences, with similar values for the rates of excellentresults(48.4%forneurolysisversus51.5%foranterior
Table3–Comparisonofpreoperativegradeamongthe patientsaccordingtosurgerygroup(neurolysisor transposition).
PreoperativegradebasedonthemodifiedMcGowanscore
GradeI Neurolysis Transposition p
Preoperativegrade n % n %
I 8 12.5 6 18.2 0.817
IIA 19 29.7 8 24.2
IIB 18 28.1 8 24.2
III 19 29.7 11 33.3
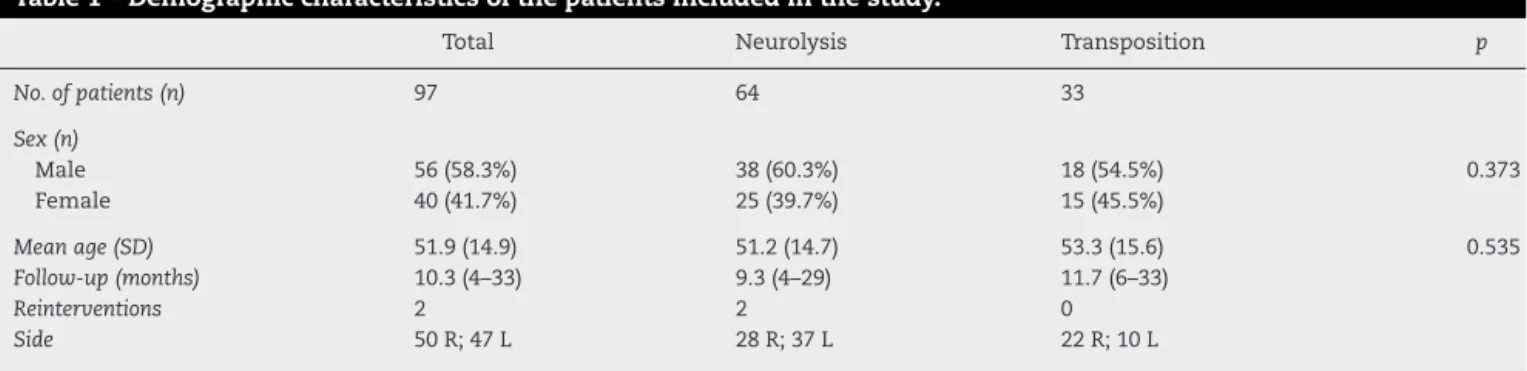
Table4–Comparisonofthepostoperativeresults accordingtothesurgicaltechniqueused.
ModifiedWilsonandKnoutscore
Result Neurolysis Transposition p
n % n %
Excellent 31 48.4 17 51.5 0.957
Good 12 18.8 6 18.2
Satisfactory/poor 21 32.8 10 30.3
Total 64 33
Table5–Comparisonofthepostoperativeresults accordingtopreoperativegradeforthesurgical techniqueofneurolysis.
Result Preoperativegrade p
I/IIA IIB/III
n % n %
Excellent 15 55.6 16 43.2 0.559
Good+satisfactory+poor 12 44.4 21 56.8
Total 27 37
Table6–Comparisonofthepostoperativeresults accordingtopreoperativegradeforthesurgical techniqueoftransposition.
Result Preoperativegrade p
I/IIA IIB/III
n % n %
Excellent 9 64.3 8 42.1 0.208
Good+satisfactory+poor 5 35.7 11 57.9
Total 14 19
transposition) and good results (18.8% versus 18.28%).
Regardingtheresultsthatwereonlysatisfactoryorpoor,the rateswere32.8%forneurolysisand30.3%forsubcutaneous transposition(Table4).
Intheanalysisstratifiedaccordingtotheinitialgradefor thetwotechniques(Tables5and6),itwasseenthat41patients wereingradesIandIIa,ofwhom27 underwentneurolysis and 14,transposition.Amongthe patientswho underwent neurolysis,55.6% achieved anexcellent result and 44.4% a good,satisfactoryorpoorresult.Anexcellentresultwasalso achievedby64.3%ofthe14patientswhounderwent transpo-sition.AmongthepatientsinitiallyclassifiedingradesIIBor III,37underwentneurolysisand19transposition,and excel-lentresultswereattainedby43.2%and 42.1%,respectively, whiletheresultsweregood,satisfactoryorpoorin56.8%and 57.9%,respectively.
Onlytwopatientshadtheneedforfurthersurgical inter-vention.Bothofthesehadundergonesimpledecompression
(Table2).
Discussion
Several surgical techniques have been put forward for treating compression of the cubital nerve in the elbow.
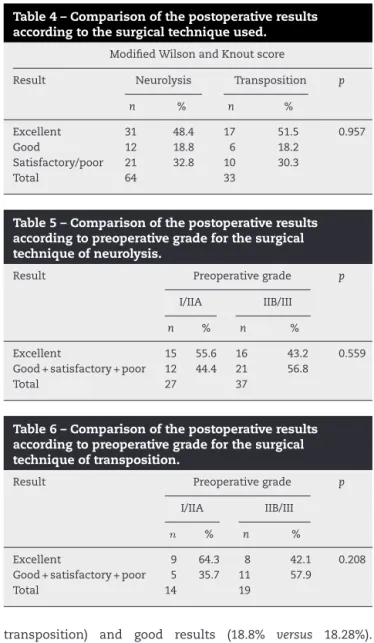
Excellent 0
10 20 30 40 50 60
Good Satisfactory/poor
Neurolysis Transposition 48.4 51.5
18.8
32.8 30.3
18.2
Fig.1–Postoperativeresultsaccordingtothesurgical techniqueused,expressedasrelativefrequencies(%).
Medial epicondylectomy is rarely performed.20,21 Subcuta-neousanteriortranspositionandsimpledecompressionare the proceduresmostused. Inourstudy,onlypatients who underwent operations using these two techniques were included, giventhatbyalargemajority,thesearethe tech-niquesmostperformedinourdepartment.
Inanalyzingtheresults,itseemsthattherewasno pre-ponderanceofonetechniqueovertheother.Independentof thetechnique,therateofexcellentresultsamongthepatients reached48.5%.Whencomparedaccordingtotechnique,the rates of excellent results were close: 48.4% for neurolysis and51.5%fortransposition.Satisfactoryorpoorresultswere obtainedby32.8%and30.3%,respectively,whichreinforced the similarity (Fig. 1).Thisanalysisalsoshowed thatthere wasatendencyforpatientswithhighergradesatthetime ofthe surgery (IIBand III)to havelower rates ofexcellent results(43.2%and42.1%),althoughnostatisticallysignificant differentwasobservedinthisregard(neurolysisp=0.957;and transpositionp=0.559).Thistendencywasshowntobe inde-pendentofthetechniqueandconfirmswhathasbeenwidely disseminatedintheliterature,i.e.thatthechancesof allevi-atingthepainandrecoveringsensitivityandmotorstrength areinverselyrelatedtotheinitialgradeofneuropathy.
The notable study on cadavers by Gelberman et al.22 demonstratedthatintraneuralpressureincreasesmorethan does extraneuralpressure whenflexionisgreater than90◦.
pressurevaluesthatwerehighallthetime,eveninextension, andwhichwerearoundfourtimeshigherinflexion.
Morerecentstudies,29 alsoconductedoncadavers,have demonstratedthatelongationofthenerveoccursespeciallyin thesegmentproximaltotheepicondyleandbetween30◦and
90◦andthenthelengthremainsconstantuntil135◦.However,
ataround135◦,theareaandsagittalcurvatureofthetunnel
decreaseand forcethe nerveinto aflattenedshape.These findingssuggestthatthecompressionisgreatestat135◦.
BasedonthefindingsofGelbermanetal.,22many ortho-pedistsabandonedthesurgicaltechniqueinitiallydescribed byOsborneand started toperformanterior transpositions. However,overthelastfewyears,severalstudieshave demon-stratednotonlythatsimpledecompressionmay bejust as effective as anterior transposition, but also that the latter maybeassociatedwithagreater numberofcomplications. Oneofthefactors maybethepossibilitythat blood vascu-larizationmight bedisturbed duringthe transposition.30–32 Ogataet al.33 demonstratedin anexperimentalstudy that thistranspositionisassociatedwithdecreasedregionalblood flowforatleastthreedaysafterthesurgery.Inarandomized prospectivestudyon44patients,BiggsandCurtis16concluded thattherewere no differencesinthe resultsbetween sim-pleneurolysisandanteriortranspositionandrecommended theformerbecauseofthelowernumberofcomplications.In anotherrandomizedprospectivestudyon152patients, Bar-tels et al.15 comparedsubcutaneous anterior transposition andsimpledecompression andalsoconcludedthat simple decompressionhadequalefficacybutwithalower compli-cationrate(23versus 7,amongatotalof30), whichwould alsobeassociatedwith lower cost.In another randomized studyon70patientsand48monthsoffollow-ups,Gervasio etal.17alsodidnotfindanystatisticallysignificantdifferences betweensimpledecompressionandsubmuscular transposi-tion.Inafourthprospectivestudy withafollow-upof63.1 months,Keineretal.34concludedthatthetwotechniquesled tosimilarresultsandthatsimpledecompressionshouldbe preferredbecause itwasless invasive.Nabhanet al.35 also prospectivelycomparedsimpledecompressionand subcuta-neousanteriortranspositionandreportedthattherewereno differencesinthe resultsand thereforealsorecommended simpledecompressionasthepreferredtreatmentbecauseit isasimplerprocedure.Furthermore,twometa-analyses con-ductedbyMacadametal.36andZlowodzkietal.37didnotfind anystatisticallysignificantdifferences betweenthevarious techniques.
Ourstudyseemstobeconcordantwithmostoftherecently publishedpapersonsurgicaltreatmentofthispathological condition.Despite the needforreinterventioninthe cases oftwopatientswhowereinitiallytreatedbymeansof sim-pledecompression,mostofthe patientstreated usingthis techniqueachievedthesameresultasthosewhounderwent subcutaneoustransposition,independentoftheinitialgrade. Theabsenceofcomplicationsinourstudy,incomparisonwith theotherscited,can beexplainedbythe factthatinsome oftheseotherstudies,anteriortranspositionthatsometimes wasintraorsubmuscularwasusedasthecomparison.Thisis generallyassociatedwithahighercomplicationrate.
From the analysis on the literature, it also seems that medial epicondylectomy has an increasingly limited role.
Muermans et al.38 analyzed their results from 60 epi-condylectomyproceduresperformedon51patientsandfound excellent resultsin 75% ofthem. However, 21 of these 51 patients reported pain in the medial epicondyle after the operation. This was similar to the result obtained by Efs-tathopoulos et al.,39 inwhich45% ofthe patientsoperated continuedtopresentpainsixmonthsafterwards.
Conclusion
Thisstudywaslimitedbyitsretrospectivenatureandbythe smallnumberofpatientsinsomeofthesubgroupsanalyzed. The postoperative results did not present any correlation withthesurgicaltechniqueused,giventhatindependentof the technique, most ofthe patients achieved an excellent result. This reinforcesthe ideathat simple decompression enablesresultssimilartothosefromsubcutaneousanterior transposition.Therefore,withdueregardforthegreater tech-nicalsimplicityofsimpledecompression,wewouldreserve transposition only forcases ofnerves with a potentialfor subluxation,post-traumaticstiffness,valgusinstability,late paralysisofthecubitalnerveorfailureofsimple decompres-sion.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.FeindelW,StratfordJ.Cubitaltunnelcompressionintardy
ulnarpalsy.CanMedAssocJ.1958;78(5):351–3.
2.OsborneGV.Thesurgicaltreatmentoftardyulnar
neuropathy.JBoneJointSurgBr.1957;39:782.
3.PanasJ.Surunecauseconnuedeparalysieduenerfcubital.
ArchGenMed.1878;2:5–22.
4.MarchandAH.Surladistensionchirurgicaledesnerfs.Gazete
HebdomadairedeMédecineetdeChirurgie.1878;25:209–12.
5.BuzzardEF.Somevarietiesoftraumaticandtoxiculnar
neuritis.Lancet.1922;1:317–9.
6.LearmonthJR.Atechniquefortransplantingtheulnarnerve.
SurgGynecolObstet.1942;75:792–3.
7.DellonAL.Reviewoftreatmentresultsforulnarnerve
entrapmentattheelbow.JHandSurgAm.1989;14(4):
688–700.
8.BednarMS,BlairSJ,LightTR.Complicationsofthetreatment
ofcubitaltunnelsyndrome.HandClin.1994;10(1):83–92.
9.ApfelbergDB,LarsonSJ.Dynamicanatomyoftheulnarnerve
attheelbow.PlastReconstrSurg.1973;51(1):76–81.
10.PatelVV,HeidenreichFPJr,BindraRR,YamaguchiK,
GelbermanRH.Morphologicchangesintheulnarnerveatthe
elbowwithflexionandextension:amagneticresonance
imagingstudywith3-dimensionalreconstruction.JShoulder
ElbowSurg.1998;7(4):368–74.
11.VanderpoolDW,ChalmersJ,LambDW,WhistonTB.
Peripheralcompressionlesionsoftheulnarnerve.JBone
JointSurgBr.1968;50(4):792–803.
12.PechanJ,JuliusI.Thepressuremeasurementintheulnar
nerveattheelbow.PlastReconstSurg.1973;51(1):79–81.
13.WernerCO,OhlinP,ElmqvistD.Pressuresrecordedinulnar
14.BartelsRH,MenovskyT,VanOverbeekeJJ,VerhagenWI.
Surgicalmanagementofulnernervecompressionatthe
elbow:ananalysisoftheliterature.JNeurosurg.
1998;89(5):722–7.
15.BartelsRH,VerhagenWI,vanderWiltGJ,MeulsteeJ,van
RossumLG,GrotenhuisJA.Prospectiverandomized
controlledstudycomparingsimpledecompressionversus
anteriorsubcutaneoustranspositionforidiopathic
neuropathyoftheulnarnerveattheelbow:Part1.
Neurosurgery.2005;56(3):522–30.
16.BiggsM,CurtisJA.Randomized,prospectivestudycomparing
ulnarneurolysisinsituwithsubmusculartransposition.
Neurosurgery.2006;58(2):296–304.
17.GervasioO,GambardellaG,ZacconeC,BrancaD.Simple
decompressionversusanteriorsubmusculartranspositionof
theulnarnerveinseverecubitaltunnelsyndrome:a
prospectiverandomizedstudy.Neurosurgery.
2005;56(1):108–17.
18.McGowanAJ.Theresultsoftranspositionoftheulnarnerve
fortraumaticulnarneuritis.JBoneJointSurgBr.
1950;32(3):293–301.
19.WilsonDH,KnoutR.Surgeryofulnarneuropathyatthe
elbow:16casestreatedbydecompressionwithout
transposition.Technicalnote.JNeurosurg.1973;38(6):780–5.
20.AmakoM,NemotoK,KawaguchiM,KatoN,ArinoH,
FujikawaK.Comparisonbetweenpartialandminimalmedial
epicondylectomycombinedwithdecompressionforthe
treatmentofcubitaltunnelsyndrome.JHandSurgAm.
2000;25(6):1043–50.
21.FroimsonAI,AnouchiYS,SeitzWHJr,WinsbergDD.Ulnar
nervedecompressionwithmedialepicondylectomyfor
neuropathyattheelbow.ClinOrthopRelatRes.
1991;(265):200–6.
22.GelbermanRH,YamaguchiK,HollstienSB,WinnSS,
HeidenreichFPJr,BindraRR,etal.Changesininterstitial
pressureandcrosssectionalareaofthecubitaltunnelandof
theulnarnervewithflexionoftheelbow:anexperimental
studyinhumancadavera.JBoneJointSurgAm.
1998;80(4):492–501.
23.WadsworthTG.Theexternalcompressionsyndromeofthe
ulnarnerveatthecubitaltunnel.ClinOrthopRelatRes.
1977;(124):189–204.
24.PechanJ,JulisI.Thepressuremeasurementintheulnar
nerve.Acontributiontothepathophysiologyofthecubital
tunnelsyndrome.JBiomech.1975;8(1):75–9.
25.OsborneG.Compressionneuritisoftheulnarnerveatthe
elbow.Hand.1970;2(1):10–3.
26.FerlicDC.Insitudecompressionoftheulnarnerveatthe
elbow.In:GelbermanRH,editor.Operativerepairand
reconstruction.Philadelphia:JBLippincott;1991.p.1063–7.
27.SchuindFA,GoldschmidtD,BastinC,BurnyF.A
biomechanicalstudyoftheulnarnerveattheelbow.JHand
SurgBr.1995;20(6):623–7.
28.IbaK,WadaT,AokiM,TsujiH,OdaT,YamashitaT.
Intraoperativemeasurementofpressureadjacenttothe
ulnarnerveinpatientswithcubitaltunnelsyndrome.JHand
SurgAm.2006;31(4):553–8.
29.JamesJ,SuttonLG,WernerFW,BasuN,AllisonMA,Palmer
AK.Morphologyofthecubitaltunnel:ananatomicaland
biomechanicalstudywithimplicationsfortreatmentofulnar
nervecompression.JHandSurgAm.2011;36(12):1988–95.
30.AsamiA,MorisawaK,TsurutaT.Funcionaloutcomeof
anteriortranspositionofthevascularizedulnarnervefor
cubitaltunnelsyndrome.JHandSurgBr.1998;23(5):613–6.
31.BaroneCM,JimenezDF,Frempog-BodeauA.Bloodflow
measurementsofinjuredperipheralnervesbylaserDoppler
flowmetry.JReconstrMicrosurg.1992;8(4):319–23.
32.LimBH,TobCL,WongHP,PhoRW.Cadavericstudyonthe
vascularanatomyoftheulnarnerveattheelbow–abasisfor
anteriortransposition?AnnAcadMedSingapore.
1992;21(5):689–93.
33.OgataK,ManskePR,LeskerPA.Theeffectofsurgical
dissectiononregionalbloodflowtotheulnarnerveinthe
cubitaltunnel.ClinOrthopRelatRes.1985;(193):195–8.
34.KeinerD,GaabMR,SchroederHW,OertelJ.Comparisonofthe
long-termresultsofanteriortranspositionoftheulnarnerve
orsimpledecompressioninthetreatmentofcubitaltunnel
syndrome–aprospectivestudy.ActaNeurochir.
2009;151(4):311–5.
35.NabhanA,AhlhelmF,KelmJ,ReithW,SchwerdtfegerK,
SteudelWI.Simpledecompressionorsubcutaneousanterior
transpositionoftheulnarnerveforcubitaltunnelsyndrome.
JHandSurgBr.2005;30(5):521–4.
36.MacadamSA,GhandiR,BezuhlyM,LefaivreKA.Simple
decompressionversusanteriorsubcutaneousand
submusculartranspositionoftheulnarnerveforcubital
tunnelsyndrome:ameta-analysis.JHandSurgAm.
2008;33(8):1314.e1–12.
37.ZlowodzkiM,ChanS,BhandariM,KalliainenL,SchubertW.
Anteriortranspositioncomparedwithsimpledecompression
fortreatmentofcubitaltunnelsyndrome.Ameta-analysisof
randomizedcontrolledtrials.JBoneJointSurgAm.
2007;89(12):2591–8.
38.MuermansS,DeSmetL.Partialmedialepicondylectomyfor
cubitaltunnelsyndrome:outcomeandcomplications.J
ShoulderElbowSurg.2002;11(3):248–52.
39.EfstathopoulosDG,ThemistocleousGS,PapagelopoulosPJ,
ChlorosGD,GerostathopoulosNE,SoucacosPN.Outcomeof
partialmedialepicondylectomyforcubitaltunnelsyndrome.