ww w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Sensitivity
and
specificity
of
assessment
instruments
of
quality
of
life
in
rheumatoid
arthritis
Silvana
Almeida
Ribas
a,
Selena
Dubois
Mendes
a,
Laís
Bittencourt
Pires
a,
Rafaela
Brito
Viegas
a,
Israel
Souza
b,
Maurício
Barreto
a,
Martha
Castro
a,
Abrahão
Fontes
Baptista
c,
Katia
Nunes
Sá
a,∗aEscolaBahianadeMedicinaeSaúdePública,Salvador,BA,Brazil
bInstitutoFederaldeEducac¸ão,CiênciaeTecnologiadoRiodeJaneiro(IFRJ),RiodeJaneiro,RJ,Brazil
cUniversidadeFederaldaBahia(UFBA),Salvador,BA,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received28July2015 Accepted6February2016 Availableonline30May2016
Keywords:
Rheumatoidarthritis Accuracy
Questionnaires Qualityoflife Evaluation
a
b
s
t
r
a
c
t
Objective:TochecksensitivityandspecificityofassessmentinstrumentsofQoLinpatients withrheumatoidarthritis(RA).
Methodology:Accuracystudyinasampleconsistingofpatientswithconfirmeddiagnosisof RA.QoLquestionnairesQVSF-36(GoldStandard),HAQandNHPwereapplied.ThePearson correlationcoefficient,ROCcurve,AUCandYoudenIndex(J)wereusedtoanalyzethedata.
Results:Thisstudyenrolled97individualswithRA.Thefunctionalcapacityestimatedby SF-36wascorrelatedwiththetotalscoreofHAQ(r=−0.666;p<0.001;J=0.579),whilethe emotionalaspectsofSF-36werecorrelatedwiththeemotionalreactionsdomainofNHP (r=−0.316;p=0.005;J=0.341).ThevitalitydomainofSF-36wascorrelatedwiththelevel ofenergyofNHP(r=−0.362;p=0.001;J=0.302).Fortheevaluationoffunctionalcapacity (AUC=0.839;p<0.001)andphysicalaspect(AUC=0.755;p<0.001)themostaccurate instru-mentwastheHAQ.Forevaluationoftheimpactofvitality,sleep(AUC=0.679;p=0.007), emotionalreactions(AUC=0.674;p=0.009)andlevelofenergyinQoL,theNHP(AUC=0.633;
p=0.045)wasthemostspecificandsensitive.Intheevaluationoftheemotionalaspect domain,the mostaccurateinstrument wastheNHP inthe“emotional reaction”score (AUC=0.699;p=0.003).Theevaluationofpainwaslimitedinthethreeinstrumentsand SF-36wastheonlyoneinassessofthedomainsofsocialaspectsandgeneralhealthstatus.
Conclusion:ForevaluationofthephysicalaspectsinpatientswithRA,theHAQisthemost accurate.ForevaluationofemotionalaspectstheNHPisthemostindicated,althoughthe SF-36wastheonlyoneintheevaluationofgeneraldomains.
©2016PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCC BY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](K.N.Sá).
http://dx.doi.org/10.1016/j.rbre.2016.03.015
Sensibilidade
e
especificidade
dos
instrumentos
de
avaliac¸ão
da
qualidade
de
vida
na
artrite
reumatoide
Palavras-chave:
Artritereumatoide Acurácia
Questionários Qualidadedevida Avaliac¸ão
r
e
s
u
m
o
Objetivo: Verificarasensibilidadeeaespecificidadedosinstrumentosdeavaliac¸ãoda qual-idadedevidaempacientescomartritereumatoide(AR).
Metodologia:Estudodeacuráciaemumaamostradepacientescomdiagnósticoconfirmado deAR.Aplicaram-seosquestionáriosdeQVSF-36(padrãoouro),HAQeNHP.Usaram-se ocoeficientedecorrelac¸ãodePearson,acurvaROC,aASCeoíndicedeYouden(J)para analisarosdados.
Resultados: Este estudo envolveu97 indivíduoscom AR. A capacidadefuncional esti-madapeloSF-36estevecorrelacionadacomapontuac¸ãototaldoHAQ(r=−0,666;p<0,001; J=0,579),enquantooaspectoemocionaldoSF-36estevecorrelacionadocomodomínio reac¸ão emocionaldoNHP(r=−0,316;p=0,005;J=0,341).OdomíniovitalidadedoSF-36 estevecorrelacionadocomoníveldeenergiadoNHP(r=−0,362;p=0,001;J=0,302).Para a avaliac¸ãodacapacidadefuncional(ASC=0,839;p<0,001)easpectofísico(ASC=0,755; p<0,001),oinstrumentomaisprecisofoi oHAQ.Paraaavaliac¸ãodoimpactoda vitali-dade,dosono(ASC=0,679;p=0,007),dareac¸ãoemocional(ASC=0,674;p=0,009)edonível deenergianaQV,oNHP(ASC=0,633;p=0,045)foioinstrumentomaisespecíficoe sen-sível.Naavaliac¸ãododomínioaspectoemocional,oinstrumentomaisprecisofoioNHPno domínioreac¸ãoemocional(ASC=0,699;p=0,003).Aavaliac¸ãodadorfoilimitadanostrês instrumentoseoSF-36foioúnicoaavaliarosdomíniosaspectosocialeestadogeralde Saúde.
Conclusão: Paraaavaliac¸ãodoaspectofísicoempacientescomAR,oHAQéoinstrumento maispreciso.Paraaavaliac¸ãodoaspectoemocional,oNHPéomaisindicado,emborao SF-36sejaoúnicoaavaliardomíniosgerais.
©2016PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobuma licenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Rheumatoidarthritisisanautoimmunedisease,ofunknown etiology,characterizedbysymmetricalperipheral polyarthri-tis.This leadstojoint deformity and destruction resulting fromboneandcartilageerosion,1,2 andalmostalwaysleads tofunctionalcompromiseofthestructuresinvolved.3,4 Epi-demiologicalstudieshaveestimatedtheprevalenceofRAat 1%oftheadultpopulation,rangingfrom0.4to1.9%atworld level,andfrom0.5to1.0%inBrazil.5,6RAaffectsthreetimes asmanywomenasmen,withthehighestincidencebetween theagesof30and50years.7,8
The majority of patients will have their independence affectedtovariabledegrees,andtakeillataproductiveage, thusgeneratinglimitationsonsocial,leisureandprofessional activities.1,9–11ThemainsymptomsofpatientswithRAare intensepainandfunctionallimitation,withsignificantimpact onqualityoflife(QoL).12–14Themainobjectivesinthe treat-mentofpatientswithRAaretopreventorcontrolarticular lesions,preventthelossoffunctionanddiminishpain,inan endeavortoimprovetheirqualityoflife.2
Becausethis isachronicdisease,theoutcomeexpected mustnotbeevaluatedbytraditionalepidemiological meas-uresalone,andtherefore,theimpactofthediseaseonQoLhas been adoptedto improve outcome measurements.15,16 The useofspecifictoolsforthispurposeismostvaluable17and variousinstruments havebeenproposed inordertodetect changes inthe stateof healthover the courseof time, in
addition toevaluating the prognosis, risks and benefitsof acertaintherapeuticintervention.5Amongtheinstruments mostusedformakingthisevaluation,theMedicalOutcomes Study, 36-Item Short-Form Health Survey (SF-36), Stanford HealthAssessmentQuestionnaire(HAQ)andtheNottingham HealthProfile(NHP)arethemostoutstanding.However,itis notclearwhichoftheseismostrecommendedfor evaluat-ingthedifferentaspectsofQoLinpatientswhosufferfrom chronicproblemsresultingfromRA.
TheSF-36 isa multidimensional, genericquestionnaire, which has been shown to besuited to the socioeconomic andculturalconditionsoftheBrazilianpopulationinpatients withRA.18Becauseitistheinstrumentmostadoptedin stud-ies atworldlevel byrecommendation ofthe World Health Organization (WHO), it is considered the Gold Standard in the evaluationof QoL.19 The NHP isa generic instrument forevaluationtheQoLofpersonswithdifferentchronic dis-eases,butithasbeenwidelyusedinpatientswithRA.20The HAQisaquestionnairespecificallyforRA,withthepurpose ofquantifyingtheimpactofthedisease onthedaily func-tionsofindividuals.21,22Itmeasuresthelevelofdifficultythe patientpresentsinperformingactivities,aswellastheneed forassistance.4,12,23
generatescores thathave been validatedand are determi-nantfortheevaluationofQoL.15,21However,eachinstrument evaluatesdifferentaspectsofQoLandthechoicefor appli-cationinclinicalpracticeandobservationalstudies,andfor responsestodifferencessometimesbecomesrandom. There-fore,theaimofthepresentstudywastoverifythesensitivity andspecificityoftheinstrumentsusedintheassessmentof QoLinpatientswithRA.
Materials
and
methods
The present accuracy study was conducted in individuals with RA, diagnosed in accordance with the criteria ofthe AmericanCollegeofRheumatology,5who camefroma Ref-erenceOutpatientsClinicfortheTreatmentofCollagenoses, in the municipality of Salvador, Bahia, Brazil. Included in thestudywere individualswithconfirmeddiagnosisofRA, withamoderate orhigh level ofactivityofthe disease,of bothsexes,andageequaltoorover18years.Patientswere excludedwhen theypresentedlimitationinunderstanding theresearchinstruments,andsowerethosewhopresented other associatedchronic,degenerative, neurological, ortho-pedic, pneumological and cardiological diseases, with the potentialofbeingconfoundingelements.
The patients were contacted by telephone, and data obtained from the clinical record charts were used. Data collection wasbased on primary data, and wasperformed inthree stages:(1) blood exam; (2)radiographic exam and (3)applicationofthe questionnaires.Theparticipantswere directedtoaprivateroom,wheretheobjectivesofthestudy andtheproceduresadoptedwereexplainedinastandardized manner.Thefirsttwostagesconstitutedthestageofinclusion ofthevolunteers,inordertodeterminethelevelofdisease activity.Thethirdstageinvolvedtheapplicationofthe spe-cificinstruments.Datawascollectedintheperiodbetween October2011andJuly2012.
TheresearchprojectwasapprovedbytheResearchEthics Committee of the Bahiana School of Medicine and Public Health,ProtocolNo.002/2011andwasconductedin compli-ancewithalltheprinciplesdefinedbyLawDecree196/96of theNationalHealthCouncilwithrespecttoresearchinhuman beings.Subjectswhoagreedtoparticipate,signedtheTermof FreeandInformedConsent.
Toestimatethesamplesizerequiredtoanswerthe ques-tion of the investigation, the following parameters were adopted:standarddeviationof10forthethreecurves(HAQ, SF-36andNHP),erroroftheestimateof2(consideringthe min-imumproximityforthevaluesoftheareaunderthecurve)and alphaof5%.UsingtheLEEon-linecalculatorofUSP(available at http://www.lee.dante.br/cgi-bin/uncgi/calculoamostra) it wasconcludedthat96individualswouldbeneeded.If appli-cationin10individualswereconsideredforeachdomainof theSF-36,whichwasconsideredthegoldstandard,the esti-matedsamplewouldbe80participants.Thusthefinalsample wasestimatedat88individuals(arithmeticmeanof96and80). Whencalculatingalossof9(10%),thesamplewasincreasedto 97.Fromtheclinicalrecordchartdatabaseoftheservice, con-taining456registeredpatients,97participantswererandomly selected,usingarandomnumbertable.Whentheindividual
wasnotavailableonbeingcontacted,ordidnotwishto par-ticipate,thenextnumberonthetablewasincludedinthelist ofparticipantsuntiltheestimatedsizewasattained.
Thesociodemographic characteristics ofeach individual wereevaluatedbymeansofaquestionnairecomposedofthe followinginformation:sex,age,educational level,smoking, alcoholconsumption,bodymassindex(BMI),maritalstatus andsocioeconomicclass,analyzedbytheABEPcriteriaof2008 (Associac¸ãoBrasileiradeInstitutosdePesquisadeMercado)– aBrazilianmarketresearchinstitutethatcategorizes socio-economicconditionsintoeightclasses,from“A1throughto E”,inwhichClass“A1”representsthehighestsocioeconomic level(besthousingqualificationandpatternofconsumption) and“E”,theworst.
Blood was collected to test for the following factors: rheumatoidfactor(RF),C-reactiveprotein(CRP),erythrocyte sedimentationrate(ESR),andantinuclearfactor(ANF).After this, the radiologic exam was performed, which includes radiographsofthewristsandhandsfordiagnostic confirma-tion and identification ofthelevel ofdiseaseactivity.Only patientswithamoderatetohighlevelofdiseaseactivitywere included, whichwasevaluatedbymeans ofusingthe DAS-protocol28.24
ThequestionnairesSF-36(version2.0),NHPandHAQwere usedtoevaluatetheQoL.All theinstrumentswereapplied inauniformmanner, bythesame researchers,andall the recommendations of the authors ofthe instruments were adopted.18,20,21Initially, thequalityoflifedimensions mea-suredbySF-36weredichotomized,usingthemedianascut-off point.Ourapriorihypothesiswasthatwewouldfindpositive correlationsbetweenthefollowingdomainsoftheSF-36and NHP:physicalaspect(SF-36)andphysicalabilities(NHP); vital-ity(SF-36)andenergylevel(NHP);emotionalaspects(SF-36) andemotionalreactions(NHP);andsocialaspect(SF-36)and socialinteraction(NHP).WealsoconsideredthattotalHAQ scorewouldcorrelatepositivelywithallthedomainsofSF-36 andNHP.
Correlation analyses were performed by means of the Pearson linearcorrelation testand receiveroperating char-acteristic (ROC) curve,area underthe curve (AUC) and the YoudenIndex,whichwereusedtoidentifywhichofthe instru-mentswouldbemostspecificandsensitiveforevaluatingQoL in patientswith RA.In the Youden Index(J), the best cut-offpointwasconsideredthatatwhichthelowestnumberof incorrectdiagnoses (falsenegativeplusfalsepositive)were obtained.ThevaluesclosesttoJ=+1wereconsideredthebest methodsfortheevaluationofQoL.Ifthetestdidnothavea diagnosticvalue,theindexwasconsideredequaltozero(J=0). Ifthevalueswerebetween0and−1itwasconsideredthat thetestwasnegativelyassociatedwiththetruediagnosis.25 Thedatawereanalyzedusingthestatisticalsoftwarepackage SPSS,version21.0,adoptinganalphavalueof5%assignificant, withthepowerofthestudyof80%.
Results
Table1–Sociodemographiccharacteristicsofpatients withrheumatoidarthritis.
Variables
n=97
N
Mean
% SD
Gender
Female 90 92.8
Age 52.5 11.0
Skincolor
White 11 11.3
Red 3 3.1
Black 37 38.1
Mulatto 46 47.4
Socialclass(ABEP)
A1 3 3.1
A2 2 2.1
B1 3 3.1
B2 17 17.5
C1 24 24.7
C2 38 39.2
D 10 10.3
Education
Illiterate(upto3rdgrade) 14 14.4
Upto4thGradePrimarySchooling 20 20.6
CompletePrimarySchooling 19 19.6
CompleteHighSchooling 34 35.1
CompletedCollegeEducation 10 10.3
Activitydiseaselevel
Remission 0 0.0
Low 0 0.0
Moderate 31 32.3
High 65 67.7
(47.4%);thesocialclassmostfrequentlycitedwasC2(39.2%) andthemostfrequenteducationallevelwascomplete sec-ondaryeducation(35.1%)(Table1).Thecorrelationsbetween SF-36andthedomainsofNHPandthetotalscoreofHAQare highlightedinTable2.Inordertodetectwhichofthe ques-tionnairespresentedthebestsensitivityandspecificity,ROC curveswerebuilt(Fig.1).Datatodescribetheareaunderthe curve ofeach domain NHPand thetotal scoreofthe HAQ incomparisonwiththedomainsoftheSF-36are shownin
Table3.
The dimension theoretically related to the functional capacity of SF-36 (Fig. 1A) was the total score of HAQ, whichpresentednegativecorrelationinthestudiedsample (r=−0.666; p<0.001) (Table 2). The dimension theoretically relatedtothephysicalaspect(Fig.1B)ofSF-36wasthe phys-icalabilitydomainoftheNHP,whichalsopresentednegative correlation inthestudiedsample (r=−0.240;p=0.033).The dimensiontheoreticallyrelatedtothedimensionpain(Fig.1C) ofSF-36wasthe paindomainoftheNHP,whichpresented nocorrelationwiththeSF-36inthestudiedsample(r=0.210;
p=0.063)(Table2).Aswasobservedinthecorrelationtests, noneofthevariablespresentedasignificantareabelowthe curve.TherearenodimensionsofHAQorNHPtheoretically relatedtothegeneralhealthstatus(Fig.1D)oftheSF-36. Sim-ilarly, inthe studiedsample,noneofthedomainsofthese scalespresentedcorrelationwiththisdomainofSF-36.The dimensiontheoreticallyrelatedtovitality(Fig.1E)ofSF-36was thelevelofenergyoftheNHP,whichpresentednegative corre-lationinthestudiedsample(r=−0.362;p=0.001)(Table2).The dimensiontheoreticallyrelatedtothesocialaspect(Fig.1F)of SF-36was thesocialinteraction domainoftheNHP, which presentedpositivecorrelationinthestudiedsample(r=0.305;
p=0.006),howeverintheoppositedirectiontothatexpected. Thedimensiontheoreticallyrelatedtotheemotionalaspect (Fig.1G)ofSF-36wastheemotionalreactionsdomainofthe NHP,whichpresentednegativecorrelationinthestudied sam-ple(r=−0.316;p=0.005).TherearenodimensionsofHAQor NHPtheoreticallyrelatedtothementalhealthdomain(Fig.1H) oftheSF-36.However,allthescalesoftheNHPandtheHAQ totalscorealsopresentedcorrelationwiththementalhealth oftheSF-36inthestudiedsample(Table2).
Discussion
Thisstudysoughttoverifythesensitivityandspecificityof threeofthemostusedtoolsinassessingtheQualityofLife inpatientswithrheumatoidarthritis.UsingtheSF-36asthe goldstandard,each ofits domainswascomparedwiththe HAQtotalscoreandwiththedifferentdimensionsoftheNHP. Theresultsshowedthattherelationshipsexpectedand con-firmedintheanalyseswereasfollows:“functionalcapacity”
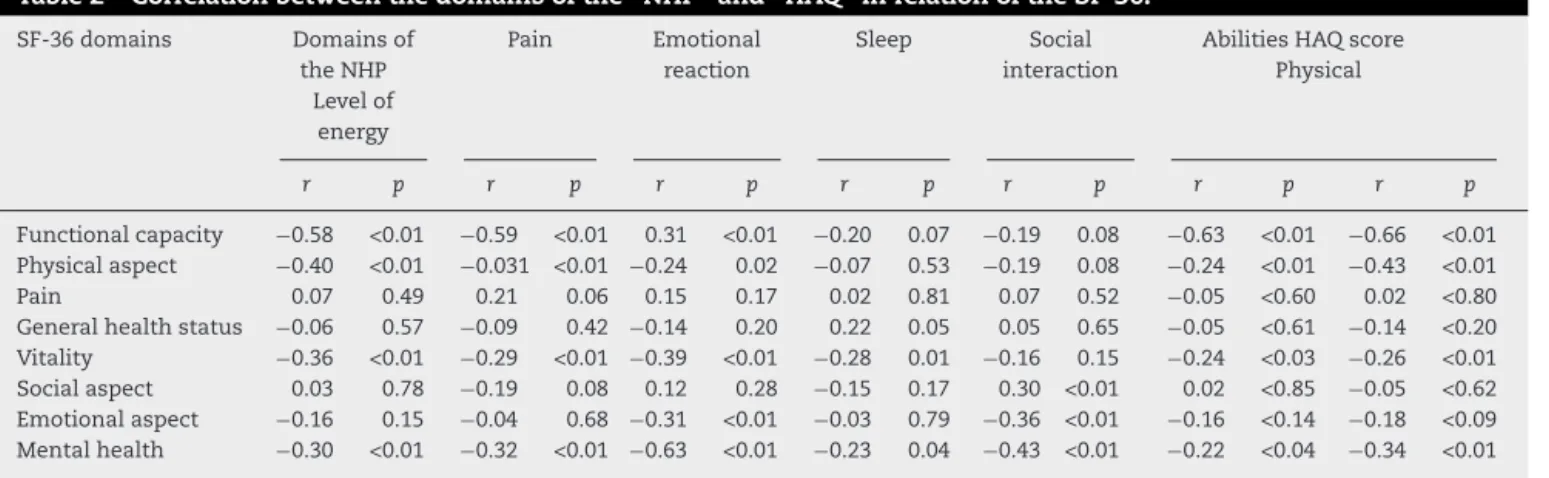
Table2–Correlationbetweenthedomainsofthe“NHP”and“HAQ”inrelationoftheSF-36.
SF-36domains Domainsof theNHP
Levelof energy
Pain Emotional reaction
Sleep Social
interaction
AbilitiesHAQscore Physical
r p r p r p r p r p r p r p
Functionalcapacity −0.58 <0.01 −0.59 <0.01 0.31 <0.01 −0.20 0.07 −0.19 0.08 −0.63 <0.01 −0.66 <0.01 Physicalaspect −0.40 <0.01 −0.031 <0.01 −0.24 0.02 −0.07 0.53 −0.19 0.08 −0.24 <0.01 −0.43 <0.01 Pain 0.07 0.49 0.21 0.06 0.15 0.17 0.02 0.81 0.07 0.52 −0.05 <0.60 0.02 <0.80 Generalhealthstatus −0.06 0.57 −0.09 0.42 −0.14 0.20 0.22 0.05 0.05 0.65 −0.05 <0.61 −0.14 <0.20 Vitality −0.36 <0.01 −0.29 <0.01 −0.39 <0.01 −0.28 0.01 −0.16 0.15 −0.24 <0.03 −0.26 <0.01 Socialaspect 0.03 0.78 −0.19 0.08 0.12 0.28 −0.15 0.17 0.30 <0.01 0.02 <0.85 −0.05 <0.62 Emotionalaspect −0.16 0.15 −0.04 0.68 −0.31 <0.01 −0.03 0.79 −0.36 <0.01 −0.16 <0.14 −0.18 <0.09 Mentalhealth −0.30 <0.01 −0.32 <0.01 −0.63 <0.01 −0.23 0.04 −0.43 <0.01 −0.22 <0.04 −0.34 <0.01
1.0
0.8
0.6
0.4
0.2
0.0
1.0
0.8
0.6
0.4
0.2
0.0 0.0 0.2 0.4 0.6
Sensitivity Sensitivity
ROC Curve ROC Curve
A
C
D
B
1-specificity
Sensitivity
ROC Curve
1-specificity
Sensitivity
ROC Curve
1-specificity 1-specificity
Source of the curve Energy level Pain
Emotional reaction
Social interaction Sleep
Physical abilities HAQ score Reference line
Energy level Pain
Emotional reaction
Social interaction Sleep
Physical abilities HAQ score Reference line
Source of the curve
Source of the curve Energy level Pain
Emotional reaction
Social interaction Sleep
Physical abilities HAQ score Reference line
Energy level Pain
Emotional reaction
Social interaction Sleep
Physical abilities HAQ score Reference line Source of the
curve
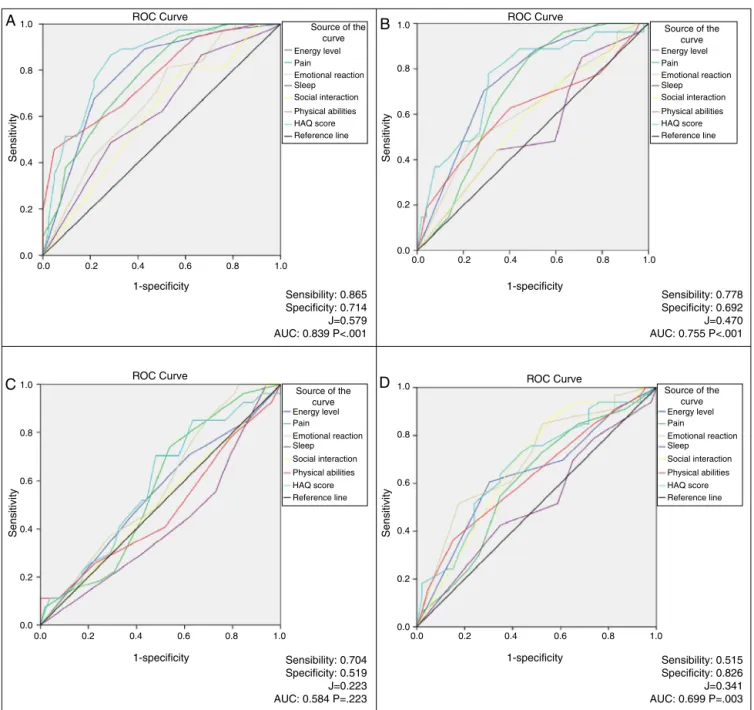
Sensibility: 0.865 Specificity: 0.714 J=0.579 AUC: 0.839 P<.001
Sensibility: 0.704 Specificity: 0.519 J=0.223 AUC: 0.584 P=.223
Sensibility: 0.515 Specificity: 0.826 J=0.341 AUC: 0.699 P=.003 Sensibility: 0.778 Specificity: 0.692 J=0.470 AUC: 0.755 P<.001
0.8 1.0 0.0 0.2 0.4 0.6 0.8 1.0
1.0
0.8
0.6
0.4
0.2
0.0
0.0 0.2 0.4 0.6 0.8 1.0
1.0
0.8
0.6
0.4
0.2
0.0
0.0 0.2 0.4 0.6 0.8 1.0
Fig.1–CurvesROCforsensibilityandspecificitymeasureofinstrumentstoassessqualityoflifeinrheumatoidarthritis individuals.(A)Functionalcapacitydomain;(B)physicalaspectdomain;(C)generalhealthdomain;(D)emotionalaspect domain.
withthe“HAQTotalScore”;“emotionalaspect” with “Emo-tionalRelationships”oftheNHP;and“vitality”withthe“level ofenergy”oftheNHP.
Bothgeneric andspecific instrumentsare importantfor studying the health-related aspects of quality of life in rheumatoidarthritis.Genericinstruments,suchastheSF-36 andNHPmayallowcomparisonwithothergroupsof individ-uals,however,theymayhavelowsensitivitytothechanges infollow-upstudies.20Whereas,specificinstruments,suchas theHAQaremoresensitivetochangesinhealthstatus, how-ever,theirresultsmaynotbecomparedwiththeresultsof othergroups.26
Themajorityofthesampleofthisstudywasmadeupof women(9:1)andwassimilartothefindingsofvariousstudies
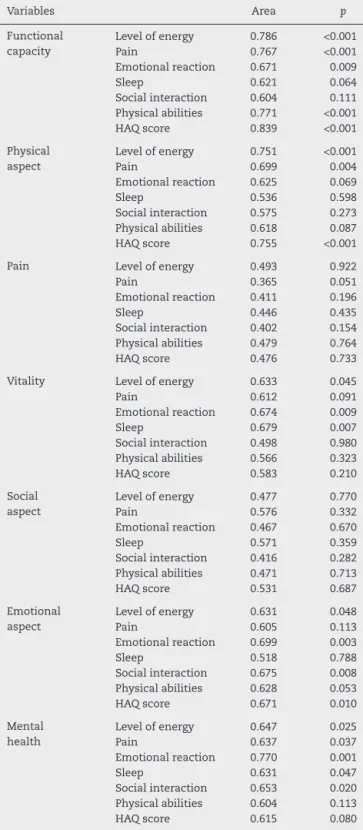
Table3–AreaundertheROCcurveinthedomainsof SF-36incomparisonwiththeaspectsofNHPandtotal scoreofHAQ.
Variables Area p
Functional capacity
Levelofenergy 0.786 <0.001
Pain 0.767 <0.001
Emotionalreaction 0.671 0.009
Sleep 0.621 0.064
Socialinteraction 0.604 0.111 Physicalabilities 0.771 <0.001
HAQscore 0.839 <0.001
Physical aspect
Levelofenergy 0.751 <0.001
Pain 0.699 0.004
Emotionalreaction 0.625 0.069
Sleep 0.536 0.598
Socialinteraction 0.575 0.273 Physicalabilities 0.618 0.087
HAQscore 0.755 <0.001
Pain Levelofenergy 0.493 0.922
Pain 0.365 0.051
Emotionalreaction 0.411 0.196
Sleep 0.446 0.435
Socialinteraction 0.402 0.154 Physicalabilities 0.479 0.764
HAQscore 0.476 0.733
Vitality Levelofenergy 0.633 0.045
Pain 0.612 0.091
Emotionalreaction 0.674 0.009
Sleep 0.679 0.007
Socialinteraction 0.498 0.980 Physicalabilities 0.566 0.323
HAQscore 0.583 0.210
Social aspect
Levelofenergy 0.477 0.770
Pain 0.576 0.332
Emotionalreaction 0.467 0.670
Sleep 0.571 0.359
Socialinteraction 0.416 0.282 Physicalabilities 0.471 0.713
HAQscore 0.531 0.687
Emotional aspect
Levelofenergy 0.631 0.048
Pain 0.605 0.113
Emotionalreaction 0.699 0.003
Sleep 0.518 0.788
Socialinteraction 0.675 0.008 Physicalabilities 0.628 0.053
HAQscore 0.671 0.010
Mental health
Levelofenergy 0.647 0.025
Pain 0.637 0.037
Emotionalreaction 0.770 0.001
Sleep 0.631 0.047
Socialinteraction 0.653 0.020 Physicalabilities 0.604 0.113
HAQscore 0.615 0.080
HAQ,StanfordHealthAssessmentQuestionnaire;NHP,Nottingham HealthProfile;ROC,ReceiverOperatingCharacteristicCurve;SF-36, ShortForm-36item.
studiespointstothepossibilityofextrapolatingthefindings toothersamples.
Inthisstudyitwaspossibletoobservethatinorderto eval-uatefunctional capacity,thebest instrument wasthe HAQ totalscore,whichpresentedthelargestareaundertheROC
curve,withelevatedsensitivityandspecificity.Thisresultwas expected,sincetheitemsofthescalethatmeasuresthe func-tional capacity of the HAQare related todependence and functional incapacity,and these patients presented impor-tantjointdamagewithlossoffunction.18,20 Inthestudyof Ciconelli,18thesignificantcorrelationsoccurredbetweenthe functionalcomponentoftheF-36andtheaspectsofmobility and pain ofthe NHP. Inthe study ofGarip,8 the question-naire Quality of Life in Rheumatoid Arthritis (RAQol) was comparedwiththeotherscales,anditwasobservedthatthe RAQolshowedhighcorrelationwiththeHAQ.TheHAQisa toolcapableofreflectingtheevolutionalconditionofthe dis-ease,objectivelyevaluatingthefunctional stateofpatients, and maypossibly beuseful forfollowing-upthefunctional responsetotreatment.21,32
Withregard tothe physicalaspectdomain ofthe SF-36, both the physical ability of NHP and the HAQ total score were shown to be efficient in determining the impact of physicallimitationscausedbyRA,allowinganyofthethree instruments tobeused.However,it wastheHAQthat pre-sentedthelargestareaunderthecurve,andisthereforethe instrument most indicatedforthis evaluation. In an accu-racystudyusingtheCedars-SinaiHealth-RelatedQualityof LifeforRheumatoidArthritisInstrument(CSHQ-RA),the SF-36andHAQdemonstratedthattheitemsrelativetophysical incapacity were strongly correlated withthe HAQand the physicalcomponentoftheSF-36.33Ourfindingsarein agree-mentwiththeresultsofthestudyofGarip,8inwhichallthe subgroups ofthe NHP presentedhigh correlation with the HAQ.
Whereas, in the evaluation of pain, which has specific domainsinbothSF-36andNHP,itwasnotpossibletoverify anycorrelationinthesampleofthisstudy.Thesubjectivity of multiplefactors involved inthe perceptionof pain ina chronicmorbiditysuchasRAmaypossiblybelimiting fac-torsfortheuseoftheseinstrumentsinthisevaluation.This resultmayalsoberelatedtothefrequentuse ofmodifying drugs,analgesicsandstrictcontrolofinflammatoryactivity inthesepatientsduringthecourseofthedisease,factorsthat mayinfluencethisdomain.20
Itwasalsonotpossibletofindany theoreticalbasisfor comparisonofthe generalhealth statusofSF-36with any scaleoftheNHPortotalscoreofHAQ.Thisfactpointsout theneedforelaborationanddevelopmentofinstrumentsfor evaluatingthisdomaininpopulationswithRA.Thisfinding alsosuggeststhatcaremustbetakenwhenusingthetotal scoreoftheinstruments,sincethedomainssuchasthesemay influencethefinalresult.
WithregardtothevitalityaspectoftheSF-36,therewas highcorrelationwiththeitemsleepoftheNHP,followedby theemotionalreactionandlevelofenergy.Thisfindingmay berelatedtothefactthatinchronicdiseaseswith incapaci-tatingcharacteristics,highlylinkedtodepressionandanxiety, itiscommontofindassociatedsleepdisturbances.20Patients considerthedimensionsenergy/vitalityandsleepimportant intheimpactonQoLanddevelopmentofthedisease,and thisisanadvantagewithregardtouseoftheNHPandSF-36 instruments.26
maybeinfluencedbysemanticaspectswhichdeservemore in-depthstudies.InthestudyforvalidationoftheSF-36inthe Portugueselanguage,inpatientswithRA,highermean val-ueswerefoundforthecomponentssocialaspectsandmental health.18Thedomainthatevaluatessocialissueshas limita-tionsasregardsthevalidityoftheclinicalapplicationinboth instruments.20
With regard to the emotional aspect of the SF-36, cor-relation was found with the emotional reaction scale of theNHP, and thispresentedalarger areaunderthe curve. This result is consistent with the tendency to present depression and anxiety.1 Lillegraven and Kvien26 revealed thatthe emotionalaspect andemotionalreactiondomains were similar dimensions. A negative correlation was also observedwiththesocialinteractionscale(NHP)andthe sec-ond highest area under the curve, which may clearly be justified, because the patient’s emotional state may have an influence on his/her social relationships and make it possible for him/her to have a tendency toward seeking isolation.20Thethreeinstrumentspresentedgoodconditions forevaluatingthis aspect,however, the NHPwasthe most suitable.
Withregardtomentalhealth,thevariablethatpresented thelargestareaunderthecurvewasemotionalreaction(NHP) andthisfindingcorroboratesthestudyofCiconelli,18which demonstratedgoodcorrelationbetweentheNHPandSF-36in thisdomain.
Theresultsofthepresentstudyindicatedthatmany stud-iesmuststillbedevelopedbeforeindiscriminateuseismade ofinstrumentsforevaluatingtheimpactonthequalityoflife inpersonswhosufferdamagetotheirhealth.Personsaffected bychronicdiseases,such asinthe caseofRA,need tobe constantlyfollowed-up,notonlyasregardstheevolutionof objectiveclinicalparameters,butmainlywithregardtothe subject’sperception,involvingbiopsychosocialaspectsofthe health-diseaseprocess.
Animportantlimitationofthisstudywastheabsenceof aprospectivereassessmentofparticipantstoestimate sen-sitivitytochangeinQoL.Thislimitationwasconsequentto thelackofadherencebytheparticipants,whichdidnotwant tocomebacktoasecondassessmentwiththesame instru-ments.
Themainconclusionofthisstudyisthatthethree instru-ments most used in the evaluation of the impact on QoL ofthe morbidityofRA, validated and availablein the Por-tuguese language of Brazil, namely: SF-36, HAQ and NHP – are useful and should beapplied in clinical studies and scientificresearches.Alloftheseinstrumentsdemonstrated good sensitivity and specificity in the major part of the domainsevaluated.However,itisalsopossibletoconclude thatforevaluationofphysicalandsubjectiveaspects, differ-encesinaccuracybetweenthemmayindicatedifferentiated choicesfortheir application.For evaluationofthe physical aspectsinpatients withRA,the HAQisthe mostaccurate. For evaluation of emotional aspects the NHP is the most indicated.SF-36,HAQandNHPareeasytounderstand, auto-applicableandquicktofill(<10mineach),andmaybeused inclinicalandresearchsettings.However,theimpactofpain on QoLwas not well evaluated byany ofthe instruments tested.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.MotaLM,CruzBA,BrenolCV,PereiraIA,FronzaLS,Bertolo MB,etal.ConsensusoftheBrazilianSocietyofRheumatology fordiagnosisandearlyassessmentofrheumatoidarthritis. RevBrasReumatol.2011;51:199–219.
2.BertoloMB,BrenolCV,SchainbergCG,NeubarthF,LimaFAC, LaurindoIM,etal.UpdateontheBrazilianConsensusforthe diagnosisandtreatmentofrheumatoidarthritis.RevBras Reumatol.2007;47:151–9.
3.BoydTA,BonnerA,ThorneC,BoireG,HitchonC,HaraouiBT, etal.Therelationshipbetweenfunctionanddiseaseactivity asmeasuredbytheHAQandDAS28variesovertimeandby rheumatoidfactorstatusinearlyinflammatoryarthritis(EIA). ResultsfromtheCatchCohort.OpenRheumatolJ.
2013;7:58–63.
4.CostaGP[dissertac¸ãodemestrado]Confiabilidadeda autoaplicac¸ãodoHealthAssessmentQuestionnaire Modificado(HAQ-M)emumapopulac¸ãodeportadoresde artritereumatoidenoBrasil.Brasília:FaculdadedeMedicina daUniversidadedeBrasília;2006.
5.MotaLM,CruzBA,BrenolCV,PereiraIA,Rezende-FronzaLS, BertoloMB,etal.Consenso2012daSociedadeBrasileirade Reumatologiaparaotratamentodaartritereumatoide.Rev BrasReumatol.2012;52:135–74.
6.SennaER,BarrosALP,SilvaEO,CostaIF,PereiraLV,Ciconelli RM,etal.PrevalenceofrheumaticdiseasesinBrazil:astudy usingtheCopcordapproach.JRheumatol.2004;31:3.
7.SorensenJ,LindeL,OstergaardM,HetlandML. Quality-adjustedlifeexpectanciesinpatientswith rheumatoidarthritis–comparisonofindexscoresfrom EQ-5D,15D,andSF-6D.ValueHealth.2012;15:334–9.
8.GaripY,EserF,BodurH.Health-relatedqualityoflifein rheumatoidarthritis:comparisonofRAQoLwithotherscales intermsofdiseaseactivity,severityofpain,andfunctional status.RheumatolInt.2011;31:769–72.
9.MendesM,KowalskiSC,CiconelliRM,FerrazMB.Evaluation ofthesociodemographic,clinical-laboratorialandtherapeutic profileofrheumatoidarthritispatientswhoparticipatedof researchprojectsintheEscolaPaulistadeMedicinainthe last25years.RevBrasReumatol.2006;46:103–9.
10.SokkaT,KautiainenH,PincusT,VerstappenSM,AggarwalA, AltenR,etal.Workdisabilityremainsamajorproblemin rheumatoidarthritisinthe2000s:datafrom32countriesin theQUEST-RAstudy.ArthritisResTher.2010;12:R42.
11.ChehataJC,HassellAB,ClarkeSA,MatteyDL,JonesMA,Jones PW,etal.Mortalityinrheumatoidarthritis:relationshipto singleandcompositemeasuresofdiseaseactivity. Rheumatology.2001;40:447–52.
12.StanmoreE,OldhamJ,SkeltonDA,O’NeillT,PillingM, CampbellAJ,etal.Riskfactorsforfallsinadultswith rheumatoidarthritis:aprospectivestudy.ArthritisCareRes. 2013;65:1251–8.
13.AletahaD,NeogiT,SilmanAJ,FunovitsJ,FelsonDT,Bingham CO,etal.Rheumatoidarthritisclassificationcriteria:an AmericanCollegeofRheumatology/EuropeanLeagueAgainst Rheumatismcollaborativeinitiative.ArthritisRheum. 2010;62:2569–81.
15.WolfeF,MichaudK.Thelossofhealthstatusinrheumatoid arthritisandtheeffectofbiologictherapy:alongitudinal observationalstudy.ArthritisResTher.2010;12:R35.
16.BrandãoL,FerrazMB,ZerbiniCAF.Evaluationofqualityoflife inrheumatoidarthritis.RevBrasReumatol.1997;37:275–81.
17.GroenMM,KloosterPM,TaalE,LaarMAFJ,GlasCAW. Applicationofthehealthassessmentquestionnairedisability indextovariousrheumaticdiseases.QualLifeRes.
2010;19:1255–63.
18.CiconelliRM,FerrazMB,SantosW,MeinãoI,QuaresmaMR. Brazilian-PortugueseversionoftheSF-36.Areliableandvalid qualityoflifeoutcomemeasure.RevBrasReumatol.
1999;39:143–50.
19.CampolinaAG,BortoluzzoAB,FerrazMB,CiconelliRM. ValidationoftheBrazilianversionofthegeneric six-dimensionalshortformqualityoflifequestionnaire (SF-6DBrazil).CiêncSaúdeColetiva.2011;16:3103–10.
20.Teixeira-SalmelaLF,MagalhãesLC,SouzaAC,LimaMC, GoulartF.AdaptationoftheNottinghamHealthProfile:a simplemeasuretoassessqualityoflife.CadSaúdePública. 2004;20:905–14.
21.FriesJF,SpitzPW,KrainsRG,HolmanHR.Measurementof patientoutcomeinarthritis.ArthritisRheum.1980;23:137–45.
22.PincusT,SokkaT.Furtherdevelopmentofaphysicalfunction scaleonaMHAQ(corrected)forstandardcareofpatients withrheumaticdiseases.JRheumatol.2005;32:1432–9.
23.MaskaL,AndersonJ,MichaudK.Measuresoffunctional statusandqualityoflifeinrheumatoidarthritis.Arthritis CareRes.2011;63:S4–13.
24.PinheiroGR.Pooledindicestomeasurerheumatoidarthritis activity–whyandhowtousethem.RevBrasReumatol. 2007;47:362–5.
25.JalaliR,RezaieM.Predictingpressureulcerrisk:comparing thepredictivevalidityof4scales.AdvSkinWoundCare. 2005;18:92–7.
26.LillegravenS,KvienTK.Measuringdisabilityandqualityof lifeinestablishedrheumatoidarthritis.BestPractResClin Rheumatol.2007;21:827–40.
27.MotaLM,LaurindoIM,SantosNetoLL.Características demográficaseclínicasdeumacoortedepacientescom artritereumatoideinicial.RevBrasReumatol.2010;50: 235–48.
28.SmolenJS,LandewéR,BreedveldFC,DougadosM,EmeryP, Gaujoux-VialaC,etal.EULARrecommendationsforthe managementofrheumatoidarthritiswithsyntheticand biologicaldisease-modifyingantirheumaticdrugs.Ann RheumDis.2010;69:964–75.
29.CruyssenBV,DurezP,WesthovensR,DeKeyserF.Seven-year follow-upofinfliximabtherapyinrheumatoidarthritis patientswithseverelong-standingrefractorydisease: attritionrateandevolutionofdiseaseactivity.ArthritisRes Ther.2010;12:R77.
30.Louzada-JuniorP,SouzaBDS,ToledoRA,CiconelliRM. Descriptiveanalysisofthedemographicalandclinical characteristicsofthepatientswithrheumatoidarthritis intheStateofSãoPaulo,Brazil.RevBrasReumatol. 2007;47:84–90.
31.AktekinLA,EserF,BaskanBM,SivasF,MalhanS,ÖksüzE, etal.Disabilityofarmshoulderandhandquestionnairein rheumatoidarthritispatients:relationshipwithdisease activity,HAQ,SF-36.RheumatolInt.2011;31:823–6.
32.BruceB,FriesJF.TheHealthAssessmentQuestionnaire (HAQ).ClinExpRheumatol.2005;23Suppl.39:S14–8.
33.ChiouCF,SherbourneCD,CornelioI,LubeckDP,PaulusHE, DylanM,etal.DevelopmentandvalidationoftheRevised Cedars-SinaiHealth-RelatedQualityofLifeforRheumatoid ArthritisInstrument.ArthritisCareRes.2006;55: