REVISTA
BRASILEIRA
DE
REUMATOLOGIA
ww w . r e u m a t o l o g i a . c o m . b r
Review
article
Influence
of
physical
activity
on
quality
of
life
in
postmenopausal
women
with
osteoporosis
Eduardo
Lucia
Caputo
∗,
Marcelo
Zanusso
Costa
UniversidadeFederaldePelotas,Pelotas,RS,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received27August2013 Accepted18February2014 Availableonline22October2014
Keywords:
Osteoporosis Qualityoflife Physicalactivity
a
b
s
t
r
a
c
t
The objectiveofthisstudy istoconduct areview ontheassociationbetweenexercise andqualityoflifeinpostmenopausalwomenwithosteoporosis.Asearchwasperformed inPubMed,SciELO,SpringerLinkandSportDiscusdatabasestoidentifyrelevantarticles thataddressedthisassociation.WeusedthefollowingdescriptorsintheEnglishand Por-tugueselanguages:osteoporosis,exercise,menopause,women,physicalactivity,qualityof life/osteoporose,exercíciofísico,menopausa,mulheres,atividadefísica,qualidadedevida.Regarding qualityoflifeandphysicalaspectslikemusclestrengthandbalance,withtheexceptionof twostudies,allothershavereportedimprovementinqualityoflifeandinphysicaldomain ofparticipants.Interventionwithexercisehasprovedessentialtoimprovingthequalityof lifeofwomenwithpostmenopausalosteoporosis.Activitiesthataimattheimprovement ofmusclestrengthandbalanceareessentialtopreventfalls,andconsequentlytoreduce theincidenceoffracturesinthispopulation.
©2014ElsevierEditoraLtda.Allrightsreserved.
Influência
do
exercício
físico
na
qualidade
de
vida
de
mulheres
pós-menopáusicas
com
osteoporose
Palavras-chave:
Osteoporose Qualidadedevida Exercíciofísico
r
e
s
u
m
o
Oobjetivodestetrabalhoérealizarumarevisãosobreaassociac¸ãoentreexercíciofísicoe qualidadedevidaemmulherespós-menopáusicascomosteoporose.Foirealizadabusca nasbasesdedadosPubMed,Scielo,SpringerLinkeSportDiscusafimdeidentificarartigos relevantesquetratassemdessaassociac¸ão.Utilizaram-seosseguintesdescritores,em lín-guainglesaeportuguesa:osteoporosis,exercise,menopause,women,physicalactivity,qualityof life/osteoporose,exercíciofísico,menopausa,mulheres,atividadefísica,qualidadedevida. Comrelac¸ãoàqualidadedevidaeaspectosfísicoscomoforc¸aeequilíbrio,comexcec¸ão dedoisestudosencontrados,osdemaisrelatarammelhorianaqualidadedevidaenos
DOIoforiginalarticle:http://dx.doi.org/10.1016/j.rbr.2014.02.008.
∗ Correspondingauthor.
E-mailaddresses:[email protected],[email protected](E.L.Caputo).
http://dx.doi.org/10.1016/j.rbre.2014.02.021
indicadoresfísicosdasparticipantes.Aintervenc¸ãocomexercíciofísicodemonstrouser fundamentalparaoaprimoramentodaqualidadedevidademulheresnapós-menopausa quesofremdeosteoporose.Atividadesquetêmporobjetivooaperfeic¸oamentodaforc¸aedo equilíbriosãoessenciaisparaevitaraocorrênciadequedase,consequentemente,reduzir aincidênciadefraturasnessapopulac¸ão.
©2014ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Osteoporosis isa systemic skeleton disease, being
charac-terizedby reducedbone density and deteriorationof bone
tissuearchitecture.1 Thisdisease hasahigherincidencein
thefemalepopulation,duetothelowerpeakbonemassin
thisgroup,andtotheconsequencesofmenopause.2
Menopause is a period of transformation in women’s
lives,in which theyare confrontedwith medicaland
psy-chologicalproblems. Inaddition ofhotflushes, headaches, sweating,fatigue,sexualdysfunctionandreductionof
estro-gen,menopausemaycauseamassiveandrapidlossofbone
mass.3
Onceestablishedthemenopause,theprevalenceof
osteo-porosis and related fractures increases according to the
durationofthishormonaldisorderandthewoman’sage.4In
thispopulation,theprevalenceofosteoporosisatthelumbar spinerangesfrom15.8%inwomenaged50-59yearsto54.5% inwomenover80years,andtheprevalenceoffracturesvaries between20%and82%forthesameagegroups,respectively.5
AccordingtotheNorthAmericanMenopauseSociety,the
mainclinicalobjectivewhentreatingosteoporosisistoreduce thefracturerisk.6Theresultingpainofthischangeinbody
imageandthelossofmobilityandindependencecanhavea
strongimpactonself-esteemandinthemood,makingthe
preventionof fallsthe mainpoint in preventing fractures.
Inthewomenwithpostmenopausalosteoporosis,the
preva-lenceoffallsispostmenopausal51.1%against29.3%ofwomen withoutosteoporosis.7
Theincreaseinlifeexpectancyofthepopulationandthe costsgeneratedbyfractures,especiallyhipfractures,
deter-mine theimportance ofstudyingthis disease,becausehip
fracturespresentwithgreatermorbidityandmortality.8
Physicalactivityplaysakeyroleinosteoporosis,mainlyby reducingboneresorption.9Theincreaseinmusclestrength,
stability,balanceandmobility,improvementofthequalityof life,reductionofpainandpreventionoffallssupplementthe benefitsgeneratedbythesystematicpracticeofexercisein patientswithosteoporosis.10
Theaimofthisarticleistoconductareviewonthe associ-ationbetweenexerciseandqualityoflife,inthepsychological
andphysicaldomains,inpostmenopausalwomenwith
osteo-porosis.
Methodology
A systematic search was conducted and relevant articles
thatanalyzedtheinfluenceofastructuredexercisetraining
program onqualityoflifeinpostmenopausalwomenwith
osteoporosiswereselected.Thesesanddissertationswerenot includedduetothelogisticinfeasibilityofasystematicsearch
throughthesedocuments.
Those publications that met the inclusion criteria were
evaluated, regardless of the journal nature. The selection ofdescriptorsusedthroughoutthereviewprocess was
per-formed according to a Medical Subject Headings (MeSH)
consultation.
AsearchwasconductedinPubMed,SciELO,SpringerLink
and Sport Discusdatabases and inthe references ofthose
identifiedarticles.SearchtermsinEnglishandPortuguese lan-guagesincluded:osteoporosis,exercise,menopause,women, physical activity, quality of life/ osteoporose, exercício físico, menopausa, mulheres, atividade física, qualidade de vida. In
order to combine the descriptors and terms used in the
search, we resorted to the logical operators “AND” and
“OR”.
Atfirst,135articlesthatpresentedarelationtothestudy subjectwereidentified.Then,weselectedthosearticlesthat met the followinginclusioncriteria: a)longitudinalstudies
includingpostmenopausalwomenwithosteoporosis;andb)
withaclinicaldiagnosisofosteoporosisobtainedby
exam-inationofbonedensitometryinthefemoralneckorlumbar
spine,andwithnohistoryofatraumaticfracture.Theselected articles were analyzed according to the following criteria establishedbyDowns&Black:11
• Hypothesesandobjectivesofthestudy
• Mainoutcomesmeasured
• Characteristicsofthesubjectsinvolved
• Descriptionoftheinterventionsofinterestandmain
out-comes
• Descriptionoftheactualvaluesforthemainoutcomes
• Adequacyofappropriatestatisticaltests
• Whetherthemeasuresusedforthemainoutcomeswere
accurate
• Whether the patients in different groupswere recruited
fromthesamepopulation
• Whether the main resultspresented sufficient power to
detectanimportanteffectwheretheprobabilityvaluefora differencebeingduetoachanceoflessthan5%
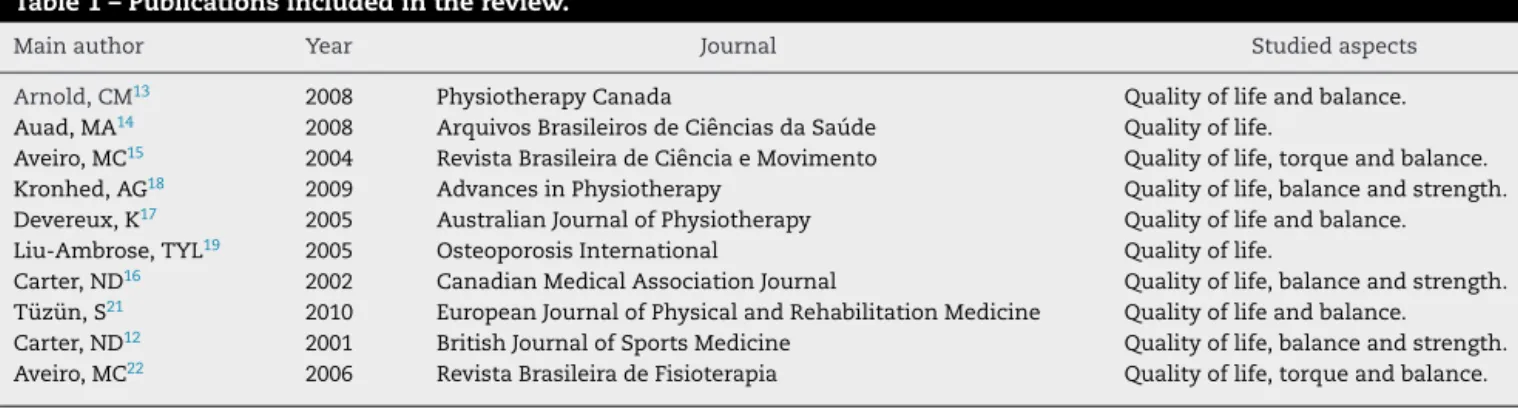
Table1–Publicationsincludedinthereview.
Mainauthor Year Journal Studiedaspects
Arnold,CM13 2008 PhysiotherapyCanada Qualityoflifeandbalance.
Auad,MA14 2008 ArquivosBrasileirosdeCiênciasdaSaúde Qualityoflife.
Aveiro,MC15 2004 RevistaBrasileiradeCiênciaeMovimento Qualityoflife,torqueandbalance.
Kronhed,AG18 2009 AdvancesinPhysiotherapy Qualityoflife,balanceandstrength.
Devereux,K17 2005 AustralianJournalofPhysiotherapy Qualityoflifeandbalance.
Liu-Ambrose,TYL19 2005 OsteoporosisInternational Qualityoflife.
Carter,ND16 2002 CanadianMedicalAssociationJournal Qualityoflife,balanceandstrength. Tüzün,S21 2010 EuropeanJournalofPhysicalandRehabilitationMedicine Qualityoflifeandbalance. Carter,ND12 2001 BritishJournalofSportsMedicine Qualityoflife,balanceandstrength. Aveiro,MC22 2006 RevistaBrasileiradeFisioterapia Qualityoflife,torqueandbalance.
Results
Table 1shows the publications that were included in this review.Amongthecriteria establishedforouranalysis,the clarityinthedescriptionoftheobjectiveswascompromised onlyinthestudybyCarteretal.12Withrespecttothestudied
outcomes,thequalityoflifewasmeasuredin10studies.12–21
Theotheroutcomesstudiedwere:balance,12,13,15–17,21–23
mus-cletorque,15lowerlimbstrength,12,16,22 gaitspeed,22fearof
falling,17frequencyoffalls,23respiratoryfunction,postureand
submaximalexercisecapacity.20
Thecharacteristics ofthesubjectswere presentedusing descriptivetablesinnine studies.12,13,16,19–23 Thestudiesby
Auadetal.,14Aveiroetal.15andDevereuxetal.17presentthis
informationonthetext,intheResultssection,havingonly theparticipants’ageasadescriptivevariable.Mostauthors measuredthequalityoflifeusingspecificquestionnaires;12–21
however,onlytwoofthemevaluatedvariablessuchaspain andnumberoffalls.18,23
Ofthestudiesevaluated,onlythatofCarteretal.16included
confoundingfactorsintheselectionandanalysisofdata.They were:height,weight,weightchangeduringthestudy,yearsof
estrogenuse,numberofmedicationstaken,smoking,
phys-icalactivity,age,mentalstate,qualityoflifescore,number offracturesthroughoutlife,numberoffallsinthelastyear and the presence ofosteoarthritis or rheumatoid arthritis. Onlyonestudydescribesadverseeventsoftheintervention inparticipants.19
Because of ethical and methodological difficulty
issues, four studies reported attempts of participants’
blinding,12,16,19,23 and three studies did not undergo
randomization.15,20,22
Table2presentstheresultsofstudiesthatevaluatedthe qualityoflifeinwomen withosteoporosis.Onlythe study byCarteretal.16foundnobeneficialeffectsofexercise
inter-ventiononqualityoflifeofthe womenstudied.Theother selectedstudiesdemonstrateapositiveimpactofthis inter-ventiononthequalityoflifeofthewomenstudied.Overall, theinterventionwithexercisehadapositiveeffectonthe fol-lowing:generalhealth,interaction,globalscores,bodyimage, activitiesofdailyliving,vitality,socialfunctionand mental health.
Muscle strength and balance were the most evaluated
physicalabilities.InexaminingTable3,itispossibletoverify thattheexerciseplaysanimportantroleinimprovingthese abilities,as theyarekey componentsforthe preventionof
falls.Twostudiesshowednoincreaseintheseabilitiesinthe groupperformingexercise.
Discussion
Osteoporosis negativelyaffects the patients’ qualityoflife, limiting their performancein activitiesofdaily living.The chronicpain generatedbyosteoporosiscanleadto depres-sion,anxiety,frustrationandsocialisolation.24Then,exercise
practicebecomesacrucialintervention,byincreasingthe con-fidenceofthewomantoindependentlyperformhertasks.14
Inadditiontoareductioninboneloss,theregularpractice
of exercise by women with osteoporosis has, as positive
effects, overallhealth, socialization,self-esteem,moodand
bodyawarenessimprovement;andreductionofdepression,
anxiety and fear of falls.13,17 Also, the family knowledge
aboutthediseasehascriticalimportance,becauseitgenerates greaterfamilysupportforthepatienttotreatherillness.15.
In the study byLiu-Ambroseetal.,19 the authors report
thatexercisesperformedinpairsincreasedthesocial interac-tionbetweentheparticipants.Thiseffect,especiallyamong the elderlywithsimilarhealthstatus,isrelatedtothe fact thatexercisespracticedingroupprovidetoitsparticipants thesharelifeexperiences,newfriendshipsandanincreased senseofwell-being,thatinfluencepositivelyontheir perma-nenceintheprogram.18
Theoccurrenceoffractureshasastrongereffectin reduc-ingthequalityoflife,comparedjusttotheillnessitself.22,25A
hipfracture,forinstance,generatesasignificantreductionin qualityoflifeofaffectedindividualsinaperiodof12-15weeks afterthefracture.26Postmenopausalwomenwith
osteoporo-siswhodonotexhibitcomplicationscausedbythedisease andarephysicallyactivehavesimilarqualityoflifeto
post-menopausalwomenwithoutosteoporosis.27,28
Only the studies byCarter et al.12 and Kronhed et al.18
reportednosignificantimprovementinthephysicaldomains
of osteoporotic women after the intervention, both when
comparedtoacontrolgroupaswhencomparedtobaseline
values. Although notindicating significant changes in bal-anceandkneeextensionstrengthafter10weeksoftraining, Carteretal.12statethattheparticipantsoftheexercisegroup
showedanincreaseinkneeextensionstrengththat,despite notbeingofstatisticalsignificance,hasimportantbiological significance.However,thestudybyCarteretal.16maintained
Table2–Resultsofstudiesevaluatingthequalityoflifeinwomenwithosteoporosis.
Author Instrumentused Exerciseprotocol Result
Arnoldetal.200813 OQLQ-OsteoporosisQualityofLife Questionnaire
Threegroupsdividedinto:agroup thatperformedexercisesinthe water,agroupwhichperformed exercisesoutofwateranda controlgroup.Thefirsttwogroups performedthreeweeklysessions lasting50minuteseach,for20 weeks.
Subjectsinthegroupthat performedexerciseoutofwater presentedabetterOQLQtotal score,whencomparedtothe groupthatdidexercisesinthe water.However,theglobalscores reportedbysubjectsinthegroup thatexercisedinwaterwasthree timeshighercomparedtothe groupthatexercisedoutofwater. Auadetal.200814 OPAQ-OsteoporosisAssessment
Questionnaire
Twogroups:controlandexercise. Thesecondgroupundertooka programofexercise,witha frequencyoftwiceaweeksessions lastingonehoureach,foreight months.
Thegroupthatpracticedexercise showedimprovementinthe generalhealth,physicaland psychologicaldomains,social interaction,symptoms,workand bodyimage,whencomparedto thecontrolgroupandto pre-interventionvalues. Aveiroetal.200415 OPAQ-OsteoporosisAssessment
Questionnaire
Onlyonegroup.Theexercise programconsistedofthreeweekly sessionslastingonehoureach,for 12weeks.
Aftertheintervention,thesubjects exhibitedareducedlevelofpain andstress,andimprovementin activitiesofdailylivingandfamily support.
Kronhedetal.200918 SF-36andQualeffo-41(qualityof lifequestionnaireoftheEuropean FoundationforOsteoporosis)
Twogroups:controlandexercise. Theexerciseprogramconsistedof twoweeklysessionslastingone houreach,forfourmonths.
Afterfourmonths,theexercise groupshowedimprovementinthe SF-36domainsofphysical function,bodilypain,general health,vitality,socialfunctionand mentalhealth.
Withrespecttothedomainsof Qualeffo-41,therewasno differencebetweengroups. Devereuxetal.200517 SF-36 Twogroups:controlandexercise.
Theexerciseprogramlasted10 weeks,witheachsessionlasting 50minutes.Thenumberofweekly sessionswasnotinformed.
Thegroupbenefitedwiththe interventionshowedimprovement intheareasofphysicalfunction, vitality,socialfunctionandmental health.
Liu-Ambroseetal.200519 QualeffoeODI-OswestryLowBack PainDisabilityQuestionnaire
Theparticipantsweredividedinto threegroups:strength,agilityand stretching(control).Thephysical exerciseprogramconsistedoftwo weeklysessionslasting50minutes each,for25weeks.
WithrespecttoODI,nodifference wasnotedinthescoresamongthe groupsaftertheintervention. Thegroupthatperformed resistanceexercisesshowed improvementintheareasofpain andworkandsocialactivity;the groupofagilityexercisesshowed improvementintheareaof physicalfunction,asassessedby Qualeffo.
Carteretal.200216 Qualeffo Twogroups:controlandexercise. Theexerciseprogramconsistedof twoweeklysessionslasting40 minuteseach,for20weeks.
Nodifferencebetweengroupswith regardtoqualityoflifewasfound, bothforbaselineand
post-interventionperiodvalues. Tüzünetal.201021 Qualeffo Twogroups:onewithintervention
throughYogaandtheotherwith nonspecificexercises.Inboth groups,theprogramconsistedof twoweeklysessionslastingone houreach,for12weeks.
Bothgroupsshowedimprovement inoverallscorecomparedwith baselinevalues.
Therewasnodifferencewhen comparingpost-trainingvaluesof thetwogroups.
strength, compared to the control group (4.9% and 12.8%,
respectively).
Atraining program aimingtoincrease muscle strength,
especiallyinthelowerlimbs,isrequiredtopreventfallsand fracturesinthispopulation.Areductionofbalanceincreases
the risk and fearoffalling.15 Themobility resultsinmore
independenceforthe individual,reducingthe likelihoodof institutionalization.23
Frailindividuals with impairedbalance and movements
Table3–Resultsofstudiesthatevaluatedphysicalandfunctionaldomainsofwomenwithosteoporosis.
Author Assessedcomponents Exerciseprotocol Results
Carteretal.200112 Staticanddynamicbalanceand strengthofkneeextension.
Twogroups:controlandexercise. Theexerciseprogramconsistedof twoweeklysessionslasting40 minuteseach,for10weeks.
Theinterventiongroupshowedno significantdifference,when comparedtothecontrolgroup, withrespecttothebalanceand kneeextensionstrengthafter10 weeksoftraining.
Carteretal.200216 Staticanddynamicbalanceand strengthofkneeextension.
Twogroups,controlandexercise. Theexerciseprogramconsistedof twoweeklysessionslasting40 minuteseach,for20weeks.
Theinterventiongroupshowed improvementindynamicbalance (4.9%)andinkneeextension strength(12.8%)after20weeksof training,whencomparedtothe controlgroup.
Arnoldetal.200813 Staticanddynamicbalance. Threegroups,dividedintoagroup thatperformedexercisesinthe water,agroupthatpracticed exercisesoutofwater,anda controlgroup.Forthefirsttwo groups,theexerciseprogram consistedofthreeweeklysessions lasting50minuteseach,for20 weeks.
Subjectswhopracticedexercisein thewaterpresented
improvementsindynamic balance,whencomparedwith thosewhoexercisedoutofwater; however,therewasnodifference whentheinterventiongroups werecomparedwiththecontrol group.
Aveiroetal.200415 Torqueofthequadricepsmuscle andbalance.
Thephysicalactivityprogram consistedofthreeweeklysessions lastingonehoureach,for12 weeks.
Aftertheinterventionperiod,the groupreportedincreaseinmuscle torqueandimprovedbalance.
Aveiroetal.200622 Torqueoftheplantarflexorsand dorsiflexors,balanceandgait speed.
Thephysicalactivityprogramhad atotaldurationof12weeks, consistingofthreeweekly sessions.Thedurationofeach sessionwasnotreported.
Aftertheinterventionperiod,the groupreportedincreaseinmuscle torqueandimprovementin balanceandgaitspeed.
Devereuxetal.200517 Dynamicbalance. Twogroups:controlandexercise. Theexerciseprogramlasted10 weeks,witheachsessionlasting 50minutes.Thenumberofweekly sessionswasnotinformed.
Theinterventiongroupshowed improvementindynamicbalance.
Kronhedetal.200918 Balanceandgripstrength. Twogroups:controlandexercise. Theexerciseprogramconsistedof twoweeklysessionslastingone houreach,forfourmonths.
Theinterventiongroupshowedno differenceswithrespecttobalance andmanualgripstrengthtests, whencomparedtocontrol. Aftertheinterventionperiod,the exercisedgroupshowedno differenceinbalanceandmanual gripstrengthtests,when comparedwithbaselinevalues. Tüzünetal.201021 Balance. Twogroups:onewithintervention
throughYogaandtheotherwith nonspecificexercises.Inboth groups,theprogramconsistedof twoweeklysessionslastingone houreach,for12weeks.
OnlytheYogagroupshowed significantimprovementin balance,whencomparedto baselinevalues.
Therewasnodifferencewhen comparingpost-trainingvaluesof thetwogroups.
exercise,whileexercisinginthe water.10 Theaquatic
envi-ronment,inadditiontostabilityandcoordination,stimulates
the visual, vestibular and perceptual systems. The
water-based activity reduces the stress incident on joints and
musclesduetothe reducedimpact,andimprovesthe
sub-ject’srangeofmotion.17AccordingtoArnoldetal.,13exercises
performed in water can be more effective, even
consider-ing thefact that exercisespracticed out ofthe waterhave higherspecificityandapplicabilitywithrespecttofunctional tasks.
usedisspecifictothestudiedpopulation,consideringthe reli-abilityofthedata.30
Noneofthestudiesreviewedanalyzedbodyweight,height, prevalenceofalcoholintakeandsmoking.Itisknownthat thesevariablesareriskindicatorsforfallsandfracturesinthis population,31,32andchangesinbodyweightorinbehavioral
variablesmayindicatetheeffectoftheinterventionprogram. Itissuggestedthatfuture researchfocus on anthropomet-ricand behavioralvariables, besidesthe qualityoflifeand physicalaspects.
Basedon thearticlesselected, it ispossibletoconclude thattheinterventionwithexerciseisimportanttoimprove thequalityoflifeofwomenwithpostmenopausal osteoporo-sis.Similarly,activitiesaimedatworkingonmusclestrength andbalanceareessentialtopreventtheoccurrenceoffalls, andtoconsequentlyreducetheincidenceoffracturesinthis population.
Conflict
of
interests
Theauthorsdeclarenoconflictofinterests.
r
e
f
e
r
e
n
c
e
s
1. GlaserDL,KaplanFS.Osteoporosis:DefinitionandCinical Presentation.Spine.1997;2:12–6.
2. WHO.Preventionandmanagementofosteoporosis.Genebra: WHO;2003.
3. SchapiraD.Aerobicsandpostmenopausalosteoporosis. StressMedicine.1990;6:157–63.
4. SteinerML,FernandesCE,StrufaldiR,AzevedoLHd,Stephan C,PompeiLM,etal.Accuracystudyon“Osteorisk”:anew osteoporosisscreeningclinicaltoolforwomenover50years old.SaoPauloMedicalJournal.2008;126:23–8.
5. BandeiraF,CarvalhoEFd.Prevalênciadeosteoporosee fraturasvertebraisemmulheresnapós-menopausa atendidasemservic¸osdereferência.RevistaBrasileirade Epidemiologia.2007;10:86–98.
6. NorthAmericanMenopauseSocietyN.Managementof osteoporosisinpostmenopausalwomen:2010position statementofTheNorthAmericanMenopauseSociety. Menopause.2010;17:25–54.
7. SilvaRB,Costa-PaivaL,OshimaMM,MoraisSS,Pinto-Neto AM.Frequênciadequedaseassociac¸ãocomparâmetros estabilométricosdeequilíbrioemmulheresna
pós-menopausacomesemosteoporose.RevistaBrasileirade GinecologiaeObstetrícia.2009;31:496–502.
8. DouradorEB.OsteoporoseSenil.ArquivosBrasileirosem EndocrinologiaeMetabolismo.1999;43:446–51.
9. YamazakiS,IchimuraS,IwamotoJ,TakedaT,ToyamaY. Effectofwalkingexerciseonbonemetabolismin postmenopausalwomenwithosteopenia/osteoporosis. JournalofBoneandMineralMetabolism.2004;22:500–8.
10.BassSL,ForwoodMR,LarsenJA,SaxonL.PrescribingExercise forOsteoporosis.InternationalSportMedJournal.2001;1: 1–13.
11.DownsSH,BlackN.Thefeasibilityofcreatingachecklistfor theassessmentofthemethodologicalqualitybothof randomisedandnon-randomisedstudiesofhealthcare interventions.JEpidemiolCommunityHealth.1998;52:377–84.
12.CarterND,KhanKM,PetitMA,HeinonenA,WatermanC, DonaldsonMG,etal.Resultsofa10weekcommunitybased strengthandbalancetrainingprogrammetoreducefallrisk
factors:arandomisedcontrolledtrialin65-75yearold womenwithosteoporosis.BritishJournalofSportsMedicine. 2001;35:348–51.
13.ArnoldCM,BuschAJ,SchachterCL,HarrisonEL,Olszynski WP.ARandomizedClinicalTrialofAquaticversusLand ExercisetoImproveBalance,Function,andQualityofLifein OlderWomenwithOsteoporosis.PhysiotherapyCanada. 2008;60:296–306.
14.AuadMA,SimõesRP,RouhaniS,CastelloV,YogiLS.Eficácia deumprogramadeexercíciosfísicosnaqualidadedevidade mulherescomosteoporose.ArquivosBrasileirosdeCiência daSaúde.2008;33:31–5.
15.AveiroMC,NavegaMT,GranitoRN,RennóACM,OishiJ. Efeitosdeumprogramadeatividadefísicanoequilíbrioena forc¸amusculardoquadrícepsemmulheresosteoporóticas visandoumamelhorianaqualidadedevida.Revista BrasileiradeCiênciaeMovimento.2004;12:33–8.
16.CarterND,KhanKM,McKayHA,PetitMA,WatermanC, HeinonenA,etal.Community-basedexerciseprogram reducesriskfactorsforfallsin65-to75-year-oldwomenwith osteoporosis:randomizedcontrolledtrial.CanadianMedical AssociationJournal.2002;167:997–1004.
17.DevereuxK,RobertsonD,BriffaNK.Effectsofawater-based programonwomen65yearsandover:Arandomised controlledtrial.AustralianJournalofPhysiotherapy. 2005;51:102–8.
18.KronhedA-CG,HallbergI,ÖdkvistL,MöllerM.Effectof trainingonhealth-relatedqualityoflife,painandfallsin osteoporoticwomen.AdvancesinPhysiotherapy. 2009;11:154–65.
19.Liu-AmbroseTYL,KhanKM,EngJJ,LordSR,LentleB,McKay HA.Bothresistanceandagilitytrainingreducebackpainand improvehealth-relatedqualityoflifeinolderwomenwith lowbonemass.OsteoporosInternational.2005;16: 1321–9.
20.RennoACM,GranitoRN,DriussoP,CostaD,OishiJ.Effectsof anexerciseprogramonrespiratoryfunction,postureandon qualityoflifeinosteoporoticwomen:apilotstudy.
Physiotherapy.2005;91:113–8.
21.TüzünS,AktasI,AkarirmakÜ,SipahiS,TüzünF.Yogamight beanalternativetrainingforthequalityoflifeandbalancein postmenopausalosteoporosis.EuropeanJournalofPhysical andRehabilitationMedicine.2010;46:69–72.
22.AveiroM,GranitoR,NavegaM,DriussoP,OishiJ.Influenceof aphysicaltrainingprogramonmusclestrength,balanceand gaitvelocityamongwomenwithosteoporosis.Revista BrasileiradeFisioterapia.2006;10:441–8.
23.MadureiraMM,TakayamaL,GallinaroAL,CaparboVF,Costa RA,PereiraRMR.Balancetrainingprogramishighlyeffective inimprovingfunctionalstatusandreducingtheriskoffalls inelderlywomenwithosteoporosis:arandomizedcontrolled trial.OsteoporosInternational.2007;18:
419–25.
24.GoldD,StegmaierK,BalesC,LylesK,WestlundR,DreznerM. Psychosocialfunctioningandosteoporosisinlatelife:Results ofamultidisciplinaryintervention.JournalofWomen’s Health.1993;2:149–55.
25.AdachiJD,IoannidisG,OlszynskiWP,BrownJP,HanleyDA, SebaldtRJ,etal.Theimpactofincidentvertebraland non-vertebralfracturesonhealthrelatedqualityoflifein postmenopausalwomen.BMCMusculoskeletalDisorders. 2002:3.
26.RandellAG,NguyenTV,BhaleraoN,SilvermanSL,Sambrook PN,EismanJA.DeteriorationinQualityofLifeFollowingHip Fracture:AProspectiveStudy.OsteoporisInternational. 2000;11:460–6.
28.NavegaMT,OishiJ.Comparac¸ãodaQualidadedeVida RelacionadaàSaúdeentreMulheresnaPós-menopausa PraticantesdeAtividadeFísicacomesemOsteoporose. RevistaBrasileiradeReumatologia.2007;47:
258–64.
29.LemosMCD,MiyamotoST,ValimV,NatourJ.Qualidadede VidaemPacientescomOsteoporose:Correlac¸ãoentreOPAQe SF-36.RevistaBrasileiradeReumatologia.2006;46:
323–8.
30.GroupOQoLS.MeasuringQualityofLifeinWomenwith Osteoporosis.OsteoporisInternational.1997;7:478–87.
31.VoortDJMvd,GeusensPP,DinantGJ.RiskFactorsfor OsteoporosisRelatedtotheirOutcome:Fractures.Osteoporis International.2001;12:630–8.