Revista de Saúde Pública
I SSN 0034- 8910 versão im pressa
Rev Saúde Pública 2003; 37(5)
Comparison between different mortality risk scores in a neonatal
intensive care unit
Mariani Schlabendorff Zardo and Renat o S Pr ocianoy
Ser v iço de Neonat ologia. Hospit al de Clínicas de Por t o Alegr e. Por t o Alegre, RS, Brasil
ABSTRACT
Objective
To evaluat e and com par e bir t hw eight and r isk scor es as pr edict or s of neonat al m or t alit y in a Neonat al I nt ensive Care Unit ( NI CU) .
Methods
( Scor e for Neonat al Acut e Phy siology ) , SNAP- PE ( Scor e for Neonat al Acut e Phy siology – Perinat al Ex t ension) , SNAP I I , SNAP- PE I I , and CRI B scores, as well as for birt hweight .
Results
Of t he 494 pat ient s st udied, 44 died ( 8.9% m ort alit y) . Of t he 102 pat ient s born weighing up t o 1,500 g, 32 ( 31.3% ) died. The area below t he ROC curves ranged from 0.81 t o 0.94. Ther e w er e no st at ist ically significant differ ences bet w een t he ar eas obt ained for all scor es ev aluat ed. All m or t alit y r isk scor es ev aluat ed per for m ed bet t er t han bir t hw eight , especially on new bor ns w it h bir t hw eight
=1,500 g.
Conclusions
All neonat al m ort alit y scores had bet t er perform ance and were superior t o birt hweight as m easures of in- hospit al m ort alit y risk for newborns adm it t ed t o NI CU.
Keywords
Neonat al m ort alit y ( public healt h) . Birt h weight .I npat ient s.I nfant, newborn. Risk
assessm ent . I nt ensive care unit s, neonat al. Score.
I N TRODUCTION
The st udy of illness severit y and m ort alit y risk m easurem ent am ong newborns adm it t ed t o neonat al int ensiv e car e unit s ( NI CUs) is at t aining an increasing level of im port ance.1 1 I n order t o com pare m or t alit y levels of differ ent NI CUs, even aft er m aking adj ust m ent s for fact or s such as gender , bir t hw eight , gest at ional age, and et hnicit y , it is st ill necessar y for subj ect disease sev er it y t o be sim ilar.1 5
I n 1993, t hree scores were described for m easuring illness severit y and neonat al m ort alit y am ong new bor ns adm it t ed t o int ensiv e car e unit s: SNAP (Score for Neonat al Acut e Physiology) , SNAP- PE (Score for Neonat al Acut e Physiology - Perinatal Extension) , and CRI B (Clinical Risk I ndex for Babies) . The SNAP score is based on 34 variables, evaluat ed during t he w orst m om ent of t he first 24 hours aft er adm ission;3 , 8 , 1 0 - 1 2 SNAP- PE adds t o SNAP3 , 8 , 1 1 birt hweight , sm all size for gest at ional age ( SSGA) , and low Apgar scor e at 5 m inut es aft er deliver y. The CRI B scor e evaluat es six fact or s dur ing t he fir st 12 hours of life, but is appropriat e only for newborns wit h gest at ional age 31 weeks or less and/ or bir t hw eight up t o 1,500 g.2 , 3 , 5 , 6 , 1 2 , 1 3
The aim of t he pr esent st udy is t o ev aluat e bir t hw eight and SNAP, SNAP- PE, SNAP I I , SNAP- PE I I , and CRI B scores as predict ors of neonat al in - hospit al m ort alit y am ong newborns adm it t ed t o NI CUs, com paring t heir result s.
M ETHODS
The st udy included all new born babies in a general hospit al in t he cit y of Port o Alegre, sout hern Brazil, adm it t ed t o a NI CU im m ediat ely aft er delivery bet ween 1 March 1997 and 30 June 1998. St udied out com e w as deat h w hile in t he NI CU. SNAP and SNAP- PE evaluat ion w as done t hr ough a cohor t st udy, whereas CRI B, SNAP I I , and SNAP- PE I I w er e ev aluat ed r et r ospect iv ely t hrough a cross-sect ional st udy .
Pat ient s dead or discharged t o norm al new born care less t han 24 hours aft er adm it t ed, adm it t ed int o NI CU not im m ediat ely aft er delivery, whose st udy prot ocol was incom plet e due t o m issing dat a in pat ient files, or w it h congenit al m alform at ions incom pat ible wit h survival were excluded.
Physiological variables and scores applied in order t o generat e SNAP, SNAP- PE, SNAP I I , and SNAP- PE I I scor es w er e ext r act ed fr om st udies by Richar dson et al.1 0 , 1 1 , 1 3 The CRI B scor e w as applied accor ding t o Tar n ow- Mordi et al.1 5
SNAP and SNAP- PE w er e evaluat ed pr ospect ively, since t hey w er e r out inely applied upon adm ission t o t he NI CU, for use in a previously published st udy.1 4 Var iables w er e r egist er ed aft er t he pat ient ’s fir st 24 hour s in t he NI CU, and t he w or st m om ent w it hin t his per iod w as consider ed. SSGA classificat ion w as obt ained based on t he bir t hw eight / gest at ional age cur v e, as descr ibed by Alex ander et al.1 I nfant s w er e consider ed as SSGA w hose bir t hw eight w as below per cent ile 5, accor d ing t o SNAP- PE recom m endat ions.
CRI B, SNAP I I , and SNAP- PE I I w er e execut ed r et r ospect ively, t hr ough an exam inat ion of pat ient files. The SNAP I I and SNAP- PE I I sy st em s w er e descr ibed in 2001, t her efor e aft er dat a collect ion, and t hus w er e analy zed r et r ospect iv ely .1 3 CRI B scor ing w as not a r out ine pr ocedur e in t he I CU st udied, and w as evaluat ed r et r ospect ively in or der t o be com par ed t o t he r em aining scor es. Physiological var iables required for score applicat ion, considering t he first 12 hours aft er delivery , w er e collect ed. SSGA classificat ion w as obt ained based on t he bir t hw eight / gest at ional age cur v e used by Richar dson et al,1 0 w hich considers as of SSGA infant s w it h birt hw eight under percent ile t hree. CRI B w as applied only for pat ient s born weighing 1,500 g or less.
Gest at ional age w as est im at ed using t he New Ballar d m et hod for new bor ns w it h gest at ional- obst et r ic ages up t o 34 weeks, and t he Capurro m et hod for t he rem ainder.
FiO2 was considered as adequat e when able t o m aint ain hem oglobin oxygen sat urat ion at 90- 95% –
as m easured by a wrist oxym et er –, a level w hich allow s for good oxygenat ion along w it h a reduced r isk of ox y gen t ox icit y .
accor ding t o t he Hanley & McNeil t est .4 Soft w ar e used w er e SPSS ( St at ist ical Pack age for t he Social Scien ces) – version 10 and Epi I nfo. P- v alues less t han 0.05 w er e consider ed as st at ist ically significant .
The r esear ch pr oj ect w as appr ov ed by t he Et hic s Com m it t ee for Research on Hum an Beings (Com it ê de Ét ica em Pesquisa em Seres Hum anos) of t he Hospital de Clínicas de Porto Alegre.
RESULT S
During t he fieldw ork st age, 789 babies w ere adm it t ed t o t he NI CU. Of t hese, 243 w ere excluded for not being adm it t ed im m ediat ely aft er birt h ( 30.7% ) , 21 for dying less t han 24 hours aft er delivery ( 2.6% ) , 22 due t o incom plet e pat ient files ( 2.7% ) , and nine due t o congenit al m alform at ions incom pat ible wit h survival ( 1% ) . Of t he 494 pat ient s st udied, 44 died, represent ing an 8.9% m ort alit y. Pat ient s born weighing 1,500 g or less were select ed for CRI B assessm ent , yielding a t ot al 102 pat ient s. Mor t alit y am ong t his gr oup w as 31.3% ( 32 deat hs) and account ed for 73% of t ot al m ort alit y.
When all pat ient s w er e ev aluat ed, m ean bir t hw eight w as 2,354 g and m ean gest at ional age, 36 weeks. Of t he 494 pat ient s, 256 were m ale and 81 had Apgar scores < 7 at t he fift h m inut e. Considering only pat ient s wit h birt hweight up t o1,500 g, m ean weight was 1,050 g and m ean gest at ional age, 31 w eek s. Of t he 102 pat ient s, 64 w er e fem ale, and 30 had Apgar scor es < 7 at t he fift h m inut e.
The m edian scor es of sur v iv ing pat ient s scor es w er e com par ed t o t hose of pat ient s w ho died. All differ ences w er e st at ist ically significant , w it h p< 0,0001 ( Table 1) .
Ta ble 1 – Median score com parison for all pat ient s st udied.
Scor e Survivals* Deat hs* Significa
nce* All subj ect s
BW ( g) 2,418( 1,775
- 3,070)
860(643 -1,690)
< 0.0001
SNAP 4( 2- 7) 14( 9- 24) < 0.0001
SNAP PE 6( 3- 11) 34( 21- 53) < 0.0001
SNAP I I 0( 0- 9) 25( 13- 42) < 0.0001
SNAP PE I I 5( 0- 18) 55( 33- 74) < 0.0001 Subj ect s w it h bir t hw eight =1,500 g
BW ( g) 1,195( 1,038
- 1,326)
773(576 -1,006)
< 0.0001
CRIB 2( 1- 5) 12( 8- 16) < 0.0001
SNAP PE 10( 8- 18) 43( 26- 55) < 0.0001
SNAP PE I I 20( 12- 25) 60( 41- 78) < 0.0001
* Median ( p25- p75)
BW – Birt hweight
SNAP (Score for neonat al acut e physiology)
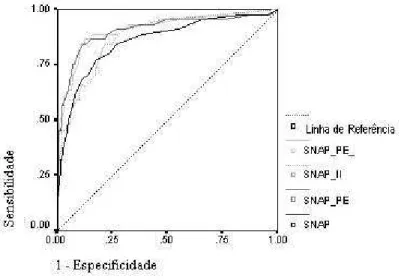
Figures 1 and 2 present t he area under t he ROC curve for all disease severit y scores. Perform ance lev els ar e locat ed bet w een good and ex cellent . Bir t hw eight achiev ed a 0.81 ar ea for all subj ect s. SNAP, SNAP- PE, SNAP I I , and SNAP- PE I I areas for t he sam e group were 0.85, 0.90, 0.88, and 0.91, r espect iv ely . I n t he bir t hw eight = 1,500 g group, Az equaled 0.82 for birt hweight , 0.93 for SNAP- PE, 0.94 for SNAP- PE I I , and 0.91 for CRI B.
Figure 1 -Area under ROC (receiver operating characteristic curve ) of all study patients’ scores
Figure 2 - Areas under ROC of scores of patients with 1,500 g birth weight
SNAP- PE I I achieved t he great est area am ong st udied scores in bot h groups. When considering all subj ect s, SNAP- PE w as st at ist ically m or e accur at e t han bir t hw eight alone in pr edict ing neonat al m or t alit y and SNAP- PE I I achieved a borderline result ( Table 2) . When considering only subj ect s w it h bir t hw eight = 1,500 g, all scor es w er e st at ist ically m or e accur at e t han bir t hw eight ( Table 3) . How ev er , t her e w as no st at ist ically significant differ ence in Az bet w een t he v ar ious scor es ( Tables 2 and 3) .
Ta ble 2 – P- v alues for t he ar eas below t he ROC cur v es of t he v ar ious scor es for all subj ect s.
SNA P SNAP PE SNAP I I SNAP PE I I Bir t hw ei
ght
0.40 4
0.030 0.188 0.055
SNAP 0.089 0.428 0.074
SNAP PE 0.401 0.791
SNAP I I 0.056
ROC – Receiver operat ing charact erist ic curve.
Ta ble 3 - P- values for t he ar eas below t he ROC cur ves of t he var ious scor es for subj ect s w it h bir t hw eight =1.500 g.
SNAP PE
SNAP PE I I
CRI B
Birt hweight 0.024 0.039 0.01
4
SNAP PE 0.547 0.25
7
SNAP PE I I 0.67
4
CRIB (Clinical risk index for babies)
D ISCUSSION
Birt hw eight has been used, for m any years, as a m ort alit y risk indicat or for new bor n babies. Recent st udies, however, have em phasized prognosis disparit ies bet ween babies born wit h sim ilar weight in differ ent NI CUs.5 , 1 0 , 1 2 Such differ ences ar e r elat ed t o var iat ions in populat ion r isk and t echnology
em ployed,1 1 w hich w ould j ust ify t he im por t ance of sev er it y indicat or s in t he com par ison of differ ent NI CUs.
bir t hw eight var ied fr om 0.74 t o 0.82, values ver y close t o t hose found in t he pr esent sur vey ( 0.81± 0.46) .5 , 7 , 1 1 This finding confirm s t he im port ance of physiological evaluat ion in det erm ining disease sever it y and evaluat ing m or t alit y r isk upon adm ission t o neonat al int ensive t her apy. The use of physiological var iables alone, how ever , has been consider ed as insufficient for pr edict ing neonat al m ort alit y in very low birt hweight pret erm babies.8 , 1 1 , 1 4
Despit e t he lack of st at ist ically significant differ ences in t er m s of Az, SNAP- PE I I w as found t o be superior t o birt hweight , SNAP, and SNAP I I when considering all pat ient s. This dem onst rat es t he im por t ance of t he per inat al ext ension included in SNAP- PE I I , w hich t ak es int o account – in addit ion t o physiological variables – bir t hw eight , Apgar scor e at fift h m inut e, and SSGA classificat ion as fact or s t hat cont r ibut e t o an incr ease in m or t alit y risk.1 2
Recent ly , Richar dson et al1 3 found a 0.78± 0.01Az for bir t hw eight alone as a pr edict or of m or t alit y for newborns adm it t ed t o NI CUs. When considering t he perinat al ext ension – t hat is, bir t hw eight , SSGA, and Apgar < 7 at fift h m inut e, Az equaled 0.84. How ever , w hen consider ing bot h physiological v ar iables and per inat al ex t ension, Az incr eased t o 0.91± 0.01, w hich indicat es t he im por t ance of bot h set s of infor m at ion as pr edict or s of m or t alit y .
The v alidat ion st udy for CRI B, conduct ed by Tar now- Mordi et al,1 5 found a 0.90 Az, a value sim ilar t o
t hat encount er ed in t he pr esent sur vey ( Az CRI B= 0.91) .5 There is a consensus in t he lit erat ure – w hich also applies t o t he pr esent st udy – as t o t he super ior it y of t he CRI B scor e in r elat ion t o birt hweight alone in predict ing neonat al m ort alit y.7 Raut onen et al9 concluded, aft er com par ing SNAP, SNAP- PE, and CRI B scor es, t hat t he lat t er had a bet t er per for m ance w it h st at ist ically significant differences in com parison t o SNAP and SNAP- PE. I n t he present survey, SNAP- PE I I had t he best perform ance am ong pat ient s born weighing up t o 1,500 g. However, a com parison bet ween SNAP- PE I I and CRI B r ev ealed no st at ist ically significant differ ences. Bot h t est s consider t he fir st 12 hour s aft er deliver y, t hus being less influenced by t r eat m ent .2 , 5 , 1 3 CRI B has t he disadvant age of being r est r ict ed
t o pat ient s w it h bir t hw eight = 1,500 g.
The scor es st udied ar e t ools for m easur ing in- hospit al m ort alit y risk am ong very ill newborns adm it t ed t o NI CUs. They should not be used for orient ing individual decisions relat ed t o any individual pat ient .
Th e pr esen t survey present ed t he result s of six disease severit y m easures in relat ion t o neonat al m or t alit y in t he NI CU st udied. All evaluat ed scor es had r esult s consider ed as good, w it h no st at ist ically significant differ ences. As t o t heir applicabilit y , CRI B, SNAP II , and SNAP- PE I I ar e fast er and easier t o apply , since t he num ber of v ar iables consider ed in t hese t est s is sm aller . The pr esent r esult s show t hat all m or t alit y r isk scor es inv est igat ed had a bet t er per for m ance t han bir t hw eight alone, part icularly am ong newborns weighing up t o1,500 g.
ACKNOWLEDGEM ENT S
To st at ist ician Vânia Naom i Hir akat a, of t he Universidade Federal do Rio Grande do Sul, for her suggest ions and or ient at ion concer ning st at ist ical analy sis; and Dr . Rit a C. Silv eir a, of t he Neonat al I nt ensiv e Car e Unit of t he Hospit al de Clínicas de Port o Alegre for her suggest ions and support in car r y ing out t he pr oj ect .
REFEREN CES
1 . Alexander GR, Him es JH, Kaufm an RB, Mor J, Kogan M. A Unit ed St at es Nat ional r efer ence for fet al gr ow t h. Obstet Gynecol 1996; 87: 163- 8 .
2 . Cou r cy- Wheeler RHB, Wolfe CDA, Fit zgerald A, Spencer M, Goodm an JDS, Gam su HR. Use of t he CRI B ( Clinical Risk I ndex for Babies) score in predict ion of neonat al m ort alit y and m orbidit y . Arch Dis Child 1995; 73: F32- 6.
3 . Fleisher BE, Mur t hy L, Lee S, Const ant inou JC, Benit z WE, St evenson DK. Neonat al sever it y of illness scor ing syst em s: a com par ison. Clin Pediatr (Phila) 1997; 4: 223 - 7 .
Hanley JA, McNeil BJ. A m et hod of com paring t he areas under receiver operat ing curves derived from t h e sam e cases. Radiology 1983; 148: 839- 43.
The I nt ernat ional Neonat al Net work. The CRI B ( Clinical Risk I ndex for Babies) score: a t ool for assessing init ial neonat al risk and com paring perform ance of neonat al int ensiv e car e unit s. Lancet 1993; 342: 193- 8
6 . Kaaresen PI , Døhlen G, Fundingsrud HP, Dahl LB. The use of CRI B ( clinical risk index for babies) scor e in audit ing t he per for m ance of one neonat al int ensiv e car e unit . Act a Paediat r 1998; 87: 195- 200.
7 . Mat suok a OT, Sadeck LSR, Haber JFS, Proença RSM, Mat aloun MMG, Ram os JLA et al. Valor predit ivo do “ Clinical Risk I ndex for Babies” para o risco de m ort alidade neonat al. Rev Saúde Pública 1998; 32: 550- 5.
8 . Pollack MM, Koch MA, Bart el DA, Rapoport I , Dhanireddy R, El- Mohandes AAE et al. A com parison of neonat al m ort alit y risk predict ion m odels in very low birt h weigt infant s. Pediat rics 2000; 105: 1051- 7 .
9 . Raut onen J, Mäkelä A, Boyd H, Apaj asalo M, Pohj avuori M. CRI B and SNAP: assessing t he risk of deat h for pret erm neonat es. Lancet 1994; 343: 1272 - 3 .
Address to correspondence
Mariani Schlabendorff Zardo Rua Barão de Ubá,194/ 502
90450 - 090 Port o Alegre, RS, Brasil E- m ail: m zardo@t elenov a.net
© 2 0 0 3 Fa cu lda de de Sa ú de Pú blica da U n iv e r sida de de Sã o Pa u lo
Ave nida D r . Ar na ldo, 7 1 5 0 1 2 4 6 - 9 0 4 Sã o Pa ulo SP Br a zil
Te l./ Fa x : + 5 5 1 1 3 0 6 8 - 0 5 3 9