Revista de Saúde Pública
I SSN 0034- 8910 versão im pressaRev Saúde Pública 2003; 37(5)
CRIB score, birth weight and gestational age in neonatal mortality
risk evaluation
Angela Sara J de Br it oa, Tiem i Mat suob, Maria Rafaela C Gonzaleza, Ana Ber enice R de Car valhoa e Lígia S L Ferraria
a
Depart am ent o de Pediat ria e Cirurgia Pediát rica da Universidade Est adual de Londrina. Londrina, PR, Brasil. bDepart am ent o de Mat em át ica Aplicada da Universidade Est adual de Londrina. Londrina, PR, Brasil
ABSTRACT
Objective
To evaluat e t he m ort alit y rat e of very low birt h w eight babies born at a Neonat al I nt ensive Care Unit ( NI CU) during a specified period of t im e according t o variat ions in CRI B ( Clinical Risk I ndex for Babies) score, birt h w eight and gest at ional age.
Methods
Results
Tw o hundr ed and eight y - four infant s m et t he inclusion cr it er ia. Mean birt h weight w as 1 , 1 4 8±248 g ( m edian = 1,180) , m ean gest at ional age was 30.2±2.4 weeks ( m edian = 30.0) and m ean CRI B score w as 3 . 8±4.4 ( m edian = 2.0) . The neonat al m ort alit y rat e was 23.2% , varying according t o m ean birt hweight < 750 g ( 72.7% ) , gest at ional age < 29 wee ks ( 57.1% ) and CRI B score > 10 ( 79.4% ) . Receiv er Oper at ing Char act er ist ic ( ROC) cur v es w er e com posed for CRI B scor e, bir t h w eight and gest at ional age t o assess t he abilit y of each t o pr edict hospit al m or t alit y and t he ar eas under t he cur v e w er e r espect iv ely 0.88, 0.76 and 0.81. Sensit iv it y , specificit y and pr edict iv e v alues w er e evaluat ed and all var iables w er e consider ed pr edict or s of m or t alit y ( p< 0.0001) . The opt im al cut off point based on t he ROC cur v e for t he CRI B scor e w as 4 w it h sensit iv it y 75.8% , specificit y 86.7, posit ive predict ive value 63.3% and negat ive predict ive value 92.2% .
Conclusions
I n t his st udy infant s w it h bir t hw eight of less t han 750 gr am s, less t han 29 w eeks gest at ional age and CRI B scores above 10 had higher m ort alit y rat es. However, a CRI B score higher t han 4 proved t o be a bet t er pr edict or of m or t alit y w hen com par ed t o bir t hw eight and gest at ional age.
Keywords
I nfant , very low birt h w eight . Neonat al m ort alit y ( public healt h) . Risk. I nt ensive care unit s, neonat al. Birt hw eight . Gest at ional age. CRI B score.
I N TRODUCTION
Advances in per inat al m edicine and t he incr easing sophist icat ion of suppor t t her apies w it hin neonat al int ensiv e car e unit s ( NI CUs) hav e led t o a not ew or t hy r educt ion in t he r at es of neonat al m or t alit y am ong very low birt hweight infant s. Progress in t his field has brought int o quest ion t he present lim it s of fet al viabilit y. Mort alit y risk assessm ent s, ut ilizing variables t hat m ay int erfere in m ort alit y rat es, h av e been t he obj ect of st udy in differ ent count r ies and differ ent neonat ology unit s. Dur ing a long t im e, birt hw eight and gest at ional age w ere significant univariat e predict ors of neonat al m ort alit y. However, m ore com plet e scoring syst em s for assessing t he risk of m ort alit y have been developed r ecent ly w hich aggr egat e phy siological par am et er s w hich r eflect t he init ial clinical st at e of t he newborn. Am ong t he scores based on physiological alt erat ions, som e are sim pler, wit h few variables and can be rapidly applied; ot hers are m ore com plet e, for t hey cont em plat e m ore variables, but t ake a longer t im e t o be applied. The scor ing sy st em s w hich hav e been st udied in gr eat er dept h and w hich are m ore frequent ly ut ilized on newborns are t he Clinical Risk I ndex for Babies ( CRI B) Scor e and t he Scor e for Neonat al Acut e Phy siology ( SNAP) . These scor es w er e v alidat ed and r e - applied in dist inct st udies in differ ent count r ies. 11,12,16
t he CRI B score has been ut ilized in different neonat al unit s, 3,4,6,8,13 because it is a sim ple inst rum ent w hich is sensit ive and can be rapidly applied. I t st resses param et ers w hich reflect t he phy siological condit ions of t he new bor n soon aft er bir t h and super cedes t he disadv ant ages of bir t hw eight specific and/ or gest at ional age specific pr edict or s of neonat al m or t alit y . This scor e m ay also be em ployed in t he evaluat ion of t he perform ance of a single NI CU t hroughout a period of t im e or w hen com par ing t he per for m ances of differ ent unit s.2,6,14 The scor e ut ilizes six different variables obt ained r out inely dur ing t he fir st 12 hour s of life, nam ely, bir t hw eight , gest at ional age, t he pr esence of congenit al m alform at ion( s) ( excluding inevit ably let hal congenit al m alform at ions) and t he indices of phy siological st at us, t ha t is, m inim um and m axim um appropriat e inspired oxygen concent rat ion and m axim um ( m ost acidot ic) base excess.16
I n Br azil, differ ent neonat al unit s hav e ut ilized scor es based on gr av it y of t he clinical st at us of t he new bor n, r einfor cing t he im por t ance of it s applicat ion and recom m ending it s use at t he m om ent t he infant is adm it t ed t o t he NI CU.8,9,13,15 The CRI B scor e has been ut ilized since 1997. The obj ect ive of t he pr esent st udy is t o ev aluat e t he m or t alit y r at e of v er y low bir t hw eight liv ebor n infant s, ac cording t o variat ions in CRI B score, birt hw eight and gest at ional age.
M ETHODS
I n a prospect ive st udy undert aken during t he period from January 1997 t o Decem ber 2000, t he CRI B score was applied t o all newborns wit h a birt hweight of < 1,500 g and/ or gest at io nal age < 31 weeks, born at t he m at ernit y of a Universit y Hospit al in Londrina and adm it t ed t o t he NI CU of t his hospit al. The lat t er is a public hospit al, w hich at t ends pat ient s under a cov enant w it h t he nat ional healt h syst em t he Sist em a Unico de Saúde or SUS. Those assist ed by t his hospit al com e predom inant ly from t he low social and econom ic st r at a of t he r egional populat ion.
Cr it er ia for exclusion fr om t his st udy w er e: new bor ns t hat died in t he fir st t w elve hour s of life, t hose
w ho pr esent ed inev it ably let hal congenit al m alfor m at ions, and t hose w ho w er e bor n at ot her hospit als and r efer r ed t o t his hospit al aft er w ar ds.
Aft er t hey were dism issed from t he NI CU, t he newborns rem ained int erned in t he sam e hospit al unt il
t hey r ecuper at ed or unt il t hey died. No ne of t he new bor ns w er e dischar ged fr om t he hospit al befor e t hey had com plet ed 28 day s of life and, in t he pr esent st udy , only neonat al deat hs w er e included, t hat is, only t hose deat hs w hich occur r ed up t o 28 day s of life.
The CRI B scor e w as calculat ed on t he basis of an est ablished num ber of point s and ar e pr esent ed on
Table 1, accor ding t o t he pr oposal m ade by t he I nt er nat ional Neonat al Net w or k. 1 6
Ta ble 1 – CRI B score.*
Fact o r Score
Birthweight (g)
>1350 0
851-1350 1
701-850 4
≤700 7
Gestational age (wk)
>24 0
≤24 1
Congenit al m alform at ion * *
None 0
Acutely life-threatening 3
Maximum base excess in first 12h
>-7.0 0
-7 to -9.9 1
-10 to -14.9 2
≤-15.0 4
Minimum appropriate FiO2 in first 12h
<0.40 0
0.41-0.80 2
0.81-0.90 3
0.91-1.00 4
Maximum appropriate FiO2 in the first 12h
<0.40 0
0.41-0.80 1
0.81-0.90 3
0.91-1.00 5
* CRI B – “ Clinical Risk I ndex for Babies” .
* * Excluding inevit able let hal m alform at ions.
FiO2: - Fr act ion of inspired oxygen.
New bor ns w ho did not r equir e r espir at or y suppor t and gasom et r ical cont r ol r eceived scor es equal t o
zer o in t he FiO2 fact or s, m ax im um and m inim um , and m ax im um base ex cess. New bor ns w er e
dist r ibu t ed accor din g t o t h e scor es t h ey r eceiv ed. Ther e being four scor e gr oups: t hose w ho r eceiv ed fr om 0 t o 5 point s, t hose w ho r eceiv ed fr om 6 t o 10 point s, t hose w ho r eceiv ed fr om 11 t o 15 point s and t hose w ho r eceiv ed m or e t han 15 point s. Gest at ional age w as calculat ed on t he basis of t he dat e of t he last m enst r uat ion, w hen t he m ot her could pr ov ide t his infor m at ion w it h pr ecision or w it h t he aid of dat a obt ained t hr ough t he ult r asound, if t he lat t er had been per for m ed befor e t he 20t h w eek of gest at ion, confer r ed by t he m odified Ballar d m et hod for sm all pr em at ur e infant s.1 All newborns were
obser v ed unt il t hey w er e dischar ged or unt il t heir deat h, and t he dat a w as r egist er ed by one of t he nenat ologist aut hor s, on a for m w hich is ut ilized in t his sect or of t he hospit al. All deat hs w hich occu r r ed u p t o 2 8 day s of life w er e consider ed neonat al deat hs.
RESULT S
During t he st udy period, 284 newborns fulfilled t he crit eria for inclusion. Eleven newborns were excluded, one of w hich suffe red from let hal congenit al m alform at ions ( renal agenesia wit h hydropsy) and 10 died in less t han t en hours aft er birt h due t o ext rem e prem at urit y and asphyxia. Tw elve liveborn infant s died m ore t han 28 days aft er birt h. The cohort analyzed present ed m ean birt hw eight of 1148± 248 g, wit h a m edian weight of 1180 g and variat ion of 530 t o 1,500 g. Mean gest at ional age was 30.2± 2.4 weeks, wit h m edian of 30, varying from 24 t o 39 weeks. The need for int ubat ion in t he delivery room occurred am ong 79 newborns ( 27.8% ) , 15 ( 5.3% ) present ed 5 m inut e Apgar scores < 5, and 174 were born by m eans of cesarean sect ions. The m ean CRI B score was 3.8± 4.4, wit h a m edian of 2.0, varying from zero t o 19. Am ong t he newborns included in t his st udy, 66 infant s died ( 23, 2% ) .
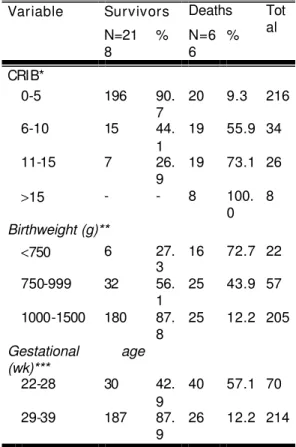
Th e r at e of m ort alit y was higher am ong newborns weighing less t han 750 g, wit h less t han 29 weeks gest at ional age and CRI B scor es higher t han 10 ( See Table 2) . The var iables analyzed above present ed a significant associat ion w it h m ort alit y ( p> 0.0001) .
Table 2 – Rate of survivals and deaths according to CRIB score, birthweight, and gestational age.
Survivors Deaths Variable
N=21 8
% N=6 6
% Tot al
CRIB*
0-5 196 90.
7
20 9.3 216
6-10 15 44.
1
19 55.9 34
11-15 7 26.
9
19 73.1 26
>15 - - 8 100.
0 8
Birthweight (g)**
<750 6 27.
3 16 72.7 22
750-999 32 56.
1 25 43.9 57
1000-1500 180 87.
8
25 12.2 205
Gestational age (wk)***
22-28 30 42.
9
40 57.1 70
29-39 187 87.
9
26 12.2 214
* CRI B: χ2
= 106.6 wit h 3 g.l. and value of p< 0,0001
* * Bir t hw eight : χ2 = 57,81 wit h 2 g.l. and value of p< 0,0001
* * * Gest at ional age: χ2
The w eight of t he new bor ns t hat died in t his st udy var ied fr om 530 t o 1495g, being t he aver age w eight 953.6± 273.2 g and t he m edian w eight 907.5 g. Those who sur v iv ed w eighed fr om 610 t o 1,500 g, being t he average w eight 1207.4± 206.7 g and 1,237 m edian w eight . These average w eight s pr esent ed significant st at ist ical differ ences ( p< 0.0001) .
Gest at ional age of new bor ns w ho died var ied significant ly fr om t hose who survived ( p< 0,0001) , being t hat t he age of t hose t hat died v ar ied fr om 24 t o 33 w eek s, w it h an av er age of 28 w eek s and one day ± t w o w eeks and t hr ee days, and a m edian of 28 w eeks. The new bor ns w ho sur vived pr esent ed gest at ional ages varying from 26 t o 39 w eeks, w it h an average of 30 w eeks and six days + t w o w eeks and one day, and a m edian of 31 weeks.
The CRI B scor e of t he new bor ns t hat died var ied fr om zer o t o 19, pr esent ing an aver age scor e of 9.0+ 5.0 and a m edian of 9.5. The score of t hose t hat surv ived var ied fr om zer o t o t hir t een, w it h an av er age of 2.3+ 2.7 and a m edian scor e of 1.0. The differ ence bet w een t hese scor es w as highly significant ( p< 0.0001) .
Ev aluat ing t he ROC cur v e of t he v ar iables ( Figur e) , for t he CRI B scor e, t he cut t ing off point which pr esent ed t he gr eat est accur acy ( ar ea of 0. 882+ 0. 028) w as four .
0
10
20
30
40
50
60
70
80
90
100
0
10
20
30
40
50
60
70
80
90
100
1 - Specificity (%)
Sensitivity (%)
CRIB BIRTHWEIGHT GI
For bir t hw eight , t he cut t ing off point w as at 1.005g and for gest at ional age, it w as 28 w eek s. When
t hese cut t ing off point s ar e ex am ined, t he CRI B scor e pr esent ed t he best per for m ance w it h a 75. 8% ( CI 95% : 63.6-85.5% ) sensit ivit y, specif icit y equal t o 86.7% ( CI 95% : 81.5- 90.9% ) , posit ive pr edict ive value of 63.3 ( CI 95% : 51.6- 73.6) and negat ive pr edict ive value of CI 95% : 87.4- 95.3% )
Ta ble 3 – Cut - off point , ar ea ± St andard error under t he ROC curve, relat ive risk, specificit y, posit ive pr edict iv e v alue ( + ) , negat iv e pr edict iv e v alue (- ) and r espect iv e 95% confidence int er v als for t he CRI B scor e, bir t hw eight ( gr am s) and gest at ional age ( w eeks) .
Variables
St at ist ics
CRI B Score Birt hweight ( gram s)
Gest at ional Age
( weeks)
Pon t o d e cor t e >4 ≤1005 ≤28
Área ± erro padrão (C. I. 95%) 0.882±0.028 0.763±0.030 0.805±0.027
(0.839-0.917) (0.709-0.811) (0.754-0.850)
Sensibilit y ( C. I . 95% ) 75.8 65.2 60.0
(63.6-85.5) (52.4-76.5) (47.1-72.0)
Specificit y (C. I. 95%) 86.7 81.7 86.6
(81.5-90.9) (75.9-86.6) (81.3-90.8)
Predict ive value + (C. I
95%) 63.3 51.8 57.1
(51.6-73.6) (40.6-62.8) (44.8-68.7)
Pr edict iv e v alue - (C. I 95%) 92.2 88.6 87.9
(87.4-95.3) (83.1-92.5) (82.5-91.8)
ROC – “ Receiv er Oper at or Char act er ist ics”
D ISCUSSION
Mor t alit y am ong very low birt hweight infant s is st ill very high in Brazil, part icularly am ong t hose w eighing less t han 750 gram s and w it h less t han 29 w eeks gest at ional age. I nt erpret at ion of m ort alit y r at es should t ak e int o consider at ion t he clinical condit ions of the new bor n, t he qualit y of at t ent ion r eceiv ed, r esour ces av ailable and m odificat ions in t her apeut ic appr oaches ut ilized at t he t im e of bir t h, which differ from count ry t o count ry and am ong NI CUs wit hin t he sam e count ry. The general m ort alit y of new borns w it h less t han 1,500 g, in t he NI CU st udied w as 23.2% , being quit e differ ent accor ding t o variat ions in w eight and gest at ional age ( Table 2) , w it h differences of 72.7% for t hose w ho w eighed less t han 750 g and 12.2% for t hose weighing from 1,000 t o 1,500 g.
I n t he present st udy, t he CRI B score w as ut ilized t o evaluat e t he risk of m ort alit y am ong new borns w it h less t han 1,500 g, due t o t he fact t hat it can be r apidly obt ained using av ailable phy siological v ar iables r out inely obt ained and t hus discar ding t he need for ext ra t im e in order t o apply t his score. The init ial clinical st at e of t he new bor n is a r eflex of pr ev ious obst et r ic ev ent s and t hose w hich occur dur ing labour , as w ell as t he car e deliver ed t o t he new bor n at bir t h and dur ing t he fir st few hour s of life.
The higher t he score, t he great er t he risk of m ort alit y. When t he dist ribut ion of CRI B scores am ong newborns t hat died ( m edian of 9.5 varying from zero t o 11) are com pared t o t hose t hat survived ( m edian 1.0 var ying fr om zer o t o one) , a st at ist ical difference ( p< 0,001) w as found.
The average CRI B score wit hin t he cohort st udied was 3.8± 4.4, wit h a m edian of 2.0, which is sim ilar t o t he result s of a nat ional st udy undergone during t he sam e period am ong a populat ion wit h t he sam e charact erist ics.13 Am ong t ho se new bor ns included in t his st udy t hat had scor es v ar y ing fr om 11 t o 15, 73.1% died, and am ong t hose w hose scor es w er e higher t han 15, t he r at e of m or t alit y w as 100% ( Table 2) , result s sim ilar t o ot her st udies.4 - 6,8,10,13
Analy sis of t he pr edict iv e accur acy of bir t hw eight , gest at ional age and CRI B scor e in r elat ion t o t he risk of m ort alit y, undergone by building a ROC curve, wit hin t he current st udy, det erm ined t hat t he CRI B scor es gr eat er t han 4 pr esent t he best char act er ist ics as a diagnost ic t est w hen c om pared t o bir t hw eight < 1,005 g and gest at ional age < 28 w eeks. As in pr evious st udies, t he pr esent invest igat ion has dem onst r at ed t hat t he CRI B scor e is m or e accur at e, w it h an ar ea under t he ROC cur v e of 0.88 ( CI 95% : 0.84- 0.92) , differing significant ly from bir t hw eight , w hich has an ar ea of 0.76 ( CI 95% : 0.71- 0.81) . However, gest at ional age, wit h an area of 0.81 under t he ROC curve ( CI 95% : 0.75- 0.85) , did not pr esent significant differ ences.
The r esult s obt ained indicat e t hat t he CRI B scor e is an appr opr iat e m eans of evaluat ing perform ance of per inat al car e based on t he out com e of m or t alit y , consider ing t he init ial clinical st at e of t he v er y low bir t hw eight new bor ns t hat w er e st udied. How ev er , it is im por t ant t o ev aluat e t he qualit y of life am ong newborn survivors, since m orbidit y and com plicat ions in t he perinat al period m ay cause im port ant sequels. An analysis of t he result s of t his t ype of st udy in a NI CU also m akes it possible t o est ablish com parisons am ong different periods of t im e and wit h ot her services, t o ev alu at e cost s an d ben ef it s and m odify procedures so as t o im prove pat t erns of perform ance.
REFEREN CES
1. Ballard JL, Khoury JC, Wedig K, Wang L, Eilers- Walsm an BL, Lipp R. New Ballard Scor e ex panded t o include ext rem ely prem at ure infant s. J Pediat rics 1991; 119: 417- 23.
2. Bard H. Assessing neonat al risk: CRI B vs SNAP. Lancet 1993; 342: 449- 50.
4. De Coursy- Wheeler RHB, Wolfe CDA, Fit zgerald A, Spenser M, Goodm an JDS, Gansu HR. Use of t he CRI B ( Clinical Risk I ndex for Babies) score in predict ion of neonat al m ort alit y and m orbidit y. Arch Dis Child 1995; 73: F32- F6 .
5. Fowlie PW, Gould CR, Tarnow- Modi WO, St rang DMA. Measurem ent propert ies of t he Clinical Risk I ndex for Babies: reliabilit y, validit y beyond t he first 12 hours and responsiveness over 7 days. Crit Care Med 1998; 26: 163- 8 .
6. Kaarensen PI , Dohlen G, Fundingsrud HP, Dahal LB. The use of CRI B ( Clinical Riak I ndex for Babies) scor e in audit ing t he per for m ance of one neonat al int ensiv e car e unit . Act a Paediat r 1998; 87: 195- 200.
7. Lago P, Fr eat o F, Bet t iol T, Chiandet t i L, Vianello A, Zar am ella P. I s the CRI B score ( Clinical Risk I ndex for Babies) a valid t ool in predict ing neurodevelopm ent al out com e in low birt h weight infant s. Biol Neonat e 1999; 76: 220 - 7 .
8. Mat suoka OT, Sadek LSR, Haber JFS, Proença RSM, Mat aloun MMG, Ram os JLS et al. Valor pr edit iv o do “ Clinical Risk I ndex for Babies” para o risco de m ort alidade neonat al. Rev Saúde Pública 1998; 32: 550- 5.
9. Procianoy RS, Benj am in ACW, Mart inez FE, Mussi- Pinhat a MM, Leone CR, Sadeck LSR et al. CRI B e peso de nascim ent o: qual o m elhor predit or de m ort alidade em recém nascidos de m uit o baixo peso. I n: Anais do 17º Congresso Brasileiro de Perinat ologia 2001, 10- 14 nov. Florianópolis; 2001. p. 187.
10. Raut onen J, Makela A, Boyd H, Apagasalo M, Pohj avuori M. Crib and SNAP: assessing t he risk of deadh for pret er m neonat es. Lancet 1994; 343; 1272- 3 .
11. Richardson DK, Gray JE, McCorm ick MC, Workm an- Daniels K, Goldm ann DA. Score for Neonat al Acut e Physiology ( SNAP) : validat ion of a new physiology - based sev er it y of illness index . Pediat r ics 1993; 91: 617- 23.
12. Ric hardson DK, Tarnow- Modi WO, Escobar GI . Neonat al r isk scor e syst em s. Can t hey pr edict m ort alit y and m orbidit y. Clin Perinat ol 1998; 25: 591- 611.
13. Sarquis ALF, Miyaki M, Cat MNL. Aplicação do escore CRI B para avaliar o risco de m ort alidade. J Pediat r 2002; 78: 225 - 9 .
14. Scot t ish Neonat al Consult ant s Collabor at ive St udy Gr oup / t he I nt er nat ional Neonat al Net w or k. CRI B ( Clinical Risk I ndex for Babies) , m ort alit y, and im pairm ent aft er neonat al int ensive care. Lancet 1995; 345: 1020- 22.
15. Silveira RC, Schlabendorff M, Procianoy RS. Valor predit ivo dos escores de SNAP e SNAP- PE na m ort alidade neonat al. J Pediat r 2001; 77: 455 - 60.
16. The I nt ernat ional Neonat al Net w ork. The CRI B ( Clinical Risk I ndex for Babies) score: a t ool for assessing init ial neonat al risk and com par ing per for m ance of neonat al car e unit s. Lancet 1993; 342: 193- 8 .
Address to correspondence
Angela Sara J. de Brit o
Rua Belo Horizont e, 1356 apt o1112 86020 - 030 Londrina, PR, Brasil E- m ail: ebr it o@ser com t el.com .br
Present ed at t he 3rd World Congress on Pediat ric I nt ensive Care, Mont real, 2000. Recieved on 8/ 10/ 2002. Reviewed on 6/ 5/ 2003. Approved on 26/ 5/ 2003.
© 2 0 0 3 Fa cu lda de de Sa ú de Pú blica da U n iv e r sida de de Sã o Pa u lo
Ave nida D r . Ar na ldo, 7 1 5 0 1 2 4 6 - 9 0 4 Sã o Pa ulo SP Br a zil
Te l./ Fa x : + 5 5 1 1 3 0 6 8 - 0 5 3 9