Copyright © ABE&M todos os dir
eitos r
eser
vados.
1 Serviço de Endocrinologia,
Hospital Universitário, Universidade Federal de Santa Catarina (UFSC), Florianópolis, SC, Brasil
Correspondence to:
Maria Isabel Cunha Vieira Cordioli Departamento de Clínica Médica Hospital Universitário, Universidade Federal de Santa Catarina
Campus Universitário – Trindade 88040-970 – Florianópolis, SC, Brasil
Received in Aug/31/2008 Accepted in Mar/23/2009
Increase incidence of thyroid cancer in
Florianopolis, Brazil: comparative study
of diagnosed cases in 2000 and 2005
Aumento da incidência do câncer de tireoide em Florianópolis, Brasil: estudo comparativo dos casos diagnosticados nos anos 2000 e 2005
Maria Isabel C. V. Cordioli1, Maria Heloísa B. S. Canalli1, Marisa Helena C. Coral1
ABSTRACT
Objective: To provide epidemiological information about thyroid cancer (TC) in the Metropoli-tan area of Florianopolis and investigate some factors that could be associated with this type of cancer. Method: This study analyzed data of patients who had TC diagnosed and underwent sur-gical treatment in 2000 and 2005. Epidemiolosur-gical factors about patients, tumors and sursur-gical procedures were evaluated. Results: In 2000 and 2005, an increasing incidence of TC at a rate of 132.33% was detected. The increased rate was mainly observed for tumors measuring less than 1 cm (p = 0.004). Results also showed an increase in the number of multifocal tumors (p = 0.02) and in the rate of total thyroidectomy (p = 0.002). Conclusions: The increasing incidence of TC in the Metropolitan area of Florianopolis is probably due to more invasive thyroid nodule manage-ment. Future studies are necessary to establish potential predicting factors for papillary thyroid microcarcinoma aggressiveness, as well as predictors of follicular lesion malignancy to identi-fying more accurately the appropriate therapy approach. Arq Bras Endocrinol Metab. 2009;53(4):453-60.
Keywords
Thyroid neoplasm; incidence; early diagnosis
RESUMO
Objetivo: Fornecer informações epidemiológicas acerca do câncer de tireoide (CT) na Grande Florianópolis e avaliar fatores que possam estar associados a tal neoplasia. Métodos: A popu-lação de estudo incluiu pacientes, com diagnóstico de CT, submetidos a tratamento cirúrgico em 2000 e 2005. Foram avaliados fatores epidemiológicos referentes aos pacientes, caracte-rísticas das lesões e procedimentos cirúrgicos realizados. Resultados: Durante o período de estudo, detectou-se um aumento na incidência do CT correspondente a 132,33%. Verificou-se um incremento estatisticamente significativo dos tumores menores de um centímetro (p = 0,004), da proporção de tumores multicêntricos (p = 0,02) e de tireoidectomias totais (p = 0,002). Conclusões: A maior incidência do CT na Grande Florianópolis está possivelmente associada a uma conduta mais intervencionista na abordagem de nódulos tireoidianos. Estudos futuros se fazem necessários para o estabelecimento de critérios preditivos da agressividade dos mi-crocarcinomas papilíferos e de malignidade das lesões foliculares no sentido de identificar com acurácia a melhor opção terapêutica. Arq Bras Endocrinol Metab. 2009;53(4):453-60.
Descritores
Câncer de tireoide; incidência; diagnóstico precoce
INTRODUCTION
T
hyroid cancer represents almost 1% of malignantneoplasms, corresponding to 0.5% of total deaths caused by cancer (1). Despite a low and progressive re-duction in mortality rate, thyroid cancer is a public
he-alth issue because of its increasing incidence, as shown in various studies worldwide (2-9).
thy-Copyright © ABE&M todos os dir
eitos r
eser
vados.
roid cancer, stable or even decreased incidence rates are reported (4,6,12). Factors associated with this relevant increase in incidence of papillary thyroid cancer have not been clearly established (11).
The existence of possible risk factors for papillary thyroid cancer has been mentioned in many studies. However, among these factors, only the association with irradiation is well established (13). The alteration of io-dine levels in the diet is associated with the pathogen-esis of thyroid cancer (7,14), though its mechanism of action is still controversial. Another reported risk factor is a previous history of benign thyroid disease, such as goiter, benign nodules and adenomas (15). Hormonal factors, such as the use of contraceptives and hormone replacement therapy, as well as reproductive factors, can also be related to this type of neoplasm (16,17). The ex-istence of genetic factors associated with thyroid cancer are reported, and in the case of the medullar type, are well established (18). Smoking, associated with various diseases, is paradoxically reported by some authors as a factor of risk reduction for thyroid cancer (19).
Despite the existence of a variety of factors possibly associated with the pathogenesis of thyroid cancer, im-provements in the accuracy of diagnostic methods and an increase in the number of thyroid investigations are reported in several studies (2,8-10,20,21) as the main factors contributing to the increased incidence of thy-roid cancer. This improvement and a wider access to diagnosis techniques, such as ultrasound and fine-nee-dle aspiration (FNA), are associated with the change in management of thyroid diseases (20) as well as with the possibility of detecting and evaluating thyroid nodules smaller than one centimeter (21).
This significant increase in the number of ultra-sonographies and FNAs coincides with the increase of tumors smaller than one centimeter, which are nor-mally asymptomatic and non-palpable. Several authors (3,5,9,11) used this fact as an argument to justify the relevant increase in the incidence of thyroid cancer, though it is still debatable in the literature (22-26).
The overall incidence and mortality rate of thyroid cancer in Brazil is similar to that described in other countries (27). However, the incidence varies between Brazilian regions evaluated (28,29).
There has only been one report on the Metropoli-tan area of Florianopolis published in 2000, which was made available by the Oncological Research Cen-ter (Centro de Pesquisas Oncológicas, CEPON). The lack of additional yearly reports renders the conclusion
about the evolution and incidence of thyroid cancer in this region impossible. Moreover, the data available is sparse and imprecise regarding the characteristics of the tumors diagnosed.
This study aims at providing epidemiologic infor-mation about thyroid cancer in the Metropolitan area of Florianopolis in 2000 and 2005, as well as evaluating factors that may be associated with the occurrence of this neoplasm.
METHOD
This is an observational, descriptive and cross-section-al study. The ancross-section-alyzed population comprised patients diagnosed with thyroid cancer in the Metropolitan area of Florianopolis. The inclusion criteria were: pa-tients who had undergone surgical treatment in 2000 and 2005 in the Metropolitan area of Florianopolis, which also includes the cities of São Jose, Biguaçu and Palhoça. Patients from other cities that were transferred to this area only to undergo the surgery or whose data could not be obtained were excluded from the analyzed population.
This research was initially conducted in pathology services in the Metropolitan region of Florianopolis. The identification of patients diagnosed with thyroid cancer was done through the analysis of histopathologic or cytologic exams. Information regarding patients who were treated by the Public Health System was obtained by visiting the public hospitals of the Metropolitan re-gion of Florianopolis. In order to gather information regarding private patients, doctors who asked for ana-tomical pathology were contacted and asked to provide patients’ file information. Besides, to obtain some in-formation that was not in the patients’ file, the authors tried to contact patients themselves by phone. The RCBP 2000 released by CEPON was used as source of information on patients with thyroid cancer in 2000.
The sources of population data used in the research were obtained from the Demographic Census (30) and population estimates (Instituto Brasileiro de Geografia e Estatística, IBGE) (31). Mortality data was derived from the Mortality Information System (Sistema de In-formação sobre Mortalidade, SIM) (32).
Statistical analysis of the obtained data was made us-ing the Chi-square and t-Student test. The two groups of patients to be compared were those in 2000 and 2005 and values of p < 0.05 were considered
Copyright © ABE&M todos os dir
eitos r
eser
vados.
to run the statistical tests. This study was submitted to and approved by the Ethics Committee in Research of Universidade Federal de Santa Catarina.
RESULTS
Cases of thyroid cancer
A total of 97 cases of thyroid cancer were diagnosed in 2000 while in 2005 this number was 305. Among these patients, 60 patients (61.85%) in 2000 and 161 patients (52.78%) in 2005 matched the criteria and were included in this study.
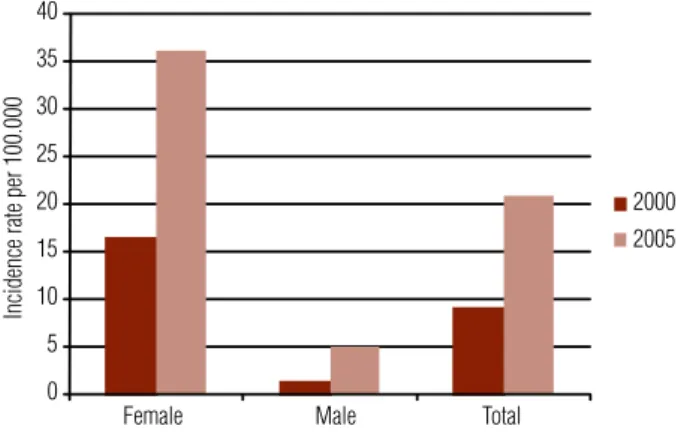
The incidence of thyroid cancer calculated for 2000 and 2005 was 8.99 and 20.90, respectively, per 100 thou-sand inhabitants. It corresponds to an increase of 132.33% between the yearly periods analyzed, or 26.46% per year. The incidence rates for women were 16.42 and 36.09 per 100 thousand inhabitants in 2000 and 2005 respectively, resulting in an increase of 119%. For men, the rate calcu-lated was 1.22 per 100 thousand inhabitants in 2000 and 5.01 per 100 thousand inhabi tants in 2005, an increase of 310% in the incidence rate (Figure 1).
of the study, a higher incidence of thyroid cancer was observed in caucasian patients. In 2000 and 2005, the rates were 85.29% (29 patients) and 84.90% (90 pa-tients) respectively, with no statistically significant dif-ference (p = 0.955).
Among the subjects in the study, in both years, a higher incidence of thyroid cancer was observed in pa-tients who had a higher education level than primary school, consisting of 24 patients (72.72%) in 2000 and 80 patients (74.07%) in 2005.
Most patients that participated in the study came from the private health system. In 2000 and 2005, only 6 (10%) and 19 (11.72%) patients, respectively, came from the public health system.
Surgical procedures
During the evaluated years, a statistically significant difference (p = 0.002) in the surgical approaches used was observed. Total thyroidectomy was performed in 81.13% of the patients (43 patients) in 2000 and in 94.80% of the patients (146 patients) in 2005. Infor-mation about other surgery procedures was also gathe-red. In 2000, 9.43% of the patients (five patients) were submitted to lobectomy, while 5.66% (three patients) were submitted to subtotal thyroidectomy and 3.77% (2 patients) to thyroid biopsy. The thyroid biopsies were performed in patients with anaplastic and folli-cular carcinomas, for which the surgery procedure was not viable and intended to confirm the diagnosis. The corresponding numbers for 2005 include: 1.96% of patients (three patients) submitted to lobectomy (two patients were later submitted to total thyroidectomy); 1.96% (three patients) submitted to subtotal thyroidec-tomy, and only one patient (1.30%), for whom surgery was not an option, had a thyroid biopsy in order to confirm the diagnosis.
Characteristics of surgical specimens
The average size of the tumors diagnosed in 2000 and
2005 was 1.51 cm (σ = 1,45) and 1.02 cm (σ = 0,91),
respectively, a statistically significant difference (p = 0.007). A comparison among the proportion of tumors with dimensions equal to or greater than one centime-ter, and tumors smaller than one centimeter was also statistically significant. In 2000 and 2005, 36.95% (17 tumors) and 61.48% of the tumors (83 tumors), re-spectively, showed a smaller dimension than one centi-meter (p = 0.003) (Figure 2).
0 5 10 15 20 25 30 35 40
Female Male Total
Incidence rate per 100.000
2000 2005
Figure 1. Incidence rate of thyroid cancer per 100.000 inhabitants in the Metropolitan area of Florianopolis according to sex, years 2000 and 2005.
Copyright © ABE&M todos os dir
eitos r
eser
vados.
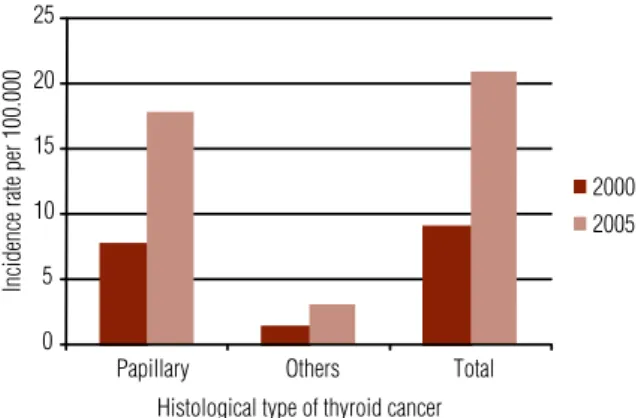
Papillary thyroid cancer was the histologic type with the largest incidence in both years: 85% (51 pa-tients) in 2000 and 85.62% (137 papa-tients) in 2005 (p = 0.81) (Figure 3). Follicular thyroid cancer represented 11.86% of the tumors (7 patients) and 13.20% of the tumors (21 patients) in 2000 and 2005, respectively. One case of anaplastic thyroid cancer was diagnosed in 2000 (1.69%) and one case of medullary thyroid cancer was diagnosed in 2005 (0.62%).
invasion was not found in 56.66% (85 patients), a non-statistically significant difference (p = 0.186). Lymphat-ic dissemination did not meet a statistLymphat-ically signifLymphat-icant difference either (p = 0.75) occurring in 12.24% of the patients (6 patients) in 2000 and in 14% of the patients (21 patients) in 2005.
Anatomopathologic exams
More anatomical pathology and cytological investiga-tions were undertaken by pathology services of the Metropolitan area of Florianopolis in 2005 than in 2000. Regarding the former, in 2000 a total of 620 exams were requested, while in 2005 this number was 1.858, which resulted in an increase of 199%. This increase was also detected in histopathology exams, since 198 exams were requested in 2000, while in 2005, 542 were requested, resulting in an increase of 173%.
In the two analyzed years, the rate of positive re-sults among exams performed was kept fairly constant. Among cytologic exams, the rates in 2000 and 2005 were 8.06% (50 exams) and 8.77% (163 exams) respec-tively (p = 0.61). For histopathologic exams, the per-centage of positive results relative to the total number of exams was 39.39% (78 exams) and 40.22% (218 ex-ams) in 2000 and 2005, respectively (p = 0.88).
Regarding the cytologic results of suspected thyroid cancer whose confirmation demanded post-surgical analysis, the rates found for 2000 and 2005 were, 23.7% (147 exams) and 29.7% (552 exams) respectively, a sta-tistically significant difference (p = 0.029).
Risk factors
A total of 36.36% of the patients (12 patients) submitted to surgical treatment in 2000 had a history of thyroid disease prior to the detection of cancer, while in 2005 there were 47 patients (37.30%), a non-statistically sig-nificant difference (p = 0.92). The existence of a family history of thyroid disease was observed in 42.85% of the patients (12 patients) in 2000 and in 43.51% of the patients (47 patients) in 2005, a non-statistically sig-nificant difference (p = 0.94). Previous family history of thyroid cancer was observed in 11.11% of cases (three patients) and 18.26% of cases (19 patients), in 2000 and 2005, respectively; again, no statistically significant difference (p = 0.37). Among the patients in the study, the prevalence of smokers was very similar in the two yearly periods analyzed: 8 patients (25.80%) in 2000 and 32 patients (26.01%) in 2005.
2000 2005
0 5 10 15 20 25 30 35 40 45 50
Tumor size
0-4 mm 5-9 mm
10-14 mm 15-19 mm 20-24 mm 25-29 mm 30-34 mm 35-39 mm ≥ 40 mm
N
um
be
r o
f c
as
es
o
f thyr
oi
d
ca
nc
er
Figure 2. Distribution of number of cases of thyroid cancer according to tumor size in the metropolitan area of Florianopolis, years 2000 and 2005.
2000 2005
0 5 10 15 20 25
Papillary Others Total
Incidence rate per 100.000
Histological type of thyroid cancer
Figure 3. Incidence rate of thyroid cancer per 100.000 inhabitants in the Metropolitan area of Florianopolis according to histological type, years 2000 and 2005.
In 2000, 84.3% of the patients (43 patients) had a unilateral tumor, while in 2005 this number was 68.27% (99 patients), with a statistically significant difference (p = 0.027). Another statistically significant difference (p = 0.027) was detected in the occurrence of multifocal tumors among the yearly periods analyzed. Specifically, 3.92% of the tumors (2 tumors) in 2000 and 15.86% of the tumors (23 tumors) in 2005 were multifocal in nature.
Copyright © ABE&M todos os dir
eitos r
eser
vados.
Thyroid cancer mortality
Despite the increasing incidence of thyroid cancer, the mortality rate has decreased (Figure 4). In 2000, four deaths caused by thyroid cancer were registered in the Metropolitan area of Florianopolis, while in 2005, three deaths were attributed to such neoplasm. These values are equivalent to a mortality rate of 0.59 and 0.38 per 100 thousand inhabitants in 2000 and 2005, respectively.
Regarding the gender, the mortality rate per 100 thousand inhabitants in 2000 was 0.58 for females and 0.61 for males, while in 2005, it was 0.25 for the for-mer and 0.52 the latter.
capitals (35). It has lead to a population with more ac-cess to health services, a fact that is possibly associated with more thyroid cancer diagnoses. The regional dif-ferences observed in incidence rates are also attributed, by Coeli and cols. (28), to the inaccuracy of cancer reg-istrations in Brazil.
The difference between incidence rates in Floria-nopolis Metropolitan area and those of international counterparts may be attributable to the fact that this area comprises a relatively small sample of the Brazil-ian population with good socio-economic conditions, while international studies comprised the populations of entire countries.
Given the high rate of thyroid cancer observed in the Metropolitan area of Florianopolis, mainly in wom-en, future studies are necessary to investigate this type of cancer in the region. To facilitate this action, the no-tification of this type of disease is extremely important. Among the possible risk factors analyzed in this study, the prevalence of gender, age, smoking, previous history and family history of thyroid disease were simi-lar in the two yearly periods analyzed and consistent with the numbers described in the literature. D’Avanzo and cols. (15) reported an association between previous benign thyroid diseases and the occurrence of thyroid cancer, with a higher association observed in the case of goiter and adenoma. The study also described a link between a family history of thyroid disease and the oc-currence of thyroid cancer; however, it was not speci-fied which type of disease has a higher risk.
The similar prevalence of the above mentioned risk factors in patients included in this study over both yearly periods suggests that the increase in the incidence of thy-roid cancer in the Metropolian area of Florianopolis can not be attributed to these factors. However, to properly evaluate the existence of risk factors for this neoplasm, it is necessary to perform longitudinal studies, as only these are able to determine the association between risk factors and the development of the disease.
The observed relevant increase in the number of thyroid anatomical pathology investigations performed during the periods analyzed, in association with more aggressive surgical treatment and a significant decrease in the average size of tumors, suggest that the main factor contributing to the increase in incidence of thy-roid cancer is a change in the approach used to evaluate thyroid nodules. Specifically, a more interventionist ap-proach is adopted in the Metropolitan area of Floriano-polis, which results in earlier diagnosis of the disease.
2000 2005
Rate per 100.000
Year
Incidence
Mortality
Figure 4. Incidence rate versus mortality rate of thyroid cancer per 100.000 inhabitants in the Metropolitan area of Florianopolis, years 2000 and 2005.
DISCUSSION
The incidence rate of thyroid cancer in the Metropoli-tan area of Florianopolis is higher than that observed anywhere else in Brazil (28) or in the rest of the world (2,22). The epidemiologic status of the patients in this study in terms of gender and age coincides with that reported in the international literature for patients with thyroid cancer, with a higher incidence in women in their fifth decade of life (2,33).
The educational level of the analyzed patients was considerably higher than the average in the Metropolitan area of Florianopolis, where about 70% of the popul a-tion has up to eight years of schooling (34). Besides this fact, most cases diagnosed in both yearly periods originated from the private health system, showing a higher number of thyroid cancers in the population with more economically favorable conditions. These findings are possibly associated with a broader access to diagnostic and therapeutic resources available to a high economic status population.
Copyright © ABE&M todos os dir
eitos r
eser
vados.
American studies show a total of 4% to 7% of the population with palpable thyroid nodules, 5% of which would be malignant. The prevalence is even higher if imaging exams such as ultrasound are used to de-tect thyroid nodules (1). Due to its high prevalence, a change towards a more aggressive approach of thyroid nodules may be associated with an increase in the inci-dence of thyroid cancer.
The relevant increase in the total number of FNAs undertaken in 2005 compared to 2000 shows that there was, in fact, a change in the management of thy-roid nodules. Since the indication for FNA is based on radiologic criteria, particularly for nodules with a small size, it would be advisable to analyze the number of ultrasound exams performed in the Metropolitan area of Florianopolis during the period of this study. Nev-ertheless, the difficulty in obtaining such data, due to the progressive increase in the number of ultrasound equipment in medical clinics, made it difficult to get this information. Leenhardt and cols. (36), however, when analyzing data from the French Cancer Report, mentioned that the increase in the number of thyroid ultrasounds in France was seven times higher than the increase in the number of FNAs.
The change in therapeutic approach of thyroid nod-ules includes not only the increase in number of surgi-cal procedures performed, but also a change in the type of procedures adopted. Results of this study show an increase in total thyroidectomy rates as also described
by Bilimoria and cols. (37). The increase observed in
the number of bilateral and multifocal tumors may be explained by this change in surgical approaches, and thus is probably not associated with an increase in tu-mor aggressiveness.
Total thyroidectomy is the recommended treatment for many types of thyroid tumors (38). However, the American Thyroid Association (39) and the European Thyroid Cancer Task Force (40) accept lobectomy as a viable option for a single well-differentiated thyroid cancer, smaller than 1 cm, with no evidence of nodal or distant metastases (very low risk patients).
Total thyroidectomy is a procedure with a small, but relevant risk of complications, including perma-nent hypoparathyroidism and damage in the recurrent laryngeal nerve. This damage can result in voice quality disorders, as well as respiratory complications due to chronic aspiration (2). Thus, it is a procedure with in-dication criteria that should be well-established.
The increase in the number of thyroid cancer in the Metropolitan area of Florianopolis was observed mainly for the papillary carcinoma type, but also for the follicu-lar and medulfollicu-lary types. Nevertheless, as the number of patients diagnosed consisted of a small sample includ-ing these two last types, such data require the analysis of a larger population to confirm or refute such an in-crease in incidence.
Thyroid cancer, especially the papillary type, is a fre-quent finding in autopsies of patients who had no prior knowledge of this diagnosis. Such evidence raises doubt as to the need of submitting all diagnosed patients with papillary thyroid microcarcinoma to surgical treatment. Davies and Welch (2) analyzed diagnosed cases in the United States over 29 years and concluded that further studies were needed to determine the possibility of us-ing less aggressive approaches in the investigation of thyroid nodules, which could lead to the classification of papillary thyroid microcarcinoma as a normal find-ing. However, despite the good prognosis associated with papillary microcarcinoma, there are reports of tu-mors with high aggressiveness (41).
Despite the increasing incidence of thyroid cancer, a decrease in mortality rates was noticed in the Metro-politan area of Florianopolis. This is compatible with the results reported in the literature (27,42), and it is probably due to the increase in the number of early di-agnosis with consequent better tumor prognosis.
Various factors associated with a higher degree of ag-gressiveness of the tumor, including post-surgery criteria, are well-established. Pelegriti and cols. (33) analyzed 299 cases of papillary thyroid cancer smaller than 1.5 cm in which factors associated with malignancy of this type of lesion were evaluated. The presence of multifocality, high levels of thyroglobulin post-surgery, and angiolymphatic invasion were associated with a higher degree of tumor aggressiveness. In terms of pre-surgery factors, only the existence of previous Graves’ disease and non incidental findings were associated with higher cancer aggressive-ness. Current guidelines, such as the European and Bra-zilian (40,38) consensuses, consider the following factors as indicators of malignancy in thyroid nodules: history of familial thyroid cancer, exposure to radiation during childhood, rapid growth, vocal hoarseness, hard and ir-regular consistency, ipsilateral cervical lymphadnopathy and fixation of the nodule to extrathyroidal tissues.
Copyright © ABE&M todos os dir
eitos r
eser
vados.
of criteria with a higher predictive value of malignancy for follicular lesions, are of outmost importance. These factors would enable a more careful analysis of patients who really need surgical treatment, thus reducing the number of patients submitted to surgery for a condi-tion that could remain indefinitely asymptomatic.
Acknowledgments: the authors wish to thank to the doctors of the Metropolitan region of Florianopolis for the collaboration during the gathering of information on patients with thyroid cancer.
Disclosure: no potential conflict of interest relevant to this article was reported.
REFERENCES
Hegedus L. Clinical practice. The thyroid nodule. N Engl J Med. 1.
2004;351(17):1764-71.
Davies L, Welch HG. Increasing incidence of thyroid cancer in the 2.
United States, 1973-2002. JAMA. 2006;295(18):2164-7.
Montanaro F, Pury P, Bordoni A, Lutz JM. Unexpected additional 3.
increase in the incidence of thyroid cancer among a recent birth cohort in Switzerland. Eur J Cancer Prev. 2006;15(2):178-86. Truong T, Rougier Y, Dubourdieu D, Guihenneuc-Jouyaux C, Orsi L, 4.
Hemon D, et al. Time trends and geographic variations for thyroid cancer in New Caledonia, a very high incidence area (1985-1999). Eur J Cancer Prev. 2007;16(1):62-70.
Levi F, Randimbison L, Te VC, La Vecchia C. Thyroid cancer in Vaud, 5.
Switzerland: an update. Thyroid. 2002;12(2):163-8.
Scheiden R, Keipes M, Bock C, Dippel W, Kieffer N, Capesius C. 6.
Thyroid cancer in Luxembourg: a national population-based data report (1983-1999). BMC Cancer. 2006;6:102.
Burgess JR, Tucker P. Incidence trends for papillary thyroid carci-7.
noma and their correlation with thyroid surgery and thyroid fine-needle aspirate cytology. Thyroid. 2006;16(1):47-53.
Smailyte G, Miseikyte-Kaubriene E, Kurtinaitis J. Increasing 8.
thyroid cancer incidence in Lithuania in 1978-2003. BMC cancer. 2006;6:284.
Liu S, Semenciw R, Ugnat AM, Mao Y. Increasing thyroid cancer 9.
incidence in Canada, 1970-1996: time trends and age-period-co-hort effects. Br J Cancer. 2001;85(9):1335-9.
Trimboli P, Ulisse S, Graziano FM, Marzullo A, Ruggieri M, Calva-10.
nese A, et al. Trend in thyroid carcinoma size, age at diagnosis, and histology in a retrospective study of 500 cases diagnosed over 20 years. Thyroid. 2006;16(11):1151-5.
Colonna M, Guizard AV, Schvartz C, Velten M, Raverdy N, Molinie 11.
F, et al. A time trend analysis of papillary and follicular cancers as a function of tumour size: A study of data from six cancer regis-tries in France (1983-2000). Eur J Cancer. 2007;43(5):891-900. Lubina A, Cohen O, Barchana M, Liphshiz I, Vered I, Sadetzki S, et 12.
al. Time trends of incidence rates of thyroid cancer in Israel: what might explain the sharp increase. Thyroid. 2006;16(10):1033-40. Cardis E, Howe G, Ron E, Bebeshko V, Bogdanova T, Bouville A, et 13.
al. Cancer consequences of the Chernobyl accident: 20 years on. J Radiol Prot. 2006;26127-40.
Lind P, Kumnig G, Heinisch M, Igerc I, Mikosch P, Gallowitsch HJ, 14.
et al. Iodine supplementation in Austria: methods and results. Thyroid. 2002;12(10):903-7.
D’Avanzo B, La Vecchia C, Franceschi S, Negri E, Talamini R. His-15.
tory of thyroid diseases and subsequent thyroid cancer risk. Can-cer Epidemiol Biomarkers Prev. 1995;4(3):193-9.
Haselkorn T, Bernstein L, Preston-Martin S, Cozen W, Mack WJ. 16.
Descriptive epidemiology of thyroid cancer in Los Angeles Coun-ty, 1972-1995. Cancer Causes Control. 2000;11(2):163-70. Ch
17. en GG, Vlantis AC, Zeng Q, van Hasselt CA. Regulation of cell growth by estrogen signaling and potential targets in thyroid cancer. Curr Cancer Drug Targets. 2008;8(5):367-77.
Lewinski A, Wojciechowska K. Genetic background of carcinogene-18.
sis in the thyroid gland. Neuro Endocrinol Lett. 2007;28(2):77-105. Schlienger JL, Grunenberger F, Vinzio S, Goichot B. Smoking and 19.
the thyroid. Annales d’Endocrinologie. 2003;64(4):309-15. Leenhardt L, Bernier MO, Boin-Pineau MH, Conte Devolx B, Ma-20.
rechaud R, Niccoli-Sire P, et al. Advances in diagnostic practi-ces affect thyroid cancer incidence in France. Eur J Endocrinol. 2004;150(2):133-9.
Roti E, Rossi R, Trasforini G, Bertelli F, Ambrosio MR, Busutti L, 21.
et al. Clinical and histological characteristics of papillary thyroid microcarcinoma: results of a retrospective study in 243 patients. J Clin Endocrinol Metab. 2006;91(6):2171-8.
Farahati J, Geling M, Mader U, Mortl M, Luster M, Muller JG, et 22.
al. Changing trends of incidence and prognosis of thyroid car-cinoma in lower Franconia, Germany, from 1981-1995. Thyroid. 2004;14(2):141-7.
Zhang Y, Zhu Y, Risch HA. Changing incidence of thyroid cancer. 23.
JAMA. 2006;296(11):1350; author reply.
Mulla ZD, Margo CE. Primary malignancies of the thyroid: epide-24.
miologic analysis of the Florida Cancer Data System registry. Ann Epidemiol. 2000;10(1):24-30.
Kohrle J. Environment and endocrinology: the case of thyroidolo-25.
gy. Annales d’Endocrinologie. 2008;69(2):116-22.
Ward L S, Graf H. Câncer da tiróide: aumento na ocorrência da 26.
doença ou simplesmente na sua detecção? Arq Bras Endocrinol Metab. 2008;52:1515-6.
Ward LS. Epidemiology of thyroid cancer in Brazil: pointing di-27.
rections in the health policy of the country. Arq Bras Endocrinol Metab. 2005;49(4):474-6.
Coeli CM, Brito AS, Barbosa FS, Ribeiro MG, Sieiro AP, Vaisman 28.
M. Incidence and mortality from thyroid cancer in Brazil. Arq Bras Endocrinol Metab. 2005;49(4):503-9.
Brasil. Ministério da Saúde/SAS/INCA. Câncer no Brasil: dados 29.
dos registros de base populacional, volume 3. Rio de Janeiro: INCA; 2003.
Instituto Brasileiro de Geografia e Estatística. Censo 2000 [data-30.
base on the Internet]. [cited 2007 Apr 08]. Available from: http:// www.ibge.gov.br/censo/default.php
Instituto Brasileiro de Geografia e Estatística [database on the In-31.
ternet]. Estimativas populacionais. [cited 2007 Apr 08]. Available from: http://www.ibge.gov.br/home/estatistica/populacao/estima-tiva2006/estimativa.shtm
Datasus [database on the Internet]. Sistema de Informação sobre 32.
mortalidade; [cited 2007 Apr 08]. Available from: http://tabnet.da-tasus.gov.br/cgi/deftohtm.exe?sim/cnv/obtSC.def
Pellegriti G, Scollo C, Lumera G, Regalbuto C, Vigneri R, Belfio-33.
re A. Clinical behavior and outcome of papillary thyroid cancers smaller than 1.5 cm in diameter: study of 299 cases. J Clin Endo-crinol Metab. 2004;89(8):3713-20.
Datasus [database on the Internet]. Informações de saúde demo-34.
gráficas e econômicas; [cited 2007 Apr 08]. Available from: http:// tabnet.datasus.gov.br/cgi/deftohtm.exe?ibge/cnv/alfSC.def Programa das Nações Unidas para o Desenvolvimento. [cited 35.
2007 Apr 08]. Available from: http://www.pnud.org.br/administra-cao/reportagens/index.php?id01 = 2011&lay = apu
Leenhardt L, Grosclaude P, Cherie-Challine L. Increased incidence 36.
Copyright © ABE&M todos os dir
eitos r
eser
vados.
Bilimoria KY, Bentrem DJ, Linn JG, Freel A, Yeh JJ, Stewart AK, et 37.
al. Utilization of total thyroidectomy for papillary thyroid cancer in the United States. Surgery. 2007;142(6):906-13.
Maia AL, Ward LS, Carvalho GA, Graf H, Maciel RM, Maciel LM, 38.
et al. Thyroid nodules and differentiated thyroid cancer: Brazilian consensus. Arq Bras Endocrinol Metab. 2007;51(5):867-93. Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel 39.
SJ, et al. Management guidelines for patients with thyroid nodu-les and differentiated thyroid cancer. Thyroid. 2006;16(2):109-42. Pacini F, Schlumberger M, Dralle H, Elisei R, Smit JW, Wiersinga W. 40.
European Thyroid Cancer Taskforce. European consensus for the
management of patients with differentiated thyroid carcinoma of the follicular epithelium. Eur J Endocrinol. 2006;154(6):787-803. Ito Y, Uruno T, Nakano K, Takamura Y, Miya A, Kobayashi K, et al. An 41.
observation trial without surgical treatment in patients with pa-pillary microcarcinoma of the thyroid. Thyroid. 2003;13(4):381-7. Gomez Segovia I, Gallowitsch HJ, Kresnik E, Kumnig G, Igerc I, 42.