www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Epidemiological
survey
of
mucus
extravasation
phenomenon
at
an
oral
pathology
referral
center
during
a
43
year
period
夽
Thâmara
Manoela
Marinho
Bezerra
a,
Bárbara
Vanessa
de
Brito
Monteiro
b,
Águida
Cristina
Gomes
Henriques
c,
Marianne
de
Vasconcelos
Carvalho
d,
Cassiano
Francisco
Weege
Nonaka
e,
Márcia
Cristina
da
Costa
Miguel
f,∗aUniversidadeFederaldoCeará(UFC),Fortaleza,CE,Brazil
bUniversidadeFederaldeCampinaGrande(UFCG),CampinaGrande,PB,Brasil cUniversidadeFederaldaBahia(UFBA),Salvador,BA,Brazil
dUniversidadedePernambuco(UPE),Arcoverde,PE,Brazil
eUniversidadeEstadualdaParaíba(UEPB),CampinaGrande,PB,Brazil fUniversidadeFederaldoRioGrandedoNorte(UFRN),Natal,RN,Brazil
Received1June2015;accepted11September2015 Availableonline6January2016
KEYWORDS
Mucocele; Ranula;
Minorsalivaryglands
Abstract
Introduction:Mucoceles are common benign pseudocystic lesions of the oral cavity; their main etiological factors are trauma and ductal obstruction. Two histological patterns are found:mucusretentionphenomenon(MRP)andmucusextravasationphenomenon(MEP).Mucus extravasationphenomenonisthemorecommonhistologicalsubtypeanditmainlyaffectsthe lowerlip.Theknowledgeofitsmainclinicalfeaturesandmanagementisimportanttoassist healthprofessionalsinclinicalpractice.
Objective:Thisstudyaimedtodeterminetherelativefrequencyanddistributionoforal muco-celesinanoralpathologyreferencecenter.
Methods:Cross-sectionalhistoricalstudy thatanalyzed allcasespathologicallydiagnosedas mucusextravasationphenomenonbythedepartmentofanatomicpathologyofanoralpathology referralcenterfromJuneof1970toMayof2014,consideringtheclinicalcharacteristicsof thelesionandthoserelatingtothepatient.SPSSv.20.0softwarefor Windowswasusedfor descriptiveanalysis.
Results:During43years,719casesofmucusextravasationphenomenon(54.7%menand45.3% women)wereregistered,withthelowerlipasthemostcommonlyaffectedsite(n=484;67.3%).
夽 Pleasecitethisarticleas:BezerraTM,MonteiroBV,HenriquesAC,deVasconcelosCarvalhoM,NonakaCF,daCostaMiguelMC.
Epidemi-ologicalsurveyofmucusextravasationphenomenonatanoralpathologyreferralcenterduringa43yearperiod.BrazJOtorhinolaryngol.
2016;82:536---42.
∗Correspondingauthor.
E-mail:[email protected](M.C.daCostaMiguel).
http://dx.doi.org/10.1016/j.bjorl.2015.09.013
Theaverageageofpatientswas20.8years(SD±14.4)withapeakoccurrenceinthesecond decadeoflife.Mostprofessionalshadoralmucocele/ranula(n=606;84.3%)astheinitialclinical impression.
Conclusion: Mucusextravasationphenomenonisalesionthatprimarilyaffectsyoungpatients, affectingmainlythelowerlip,andiscommonlyfoundinoraldiagnosticservices.
© 2015 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE
Mucocele; Ranula;
Glândulassalivares menores
Levantamentoepidemiológicodefenômenodeextravasamentodemucodeum centrodereferênciaempatologiaoralporumperíodode43anos
Resumo
Introduc¸ão: Mucoceles são lesões pseudocísticas benignas comuns da cavidade oral, que possuem como principais fatores etiológicos trauma ou obstruc¸ão ductal. Dois padrões histopatológicos são encontrados: fenômeno de retenc¸ão de muco (FRM) e fenômeno de extravasamentodemuco(FEM).OFEMéosubtipohistológicomaiscomumetemcomoprincipal localdeacometimentoolábioinferior.Oconhecimentoacercadesuasprincipais característi-casclínicaseformasdetratamentosefazimportanteparaauxiliarprofissionaisdasaúdena práticaclínica.
Objetivo: Estetrabalhoobjetivoudeterminarafrequênciarelativaeadistribuic¸ãodas muco-celesoraisemumcentrodereferênciaempatologiaoral.
Método: Estudotransversaldecaráterhistórico,noqualforamanalisadososcasos diagnosti-cadoshistopatologicamentecomoFEMpeloservic¸odeanatomiapatológicadeum centrode referênciaempatologiaoral,noperíododejunhode1970amaiode2014,considerando-se variáveisclínicasdalesãoerelativasaopaciente.OprogramaestatísticoSPSS20.0forWindows
foiutilizadoparaaanálisedescritivadosdados.
Resultados: Durante43anosforamobservados719casosdeFEM(54,7%homense45,3% mul-heres),sendoolábioinferior(n=484;67,3%)olocaldeprincipalacometimento.Amédiade idadedospacientesfoide20,8anos(DP±14,4),comumpicodeocorrêncianasegundadécada devida.Amaioriadosprofissionaistevemucoceleoral/rânula(n=606;84,3%)comoprimeira hipóteseclínica.
Conclusão:OFEMéumalesãoqueafetaprincipalmentepacientesjovens,acometendo pref-erencialmenteolábioinferior,sendocomumenteencontradanosservic¸osdediagnósticooral. © 2015 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Mucoceles arecommonbenignpseudocysticlesionsof the oralcavitythatdevelopsecondarytoleakageorretentionof mucousmaterialfromsalivaryglands,principallytheminor salivaryglands.1Theselesionsaccountfor70%ofcysticand
pseudocystic lesionsof the salivary glands, thus they can appearanywhereontheoralmucosawherethereisa sali-varygland.1,2
Etiologicfactorsinvolvedinmucoceleformationinclude traumaandductalobstrction,3,4whichmayleadto
forma-tionoftwohistologicalpresentations:thephenomenonof mucusretentionorextravasation.1,5Themucus
extravasa-tionphenomena(MEP)areactuallypseudocysts,astheyare devoidofepitheliallining.Theextravasatedmucusinduces an inflammatory and granular reaction in an attempt to containtheextravasation.4,6Thistypeofmucoceleis
com-monlyfoundinminorsalivaryglands.7Themucusretention
phenomenon (MRP) induces formation of another type of
mucocele:themucusretention cyst or sialocyst.1 Mostof
thesegrowfrommajorsalivaryglandsandductsandhave the following etiological factors: sialolithiasis, periductal scarring,orinvasivetumors.5,7Histopathologically,MRPare
characterizedbyepitheliumliningcomingfromthepartially obstructedsalivaryduct.4
Clinically, there is no difference between the mucus extravasationandretentionphenomena,andboth present withincreasedvolumeofcysticappearance,arepainless, softtopalpation,andshowatransparentbluishcolor.2The
mostcommonsiteofextravasationmucocelesisthelower lip,whichisalsothemostsusceptibleplacetoinjuries.Such locationis less common in retention mucoceles,2,5 which
mayaffectanyothersiteoftheoralcavity.8Extravasation
mucocelesaffectyoungpatients(20---30years)andusually resolve spontaneously, requiring surgical excision in some cases.2 Micro-marsupialization, cryosurgery, steroid
Theaimofthisstudywastoperformanepidemiological surveyoforalmucocelecasesdiagnosedintheDepartment ofAnatomicPathologyoftheOralPathologyDisciplineofa universityintheperiodof1971---2014,aswellastodescribe themainclinicalcharacteristicsandtreatment,inorderto assisthealthprofessionalsinclinicalpractice.
Methods
Cross-sectional,retrospective,historicalstudy,approvedby the ResearchEthics Committee under No. #675,422, that included719casesoforalmucocelesselectedfrom11,589 casesrecordedinthefilesofthePathologicAnatomy Labo-ratorybetweenJuneof1970andMayof2014.
Thecollectionprocedurewasbasedontheinformation inthehistopathology reportsandmedicalrecordsof biop-sies,whichweretranscribedintoastandardfiledeveloped specificallyforthisanalysis.Theassessedvariablesrelated tothepatientweregender,age,andrace.Regardingclinical features of oral mucocele, the following data were col-lected:lesionlocation,shapeofthemain lesion,surface, symptoms,duration,size,historyoftrauma,sizevariation, clinicaldiagnosis,andtypeofbiopsyperformed.Itis note-worthythatbecauseranulaisconsideredaclinicalvariant ofmucoceles,8itwasdecidedtogroupthemtogetherinthis
study.
Results
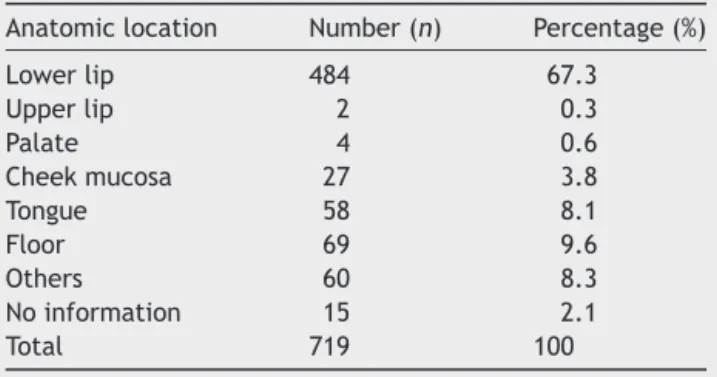
The719casesoforalmucocelesrepresent5.8%ofallcases registeredbytheoralpathologylaboratoryduringthestated period.Consideringtheanatomicalsite,itwasfoundthat thelowerlipwasthemostaffectedregion(67.3%;Table1). Regardingpatients’gender,thelesionwasmorefrequentin females(54.7%).Theaverageageofpatientswithmucocele was20.8years(SD±14.4),witharangeof1---82yearsold.A higherprevalenceoflesionswasobservedinwhitepatients (48.4%;Table2).
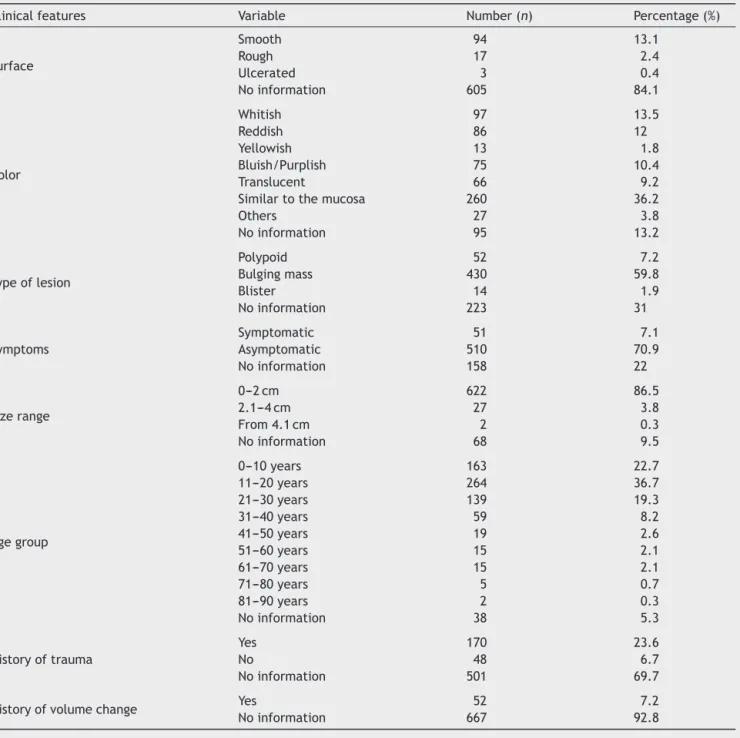
The most frequent clinical aspects of oral mucoceles wereanodular(59.8%)asymptomatic (70.9%)lesion, with a smooth surface (13.1%), measuring on average 0.9cm (SD±0.70),withthesamecolorasthemucousmembrane (36.2%),andmeandurationof20weeks(SD±28.7),ranging fromoneweektosixyears(Table3).Regardingthe medi-calhistory,somepatientsreportedprevioustraumatothe
Table1 Distributionofabsoluteandrelativefrequencies regardingthelocationoforalmucoceles.
Anatomiclocation Number(n) Percentage(%)
Lowerlip 484 67.3
Upperlip 2 0.3
Palate 4 0.6
Cheekmucosa 27 3.8
Tongue 58 8.1
Floor 69 9.6
Others 60 8.3
Noinformation 15 2.1
Total 719 100
Table2 Distributionofabsoluteandrelativefrequencies accordingtoskincolorofpatientsaffectedbyoralmucocele.
Skincolor Number(n) Percentage(%)
Leucoderma 348 48.4
Melanoderma 135 18.8
Feoderma 133 18.5
Noinformation 103 14.3
Total 719 100
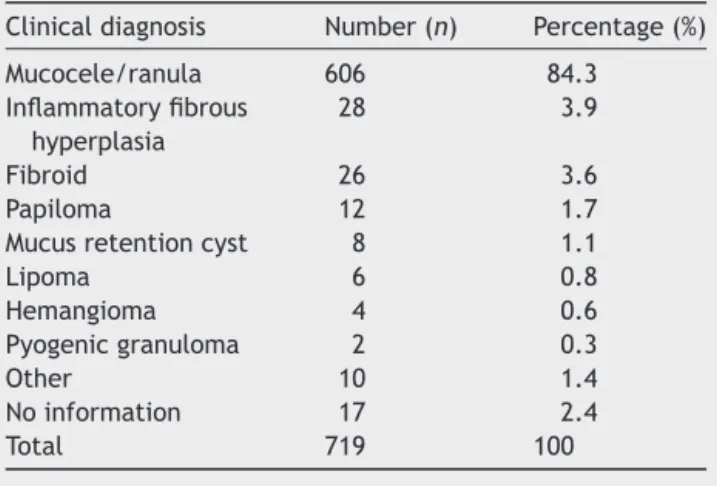
formation of thelesion (23.6%)andonly 7.2%reportedat thetimeoftheinterviewthattheynoticedthelesion show-ing variation in size during the clinical course (Table 3). Uponfirstcontactwiththelesion,mostdentistslistedoral mucocele/ranula (84.3%) as their first clinical impression (Table4).Ultimately,excisional biopsywasthetreatment ofchoiceformostlesions(83.3%).
Discussion
The incidence of mucocele is generallyhigh in the popu-lation,with2.5lesionsper1000patients.2Thisinjurywas
the17thmostcommonaffectingtheoralcavity, represent-ing 0.08% of oral lesionsin a study in Brazil.10 The term
mucoceleisstrictlyclinicalandservestodescribeincreased volumecausedbysalivacomingfrombrokenorcloggedduct ofminorsalivarygland.Oralmucoceleslocatedinthefloor ofthemoutharecalledranulaandcommonlyoriginatefrom thebodyofthesublingualgland,andoccasionallyfrom Riv-ini’sductorWharthon’sduct.11
Amongthebenignlesionsofminorsalivaryglands, muco-cele isthe mostcommon.8,12,13 Cecconietal.5 found that
mucoceleaccounts for 4.61% oforal cavity biopsies, indi-catingthatit isalesioncommonly foundinoral medicine services.Similarly,a15-yearretrospectivestudybyMohan etal.14found393salivaryglandlesions,ofwhich216were
reportedasnon-neoplasticlesions,withmucocelebeingthe most prevalent lesion (54.5%). These findings are similar to data from this study, where oral mucocele accounted for 5.8% of all lesions diagnosed during 44 years of the Pathologic AnatomyLaboratoryservice of theDepartment ofDentistryofauniversity.
Minorsalivaryglandsarefoundanywhereinthemouth, exceptthegums.8Thus,retentionandextravasation
muco-celes are commonly found in different locations, with no clinical differences between them.2,15,16 To Bhargava
etal.,6histopathologicalexaminationiscrucialtoconfirm
theclinicaldiagnosis.Microscopically,mucousextravasation phenomenaarepseudocystsbecausetheyhave no epithe-lialwallcovering,andoccurinthreeevolutionaryphases. First,thereismucinspillintothesurroundingtissue,where someleukocytesandhistiocytesareseen.Second,the gran-ulationreactionappears,withthepresenceofhistiocytes, macrophages, and multinucleated giant cells associated with a foreign body reaction. Later, in the third stage, thereistheformation ofapseudocapsulewithout epithe-lium around the mucosa, comprised of connective tissue cells.2 The retention cystscharacteristically present with
Table3 Distributionofabsoluteandrelativefrequenciesregardingclinicalfeaturesoforalmucoceles.
Clinicalfeatures Variable Number(n) Percentage(%)
Surface
Smooth 94 13.1
Rough 17 2.4
Ulcerated 3 0.4
Noinformation 605 84.1
Color
Whitish 97 13.5
Reddish 86 12
Yellowish 13 1.8
Bluish/Purplish 75 10.4
Translucent 66 9.2
Similartothemucosa 260 36.2
Others 27 3.8
Noinformation 95 13.2
Typeoflesion
Polypoid 52 7.2
Bulgingmass 430 59.8
Blister 14 1.9
Noinformation 223 31
Symptoms
Symptomatic 51 7.1
Asymptomatic 510 70.9
Noinformation 158 22
Sizerange
0---2cm 622 86.5
2.1---4cm 27 3.8
From4.1cm 2 0.3
Noinformation 68 9.5
Agegroup
0---10years 163 22.7
11---20years 264 36.7
21---30years 139 19.3
31---40years 59 8.2
41---50years 19 2.6
51---60years 15 2.1
61---70years 15 2.1
71---80years 5 0.7
81---90years 2 0.3
Noinformation 38 5.3
Historyoftrauma
Yes 170 23.6
No 48 6.7
Noinformation 501 69.7
Historyofvolumechange Yes 52 7.2
Noinformation 667 92.8
duringsurgery,whenthefibrouswallofthelesionappears thick,itmaybeasalivaryglandneoplasm.However, regard-lessofthelesion wallthicknessandcharacteristicclinical findings,itisrecommendedtosendaportionfor histopatho-logicalexaminationtoconfirmtheclinicalsuspicion.
Extravasation mucoceles are the most common subtype8,13 and often appear in the lower lip.2
How-ever,theretention-typemucocelesarerarelyfoundatthat location,5andmayappearelsewhereintheoralcavity,2as
theyare moreclosely related tomajor salivaryglands.4,6
Themostfrequentlyaffectedsitesforretentionmucoceles in the minor salivary glands are the upper lip, palate, cheeks, oral floor, and maxillary sinus.5,8 In the present
study,allcasesanalyzedwereextravasationmucocele.
Among the 719 mucoceles analyzed in this study, the majority (67.2%) occurred in the lower lip. Several pub-lishedepidemiologicalstudiesvalidatethisfinding.2,5,10,12,13
Thelower lipis the anatomicsitein theoral cavity most pronetotrauma,especiallyinthepremolarregion.2,17This
factexplainsthe highincidenceof extravasation mucoce-les in this region, as trauma is suggested as the primary etiologicfactoroftheselesions.5,14ToKhannaetal.,18
Table4 Distributionofabsoluteandrelativefrequencies regardingthemainclinicalhypothesisoforalmucocele.
Clinicaldiagnosis Number(n) Percentage(%)
Mucocele/ranula 606 84.3 Inflammatoryfibrous
hyperplasia
28 3.9
Fibroid 26 3.6
Papiloma 12 1.7
Mucusretentioncyst 8 1.1
Lipoma 6 0.8
Hemangioma 4 0.6
Pyogenicgranuloma 2 0.3
Other 10 1.4
Noinformation 17 2.4
Total 719 100
(n=676;64.5%),butalsothemostaffectedsiteofallsoft tissue injuries associated with trauma (n=815; 29.5%).12
Althoughitwasnotpossibleinthisstudytocollect informa-tionregardinghistoryoftraumain69.7%ofbiopsyrecords,a considerableproportionofpatients(23.6%)reportedhistory ofprevioustrauma beforethelesionformation. Traumais theetiologicalfactormostwelldocumentedandaccepted instudiesoforalmucoceles.6
According to some studies in the literature, there is nodifferenceinthe incidenceoforal mucocelesbetween genders,6,17,19 similar to the present study. However, in
otherstudies,theincidenceofmucocelebetweengendersis quitevariable,withcasesofhigherprevalencebothamong women20 and among men.10,12,16 According to an Indian
study,menintheseconddecadeoflifearemostaffectedby mucoceleduetomanypsychologicalproblems,leadingthem tothehabitof bitingthe lip,which wouldcauseinjury.21
Despitethesedifferencesbetweenstudies,theyall recog-nizethattraumaisthemainetiologicalagentforthistype ofinjury,withvariationsbetweenthesexesonthetrauma origin(stress,psychologicalfactor,bite,etc.).
Extravasationmucocelesaffectpatientsofallages,with ahigh incidenceinthe second decadeof life.2,6,8,10,12,19,20
Incontrast,MRPcommonlyaffectolderindividuals.1,4,20 In
agreementwiththeliterature,theagegroupmostaffected inthisstudywastheseconddecadeoflife(Table3). Further-more,acaseofmucoceleinaone-year-oldchildwasfound. Mucoceles can be congenital or arise immediately after birth,buttheyarerareinchildrenunderoneyearofage.6,13
Clinicalpresentationoforalmucocelemayvary depend-ing on the lesion depth.10 Those located just below the
mucosa present superficially with the clinical features of avesicleorblister;thoselocatedintheuppersubmucosa comprisetheclassicmucoceles,withtheclinicalfeatureof anodule.8ThesevariationsareseenindetailinTable3.The
colorofmucocelesvariesbetweenmucosalcolor (pink)to bluish,andthedepthoftissuedamagealsohasaninfluence in this regard.5,7 Superficial lesions cause tissue stretch,
whichmakesthetissuethinnerandcyanoticandcauses vas-cular congestion, resulting in bluish lesions.2,5,8 However,
deeper mucoceles arewell-circumscribed massescovered by normal oral mucosa.8 The size of the lesion and the
elasticityofitsliningtissueareotherfactorsthatinfluence
thisclinicalaspect.7,21Inthepresentstudy,oralmucoceles
simulatedthesefindings(Table3).
Despite the clinical variations of mucoceles identified in this study, they are small and their appearance is pathognomonic:8 nodular lesion; asymptomatic; smooth
surface;and withavarietyof colors,suchasblue, trans-parent,pink, and whitish.2,5,6 The lesionsmay besolitary
or multiple, and do not have constant duration, ranging fromafew daystothreeyears.8Thus,despite mucoceles
beingaclinicaldiagnosis,2,8,10 itusuallyisnotdifficultfor
thedentisttoidentifythem,whichfacilitatesthetargeted treatment. These findings can be observed in this study wheremostprofessionals(78.4%)indicatedmucoceleasthe initialclinical impression,whichresulted intheexcisional biopsy asthe primary treatment of choice (83.4%). Thus, the patient’s medical history combined with information aboutthelocation,historyoftrauma,rapidonset,change in size, lesion color and consistency lead to the correct diagnosis of the lesion and clinical management by the professional.6Itisnoteworthythatsomespecificcasesmay
require further evaluation for diagnosis, such as routine X-rays, ultrasound, or methods of advanced diagnostics (computedtomographyandmagneticresonanceimaging)in ordertobettervisualizetheshape,diameter,position,and to determine the source of the lesion.1,8 The cytological
techniqueoffine-needleaspirationisauseful toolfor the diagnosisofpatientswithnodulesandmassesinthesalivary glands,especiallywhenconsideringangiomatouslesionsin thedifferentialdiagnosis.1,2
Inmostcases,althoughtheclinicaldiagnosisofmucocele doesnotofferdifficultiesfortheprofessional,itssimilarity tootherlesionsthatcanaffecttheoral cavityiscommon. Superficialmucocelemaybeconfusedwithscarpemphigoid, bullouslichenplanus,orherpes.22,23Thedifferentially
diag-nosis of deeper mucoceles includes lipoma, hemangioma, orallymphangioma,benignandmalignanttumorsofsalivary glandorigin, varicosevein, irritationfibroma,oral lymph-epithelial cyst, gingival cyst of the adult, tissue abscess, cysticercosis,pyogenicgranuloma,andothers.8
Itisnoteworthythatsomesuperficialmucoceleswitha historyofrecurrencehavebeenassociatedwithorallichen planusandchronicgraftversushostdisease.22,23ToBermejo
et al.,22 the patient’s oral mucosa with erosive lichen
planusundergoesconstanterosionandre-epithelialization, enabling the rupture of a small output of the salivary gland duct, which causes mucus accumulation below the epithelium. There is also the possibility that the inflam-matory process may play a role in the pathogenesis of recurrent mucoceles, as lymphocytic infiltrate can block theductofaccessorygland,whichwouldinduceits disrup-tionandsubepithelialextravasationofmucus.23Thecorrect
identification of recurrent superficial mucocele andother conditions thatmay beassociated withit contribute toa betterclinicalmanagementofpatients.
percentagedoesnotcorrespondtotherealityofthis find-ing,asmuchofthebiopsyrecordsarestructured,thereis no room for additional information that may be relevant notonlytothecorrecthistopathologicaldiagnosisbutalso forfutureepidemiologicalstudiesthatusetheserecordsas tools.Furthermore,avariationinsizeisavery characteris-ticclinicalfeatureoforalmucoceles.AccordingtoCecconi et al.5 it occurs due to rupture, especially in superficial
lesions,or reabsorptionof salivaandsubsequent accumu-lationofmucus.5,8Likewise,theoccurrenceofatraumain
thewoundregionwasrecordedinonly23.6%ofcases,while 69.7%didnotaddthisinformation(Table3).Similarlytothe previousdata,itdoesnotmatchtheexpected,andmayalso betreated,inthiscase,asabsenceofinformation.Ahistory oftrauma iswidelyreportedintheliterature asthemain causeofextravasationmucocele.8
It wasfound that mostoral mucoceles (n=510; 70.9%) were asymptomatic, asonly 7.1% (n=51)presented some symptoms(Table3).Aclinicopathological studyof 25oral mucoceles byBagán Sebastianet al.24 found that only4%
ofpatientshadsomediscomfort,butnotpain.Accordingto Baurmash,7mucocelesgreaterthan1.5cmarelocatedmore
deeplyinthetissues.Thus,minorlesionsbringless discom-forttothepatientbecausetheyaremoresuperficial,and arelocatedin less vascularizedtissue layersandless rich in nerve structures. In addition,large lesionsmay impair speaking or chewing.5,7 In the present study, onaverage,
patientswithoralmucolelestookfourmonthstoseek treat-ment,andsomeexhibitedfiveyearsofevolution.According toBhargavaetal.,6becausetherearenopainfulsymptoms,
it is usually the professional who detects the lesion in a routineoralexamination.
There arenodifferences inthe managementof reten-tionandextravasationmucoceles, andsurgicalremovalis the standard method widely used for both.2,6 According
to Romeo et al.,25 surgical excision is the only
treat-mentfor thislesion,asconstantrelapses inextravasation mucocele are observed when this procedure is not per-formed. In the present study, excisional biopsy was the mostwidelyusedformoftreatmentforextravasation muco-cele,whichisconsistentwiththerecommendationsinthe literature.1,2,4---8,10,13,20Astrategytopreventrecurrencesis
theexcision of smalllesionsdowntothe muscularplane, togetherwithamarginof salivaryglandtissue.In caseof largelesions,marsupializationhelppreventdamagetovital structures,suchasthelabialbranchofthementalnerve.17
Micro-marsupializationcanbeconsideredasanalternative surgicalmethodincaseofpediatricpatients,asitisa sim-pletechnique,lesstraumatic,relativelypainless,andhasa lowlikelihoodofrecurrence.6,17
Anothersurgicalmethodoforalmucocelemanagement is ablation with CO2 laser, which decreases the chances ofrecurrenceandcomplicationandallowsfastandsimple lesionablation.Thisprocedureisalsosuitableforpatients whocannottoleratelongprocedures.17 Thistechniquehas
thedisadvantageofnotallowinghistologicalexaminationof thelesion.
Conclusions
Oral mucocele is a fairly common lesion that primar-ily affects young patients and preferentially affects the
lower lip. Extravasation mucocele is the most common subtype, affecting patients. Conservative surgery is the most widely used treatment, but alternative forms have been reportedinthe literature,such asmarsupialization, dissection, cryosurgery, carbon dioxide laser, electrocau-terization,intralesionalinjectionofsclerosingagents,and steroidinjections.
Thisstudyhaslimitations,asdoallretrospectivestudies. Itwasnotpossibletodeterminesomeclinicaldatadueto lack ofcorrect completionof biopsyrecords.The correct handlingofthisdocumentisanimportantlearningtoolfor students,asanepidemiological researchtoolaswellasa toolforpatientmonitoring.Weemphasizetheimportanceof healthprofessionalsandstudentsbeingstricternotonlywith thepatient’smedicalhistory,butalsoinbettercompletion ofclinicalrecords.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.ChoiHJ,KimSG,KimJD,KimJH,KimJH,KimSM.Acaseof bilat-eralsubmandibularglandmucocelesina16-month-oldchild. KoreanJPediatr.2012;55:215---8.
2.Ata-Ali J, Carrilo C, Bonet C, Balaguer J, Pe˜narrocha M, Pe˜narrochaM.Oralmucocele:reviewoftheliterature.JClin ExpDent.2010;2:E18---21.
3.Yamasoba T, Tayama N, Syoji M,Fukuta M. Clinicostatistical studyoflowerlipmucoceles.HeadNeck.1990;12:316---20.
4.Hze-Khoong EP, Xu L, Shen S, Yin S, Wang L, Zhang C. Submandibular glandmucocele associatedwithamixed ran-ula. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;55: 215---8.
5.ReCecconiD,AchilliA,TarozziM,LodiG,DemarosiF,Sardella A, et al. Mucoceles of the oral cavity: a large case series (1994---2008)and aliteraturereview.MedOralPatolOralCir Bucal.2010;15:551---6.
6.Bhargava N, Agarwal P, Sharma N, Agrawal M, Sidiq M, NarainP.Anunusualpresentationoforalmucoceleininfant and its review. Case Rep Dent. 2014, http://dx.doi.org/ 10.1155/2014/723130.
7.BaurmashHD.Mucocelesandranulas.JOralMaxillofacSurg. 2003;61:369---78.
8.More CB, Bhavsar K, Varma S, Tailor M. Oral mucocele: a clinicalandhistopathologicalstudy.JOralMaxillofacPathol. 2014;18:S72---7.
9.Luiz AC, Hiraki KR, Lemos CA Jr, Hirota SK, Migliari DA. Treatmentofpainfulandrecurrentoralmucoceleswitha high-potencytopicalcorticosteroid:acasereport.JOralMaxillofac Surg.2008;66:1737---9.
10.RashidAK,AnwarN,AzizahAM,NarayanKA.Casesof muco-celetreatedintheDentalDepartmentofPenangHospital.Arch OrofacSci.2008;31:7---10.
11.NicoMM,ParkJH,Lourenc¸oSV.Mucoceleinpediatricpatients: analysisof36children.PediatrDermatol.2008;25:308---11.
12.ChenJY,WangWC,ChenYK,LinLM.Aretrospectivestudyof trauma-associatedoralandmaxillofaciallesionsinapopulation fromsouthernTaiwan.JApplOralSci.2010;18:5---9.
14.MohanH,TahlanA,MundiI,PuniaRP,DassA.Non-neoplastic salivaryglandlesions:a15-yearstudy.EurArch Otorhinolaryn-gol.2011;268:187---90.
15.AndiranN,SarikayalarF,UnalOF,BaydarDE,OzaydinE. Muco-celeoftheanteriorlingualsalivaryglands:fromextravasation toanalarmingmasswithabenigncourse.IntJPediatr Otorhi-nolaryngol.2001;61:143---7.
16.Conceic¸ão JG, Gurgel CA, Ramos EA, de Aquino Xavier FC, Schlaepfer-SalesCB,CangussuMC,etal.Oralmucoceles:a clin-ical, histopathologicaland immunohistochemical study.Acta Histochem.2014;116:40---7.
17.Yagüe-GarcíaJ,Espa˜na-TostAJ,Berini-AytésL,Gay-EscodaC. Treatmentoforalmucocele---scalpelversusCO2laser.MedOral
PatolOralCirBucal.2009;14:469---74.
18.KhannaS,SinghNN,SreedharG,PurwarA,GuptaS.Oralmucous extravasation cyst:case serieswith comprehensive and sys-tematicreviewondifferentialdiagnosis.IntJDentCaseRep. 2013;3:17---27.
19.ChiAC,LambertPR3rd,RichardsonMS,NevilleBW.Oral muco-celes: a clinocopathologic review of 1,824 cases, including unusualvariants.JOralMaxillofacSurg.2011;69:086---93.
20.HayashidaAM,ZerbinattiDC,BaiducciI,CabralLA,AlmeidaJD. Mucusextravasationandretentionphenomena:a24-yearstudy. BMCOralHealth.2010;7:10---5.
21.JaniDR,ChawdaJ, SundaragiriSK, ParmarG. Mucocele--- a studyof36cases.IndianJDentRes.2010;21:337---40.
22.BermejoA,AguirreJM,LópezP,SaezMR.Superficialmucocele: reportof4cases.OralSurgOralMedOralPatholOralRadiol Endod.1999;88:469---72.
23.García-F-Villalta MJ, Pascual-López M, Elices M, Daudén E, García-Diez A, Fraga J. Superficial mucoceles and lichenoid graft versus hostdisease: reportof three cases.Acta Derm Venereol.2002;82:453---5.
24.BagánSebastiánJV,SilvestreDonatFJ,Pe˜narrochaDiagoM, Mil-iánMasanetMA.Clinico-pathologicalstudyoforalmucoceles. AvOdontoestomatol.1990;6:389---91.