www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Effectiveness
of
sound
therapy
in
patients
with
tinnitus
resistant
to
previous
treatments:
importance
of
adjustments
夽
Flavia
Alencar
de
Barros
Suzuki
a,∗,
Fabio
Akira
Suzuki
b,
Fernando
Kaoru
Yonamine
b,
Ektor
Tsuneo
Onishi
a,
Norma
Oliveira
Penido
aaHealthSciences,DepartmentofOtolaryngologyandHeadandNeckSurgery,EscolaPaulistadeMedicina,
UniversidadeFederaldeSãoPaulo(EPM-UNIFESP),SãoPaulo,SP,Brazil
bHealthSciences,EscolaPaulistadeMedicina,UniversidadeFederaldeSãoPaulo(EPM-UNIFESP),SãoPaulo,SP,Brazil
Received13March2015;accepted12May2015 Availableonline16October2015
KEYWORDS
Tinnitus; Soundtherapy; Treatment; THI
Abstract
Introduction:Thedifficultyinchoosingtheappropriatetherapyforchronictinnitusrelatesto
thevariableimpactonthequalityoflifeofaffectedpatientsand,thus,requires
individualiza-tionoftreatment.
Objective: Toevaluatetheeffectivenessofusingsoundgeneratorswithindividualadjustments
torelievetinnitusinpatientsunresponsivetoprevioustreatments.
Methods:A prospectivestudyof10patientswithchronictinnituswhowereunresponsiveto
previousdrugtreatments,fivemalesandfivefemales,withagesrangingfrom41to78years.
Bilateralsoundgenerators(Reach62orMind9models)wereuseddailyforatleast6hduring18
months.Thepatientswereevaluatedatthebeginning,after1monthandateach3monthsuntil
18monthsthroughacuphenometry,minimummaskinglevel,theTinnitusHandicapInventory,
visualanalogscale,andtheHospitalAnxietyandDepressionScale.Thesoundgeneratorswere
adjustedateachvisit.
Results:TherewasareductionofTinnitusHandicapInventoryinninepatientsusingaprotocol
with acustomizedapproach, independentofpsychoacousticcharacteristicsoftinnitus.The
bestresponsetotreatmentoccurredinthosewithwhistle-typetinnitus.Acorrelationamong
theadjustmentsandtinnitusloudnessandminimummaskinglevelwasfound.Onlyonepatient,
whohadindicationofdepressionbyHospitalAnxietyandDepressionScale,didnotrespondto
soundtherapy.
夽 Pleasecitethisarticleas:SuzukiFAB,SuzukiFA,YonamineFK,OnishiET,PenidoNO.Effectivenessofsoundtherapyinpatientswith
tinnitusresistanttoprevioustreatments:importanceofadjustments.BrazJOtorhinolaryngol.2016;82:297---303.
∗Correspondingauthor.
E-mail:[email protected](F.A.BarrosSuzuki). http://dx.doi.org/10.1016/j.bjorl.2015.05.009
Conclusion:Therewasimprovementinqualityoflife(TinnitusHandicapInventory),withgood
responsetosoundtherapyusingcustomizedsettingsinpatientswhodidnotrespondtoprevious
treatmentsfortinnitus.
© 2015Associac¸˜ao Brasileira de Otorrinolaringologiae CirurgiaC´ervico-Facial. Publishedby
ElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Zumbido; Terapiasonora; Tratamento; THI
Eficáciadaterapiasonoraempacientescomzumbidoresistenteatratamentos anteriores:importânciadosajustes
Resumo
Introduc¸ão:Adificuldadeemescolheraterapiaapropriadaparazumbidocrônicoencontra-se
nassuasdiversasformasdeimpactosobreaqualidadedevidadospacienteserequerasua
individualizac¸ão.
Objetivo:Avaliaraeficáciadousodogeradordesomcomajustesindividuaispara aliviaro
zumbidoempacientessemrespostaaostratamentosanteriores.
Método: Umestudoprospectivoem10pacientes,5homense5mulheres,nafaixaetáriade41
a78 anoscomzumbidocrônicoeresistenteatratamentosmedicamentosos.Foramutilizados
geradoresdesombilaterais nosmodelosReach 62ouMind 9pornomínimo6 horasdiárias
durante18 meses.Ospacientesforamavaliadosnoinício,depoisde1mêseacada3 meses
até18 mesesatravés daacufenometria,MinimumMasking Level (MML), Tinnitus Handicap
Inventory (THI),EscalaVisualAnalógica(EVA)eHospitalAnxietyandDepressionScale(HADS).
Osgeradoresdesomforamajustadosemcadavisita.
Resultado:Houveumareduc¸ãodoTHIem9pacientesusando-seumprotocolocomuma
abor-dagempersonalizada,independentedascaracterísticaspsicoacústicasdozumbido.Amelhor
respostaaotratamentoocorreunaquelespacientescomzumbidodotipoapito.Encontramos
umacorrelac¸ãoentreosajusteseaintensidadedozumbidoeoMML.Apenasumpacientecom
indicac¸ãodedepressãoHADSnãorespondeuàterapiasonora.
Conclusão:Houveumamelhoranaqualidadedevida(THI)comboarespostaaterapiasonora
comajustespersonalizadosempacientesresistentesatratamentosanterioresparaozumbido.
©2015Associac¸˜aoBrasileira deOtorrinolaringologiaeCirurgiaC´ervico-Facial.Publicadopor
ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Subjectivetinnituscanbedefinedasanauditoryperception intheabsenceofanexternalsoundstimulus,1describedas asoundlikeawhistleorahiss.Itisestimatedthatover30 millionAmericanshavetinnitus;2inBrazil,itisbelievedthat thisnumberisabout28million.3Thus,itisapublichealth problem.
Itisacommon-senseconclusionamongresearchersthat symptomseveritycanleadtolossesinqualityoflife.The lackofcontroloftinnitusanditsconstantpresenceproduces ahighdegreeofstress;indeed,theemotionaleffectis vari-ableandmayrangefroma mildirritation associatedwith tinnitus,tostatesofanxiety,depression,andinsomnia,even leadingtosuicide.4
Inpatientswithtinnitus,itisdifficulttomakeobjective measurementsofemotional disorderssuch asanxietyand depression. However, several subjective assessment tools areavailable inPortuguese, andthe Hospital Anxietyand DepressionScale (HADS)5,6 isone ofthemost used instru-ments,duetoitseaseofapplication.
Since tinnitus is a subjective symptom, it is difficult toanalyze, measure,and treat. Thus evaluationssuch as
acuphenometry,the useofvisual analog scales(VAS),and questionnairesto determine the impactonquality of life such as the Tinnitus Handicap Inventory (THI)7,8 are very important strategies, as are individual approaches in the treatmentofthesepatients,.
Among the therapeutic possibilities for sensorineural tinnitus, drug therapy, acupuncture,9,10 transcranial mag-netic stimulation,11 cognitive-behavioral therapy (CBT),12 andsoundtherapy(maskingtherapy13andhabituation ther-apy) can be cited.4 Some patients try several resources attemptingtofindatreatmentthatbringssignificantrelief fortheirtinnitus.
generator that produces fractal sounds (music); in this manner,themelodyismaintainedbutdoesnotrepeatitself. Toobservetheeffectivenessofsoundenrichmentin tinn-itussensation, minimummasking levels(MML)areusedin ordertoevaluate theeffectofmasking theperceptionof tinnitusthroughtheuseofabroadbandnoise.15
Currently, several protocols have been used for sound therapy;however,reportsonthesettingsusedinsound gen-erators of hearing aids were not found in the literature. Theaimofthisstudywastodemonstratetheeffectiveness ofsoundtherapy withdifferenttypesofsoundgenerators throughpatients’ follow-up,therelationshipofsequential evaluationsthroughpreviouslyestablishedparameters(THI, VAS,MML),andtheneedforindividualinterventionsthrough detailing the customized settings of these generators in patientsunresponsivetoprevioustreatmentsfortinnitus.
Methods
ThisstudywasapprovedbytheEthicsCommitteeunderCEP protocol No. 1090/11. Patients were instructed about all proceduresofthestudyandsignedaninformedconsent.
A prospective study of 10 selected patients from the TinnitusOutpatient Clinicwasconductedbythe otolaryn-gologistsresponsibleforthisdepartment.Fortheresearch, 20retroauricularbehindtheear(BTE)hearingaidswithan openfittingweredonatedtobeusedbypatientsbilaterally. Ofthese 10patients, fiveusedtheMind 9440 modelwith fractalsounds(WidexTM)andfiveusedtheReach62Model (BeltoneTM)withwhitenoise.
Patientswererecruitedsequentiallyfromthebeginning ofthestudy,alternatingtheindicationofMind9andReach 62generators,accordingtoinclusionandexclusioncriteria. Inclusioncriteria:continuouschronictinnituscomplaints foroverayearwithoutimprovementwithdrugtherapiesand withnospecifictreatmentfortinnitusforatleast3months. Hearingloss,whenpresent,wasnotthemaincomplaintof thepatient.
Exclusioncriteria:conductivehearinglossorchangesin theexternaland/ormiddleear.
Duringtheuseofsoundgenerators,thesepatientswere evaluatedat thebeginning of therapy, and at 1, 3, 6, 9, 12,15,and18months,whenthegeneratorswereswitched off. Inall thevisits, adjustments forthe generators were performedwhenneeded,andallofthefollowingevaluations werecarriedout:
Otolaryngologyevaluation
Puretoneaudiometryandvocalaudiometry Immitanciometrywithstapedialreflexsurvey HADS
VAS THI
Acuphenometry(loudnessandpitchmatching) MML
The HADS questionnaire wasused because it is a sim-ple,rapidassessmenttoolthatprovidesdataandidentifies symptomsofanxietyanddepressioninindividualsunderno psychiatrictreatment.
Tobetter understandtheeffectof tinnitusinpatients, thetypeoftinnituspresentedwasconsideredand character-izedbyacuphenometry:agroupwithwhistle-typetinnitus equivalenttopuretone,agroupwithhissing-typetinnitus equivalenttowhitenoise(WN)ornarrowband(NB),anda groupwithbothtypesoftinnitus.Inallgroups,evaluations andadjustmentsmetthesamecriteria.
ThroughMML,theauthorssought toascertain the min-imum intensity of tinnitus masking in ascending form by usingbilateralnoise: inthefirstinstance, WN;inthe sec-ond instance, NB at tinnitus frequency, and then NB at 500Hz.
ReductioninTHIscore≥20pointsandreducedVASwere
consideredasimprovedparametersoftherapy.
Thefivepatientswhousedsoundgeneratorswithmusic could choose between five types of fractal sounds, ran-dom and harmonic, known as Zen. Where necessary, the adjustmentschangedtherhythm(betweenslowandfast), frequency(betweenlow andhigh), thevolumeinarange from0to15,and,insomecases,thetypeofZensound.
Theotherfivepatientsusingsoundgeneratorswithwhite noisecouldadjusttheinitialvolumebysoundpressurelevel (SPL),from0to100dBSPL;uselowsoundcutsbetween500 and2000Hzandhighsoundcutsbetween2000and6000Hz; insertslight,moderate,or strongmodulation; andchange betweenslow,medium,andfastspeed.
Patientswithassociatedhearinglossweregivenamonth ofinitialmonitoringtoadaptandadjustthesound amplifi-cationbeforebeingconnectedtothesoundgenerator.
TheequipmentusedincludedanAC40audiometer (Inter-acoustics)andanAZ7immitanciometer(Interacoustics).
Hearing aids with sound generator were obtained by donation from Centros Auditivos Widex and Audibel do Brasil.
Results
Ofthetotalof10patients,fivewerefemaleandfivemale, aged41---78years.Sixpatientspresentedwithbilateral tinn-itusshowingmoreintensityontheleftside;in three,the problemwasunilateralontheleftside;andonepatienthad unilateraltinnitusontherightside.
Intheanalysisoftonalaudiometry,itwasfoundthattwo subjectshadnohearinglossandeighthadmild-to-moderate sensorineuralhearinglossathighfrequencies.Ofthese,only foursubjectshadassociatedhearing complaints,withthe necessity for placement of amplification in their hearing aidsto improve speechunderstanding and avoid auditory deprivation.
All patients usedthe sound generators for at least 6h dailythroughout the treatment, regardlessof the typeof generator.
In acuphenometry, throughout therapy, 10 patients exhibitedtinnitusbetween3000and8000Hz;twopatients startedsoundtherapywithwhistle-typetinnitus,fourwith hissing-typetinnitus,andfourwithwhistle-andhissing-type tinnitus(Table1).
Table1 Visualanalogscale(VAS)scoresaccordingtotypeoftinnitusinthebeginningandattheendofsoundtherapy.
Patient BaselineVASfortinnitus VASfortinnitusafter18months
Right Left Right Left
1 Absent Hissing7 Absent Hissing5
2 Whistle8
Hissing8
Whistle10
Hissing10
Whistle0
Hissing3
Whistle0
Hissing6
3 Absent Hissing8 Absent Hissing2
4 Whistle5 Whistle9 Whistle3 Whistle5
5 Whistle9 Absent Whistle1 Absent
6 Hissing2 Hissing5 Hissing2 Hissing4
7 Absent Hissing6 Hissing2 Hissing4
8 Whistle7
Hissing7
Whistle10
Hissing9
Whistle5
Hissing7
Whistle6
Hissing9
9 Whistle5
Hissing3
Whistle8
Hissing7
Whistle0
Hissing0
Whistle0
Hissing3
10 Whistle0
Hissing4
Whistle8
Hissing4
Whistle0
Hissing3
Whistle3
Hissing3
Ofthe10 patientsmonitored,in nineadecreaseof20 pointsinTHI score (with respecttobasal levels,Table2) andreduction in VAS (Table 1) were observed at the end ofthesound therapy.Twopatients,whohad been consis-tentlyshowingagoodresponsetotreatment,demonstrated aworse scoreat 15 months (patient7)and at 18months (patient2).
Inacuphenometry,theintensityoftinnituswasreduced orremainedatthesamelevelinallpatients,when compar-ingthebeginningandtheendofsoundtherapy.Regarding MMLwithWN, volume reductionor stabilization occurred ineightpatients.Comparedtobaseline,therewasaneed toincrease thevolumeof soundgenerators inallpatients (Table3).
ThevolumeofMMLNBattinnitusfrequencywasreduced orremainedatthesamelevelinninepatientsandincreased only in the patient who reported no improvement with therapy. However, when MML volume with NB at 500Hz was evaluated, this occurred in only six patients. These responseswereimportant insetting thecharacteristics of thesoundgenerators(Table4).
Thestabilizationofvolumeandgeneratorcharacteristics required3---12monthsofsoundtherapy.
Of the six patients who used only the generator, two (patients1and5)returnedthedevices;onecontinuedwith thetherapy(patient2),andthreekeptthegeneratorsfor sporadic use (patients8, 9,and 10).Of the foursubjects presenting hearingloss,threeremainedonlywith amplifi-cation(patients4,6,and7)andonewithamplificationand agenerator(patient3).
Discussion
Numerous proposals to determine the origin of tinnitus exist,4,16,17butnotwithstandingthecause,themost impor-tant aspect is when this information is interpreted as something unpleasant by the limbic system. This emo-tionalreactioncanbeintensifiedandworsened,resultingin increasingstressandexacerbationofthetinnitussensation, withanimportantimpactonqualityoflife.
Veryanxiousindividualsprocessemotionalstimulimore rapidlythannon-anxiouspeople,18andevenconsideringthat anxietyhasnotbeenestablishedasacausalfactorintinnitus worsening,HADSshowedthatthisconditionwaspresentin threepatients(2,3and9)whowerealreadyusingcontrolled
Table2 TinnitusHandicapInventory(THI)scoresduringsoundtherapy.
Patient THI
Baseline 1month 3months 6months 9months 12months 15months 18months
1 74 58 58 44 50 38 40 24
2 72 56 40 26 22 22 22 54
3 72 38 22 20 20 24 12 16
4 38 14 24 34 20 26 24 18
5 44 46 0 0 0 0 0 0
6 38 34 26 22 30 22 14 16
7 40 12 20 14 22 10 38 40
8 58 56 62 60 66 66 58 68
9 64 44 44 44 38 38 36 12
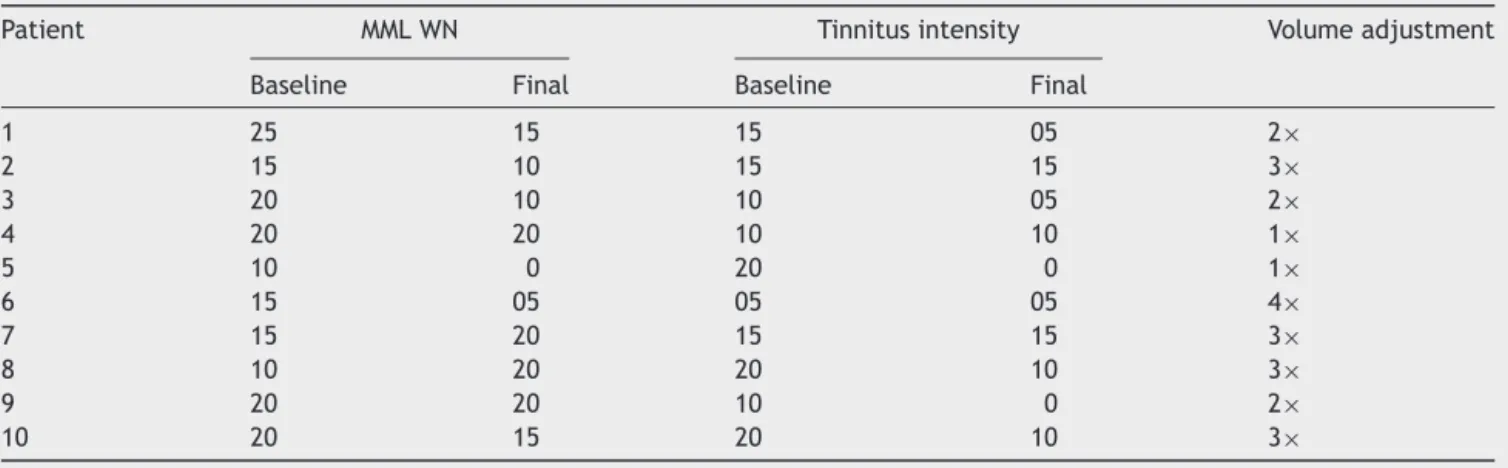
Table3 Baselineandfinalintensity(dB)oftinnitusandvolume(dB)ofminimummaskinglevels(MML)withwhitenoise(WN)
insensationlevel,andthenumberoftimesthegeneratorvolumewasadjusted.
Patient MMLWN Tinnitusintensity Volumeadjustment
Baseline Final Baseline Final
1 25 15 15 05 2×
2 15 10 15 15 3×
3 20 10 10 05 2×
4 20 20 10 10 1×
5 10 0 20 0 1×
6 15 05 05 05 4×
7 15 20 15 15 3×
8 10 20 20 10 3×
9 20 20 10 0 2×
10 20 15 20 10 3×
medicationsfor their treatment. The correlation of HADS withtinnitus showed that, despite the non-occurrenceof change in anxiety characteristics throughout therapy, this factdidnothindergoodresponsestosoundtherapy.
Inpatient8,characteristicsofanxietyanddepressionin HADS were found fromthe beginning of therapy,but the patientreportedthatshewasnotinanyspecifictreatment, becauseshehadnotthoughtthatprevioussuggestionswere beneficial. She wasthe only patient whodid notachieve improvement of the impactof tinnituson qualityof life, whichleadstotheconclusionthatdepression,asreported byotherauthors,19preventedtheadaptationtotinnitus.
Several authors20---23 have demonstrated theefficacy of THIinmonitoringtinnitustreatments,andwe,usedthistool asanimportantmeasuretoevaluatetheimpactoftinnitus onquality of life.Therefore, when considering that tinn-itus is dynamic and influenced by emotional and physical changes,itwasimportanttoassessTHIthroughouttherapy, aswell as tomake adjustments in the intervention when necessary.
Theauthorsobservedimprovementof≥20pointsinTHI
scoresduringtherapyinninepatients,whichisinlinewith thefindingsofotherauthors(Table2).20,24Inthosesubjects
that worsened (patient 2 at 18 months and patient 7 at 15 months), the emotional, functional, and catastrophic aspects of tinnitus in THI were analyzed. Worsening was found in all three aspects with respect to the previous evaluationofpatient2,whohadworsened emotional sta-tus due to personal factors, with no change in auditory thresholds.However,patient7hadbothworsenedtinnitus andhearingthresholdsafteradiagnosisofcancerandthe startofchemotherapy/radiotherapy.Inthissubject,theTHI scorefor functional aspect wasthe most affected. These responseswereofinterestwhenrelatingthecauseof wors-ening(emotionalorfunctional)withthequalitativeaspects oftinnitus.
There are several possibilitiesto treat the etiology or the effect of tinnitus. Treating the cause is more diffi-cult,giventhedifficultytodeterminetheoriginoftinnitus andalso because, in most cases, there is no relationship betweenacureforthediseaseandtheeliminationor reduc-tion of tinnitus. When the neurophysiological process of habituationtakes placeduring soundtherapy, thecentral nervoussystemceasestoperceivetinnitusasanunpleasant sensationandmayreduce itsperceptionor evensuppress it.4,14
Table4 Baselineandfinalvolume(dB)ofminimummaskinglevels(MML)withnarrowband(NB)attinnitusfrequencyandat
500Hzinsensationlevel,andthenumberoftimesthatchangesweremadetogeneratorcharacteristics.
Patient MMLNBTF MMLNB500Hz Adjustmentofcharacteristics
Baseline Final Baseline Final
1 45 25 70 50 3×
2 20 10 25 30 3×
3 20 10 30 35 2×
4 05 05 55 50 4×
5 20 0 25 0 1×
6 15 05 25 20 4×
7 20 15 20 20 1×
8 15 20 20 30 4×
9 20 15 30 35 1×
10 20 10 40 20 2×
WhenmeasuringtinnituswiththeuseofVAS,weobserved adifferenceinhissing-andwhistle-typetinnitusreduction atthebeginningandattheendoftherapy(Table1), with-outanychangeinpitchduringthetreatment.Asignificant reductionofwhistle-typetinnitusoccurredinsixpatients, withsuppressionoftinnitus intwopatients at theend of treatment.However,inthosewithhissing-typetinnitus,the reduction was less noticeable, or the intensity remained the same, and in patient 7, who underwent chemother-apy,theauthorsevennotedtheonsetofhissingintheside previously without tinnitus. The decrease of whistle-type tinnitusoccurred evenin patient8, whodid not achieve agoodresponsetosoundtherapy,andwhoseHADS scores suggestedanxietyanddepression;thispatientalsonotedno improvementonhisTHI,andanunalteredVASforhissing. These findings suggest that the corticalrepresentation of whistle-typetinnitus,expressedinacuphenometrybypure tone,canbemorepronetomodulationinthecentral ner-voussystem.Nonetheless,consideringthesmallnumberof subjectsin thisseries, theauthors cannotclaim thisasa hypothesis.
According toFigueiredo et al.,25 thereis a correlation betweenTHIandVASscores,whichagreeswiththisstudy.
Throughouttherapy,onetofouradjustmentsofthe vol-ume and characteristics of the sound of generators were carriedoutuntilstabilization(Tables3and4).Newchanges occurredat15and18monthsinbothpatientswhoworsened (patients2and7).
Inisolation,theintensityoftinnitusevaluatedin acuphe-nometry did not indicate the success of the therapy. In allsubjects,thebaselineintensitydecreasedorwas main-tained at the same level, including in patient 8, who reported no significant improvement and did not show improvementinTHI(Table3).
Despitethereductionormaintenanceoftinnitus inten-sity after treatment of these patients, there was a need toincreasethevolumeofthesoundgeneratorsduringthe therapyforallsubjects(Table3).Conversely,areductionin MMLwithWNin eightpatients occurred,withan increase attheendinthepatientwithworseningofhearing thresh-olds(patient7)andalsointhatpatientwhodidnotimprove (patient8).
Thus, there was a correlation between intensity of tinnitus and MML WN intensity from the generator. With habituation, the tinnitus and the level of sound required tomask it quickly, asin MML WN, tended todiminish or stabilize,and the central nervoussystem tended to con-formtothesoundofgenerators,thusitbecamenecessary toincreasetheirvolume(Table3).Interventionsthroughout therapywererequiredtomaintaintheresponse.
Theliteratureshowsthatthebestoptionforhabituation isbroadbandWN,becauseitislessbothersomeandcovers morefrequencies;23 however,the algorithms of the hear-ingaidsenabledchangesintheircharacteristics.Thus,this studyusedothersupportmeasurestoevaluateandchange thecharacteristicsofsoundgenerators:MMLNBatthe tinn-itusfrequency,andMMLNBat500Hz.
ThefirsthadaresponsesimilartothatofMMLWN,i.e., volume reduction or maintenance in nine patients. How-ever,thisrelationshipwasnotobservedwithMMLNB500Hz, (Table4).Despitethefactthatlowfrequenciesare consid-ered more relaxing comparedto high frequencies, better
acceptance of changes tohigher pitchwas observed, but the acceptance was not goodfor modulation and rhythm changes.
ThisstudyalsoobservedarelationshipbetweenTHIand MMLWN,whichwasreducedinpatientswithgoodresponses totreatmentandwithoutmajorcomplicationsduring ther-apy.AlthoughFigueiredoetal.26didnotobservethiseffect intheirstudy,theseauthorsdidnotcompareTHIandMML WN throughout the treatment, but only at their initial assessment.
Althoughseveralstudieshavedemonstratedthe impor-tance of determining the mixing point for habituation of tinnitus,inthepresentstudywedidnotconsistentlyobserve this,and noteditonly intwopatients (9and10) with12 and15monthsofuseofthesoundgenerator,respectively. The findings of Tyler etal.27 also showedthat therewas noneed todetermine the mixingpoint for habituationto occur.
Conclusion
Itispossiblethatpatientswithwhistle-typetinnitushavea betterresponsetosoundtherapy.
Acorrelation of MML WN with THI during therapy was observed.
Apparently,thereisacorrelationofadjustmentstosound generatorswithhabituationoftinnitus,anaspectobserved intheseevaluations;thisrequiresthecustomizationofthese settings, according to the patient’s symptoms and their answers in matching pitch, loudness,and MML,which we performedoneverypatient’sreturn.
ThepatientwithresponsetoHADSfordepressiondidnot respondwelltotreatment.
Norelationshipwasfoundbetweenthefindingsregarding locationof tinnitus,presenceof hearingloss,and typeof sound generator with the other criteria evaluated in this study.
Conflict
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
The authors would like to thank Centros Auditivos Widex and Audibeldo Brasilfor the donationof hearingaidsfor thisresearch.
References
1.TylerRS,CoelhoC,NobleW.Tinnitus:standardofcare, person-alitydifferences,geneticfactors.ORLJOtorhinolaryngolRelat Spec.2006;68:14---9.
2.KochkinS,TylerR, BornJ.MarkeTrakVIII:theprevalenceof tinnitusintheUnitedStatesandtheself-reportedefficacyof varioustreatments.HearRev.2011;18:10---26.
4.Jastrebroff PJ. Phantom auditory perception (tinnitus): mechanisms of generation and perception. Neurosci Res. 1990;8:221---54.
5.ZigmondAS, Snaith RP. The hospital anxiety and depression scale.ActaPsychiatrScand.1983;67:361---70.
6.BotegaNJ,BioMR,ZomignaniMA,GarciaCJr,PereiraWAB. Transtornos de humor em enfermarias de clínica médica e validac¸ãodeescalademedida(HAD)deansiedadeedepressão. RevSaudePublica.1995;29:355---63.
7.NewmanC,JacobsonGP,SpitzerJB.Developmentofthe tinn-itus handicap inventory. Arch Otolaryngol Head Neck Surg. 1996;122:143---8.
8.FerreiraPEA,CunhaF,OnishiET,Branco-BarreiroFCA,Gananc¸a FF.Tinnitushandicapinventory:adaptac¸ãoculturalparao Por-tuguêsbrasileiro.ProFonoRevAtualCient.2005;17:303---10. 9.OnishiE,Kasse CA,Rodrigues C,OliveiraMHP,Bataglia PUR,
AprileMR,etal.Comodiagnosticaretratar:zumbido.RevBras Med.2008;65:32---7.
10.OkadaDM,OnishiET,ChamiFI,BorinA,CassolaN,Guerreiro VM.Ousodaacupunturaparaalívioimediatodozumbido.Rev BrasOtorrinolaringol.2006;72:182---6.
11.KleinjungT,LangguthB.Strategiesforenhancementof trans-cranialmagnetic stimulation effects in tinnituspatients. Int TinnitusJ.2009;15:154---60.
12.RobinsonSK,ViirreES,BaileyKA,KindermannS,MinassianAL, GoldinPR, etal. Arandomizedcontrolledtrialof cognitive-behaviortherapyfortinnitus.IntTinnitusJ.2008;14:119---26. 13.VernonJA,Meikle MB.Tinnitus masking.In: TylerRS,editor.
Tinnitushandbook.CengageLearning;2000.p.313---56. 14.Sweetow RW, Sabes JH. Effects of acoustical stimuli
deliv-ered through hearing aids on tinnitus. J Am Acad Audiol. 2010;21:461---73.
15.JastreboffPJ,JastreboffMM.Tinnitusretrainingtherapy(TRT) asamethodfortreatmentoftinnitusandhyperacusispatients. JAmAcadAudiol.2000;11:162---77.
16.HellerMF,BergmanM.Tinnitusinnormallyhearingpersons.Ann OtolRhinolLaryngol.1953;62:73---83.
17.KaltenbachJA,ZhangJ,FinlaysonP.Tinnitusasaplastic phe-nomenonand its possibleneural underpinningsinthe dorsal cochlearnucleus.HearRes.2005;206:200-26[Review]. 18.OomsE,VanheuleS,MeganckR,VinckB,WateletJB,Dhooge
I. Tinnitus, anxiety and automatic processing of affective information:anexplorativestudy.EurArchOtorhinolaryngol. 2013;270:823---30.
19.GeoczeL,MucciS,AbranchesDC,MarcoMA,PenidoNO.Revisão sistemáticasobreasevidênciasdeassociac¸ãoentrezumbidoe depressão.BrazJOtorhinolaryngol.2013;79:106---11.
20.Stouffer JL,TylerRS.Characterizationoftinnitusbytinnitus patients.JSpeechHearDisord.1990;55:439---53.
21.BaguleyDM,HumphrissRL,HodgsonCA.Convergentvalidityof thetinnitushandicapinventoryandthetinnitusquestionnaire. JLaryngolOtol.2000;114:840---3.
22.BerryJA,GoldSL,FrederickEA,GrayWC,StaeckerH. Patient-basedoutcomes inpatientswithprimary tinnitusundergoing tinnitusretrainingtherapy.ArchOtolaryngolHeadNeckSurg. 2002;128:1153---7.
23.KinBJ,ChungSW,JungJY,SuhMW.Effectofdifferentsounds onthetreatmentoutcomeoftinnitusretrainingtherapy.Clin ExpOtorhinolaryngol.2014;7:87---93.
24.Newman CW,Sandridge SA, Jacobson GP.Psychometric ade-quacyoftheTinnitusHandicapInventory(THI)forevaluating treatmentoutcome.JAmAcadAudiol.1998;9:153---60. 25.FigueiredoRR,AzevedoAA,OliveiraPM.Análisedacorrelac¸ão
entreaescalavisual-análogaeoTinnitus HandicapInventory naavaliac¸ãodepacientescomzumbido[Correlationanalysisof thevisual-analoguescaleandtheTinnitusHandicapInventory intinnituspatients].BrazJOtorhinolaryngol.2009;75:76---9. 26.FigueiredoRR,RatesMA,AzevedoAA,OliveiraPM,NavarroPB.
Análise da correlac¸ão entrelimiares auditivos,questionários validadosemedidaspsicoacústicasempacientescomzumbido. BrazJOtorhinolaryngol.2010;76:522---6.