w w w . r b o . o r g . b r
Original
Article
Reconstruction
of
the
anterior
cruciate
ligament
by
means
of
an
anteromedial
portal
and
femoral
fixation
using
Rigidfix
夽
,
夽夽
André
Manoel
Inácio
a,∗,
Osmar
Valadão
Lopes
Júnior
a,b,
André
Kuhn
b,
José
Idílio
Saggin
b,
Paulo
Renato
Fernandes
Saggin
b,
Leandro
de
Freitas
Spinelli
a,c,
Daniela
Medeiros
de
Castro
daInstituteofOrthopedicsandTraumatologyofPassoFundo,PassoFundo,RS,Brazil
bHospitalSãoVicentedePaulo,PassoFundo,RS,Brazil
cOrthopedicsandTraumatologyServiceoftheHospitalComplex,SantaCasadePortoAlegre,PortoAlegre,RS,Brazil
dRadiologyandImagingDiagnosticsService,KozmaClinicofPassoFundo,PassoFundo,RS,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received25June2013 Accepted15October2013 Availableonline22October2014
Keywords:
Knee/surgery
Anteriorcruciateligament Reconstruction
a
b
s
t
r
a
c
t
Objective:Toevaluateaseriesofpatientswhounderwentsurgeryforreconstructionofthe anteriorcruciateligamentwithflexortendons,bymeansoftheanteromedialtransportal techniqueusingRigidfixforfemoralfixation,andtoanalyzethepositioningofthepinsby meansoftomography.
Methods:Thirty-twopatientswereincludedinthestudy.Theclinicalevaluationwasdone usingtheLysholm,subjectiveIKDCandRolimeter.Allofthemunderwentcomputed tomo-graphywith3Dreconstructioninordertoevaluatetheentrypointandpositioningofthe Rigidfixpinsinrelationtothejointcartilageofthelateralcondyleofthefemur.
Results:ThemeanLysholmscoreobtainedwas87.81andthesubjectiveIKDCwas83.72. Amongthe32patientsevaluated,43%returnedtoactivitiesthatwereconsideredtobe veryvigorous,9%vigorous,37.5%moderateand12.5%light.In16patients(50%),thedistal entrypointoftheRigidfixpinwaslocatedoutsideofthecartilage(extracartilage);inseven (21.87%),thedistalpininjuredthejointcartilage(intracartilage);andinnine(28.12%),itwas attheborderofthelateralcondyleofthefemur.
Conclusion: ThepatientswhounderwentACLreconstructionbymeansoftheanteromedial transportalusingtheRigidfixsystempresentedsatisfactoryclinicalresultsoverthelength offollow-upevaluated.However,theriskoflesionsofthejointcartilagefromthedistal Rigidfixpinneedstobetakenintoconsiderationwhenthetechniqueviaananteromedial portalisused.Furtherstudieswithlargernumbersofpatientsandlongerfollow-uptimes shouldbeconductedforbetterevaluation.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
Pleasecitethisarticleas:InácioAM,LopesJúniorOV,KuhnA,SagginJI,FernandesSagginPR,deFreitasSpinelliL,deCastroDM. Reconstruc¸ãodoligamentocruzadoanteriorpeloportalanteromedialefixac¸ãofemoralcomRigidfix.RevBrasOrtop.2014;49:619–624.
夽夽
WorkdevelopedintheInstituteofOrthopedicsandTraumatologyofPassoFundo,PassoFundo,RS,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](A.M.Inácio).
http://dx.doi.org/10.1016/j.rboe.2014.10.004
Reconstruc¸ão
do
ligamento
cruzado
anterior
pelo
portal
anteromedial
e
fixac¸ão
femoral
com
Rigidfix
Palavras-chave:
Joelho/cirurgia
Ligamentocruzadoanterior Reconstruc¸ão
r
e
s
u
m
o
Objetivo:Avaliarumasériedepacientessubmetidosàcirurgiadereconstruc¸ãodoligamento cruzadoanteriorcomtendõesflexorespelatécnicatransportalanteromedialcomousode Rigidfixparafixac¸ãofemoraleanalisaroposicionamentodospinospormeiodetomografia.
Métodos:Foramincluídosnoestudo32pacientes.Aavaliac¸ãoclínicafoifeitacomosescores deLysholm,IKDCsubjetivoeRolimeter.Todosforamsubmetidosatomografia computa-dorizadacomreconstruc¸ãoem3Dparaavaliac¸ãodopontodeentradaedoposicionamento dospinosdoRigidfixemrelac¸ãoàcartilagemarticulardocôndilolateraldofêmur.
Resultados: AmédiadoescoredeLysholmobtidofoide87,81edoIKDCsubjetivo,de83,72. Dos32pacientesavaliados,43%retornaramaatividadesconsideradasmuitovigorosas,9% avigorosas,37,5%amoderadase12,5%aleves.Em16pacientes(50%),opontodeentradado pinodistaldoRigidfixfoilocalizadoforadacartilagem(extracartilagem),emsete(21,87%)o pinodistallesouacartilagemarticular(intracartilagem)eemnove(28,12%)ficounaborda dacartilagemarticulardocôndilolateraldofêmur.
Conclusão: Ospacientessubmetidosàreconstruc¸ãodoLCAcomosistemaRigidfixpela técnicatransportalanteromedialapresentaramumresultadoclínicosatisfatórionotempo deseguimentoavaliado.Entretanto,oriscodelesãodacartilagemarticularpelopinodistal doRigidfixdeveserconsideradoquandoatécnicaviaportalanteromedialéusada.Outros estudoscommaiornúmerodepacientesecomumtempodeseguimentomaislongodevem serfeitosparamelhoravaliac¸ão.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Anteriorcruciateligament(ACL)injuriesareamongthe com-monestligament injuriesofthe knee. Differenttechniques with different types of graft and different fixation meth-ods have been described for surgical treatment, all with satisfactoryclinicalresults.Today,ACLreconstructionusing autologousgraftsfromthetendonsofthegracilisand semi-tendinosus muscles has gained popularity because of the lower morbidityatthe graft donor site, lower incidenceof femoropatellarsymptomsandlowerincidenceofcontractures inflexion.1,2
Thesuccess ofACL reconstruction surgeryis related to various preoperative, transoperativeand postoperative fac-tors. Amongthese, the positioning ofthe bone tunnels in ACLreconstructionsurgery,and consequentlythe position-ingofthetendongraft,isconsideredtobeoneofthesingle mostimportantfactors.Recentstudieshaveshownthatwhen thefemoraltunnelispositionedmoreanatomicallyin rela-tion tothe femoralinsertionofthe ACL,it provides better rotationalcontroloftheknee,betterkneemobilityandless chanceofimpactofthe ACLontheposteriorcruciate liga-ment (PCL) duringflexion.3 There are threetechniques for
constructing the femoral tunnel: the transtibial technique, theoutside-to-insideortwo-incisiontechniqueandthe trans-portaltechnique(anteromedial oraccessorymedialportal). Somestudieshaveshownthatwiththetranstibialtechnique, inwhichthefemoraltunnelisconstructedthroughthetibial tunnel,itismoredifficulttoachieveanatomicalpositioning
of thefemoral tunnel.4,5 For this reason,the anteromedial
transportal technique, with tunnels constructed indepen-dently and without the need for an additional incision in the lateralfaceofthefemur, isaconstant focusof discus-sion.
The different types of tendon graft and the pursuit of femoral tunnel positioning that is more horizontal in the lateralfemoralcondylehavegivenrisetoadaptationofthe fix-ationmethodstraditionallyusedinACLreconstructionwith flexortendons.Thus,transversefixationmethodswithfixed anglesofimplantentryinthelateralfaceofthefemurhave beenreassessed,becausetheymayputtheposterolateraland intra-articularstructuresofthekneeatrisk.4
TheRigidfixsystem(Mytek,Norwood,MA)consistsoftwo pinsmadeofpolylacticacid,diameter2.7mm,forfemoral fix-ationofthegraftinthefemoraltunnel.Thesystemtransfixes thegraftattwopoints,whichproducescompressionagainst thetunnelwallandenablesawidebone-graftcontactarea.6In
ananatomicalstudy,Castoldietal.7evaluatedthepositioning
oftheentryofRigidfixpinsinthelateralcondyleinrelation tothetechniqueviaananteromedialportal. Theseauthors concludedthattheriskofchondrallesionsresultingfromthe entryoftheimplantvariedaccordingtotheangleofthepin insertionguidesandalsoaccordingtothesizeofthefemoral condyles.
alsohadthesecondaryobjectiveofevaluatingthepositioning oftheentryoftheRigidfixpins,bymeansof3Dtomography.
Materials
and
methods
Thirty-twopatientswereselectedforthisstudy.Allofthem were operatedbythe samesurgical teambetween January 2009and July 2010. Thepatients included underwent ACL reconstruction surgery using a quadruple autologous graft fromtheflexortendons(gracilisandsemitendinosus),using RigidfixforfemoralfixationandBiointrafix(Mitek,Norwood, MA,USA)fortibialfixation.Theoperationswereperformed bymeansoftheanteromedialtransportal technique,8 with
atleast24monthsofpostoperativefollow-up.Weexcluded patients from the study in the following situations: if anothertypeofgraftwasusedforACLreconstruction (patel-lar tendon, quadriceps tendon or an allograft); if a route other than the anteromedial transportal route was used for constructing the femoral tunnel; if the follow-up was less than 24 months; or if another method was used for femoral fixation of the graft. This study was approved by our institution’s research bioethics committee and all the individuals evaluated signed a free and informed consent statement.
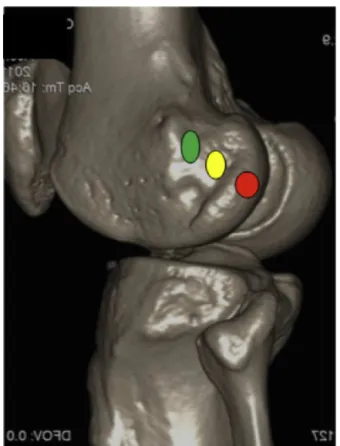
Toevaluatethepositioningofthepointofentryandthe Rigidfixpins,allthepatientsunderwentmultislicecomputed tomography examination with 3D reconstruction (Toshiba; AquilionTSX-101modelwith64channels)withinsixweeks afterthesurgery.Thepositioningofthepointofentryofthe proximalanddistalRigidfixpinsinthelateralfaceofthe lat-eralfemoralcondylewasclassifiedas“intracartilage”(IC),“on theborderofthecartilage”(BC)or“extracartilage”(EC)(Fig.1). Fortheclinicalevaluation,thepatientsunderwent objec-tive measurements on the pre and postoperative anterior and functional translation using the Lysholm scale9,10 and
thesubjectiveIKDCscale.11 TheLysholmscale usesordinal
assessmentscoresandthesearedefinedas“excellent”ifthey arebetween95and100points,“good”ifbetween84and94 points,“fair”ifbetween65and83pointsand“poor”if64points andunder.9,10ThescoresobtainedusingthesubjectiveIKDC
scalecanvaryfromzeroto100andthehigherthescoreis, thebetterthefunctionisconsideredtobe.Theobjective eval-uationoftibialtranslationwasperformedusingaRolimeter (Aircast).12Theclinicalassessmentwasperformedbyan
inde-pendentevaluatorwithoutknowledgeofthepositioningofthe pinsobtainedinthetomographyexamination.
Allthepatientsunderwentthesamepostoperative reha-bilitationprotocol.Partialweight-bearingusingcrutcheswas allowedafterthefirstdayafterthesurgeryandthiswas main-tainedfortwoweeks.Notypeofbracewasused.Exercisesfor achievingcompleterangeofmotionofthejointwereallowed astolerated.Closedkineticchainexerciseswerestartedfour weeksafterthesurgery.Runningandopenkineticchain exer-ciseswerestartedthreemonthsaftertheoperationandthe patientswereallowedtoreturntocontactsportsaftereight monthshadpassed.
ThestatisticalevaluationwasperformedusingtheExcel software(Microsoft)andconsistedofdescriptivestatisticsand frequencydistributions.
Fig.1–Tomographicimageofthekneewith3D
reconstruction,showingthereferencesusedfordefining thepointsofentryoftheRigidfixpinsinthelateralcondyle ofthefemur,inrelationtothejointcartilage.Greenspot– extracartilage;yellowspot–borderofcartilage;andred spot–intracartilage.
Surgical
technique
Thepatientwaspositionedindorsaldecubitusunderspinal anesthesia usedinassociation withperipheralblockofthe ipsilateralfemoralnerve.Apneumatictourniquetwasused ontheproximalthirdofthethighoftheleginvolved.After performingasepsisandantisepsisandplacingsterilefields, thelegwaspositionedwithhipflexionof45◦andkneeflexion
of90◦.
The graft from the tendons of the gracilis and semi-tendinosus muscleswas harvestedinthe usual manner.A quadruplegraftwaspreparedusingKrackowstitches.13The
jointwastheninspectedanddebridementoftheACLstumps was performed, along with arthroscopic treatment for the otherlesionspresent.Aguidewirewasinsertedthroughthe anteromedial portal and was introduced into the femoral insertionoftheACLwiththekneeflexedat120◦,seekingthe
locationoftheinsertionoftheanteromedialbandoftheACL. Thefemoraltunnelwasconstructedthroughthe anterome-dialportal,withalengthof30mm.Thismeasurementwas markedontheproximalextremityofthetendongraft.The tibialtunnelwas constructedwiththeaid ofatibial guide angledat45◦andplacedatthecenterofthetibialinsertionof
thefemoralguide,twoguidecannulaeforintroducingRigidfix werefixedtothelateralfaceofthelateralcondylebymeansof accessoryincisions.Thequadrupletendongraftwaspassed throughthebonetunnelsunderarthroscopicguidance.The femoralfixationofthetendongraftwasperformedusingthe Rigidfixsystem(2.7mm).Thetibialfixationwasperformed withthekneeflexedat30◦,usingtheBiointrafixsystem.
Results
Forthisstudy,32patientswithameanpostoperative follow-upof30months(range:24–36months)wereselected.There were 28males and fourfemales.Their mean age was33.1 years(range:16–56)atthetimeofthesurgery.Twenty-nine patientspresentedmeniscallesions(90.6%),amongwhich20 werelesionsofthemedialmeniscusalone(68.9%),fivewere lesionsofthe lateralmeniscusalone (17.2%)and fourwere lesionsofbothmenisci(13.8%).Partialmeniscectomywas per-formedonthelesionsinallcases.
Regardingthefunctionalevaluation,themean preopera-tiveLysholm score was 74.53 (range: 43–83) and the mean postoperativescorewas87.81(range:53–95),andthisresult canbeconsidered good.9,10 ThemeansubjectiveIKDCwas
74.16 (range: 37.93–91.95) before the operation and 83.72 (57.5–100)aftertheoperation.
Regarding the return to physical activity, 14 patients (43.75%)reportedthattheywereregularlydoingactivitiesthat canbeconsideredtobeveryvigorous,suchassocceror bas-ketball;three(9.3%)citedvigorousactivitiessuchasvolleyball andtennis;12(37.5%)reporteddoingmoderateactivities,such asgymtrainingorrunning;andfour(12.5%)mentionedlight activitiessuchaswalkinganddomesticwork.
Inrelation tosymptoms, 11 ofthe 32 patientsreported painonmakingeffort(34.4%)andsixreportedsporadicedema (18.75%).Inthephysicalexamination,atrophyofthe quadri-cepsmuscleofthethighwasfoundin20patients(62.5%),but theatrophywasonlyconsideredsevereinonepatient(>2cm differenceinrelationtotheoppositeside).
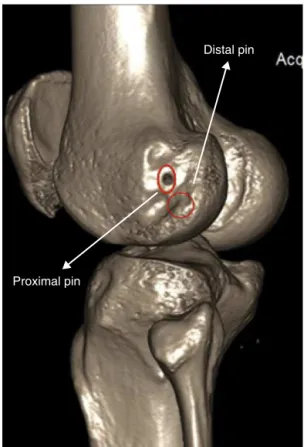
Regardingtheevaluationofthepositioningofthepointof entryoftheRigidfixpins,thepointofentryoftheproximalpin wasoutsideofthecartilageinallthepatients(Fig.2).Thepoint ofentryofthedistalpinwasintheperipheralregionofthe jointcartilageinsevenpatients(21.87%)(Fig.3),attheborder ofthecartilageinnine(28.12%)andoutsidethecartilagein16 (50%)(Table1).
Combinedanalysisonthepinpositionsinrelationtothe jointcartilageandtheresultsfromtheLysholmandsubjective IKDCscoresshowedthat inthe patientsinwhom the dis-talRigidfixpinwaspositionedwithinthecartilage,themean
Table1–PositionoftheRigidfixpinsinthelateral condyleinrelationtothejointcartilage.
Positionofdistal Rigidfixpin
Positionofproximal Rigidfixpin
Extracartilage 16 32 Borderofcartilage 9 – Intracartilage 7 –
Proximal pin
Distal pin
Fig.2–Tomographicimagedemonstratingthepointof
entryoftheproximalRigidfixpinoutsideofthejoint cartilageandthepointofentryofthedistalRigidfixpinat theborderofthejointcartilageofthelateralfaceofthe lateralfemoralcondyle.
Lysholm scorewas89.85(range:89–93) andthemeanIKDC scorewas79.95(range:65.5–95.4);inthoseinwhomthedistal pinwasattheborderofthecartilage,themeanwas88.33for theLysholmscore(range:53–95)and86.2fortheIKDCscore (range:69–100),whileinthoseinwhomthedistalpinwas pos-itionedoutsideofthecartilage,themeanLysholmscorewas 87.2(range:68–95)andthemeanIKDCscorewas83.82(range: 62–98.9)(Table2).
Theanteriortranslationofthetibiainrelationtothefemur wasfoundtobeamean of2.09mminrelationtothe con-tralateralside(1–6mm).Onepatientpresentedanincreasein translationof6mm,relatingtorepeatedtearingoftheACL, andunderwentrevisionsurgeryafterassessmentand inclu-sionofthedataforanalysis.
Table2–Relationshipbetweenthepositionofthedistal RigidfixpinandthemeanLysholmandsubjectiveIKDC scores.
Lysholm SubjectiveIKDC
Distal pin
Proximal pin
Fig.3–Tomographicimagedemonstratingthepointof entryofthedistalRigidfixinthejointcartilageofthelateral faceofthelateralfemoralcondyle.
Discussion
Thereare severalsurgicaltechniquesanddifferentfixation methodsfor ACL reconstructionsurgery. However,none of theserecreatesthe anatomyand tensionalbehaviorofthe fibersthatmakeupthenativeACL.14Thesurgeon’sobjective
incarryingouttheACLreconstructionprocedureissimplyto recreatethefunctionalpatternoftheligament.15
Theidealpositioningofthe bonetunnelsinACL recon-structionsurgeryhasbeenasubjectofconstantdiscussion intheliterature.Somestudieshaveshownthatchangesto thepositioning ofthe femoraltunnelhaveagreater effect onthetensionalbehaviorofthegraftthandochangestothe positioningofthetibialtunnel.15,16FewfibersoftheACLare
isometricthroughouttherangeofmotionoftheknee.14When
amoreisometricgraftisdesired,thefemoraltunnelshouldbe positionedascloseaspossibletothefemoralinsertionofthe anteromedialbandoftheACL.17,18
Therearethreetechniquesthatcanbeusedfor construc-tingthefemoraltunnelwithinarthroscopicreconstructionof theACL:the transtibialand anteromedialtransportal tech-niquesanduseofbothoftheseincisions,ortheoutside-in technique.Inthetranstibialtechnique,thefemoraltunnelis constructedthroughthetibialtunnelandthusthe position-ingofthefemoraltunnelisrestrictedbythepositioningof thetibialtunnel.Thetensionalbehavioroftheneoligamentis moreisometric.However,thereisagreatertendencytoward posteriorizationofthetibialtunnelandverticalizationofthe femoraltunnel,whichdoesnotseemtobeapositionthatcan beconsidered tobemoreanatomical.19 Inthetwo-incision
technique, the bonetunnels are positioned independently, butanadditionalincisionisneededinthelateralfaceofthe femoraltunnel,withafemoraltunnelmadealongtheentire lateralfemoralcondyle.8
Theanteromedialtransportaltechniqueprovidesfemoral tunnelpositioningthatismoreanatomicalandthusbetter rotationalcontrolandlesschanceofimpactonthePCLduring kneeflexion.8Thereisnoneedforadditionalincisionsandthe
femoraltunnelisshorterthaninthetwo-incisiontechnique. Withnewconcepts forfemoraltunnelpositioning,thereis aneedfornewadaptationofthe femoralfixationmethods usedandforgraftfixationinafemoraltunnelthatismore anatomicalandlowerandwhichhasapointofentryinthe medialwallofthe lateralcondyle.20–26 AccordingtoChang
et al.,27 the current efforts for horizontalizing the femoral
tunnelinthemedialwallofthelateralcondylemay compro-misefixationusingtransverse-pinmethodssuchasRigidfix and lead to protrusion ofthese pins. The transverse fixa-tionmethodstraditionallyusedweredevelopedtobeusedby meansoftheanteromedialportaltechniqueandtheypresent afixedangleofentry,whichmayputthelateralstructures ofthe kneeatrisk, alongwiththe jointsurfaceofthe lat-eral femoralcondyle.4,20 In the present study,we choseto
evaluateaseriesofpatientsinwhomRigidfixwasusedfor fixation of a quadruple graft from the flexor tendonsin a femoraltunnel,performedbymeansofananteromedial por-tal.TheRigidfix system theoreticallyprovidesfixation that ismorejuxta-articularbecauseofthepresenceofasecond pinclosertotheintra-articularopeningofthefemoral tun-nel,incomparisonwithothertransverse fixationmethods. Moreover,itenablesagreaterareaofbone-graftcontactthan dointratunnelfixationmethodssuchasuseofinterference screws.7,20Initially,Rigidfixwasdevelopedtoprovidefixation
bymeansofthetranstibialtechnique.6AccordingtoCastoldi
etal.,7fromastudyoncadavers,theriskofchondrallesions
throughusingthistechniqueishigh(between80%and100%), withatleastonepinwithinthejointcartilageofthelateral femoral condyle.They thereforedid notrecommend using RigidfixbymeansofthetransportaltechniqueforACL recon-struction.
Thisstudy presents somelimitations. Itwas a descrip-tivestudyonpreliminaryresultsfromacaseseries.Alonger follow-upperiodandalargernumberofpatients,ina prospec-tivestudywithabetterdesign,areneededinordertoobtain informationofgreaterprecision,withregardtowhetherthe presenceofchondrallesionsinsomepatientsisresponsible forworseningoftheclinicalresults.
Conclusion
ThepatientswhounderwentACLreconstructionbymeansof theRigidfixsystemwiththeanteromedialtransportal tech-niquepresentedasatisfactoryclinicalresult.Theriskofjoint cartilagelesionsduetothedistalRigidfixpinneedstobetaken intoconsiderationbut,inthepresentstudy,thepresenceof chondrallesionsdidnotinterferewiththeresultsoverthe shortfollow-uptimeevaluated.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. BeynnonBD,JohnsonRJ,AbateJA,FlemingBC,NicholsCE.
Treatmentofanteriorcruciateligamentinjuries,partI.AmJ
SportsMed.2005;33(10):1579–602.
2. WebsterKE,FellerJA,HameisterKA.Bonetunnel
enlargementfollowinganteriorcruciateligament
reconstruction:arandomisedcomparisonofhamstringand
patellartendongraftswith2-yearfollow-up.KneeSurg
SportsTraumatolArthrosc.2001;9(2):86–91.
3. ChaPS,ChhabraA,HarnerCD.Single-bundleanterior
cruciateligamentreconstructionusingthemedialportal
technique.OperTechOrthop.2005;15:89–95.
4. GelberPE,ReinaF,TorresR,PelfortX,TeyM,MonllauJC.
Anatomicsingle-bundleanteriorcruciateligament
reconstructionfromtheanteromedialportal:evaluationof
transversefemoralfixationinacadavericmodel.
Arthroscopy.2010;26(5):651–7.
5. GavriilidisI,MotsisEK,PakosEE,GeorgoulisAD,MitsionisG,
XenakisTA.Transtibialversusanteromedialportalofthe
femoraltunnelinACLreconstruction:acadavericstudy.
Knee.2008;15(5):364–7.
6. RodeoSA,ArnoczkySP,TorzilliPA,HidakaC,WarrenRF.
Tendon-healinginabonetunnel.Abiomechanicaland
histologicalstudyinthedog.JBoneJointSurgAm.
1993;75(12):1795–803.
7. CastoldiF,BonasiaDE,MarmottiA,DettoniF,RossiR.ACL
reconstructionusingtheRigidfixfemoralfixationdevicevia
theanteromedialportal:acadaverstudytoevaluatechondral
injuries.KneeSurgSportsTraumatolArthrosc.
2008;16(3):275–8.
8. HantesME,DailianaZ,ZachosVC,VaritimidisSE.Anterior
cruciateligamentreconstructionusingtheBio-TransFix
femoralfixationdeviceandanteromedialportaltechnique.
KneeSurgSportsTraumatolArthrosc.2006;14(5):497–501.
9. LysholmJ,GillquistJ.Evaluationofkneeligamentsurgery
resultswithspecialemphasisonuseofascoringscale.AmJ
SportsMed.1982;10(3):150–4.
10.PeccinMS,CiconelliR,CohenM.Questionárioespecíficopara
sintomasdojoelhoLysholmKneeScoreScale–Traduc¸ãoe
validac¸ãoparaalínguaportuguesa.ActaOrtopBras.
2006;14(5):268–72.
11.IrrgangJ.ACLoutcomes.PaperpresentedatInternational SocietyofArthroscopy,KneeSurgeryandOrthopaedicSports Medicine,2001.Montreux,Switzerland:InternationalKnee DocumentationCommittee;2000.Availableinhttp://www. udel.edu/PT/PT%20Clinical%20Services/journalclub/sojc/03 04/sep03/IKDC.pdf
12.GankoA,EngebretsenL,OzerH.Therolimeter:anew
arthrometercomparedwiththeKT-1000.KneeSurgSports
TraumatolArthrosc.2000;8(1):36–9.
13.KrackowKA,ThomasSC,JonesLC.Anewstitchfor
ligament-tendonfixation.JBoneJointSurgAm.
1986;68(5):764–6.Briefnote.
14.VanEckCF,LesniakBP,SchreiberVM,FuFH.Anatomicsingle
anddouble-bundleanteriorcruciateligamentreconstruction
flowchart.Arthroscopy.2012;26(2):258–68.
15.HefzyMS,GroodES,NoyesFR.Factorsaffectingtheregionof
mostisometricfemoralattachments.PartII:theanterior
cruciateligament.AmJSportsMed.1989;17(2):208–16.
16.WooSL,KanamoriA,ZeminskiJ,YagiM,PapageorgiouC,Fu
FH.Theeffectivenessofreconstructionoftheanterior
cruciateligamentwithhamstringsandpatellartendon.A
cadavericstudycomparinganteriortibialandrotational
loads.JBoneJointSurgAm.2002;84(6):907–14.
17.AmisAA,DawkinsGP.Functionalanatomyoftheanterior
cruciateligament.Fibrebundleactionsrelatedtoligament
replacementsandinjuries.JBoneJointSurgBr.
1991;73(2):260–7.
18.BradleyJ,FitzpatrickD,DanielD,ShercliffT,O’ConnorJ.
Orientationofthecruciateligamentinthesagittalplane.A
methodofpredictingitslength-changewithflexion.JBone
JointSurgBr.1988;70(1):94–9.
19.ArnoldMP,KooloosJ,vanKampenA.Single-incision
techniquemissesanatomicalfemoralanteriorcruciate
ligamentinsertion:acadaverstudy.KneeSurgSports
TraumatolArthrosc.2001;9(4):194–9.
20.AhnJH,ParkJS,LeeYS,ChoYJ.Femoralbioabsorbable
cross-pinfixationinanteriorcruciateligament
reconstruction.Arthroscopy.2007;23(10):1093–9.
21.GironF,CuomoP,AgliettiP,BullAM,AmisAA.Femoral
attachmentoftheanteriorcruciateligament.KneeSurg
SportsTraumatolArthrosc.2006;14(3):250–6.
22.ButlerDL,NoyesFR,GroodES.Ligamentousrestraintsto
anterior-posteriordrawerinthehumanknee.A
biomechanicalstudy.JBoneJointSurgAm.1980;62(2):259–70.
23.YagiM,WongEK,KanamoriA,DebskiRE,FuFH,WooSL.
Biomechanicalanalysisofananatomicanteriorcruciate
ligamentreconstruction.AmJSportsMed.2002;30(5):660–6.
24.EngebretsenL,LewWD,LewisJL,HunterRE,BenumP.
Anterolateralrotatorinstabilityoftheknee.Cadaverstudyof
extraarticularpatellar-tendontransposition.ActaOrthop
Scand.1990;61(3):225–30.
25.NoyesFR.IncommentstoEngebretsenL,LewWD,LewisJL,
HunterRE,BenumP.Anterolateralrotatoryinstabilityofthe
knee.ActaOrthopScand.1990;61(3):225–30.
26.YasudaK,vanEckCF,HoshinoY,FuFH,TashmanS.
Anatomicsingle-anddouble-bundleanteriorcruciate
ligamentreconstruction,part1:basicscience.AmJSports
Med.2011;39(8):1789–99.
27.ChangCB,YooJH,ChungBJ,SeongSC,KimTK.Oblique
femoraltunnelplacementcanincreaserisksofshortfemoral
tunnelandcross-pinprotrusioninanteriorcruciateligament