rev bras reumatol.2016;56(6):530–542
ww w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Review
article
Effects
of
aquatic
exercise
on
muscle
strength
and
functional
performance
of
individuals
with
osteoarthritis:
a
systematic
review
Fernanda
de
Mattos
a,∗,
Neiva
Leite
a,
Arthur
Pitta
b,
Paulo
Cesar
Barauce
Bento
aaUniversidadeFederaldoParaná(UFPR),Curitiba,PR,Brazil
bUniversidadeFederaldoParaná(UFPR),DepartamentodeEducac¸ãoFísica,ProgramadePós-graduac¸ãoemEducac¸ãoFísica,Curitiba,
PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received27October2015
Accepted15June2016
Availableonline4October2016
Keywords: Osteoarthritis
Water-basedexercise
Physicalfunction
Musclestrength
a
b
s
t
r
a
c
t
Water-basedexercises arerecommendedforpeoplewithosteoarthritis(OA), duetothe
beneficialeffectsonphysicalfunction,qualityoflifeandsymptomreduction.However,the
effectsonmusclestrengtharestillcontroversial.Theaimofthisreviewwastoassessand
comparetheeffectsofaquaticexerciseprogramsonmusclestrengthandphysicalfunction
inpeoplewithOA.AsystematicsearchwasperformedatPubmed,ScopusandWebof
Sci-encedatabases.Clinicaltrialswithinterventionsinvolvingaquaticexercisesforindividuals
withOAwereincluded.Themethodologicalqualityofthestudieswasevaluatedusingthe
PEDroscale.296studieswerefoundandtwelvewereselected:sixstudiescomparing
water-basedexerciseswithland-basedexercise,andsixcomparingwater-basedexercisegroups
withthecontrolgroup.Exerciseprogramsincludedmusclestrengthening,aerobic,balance,
flexibilityandstretchingexercises.Durationoftheprogram,weeklyfrequency,intensity
andprogressionvariedbetweenstudies.Beneficialeffectsofaquaticexercisewerefoundon
physicalfunction.However,onlytwooffivestudiesthatassessedmusclestrengthobserved
positiveeffectofaquaticexercise.Althoughitisdifficulttocomparestudiesandestablish
guidelinesforthestandardizedprotocolformulation,itwasobservedthatwater-based
exer-cisescanbeeffectiveonimprovingphysicalfunctionandincreasingmusclestrength,since
theyarewell-structured,withexerciseintensityandoverloadcontrolled.
©2016ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND
license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](F.Mattos).
http://dx.doi.org/10.1016/j.rbre.2016.09.003
2255-5021/©2016ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/
rev bras reumatol.2016;56(6):530–542
531
Efeitos
do
exercício
aquático
na
forc¸a
muscular
e
no
desempenho
funcional
de
indivíduos
com
osteoartrite:
uma
revisão
sistemática
Palavras-chave: Osteoartrite
Exercícioaquático
Funcionalidade
Forc¸amuscular
r
e
s
u
m
o
Exercíciosaquáticossãorecomendadosparapessoascomosteoartrite(OA),pois
melho-ramafuncionalidade,aqualidadedevidaereduzemossintomasdadoenc¸a.Entretanto,
osefeitosnaforc¸amuscularaindasãocontroversos.Oobjetivodestarevisãofoiavaliare
compararoefeitodeprogramasdeexercíciosaquáticosnaforc¸amuscularena
funcionali-dadedepessoascomOA.FoirealizadaumabuscabibliográficanasbasesdedadosPubmed,
ScopuseWebofScience.Foramincluídosensaiosclínicosrealizadoscomintervenc¸ões
envolvendoexercíciosaquáticosparaindivíduoscomOA.Aqualidademetodológicados
estudosfoiavaliadapormeiodaescalaPEDro.Foramencontrados296estudosnototal.
Destes,dozeforamselecionados,sendoseisestudosquecompararamexercíciosaquáticos
comexercíciosrealizadosemsolo,eseisquecompararamumgrupodeexercíciosaquáticos
comgrupocontrole.Osprogramascontemplaramexercíciosdefortalecimentomuscular,
aeróbios,deequilíbrio,deflexibilidadeealongamento.Adurac¸ãodoprograma,afrequência
semanal,aintensidadeeaprogressãovariaramentreosestudos.Foramencontradosefeitos
benéficosdoexercícioaquáticonafuncionalidade,porém,doscincoestudosqueavaliaram
aforc¸amuscular,apenasdoisverificaramefeitopositivodosexercíciosaquáticos.
Emb-orahajadificuldadesparacompararosestudoseestabelecerdiretrizesparaaformulac¸ão
deprotocolospadronizados,observou-sequeexercíciosaquáticospodemsereficientesna
melhoradafuncionalidadeenoaumentodaforc¸amuscular,desdequeosprogramassejam
bemestruturadoscomintensidadeesobrecargacontroladaeprogressiva.
©2016ElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCC
BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Osteoarthritis(OA)isachronicdegenerativediseaseof
mul-tifactorialorigin,beginningusuallybetween50and60years
ofage,1primarilyaffectingkneeandhipjoints.2,3Painisthe
mainsymptomofthediseaseand,whenassociatedwithjoint
stiffness,instabilityandweakness,cancausefunctional
limi-tationsanddifficultiesinperformingactivitiesofdailyliving.4
The treatment of OA includes drug therapy, manual
therapy,and exercise.5,6 Exerciseis ahighlyrecommended
conservativetreatment,witheasyapplicationandlowcost,
andwithlittlechanceofadversereactions.4Thetypesof
exer-cisesmostrecommendedforpeoplewithOAarethosecausing
alow-impactonthejoints,formusclestrengthening,aerobics,
orsomecombinationthereof,carriedoutinwateroronthe
floor.7
Thestrengtheningofthemusclesaroundtheaffectedjoint
isakeypartinthetreatmentofOA,becausethiscontributes
to the quality of cartilage, increases the neural activation
andimprovesintra-andintermuscularcoordination.8In
addi-tion,musclesactasaload-absorbingmechanismduringthe
gait.Therefore,strongermusclescanbetterabsorband
dis-tributetheimpactonthehipandknee,whichincreasesthe
stability8–10andcontributestotheimprovementofthe
func-tionalityandmobility.11
Whencomparedtoland-basedexercises,waterexercises
canoffersomeadvantagestooverweightpatients,with
mobil-itydifficulties,sincethebody weightreliefprovidedbythe
fluctuationreducestheimpactonjointsandtheperception
ofpainintensity.12,13 Theheatedwaterandthehydrostatic
pressure promote muscle relaxation and stress relief, and
alsodecreasemusclespasms,13–16whichfacilitatethe
execu-tionofmovements.Inaddition,studiesinhealthyadultsand
oldersubjectshaveshownthatwaterexercisesareeffective
toincreasemusclestrength.13,17
Previouslyconductedsystematicreviewsontheeffectsof
aquaticexerciseinpeoplewithosteoarthritisfoundbenefits
forpain,functionandqualityoflife.12,13,15,18However,there
arenoreviewstoidentifytheeffectoftheseinterventionson
theperformanceoffunctionandmusclestrengthtests.Thus,
theaimofthisreviewwastoevaluateandcomparetheeffect
ofaquaticexerciseprogramsonmusclestrengthandonthe
functionalityofpeoplewithOA.
Methods
Todevelopthisstudy,aliteraturesearchwasperformedin
thefollowingelectronicdatabases:Pubmed,Scopus,andWeb
ofScience.Theselectionofdescriptorswasbasedonterms
indexedinDescriptorsinHealthSciences(DeCS)andincluded
the following keywords in English: osteoarthritis, aquatic,
aqua,deep-water,water-based,exercise,motoractivity,
phys-icalactivity,andtraining.Thekeywordswerecombinedusing
theBooleanoperators“AND”and“OR”,andwereadaptedfor
eachdatabase,asrequired.
Therewasnorestrictiononthepublicationyear,
consid-ering the low number of studies found in this area. Two
researchers surveyed all databases and, at the end of the
applicationofinclusionandexclusioncriteria,confrontedthe
532
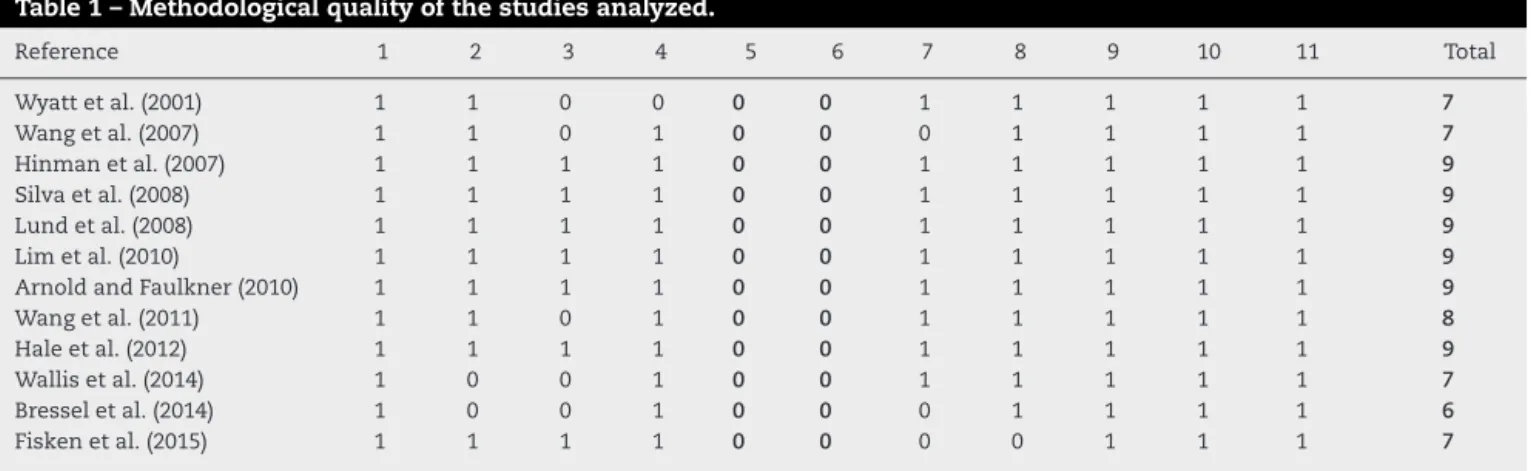
rev bras reumatol.2016;56(6):530–542Table1–Methodologicalqualityofthestudiesanalyzed.
Reference 1 2 3 4 5 6 7 8 9 10 11 Total
Wyattetal.(2001) 1 1 0 0 0 0 1 1 1 1 1 7
Wangetal.(2007) 1 1 0 1 0 0 0 1 1 1 1 7
Hinmanetal.(2007) 1 1 1 1 0 0 1 1 1 1 1 9
Silvaetal.(2008) 1 1 1 1 0 0 1 1 1 1 1 9
Lundetal.(2008) 1 1 1 1 0 0 1 1 1 1 1 9
Limetal.(2010) 1 1 1 1 0 0 1 1 1 1 1 9
ArnoldandFaulkner(2010) 1 1 1 1 0 0 1 1 1 1 1 9
Wangetal.(2011) 1 1 0 1 0 0 1 1 1 1 1 8
Haleetal.(2012) 1 1 1 1 0 0 1 1 1 1 1 9
Wallisetal.(2014) 1 0 0 1 0 0 1 1 1 1 1 7
Bresseletal.(2014) 1 0 0 1 0 0 0 1 1 1 1 6
Fiskenetal.(2015) 1 1 1 1 0 0 0 0 1 1 1 7
1,Eligibilitycriteriaspecified;2,randomizationorrandomassignment;3,secretallocation;4,similargroupsatthebeginning;5,subjectsblinded toparticipation;6,treatmentcarriedoutbyblindedresearchers;7,blindedevaluators;8,evaluationscarriedoutinatleast85%ofthesample; 9,allevaluatedsubjectsweresubmittedtotheintervention;10,resultsofthecomparisonsbetweengroupsweredescribed;11thestudyshows precisionandvariabilitymeasurementsfortheresults.
studies,theresearchersconductedapooledanalysisofstudies
withtheaimofreachingconsensus.
The following inclusion criteria were adopted: articles
publishedinEnglish,PortugueseorSpanish;onlyoriginal
arti-cles; controlledclinical trials or experimental studies with
anexperimentalgroupversus controlgroupor period;
pre-senting an intervention with supervised aquatic exercises
forpeoplewithosteoarthritis;describinginterventiondetails,
suchasduration,frequency,typeandintensity ofexercise;
withanevaluationandpresentation,asprimaryorsecondary
outcomes,ofmuscle strength and/orfunctionalitythrough
physicalperformancetests.
Conferenceabstracts,monographs,dissertationsand
the-ses,casestudies, non-controlledtrials, systematicreviews,
animalstudiesand alsostudieswithmixedgroupsof
sub-jects(osteoarthritisandotherconditionsinfluencingstrength
and/orfunctionality);interventionalstudieslastinglessthan
sixweeks,andthosewithaweeklyfrequencyoftheexercise
programundertwosessions/week,basedonreviewsof
rec-ommendationsforthetreatmentofOA,wereexcludedfrom
thisreview.4,19
The selected studies were also analyzed for
methodo-logicalquality,accordingtotheevaluationprotocoladapted
forthis study,based on the PEDroscale.20 This evaluation
includedelevencriteriawhich,together,generatedascoreof
11(Table1).Criteria5and6,whichdealwiththeblindingof
participantsandtherapistsregardingthetreatmentapplied,
were notscored, due tothe characteristics ofthe selected
studies.Inexperimentalstudiesincludinginterventionswith
programsofphysicalactivity,onecannotomitfrom
partici-pantsandtherapiststhetreatmentcarriedout.Therefore,the
maximumscoreachievedis9points.Thehigherthescoreon
thescale,thebetterthequalityofthestudy.
Theanalysisofthequalityofthestudieswasperformed
independentlybytworesearchers,anddisagreementswere
discussedinconsensusmeetings.Methodologicalqualitywas
assessed with the aim of identifying the internal validity
(criteria2–9)andthequalityofstatisticalinformationforthe
interpretationofresults(criteria10–11).20Afterthisstep,the
outcomesassessedandtheresultsofthestudieswere
ana-lyzedandgroupedintotopics,forcomparisonanddiscussion.
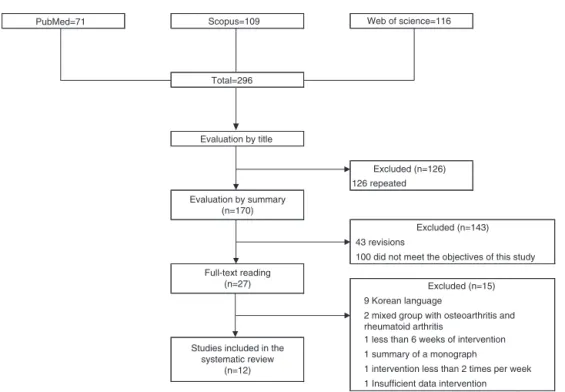
Results
In theelectronicsearch conducted,296studies inallthree
databaseswerefound.Aftertheexclusionofrepeatedtitles,
170 articles remained foranalysis. Afterthe applicationof
inclusionandexclusioncriteria,83titleswereexcluded.Inthe
abstractanalysisstage,48articlesand8systematicreviews
wereexcluded,sincethesestudiesdidnotmeettheobjectives
ofthisreview.Ofthe31remainingarticlesforafullreading,
12wereincludedinthisreview:eightrandomizedcontrolled
trialsandfourexperimentalstudies(Fig.1).
Methodologicalquality
Thescoringoftheselectedstudiesintheevaluationoftheir
methodologicalqualityisdescribedinTable1.Themeanscore
ofthestudieswas8(6–9)points.Themaximumscore(9points)
wasascribedtosixofthe12studiesassessed.14,21–25Four
crite-riawerecoveredbyallstudiesselected:“eligibilitycriteria”;
“allevaluatedsubjectsreceivedintervention”;“resultsofthe
comparisonsbetweengroups”;and“precisionandvariability
measurements.”Innineofthe12studies,theevaluatorswere
unaware ofthe groupinwhich participantswere allocated
(single-blinded).14,21–28Onlythosestudieswhichusedasingle
groupwithadoublepre-test(withafour-weekcontrolperiod)
hadnotarandomallocationofparticipants.28,29
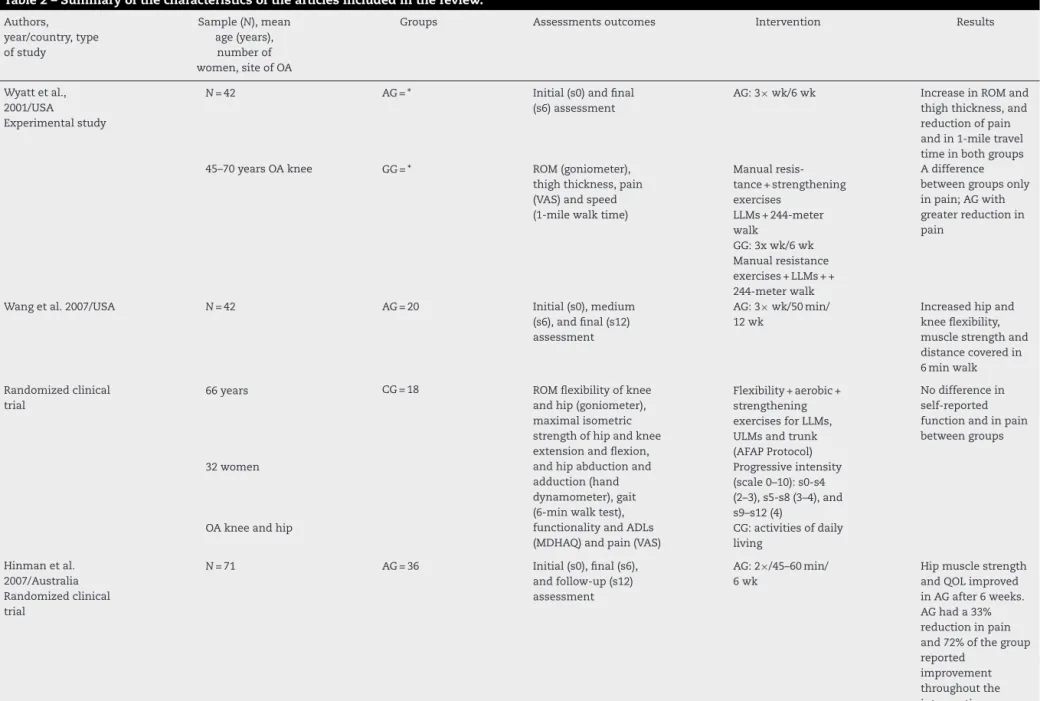
Characteristicsofstudies
The characteristics ofthe studies (participants, measuring
instruments, interventions, and main results) are
summa-rized inTable2.However,thesefeaturesarepresentedand
groupedinthefollowingtext.
Locationandcharacteristicsoftheparticipants
The selected studies were performed in the United
States,26,29,30 Australia,14,28 Brazil,25 Denmark,24 Korea,23
Canada,21 Taiwan,27 and New Zealand.22,31 The study
par-ticipants were recruited from Orthopedic Clinics in local
rev bras reumatol.2016;56(6):530–542
533
PubMed=71 Scopus=109 Web of science=116
Total=296
Evaluation by title
Excluded (n=126) 126 repeated Evaluation by summary
(n=170)
Full-text reading (n=27)
Studies included in the systematic review
(n=12)
9 Korean language
2 mixed group with osteoarthritis and rheumatoid arthritis
1 less than 6 weeks of intervention 1 summary of a monograph
1 intervention less than 2 times per week 1 Insufficient data intervention
Excluded (n=15) 43 revisions
100 did not meet the objectives of this study Excluded (n=143)
Fig.1–Schematicrepresentationoftheselectionofthestudiesincludedinthisreview.
clinics,14,21,22,24,27,29 through dissemination in the local
community and in community centers.14,21,22,24,27,29–31 All
participantshadadiagnosisofkneeand/orhipOA,14,22,28–31
onlyhipOA,21andonlykneeOA,23–27wereagedbetween60
and75years,andmostwerefemale(72%oftotalparticipants).
Characteristicsofinterventions
Theprotocolsofexerciseprogramsdifferamongstudies,but
onecanidentifythemaincomponentsofeachprogram.Six
studies conductedinterventions with a group that
partici-patedinaquaticexerciseandanothergroupthatperformed
land-based exercise,21,23–27 and six other studies only
con-ductedinterventionswithaquaticexercise.14,22,28–31
The programs’ duration ranged from six14,26,28,29 to 18
weeks.25 Two studies conducted 8-week interventions,23,24
ArnoldandFaulkner21did11weeksofexercise,andother4
studiesused12weeksintheirprotocol.22,27,30,31Theweekly
frequencyofexerciseprogramsvariedfromtwo14,21,22,24,28,31
tothree23,25–27,29,30weeklysessions.
Aquatic exercise protocols were composed primarily of
muscle strengthening exercises for upperand lower limbs
andtrunk,14,21,28,30,31aerobicwalkingexercisesandshiftsin
water,14,22,28–30andHigh-IntensityTraining(HIT)inanaquatic
treadmill,29 balancedisturbanceexercises,29 one-footshifts
andmovements,21,22flexibility,27,30andstretching.24,25
Studies comparingprograms ofwaterversusland-based
exercisessoughttofollow similarprotocols inbothmedia,
withstrengtheningexercisesofupperandlower limb
mus-cles,stretching,23–27aerobicwalkingexercises24–27andwater
bikeandonthefloor,23asdetailedinTable2.
Fiveofthe12studiesusedacontrolgroupwithout
inter-vention for comparison with the groups that performed
the exercise.14,21,24,27,30 In studies wherethe controlgroup
receivedsomekindofintervention,exerciseswereperformed
athome,23hydrotherapyexerciseswereperformedin
immer-sioninasittingpositioninthewater,31andcomputer-assisted
activities.22
Theappliedintensityalsovariedamongprotocols.Only
onestudyusedheartrateasareference,fromabasalvalue
of65%HRforaquaticexerciseand40–60%ofone-repetition
maximum(1RM)forland-basedexercise.23 Inotherstudies,
theintensitywascontrolledonthebasisofperceivedexertion
scales(0–10,BorgCR10or6–20),27,29,30cadenceofmusic,24,31
andthenumberofsetsandrepetitions.14,25Onlytwostudies
didnotcontrolordescribetheintensity,21,26andsome
stud-iesdidnotofferin-depthinformationontheprogressionof
intensity.22,28
Outcomes
To be included in this review, the studies should
indi-cate thefunctionalityand/or musclestrength asaprimary
or secondary outcome, assessed by physical performance
tests. Only two studies pointed out functionality as a
primaryendpoint.21,31Ofthefivestudiesthatevaluated
mus-cle strength, three presented this variable as the primary
outcome,23,24,30andtwoasasecondaryoutcome.14,31Painwas
assessedinallstudies;however,itwasconsideredasthe
pri-maryoutcomeinthreeofthem.4,24,25
Ofthe 12 studies included, only the work byLim et al.
(2010)evaluatedthefunctionalitywithoutperforming
phys-icalperformancetests.Inthisstudy,theauthors usedonly
questionnaires.Thephysicaltestsmostusedinother
stud-ies to evaluate the functionality were walking tests that
measure the distance covered in a given time in a usual
speed,14,21,27,28,30teststhatmeasurethetimetocoveracertain
distanceatdifferentspeeds,25,26,29,31andtheTimedUpandGo
534
r
e
v
b
r
a
s
r
e
u
m
a
t
o
l
.
2
0
1
6;
5
6(6)
:530–542
Table2–Summaryofthecharacteristicsofthearticlesincludedinthereview.
Authors, year/country,type ofstudy
Sample(N),mean age(years),
numberof women,siteofOA
Groups Assessmentsoutcomes Intervention Results
Wyattetal., 2001/USA
Experimentalstudy
N=42 AG=* Initial(s0)andfinal
(s6)assessment
AG:3×wk/6wk IncreaseinROMand thighthickness,and reductionofpain andin1-miletravel timeinbothgroups 45–70yearsOAknee GG=* ROM(goniometer),
thighthickness,pain (VAS)andspeed (1-milewalktime)
Manual resis-tance+strengthening exercises
Adifference betweengroupsonly inpain;AGwith greaterreductionin pain
LLMs+244-meter walk
GG:3xwk/6wk Manualresistance exercises+LLMs++ 244-meterwalk Wangetal.2007/USA N=42 AG=20 Initial(s0),medium
(s6),andfinal(s12) assessment
AG:3×wk/50min/ 12wk
Increasedhipand kneeflexibility, musclestrengthand distancecoveredin 6minwalk
Randomizedclinical trial
66years CG=18 ROMflexibilityofknee andhip(goniometer), maximalisometric strengthofhipandknee extensionandflexion, andhipabductionand adduction(hand dynamometer),gait (6-minwalktest), functionalityandADLs (MDHAQ)andpain(VAS)
Flexibility+aerobic+ strengthening exercisesforLLMs, ULMsandtrunk (AFAPProtocol)
Nodifferencein self-reported functionandinpain betweengroups
32women Progressiveintensity
(scale0–10):s0-s4 (2–3),s5-s8(3–4),and s9–s12(4)
OAkneeandhip CG:activitiesofdaily
living
Hinmanetal. 2007/Australia Randomizedclinical trial
N=71 AG=36 Initial(s0),final(s6), andfollow-up(s12) assessment
AG:2×/45–60min/ 6wk
Hipmusclestrength andQOLimproved inAGafter6weeks. AGhada33% reductioninpain and72%ofthegroup reported
r
e
v
b
r
a
s
r
e
u
m
a
t
o
l
.
2
0
1
6;
5
6(6)
:530–542
535
Table2– (Continued)
Authors, year/country,type ofstudy
Sample(N),mean age(years),
numberof women,siteofOA
Groups Assessmentsoutcomes Intervention Results
62years CG=35 Pain(VAS),changeinpain andfunctionality(5-point scale),osteoarthritis (WOMAC),QOL(15-item scale),physicalactivity level(PASE),isometric strengthofhipabduction andkneeextension(hand dynamometer),theStep test,TUGand6-minwalk test
Strengthening exercisesforLLMs: 2×10
reps+6–10minwalk onwater
Atfollow-up(s12) thebenefitswere maintained
48women Waterdepth
decreased throughoutthe intervention
OAkneeandhip CG:activitiesofdaily
living
Silvaetal., 2008/Brazil Randomizedclinical trial
N=64 AG=31 Initial(s0),medium
(s9),andfinal(s18) assessment
AG:3×wk/50min/ 18wk
The15-mtestina comfortablespeed↓ inbothgroups,but athigh-speedGG improvedbetween s1ands9,andAG betweens9ands18A
59years GG=26 Pain(VAS),
osteoarthritis (Lequesneand WOMAC),speed (two-speed15-meter walktest)andpain duringthewalktest (VAS)andNSAIDs
Stretching:
2×20s+Strengthening exerciseforLLMs: 7–10repsof6s (isometric contractions)and 20–40reps
Pain↓inboth groups.LEQUESNE andWOMAC↓in bothgroupsuntilS9; fromS9toS18a decreaseoccurred onlyinAG
59womenOAknee Increasedresistance
totheuseofelastic orofa1-kgweight GG:3×wk/50min/ 18wk
Stretching
536
r
e
v
b
r
a
s
r
e
u
m
a
t
o
l
.
2
0
1
6;
5
6(6)
:530–542
Table2– (Continued)
Authors, year/country,type ofstudy
Sample(N),mean age(years),
numberof women,siteofOA
Groups Assessmentsoutcomes Intervention Results
Lundetal., 2008/Denmark Randomizedclinical trial
N=79 AG=27 Initial(s0),final(s8), andfollow-up(s20) assessment
AGandGG:2× wk/50min/8wk
Musclestrength↑inGG and↓inAGversusCG bothattheendofthe interventionandat follow-up.Theaquatic exerciseshoweda bettereffectonbalance
versusgroundexercise. Pain↓inGGversusCG infollow-up
68years GG=25 Pain(VAS),
osteoarthritis(KOOS), bodysway(static equilibrium–Balance MasterPro)and isokineticstrengthat 30,60and90◦/s (isokinetic
dynamometer–Biodex)
Resisted
exercises+balance and
stability+stretching ofLLMs
62womenOAknee CG=27 Intensitycontrol:
music
CG:activitiesofdaily living
Limetal., 2010/Korea Randomizedclinical trial
N=75 AG=26 Initial(s0)andfinal (s8)assessment
AG:3×wk/40min/ 8wk
AGshowedimproved functionality,painand qualityoflife.Both groupsimprovedthe functionalityoflower limbs.Therewasno changeinkneeflexor andextensorstrength inbothgroups.The physicalcomponent scaleimprovedslightly inbothgroups 65years GG=25 Pain(BPI),osteoarthritis
(WOMAC),QOL(SF-36 version2.0),isokinetic strengthofknee extensorsandflexorsat 60◦/s(isokinetic dynamometer–Biodex)
Heating+Walk+strength+ resistance+
force−aerobic exercises
65womenOAknee CG=24 Intensity>65%ofCF
GG:3×wk/40min/ 8wk
Joint mobiliza-tion+strengthening Intensityof40–60% of1RM
CG:homeexercises: isometrics (quadriceps)and partialsquats
ArnoldandFaulkner, 2010/Canada Randomizedclinical trial
N=83 AG=28 Initial(s0)andfinal (s11)assessment
AG:2×wk/45min/ 11wk
Inphysical
performance,AEGhas improvedversusCGand AG.Similartrendswere foundforTUGandfor the6-minwalktest.An improvementwas foundinefficacyoffalls inAEGversusCG 75years AEG=26 Balance(BergBalance
Scale),gait(6-min walktest),falls(ABC), functionality(STSand TUG),osteoarthritis (AIMS-2),andphysical activitylevel(PASE)
r
e
v
b
r
a
s
r
e
u
m
a
t
o
l
.
2
0
1
6;
5
6(6)
:530–542
537
Table2– (Continued)
Authors, year/country,type ofstudy
Sample(N),mean age(years), numberof women,siteofOA
Groups Assessmentsoutcomes Intervention Results
56womenOAhip CG=27
AEG:2× wk/45min/11wk Sameprogramof AG+30-min educationalsession beforewatertraining (functionaltasks) CG:activitiesofdaily living
Wangetal., 2011/Taiwan Randomizedclinical trial
N=78 AG=26 Initial(s0),medium
(s6),andfinal(s12) assessment
AG:3×wk/60min/ 12wk
Significant
improvementinKOOS, ROM,6-minwalktest andpaininAGandGG
versuscontrolgroup;no significantchangewas foundbetweenAGand GG
67years GG=26 Osteoarthritis
(KOOS),ROM (goniometer)and gait(6-minwalk test)
Flexibility+aerobic exercises(AFAP protocol)
67womenOAknee CG=26 Intensity3–4(Borg
CR10Scale) GG:3×wk/60min/ 12wk
Flexibility+aerobic exercises(PACE Protocol) Intensity3–4(Borg CR10Scale) CG:activitiesofdaily living
Haleetal.,2012/New Zealand
Randomizedclinical trial
N=39 AG=23 Initial(s0)andfinal (s12)assessment
AG:2×
wk/20–60min/12wk
Inbothgroupsthere wasasignificant improvementinStep testandalso improvementintwo itemsofPPA(reaction timeandcontrast sensitivity)inCG.There wasnosignificant improvementinTUG
74years CG=16 Falls(PPAandABC),
dynamicbalance(Step Test),functionality (TUG),and
osteoarthritis(WOMAC andAIMS-2)
Heating+balance exercises↑difficulty 29womenOAknee
andhip
Waterdepth↓ throughoutthe intervention CG:2×wk/60min/ 12wk
538
r
e
v
b
r
a
s
r
e
u
m
a
t
o
l
.
2
0
1
6;
5
6(6)
:530–542
Table2– (Continued)
Authors, year/country,type ofstudy
Sample(N),mean age(years),
numberof women,siteofOA
Groups Assessmentsoutcomes Intervention Results
Wallisetal., 2014/Australia Experimentalstudy
N=20 AG=20 Pre(s-0),initial(s0),and final(s6)assessment
AG:2×wk/105min/ 6wk
Anincreaseof12% wasfoundforthefast walktest.Therewas nosignificant improvementinSTS
71years Self-efficacy(Arthritis
Self-efficacyScale), osteoarthritis(WOMAC), gait(10-minwalktest), functionality(STS),and QOL(EQ-5DandEQ-VAS)
Educationalsessions (60min)+water exercises(45min): Functional,aerobic, ROM,strengthening exercisesofLLMsand exercisesathome (counseling) 9womenOAknee
andhip
Moderateintensity andindividual progression
Bresseletal., 2014/USASingle groupposttest, doublepretest design
N=18 AG=18 Pre-(s4),initial(s0),and final(s6)assessment
SG:2-3x
wk/18–30min/6wk
Therewas significant improvementin functionality, mobilityand balance,and reductioninknee pain
64years Osteoarthritis(KOSS),
pain(VAS),balanceand motorfunction(SMART EquiTestsystem),and functionality(STS,FLT and10-minwalktest)
Balance exercises+HIT components(aquatic mat)/waterjetsto balancedisorder
16women Intensityof14–19
overRPE OAkneeandhip
Fiskenetal., 2015/NewZealand Experimentalstudy
N=35 AG=19 Initial(s0)andfinal(s12) assessment
AG:2×
wk/45–60min/12wk
Inbothgroups,↓in timeinthe400-m walktest.AG improvedonStep testandAIMS-2.AG improvedinFES-I
versusCG.Therewas nosignificant changeinTUG,STS andgripstrengthin bothgroups 70years CG=16 Functionality(TUGandSTS),
dynamicbalance(15-secStep Test),musclestrength(hand dynamometer),gripstrength (Jamardynamometer),gait (400-mwalktest),
osteoarthritis(AIMS2-SF),falls (FES-I),physicalactivitylevel (RAPA)
Strength+aerobic exercise 23womenOAknee,
hip,spineandhands
Intensitycontrol: music
CG:1×
wk/35–40min/12wk HT-type exer-cise+hydrotherapy exercises(AFAP)wk progression
rev bras reumatol.2016;56(6):530–542
539
The evaluation of muscle strength of lower limbs was
performed by indirect tests (Chair Stand Test) in four
studies.21,28,29,31Onlytwostudiesconductedmusclestrength
testsusinganisokineticdynamometer.23,24Threeother
stud-ies assessed muscle strength through isometric testing of
lowerlimbswithadynamometer14,30andhandgripstrength
test.31
Pain is the only outcome present in all studies and
was assessed by a visual analog scale (VAS) of pain
perception,14,24–26,29,30 or through questionnaires.21–23,27,28,31
Althoughnotaninclusioncriterioninthisstudy,theoutcome
“pain”wasaddedtotheresults,consideringthatthisfactor
waspresentinallanalyzedstudies.Additionally,painisone
ofthemostcommonsymptomsofOAandisassociatedwith
functionallimitationscausedbythedisease32,33 andbythe
impactofOAonthepatients’qualityoflife.34,35
Effectsofinterventions
Water×land-basedexercises
All studies comparing aquatic exercise programs and
land-basedexercisefoundsomebeneficialeffectonthe
func-tionality,forexample,anincreaseinthedistancecovered27
andadecreaseinthetimetoperformwalkingtests.25
How-ever,theaquaticexerciseprovedtobemoreefficientversus
land-basedexercisetoimprovebalanceinthestudybyLund
etal.(2008).
Theresultsofmusclestrengtharecontroversial.14,30Only
twoofthefivestudiesthatevaluatedmusclestrengthfound
improvementafterthepracticeofaquaticexercise.Noneof
thestudiescomparingmusclestrengthbetweenthegroups
whounderwentaquaticversusland-basedexercise14,23,24,30,31
foundsomeeffectofaquaticexerciseinincreasingstrength.
Limetal.(2010)couldnotobservechangesinmusclestrength
innoneof theirgroups. However, Lundet al. (2008) found
improvement in muscle strength only in the group that
performed floor exercise, while the group that underwent
aquaticexerciseshowedadecreasedstrengthintheisokinetic
test.
Inallarticlescomparingthetwointerventions,significant
reductionswereobservedinpain,regardlessofthe
environ-mentwheretheexercisewasheld,24,25 butonlyWyattetal.
(2001),Silvaetal.(2008)andLimetal.(2010)reportedagreater
effectinthegroupthatperformedaquaticexercises.
Waterexercises×control
Thestudiesthatcomparedagroupofaquaticexercisesand
acontrolgroupfoundbenefitsofaquaticexercise,interms
offunctionality,with physicalperformancetests. However,
Hale et al. (2012) found no difference between the group
that received the intervention with aquatic exercise and
the control group, as bothshowed improvedfunctionality.
Of the studies that performed the 30-Second Chair Stand
Test,21,28,31,36 only Arnold and Faulkner (2010) founda
sig-nificantimprovementaftertheintervention.Thegroupthat
performedaquaticexercisesandparticipatedineducational
sessionsforthepreventionoffallsincreasedby12%the
num-berofrepetitionsversustheothertwogroups.
Significanteffectsofaquaticexercisewerefoundinmuscle
strengthcomparedtothegroupwithoutinterventionintwo
studies,whichreportedanincreaseof5–10%ofthe
isomet-ricstrengthofthehipabductormuscles,1445%intheknee
extensors, 11.5%inthehipextensors, and14.3%inthehip
abductors.30Ontheotherhand,Fiskenetal.(2015)foundno
effectofaquaticexerciseintheevaluationthrough
manome-try.Painlevelsalsoshowedcontroversialresults.Threestudies
reportedreducedpainaftertheintervention.14,29,31However,
inthestudybyFiskenetal.(2015)bothgroupshada
reduc-tion inpain, but withnodifferencebetweenthem.On the
otherhand,Wangetal.(2007)andWallisetal.(2014)found
nosignificanteffectsofaquaticexerciseinreducingpain.
Discussion
Theobjectiveofthisreviewwastoevaluateandcomparethe
effectofaquaticexerciseprogramsonmusclestrength and
functionofpeoplewithhiporkneeosteoarthritis.
Interven-tionswithexercisesthatcansloworstoptheprogressionof
thediseaseareimportanttothehealthsystem,considering
that theycan reducethe costoftreatments, surgeries,and
hospitalizations;moreover,theseinterventionscanimprove
thequalityoflifeofparticipants.12
The aquaticexercise, a procedure highly recommended
inthe treatmentofOA,may haveadvantagescomparedto
land-basedexercise,because,duetothephysicalproperties
ofwater,theexecutionofthemovementscanbecomeeasier,
decreasingalsothesensationofpain.12,13Strengtheningthe
musclessurroundingtheaffectedjointisanimportantpart
ofthetreatmentofOA.8–10 Therefore, theresistanceofthe
waterisusedasanoverloadingfactorformuscle
strength-eningexercises.Theuseofresistivematerialspromotesan
increasedareaofcontactwithwater,andwillalsoincrease
theexerciseoverload.17,37However,thereisnoconsensusyet
ontheeffectsofaquaticexerciseonmusclestrength.
In this review, only two of the five studies that
evalu-ated muscle strength showed significant effects.14,30 Wang
etal.(2007)conducteda12-weekprogramwiththreeweekly
sessionswithastandardizedprotocolofmuscle
strengthen-ing, aerobicand flexibility exercises(AFAP protocol)38 with
controlledandprogressiveintensity,andachievedsignificant
improvement in isometric muscle strength of knee
exten-sorsandflexorsandhipabductors,adductors,extensorsand
flexors.Similar resultswerefoundbyHinmanetal. (2007),
who prescribedtwoweeklysessionsofaquaticexercisefor
six weeks,with the progressionofthe volume and degree
ofdifficulty oftheexercises;these authorsreported
signif-icantimprovementinisometricmusclestrengthofthehip,
as assessed with hand dynamometry. The progression of
the intensityand thespecificityofexerciseare crucial
fac-tors. Both studies performed specific exercises of muscle
strengthening,whosestrengthandvolumeincreasedoverthe
program,whichmayhaveresultedinneuromuscular
adapta-tionsthroughouttheexerciseprogram.
Ontheotherhand,studiesbyLundetal.(2008),Limetal.
(2010)andFiskenetal.(2015)foundnoimprovementin
mus-clestrength.Whileonestudyreportedasignificantreduction
inmusclestrengthofkneeextensorsandflexorsinan
isoki-neticevaluationat60◦/sinthegroupthatunderwentaquatic
540
rev bras reumatol.2016;56(6):530–542(waterexercise,land-basedexercise,andcontrol)inthe
isoki-neticevaluation23 orinhandgripstrengthinthegroupthat
performed aquaticexercises.31 These resultsmay be
asso-ciatedwith the choiceof exercises,the progressionofthe
program,exerciseintensity,andtestsused.Perhapsthe
hand-gripstrengthtestdoesnotproperlyidentifystrengthgainsin
lowerlimbs.39,40
Interventionsofthesestudieshaveexaminedaquatic
exer-ciseswithoutusingresistivematerialstoincreaseoverload;
thiswasdonewiththeprogressionofthevolumeofexercise,
increasesinthenumberofrepetitions,24orinthedegreeof
dif-ficultyofmovements23andalsointhespeedandmagnitude
ofimplementation of exercises31 throughout the program.
Lundetal.(2008)suggestedthattherewasnoimprovement
inmusclestrengthduetothesmallresistanceimposedinthe
exercises.Theuseofmaterialsthatincreasethecontactarea
withthewaterandthepracticeofhigh-speedmovements
pro-moteanincreasedexerciseoverloadandconsequentincrease
inforceproduction.17,37,41
Additionally, Lund et al. (2008) and Fisken et al. (2015)
usedtherhythmofthemusictodetermineexerciseintensity.
Perhapsthisisnotaneffectivestrategybecauseitdoesnot
respecttheindividualityoftheparticipants.Byusingthesame
rateforallparticipants,theabsoluteeffortisthesame,butthe
relativeeffortmaydifferdependingontheparticipant’s
phys-icalfitness.InthestudyofFiskenetal.(2015),theincreasein
thespeedofexecutionofexercises,accordingtotherhythmof
themusic,wasnotenoughtopromoteimprovementin
mus-clestrength.Themusiccadenceprogressedeverytwoweeks,
rangingfrom92to162bpminthefirstfourweeks,andfrom
92to220bpmfortheremainingperiod.
Studiescomparingaquaticexerciseprogramsversus
land-basedexercises23–27 foundsimilareffectsinbothgroupsin
termsoffunctionalityandinreducingthepain;however,
land-based exerciseprogramswere more effectivein increasing
musclestrength.24Similarresultswereobservedinprevious
experimentalstudies4,42 andinsystematicreviews.43,44 The
land-basedexercisecanbemoreeffectiveversuswater
exer-cise,asthecontrolandincreaseinoverloadcanbeperformed
moreobjectively.
However,whenproperlyknown,thehydrodynamic
prop-ertiesofwatercanbeusedtoincreaseefficientlytheexercise
overload.45Bentoetal.(2014)reportedanincreaseinmuscle
strengthinhealthyoldersubjectswhencomparinga
proto-colofaquaticversusland-basedexercises.Thestrategyused
wasthegradualincreaseintheintensityofexerciseatevery
fourweeks,increasingtheprojectedareaofthelowerlimbs
andthespeedofexecutionofmovements,whichincreases
theresistanceofferedbythewater.
TheresultsfoundbyWyattetal.(2001),Silvaetal.(2007),
Wangetal.(2007;2011),Wallisetal.(2014),Bresseletal.(2014)
andFiskenetal.(2015)forfunctionalityandmobilityindicate
thataquaticexerciseprogramslastingsixweeksormoreand
withtwotothreeweeklysessionsof45–60mincanbeeffective
inimprovingmobilityandgaitspeed.Thesimilaritybetween
themovementsperformedinaquaticexerciseanddailytasks
evaluatedinfunctionaltestscanfacilitatethetransferofthe
gainsfromtheexercise.46,47
Hinmanetal.(2007)andHaleetal.(2012)foundno
improve-ment in mobility tests, due to somecharacteristics ofthe
interventions.InthestudybyHinmanetal.(2007),thesample
wasmorephysicallyactiveandhadalowerfunctional
impair-ment,astheparticipantswereagedunder65andwithonlya
slightdegreeofinvolvementofOA,whichmayhaveinfluenced
theresults.14Physicalexercisepromotesmoresignificant
ben-efitsinolderpeoplewithgreaterfunctionalimpairment.47,48
Evenusingbalance-specificexercises,Haleetal.(2012)found
no difference between experimentaland control groupsin
terms ofbalance,duetotheinterventionperformedinthe
controlgroup.Accordingtotheseauthors,theincreaseindaily
physicalactivityandinsocialinteractionresultingfromthe
interventionwithcomputergamespromotedbenefitssimilar
tothoseintheexperimentalgroup.
Somelimitationsofthisreviewwereobserved.Thespecific
goalofthisstudyrestrictedthenumberofarticlesthatmet
theinclusionandreviewqualitycriteria.However,thestudies
foundrepresenttheliteratureonthesubject.Itwasnot
pos-sibletopoolthedatatoperformameta-analysis,duetothe
methodologicaldiversityofthestudiesandthelackofdetail
inthedescriptionofinterventions,whichalsomadeitdifficult
toidentifyastandardizedprotocolforexerciseprograms.
Conclusion
Thisreviewstudysuggeststhatwell-designedandcontrolled
interventionswithaquaticexerciselastingatleastsixweeks,
contemplating muscle strengthening exercises and aerobic
exercises, canbeeffectiveinincreasingmusclestrengthof
lower limbs and inimproving the functionalityofpatients
withOA.
Althoughthereisdifficultyincomparingdifferentexercise
programsduetomethodologicaldifferences,itseems
impor-tant anindividualizedcontrolofintensity andoverload,as
wellasoftheirprogression.However,thereisnowayto
estab-lish safeguidelines toformulate protocols. Therefore, it is
suggestedgreaterstandardization/controlandalsoagreater
levelofdetailoftheprogramsinfutureexperimentalstudies.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.DuarteVDS,SantosML,RodriguesKDA,RamiresJB,Arêas GPT,BorgesGF.Exercíciosfísicoseosteoartrose:umarevisão sistemática.RevistaFisioterapiaeMovimento(Curitiba). 2013;26:193–202.
2.FelsonDT,LawrenceRC.NIHConferenceOsteoarthritis:new insights.AnnInternMed.2000;133:637–9.
3.CrossM,SmithE,HoyD,NolteS,AckemanI,FransenM,etal. Theglobalburdenofhipandkneeosteoarthritis:estimates fromtheGlobalBurdenofDisease2010study.AnnRheum Dis.2014;73:1323–30.
4.BennellKL,HinmanRS.Areviewoftheclinicalevidencefor exerciseinosteoarthritisofthehipandknee.JSciMedSport. 2011;14:4–9.
rev bras reumatol.2016;56(6):530–542
541
6. McAlindonTE,BannuruRR,SullivanMC,ArdenNK, BrenbaumF,Bierma-ZeinstraSM,etal.OARSIguidelinesfor thenon-surgicalmanagementofkneeosteoarthritis. OsteoarthrCartil.2014;22:363–88.
7. NelsonAE,AllenKD,GolightlyYM,GoodeAP,JordanJM.A systematicreviewofrecommendationsandguidelinesforthe managementofosteoarthritis:TheChronicOsteoarthritis ManagementInitiativeoftheU.S.BoneandJointInitiative. SeminArthritisRheum.2014;43:701–12.
8. BeckwéeD,VaesP,CnuddeM,SwinnenE,BautmansI. Osteoarthritisoftheknee:whydoesexercisework?A qualitativestudyoftheliterature.AgeingResRev. 2013;12:226–36.
9. KnoopJ,DekkerJ,vanderLeedenM,vanderEschM, ThorstenssonCA,GerritsenM,etal.Kneejointstabilization therapyinpatientswithosteoarthritisoftheknee:a randomized,controlledtrial.OsteoarthrCartil. 2013;21:1025–34.
10.HinmanRS,HuntMA,CreabyMW,WrigleyTV,McManusFJ, BennellKL.Hipmuscleweaknessinindividualswithmedial kneeosteoarthritis.ArthritisCareRes(Hoboken).
2010;62:1190–3.
11.DeOliveiraAMI,PeccinMS,daSilvaKNG,dePaivaTeixeira LEP,TrevisaniVFM.Impactodosexercíciosnacapacidade funcionaledorempacientescomosteoartritedejoelhos: ensaioclínicorandomizado.RevBrasReumatol.
2012;52:876–82.
12.LuM,SuY,ZhangY,WangW,HeZ,LiuF,etal.Effectiveness ofaquaticexercisefortreatmentofkneeosteoarthritis: Systematicreviewandmeta-analysis.ZRheumatol. 2015;74:543–52.
13.YázigiF,EspanhaM,VieiraF,MessierSP,MonteiroC,Veloso AP.ThePICOproject:aquaticexerciseforkneeosteoarthritis inoverweightandobeseindividuals.BMCMusculoskelet Disord.2013;14:320.
14.HinmanRS,HeywoodSE,DayAR.Aquaticphysicaltherapy forhipandkneeosteoarthritis:resultsofasingle-blind randomizedcontrolledtrial.PhysTher.2007;87:32–43. 15.BarkerAL,TalevskiJ,MorelloRT,BrandCA,RahmannAE,
UrquhartDM.Effectivenessofaquaticexercisefor
musculoskeletalconditions:ameta-analysis.ArchPhysMed Rehabil.2014;95:1776–86.
16.AmbrosiniAB,BrentanoMA,CoertjensM,KruelLFM.The effectsofstrengthtraininginhydrogymnasticsfor middle-agewomen.IntJAquatResEduc.2010;4:153–62. 17.BentoPCB,PereiraG,UgrinowitschC,RodackiALF.Theeffects
ofawater-basedexerciseprogramonstrengthan functionalityofolderadults.JAgingPhysAct.2012;20: 469–84.
18.BatterhamSI,HeywoodS,KeatingJL.Systematicreviewand meta-analysiscomparinglandandaquaticexercisefor peoplewithhiporkneearthritisonfunction,mobilityand otherhealthoutcomes.BMCMusculoskeletDisord. 2011;12:123.
19.ZhangW,NukiG,MoskowitzRW,AbramsonRD,AltmanNK, ArdenS,etal.OARSIrecommendationsforthemanagement ofhipandkneeosteoarthritis.PartIII:Changesinevidence followingsystematiccumulativeupdateofresearch publishedthroughJanuary2009.OsteoarthrCartil. 2010;18:476–99.
20.PedroT,ApV,DelphiT.PEDroscale.1999.Availableat:
http://www.pedro.org.au/portuguese/downloads/pedro-scale
[acessedon15.07.15].
21.ArnoldCM,FaulknerRA.Theeffectofaquaticexerciseand educationonloweringfallriskinolderadultswithhip osteoarthritis.JAgingPhysAct.2010;18:245–60.
22.HaleLA,WatersD,HerbisonP.Arandomizedcontrolledtrial toinvestigatetheeffectsofwater-basedexercisetoimprove fallsriskandphysicalfunctioninolderadultswith
lower-extremityosteoarthritis.ArchPhysMedRehabil. 2012;93:27–34.
23.LimJ-Y,TchaiE,JangS-N.Effectivenessofaquaticexercisefor obesepatientswithkneeosteoarthritis:arandomized controlledtrial.Pm&R.2010;2:723–31.
24.LundH,WeileU,ChristensenR,RostockB,DowneyA,Bartels EM,etal.Arandomizedcontrolledtrialofaquaticand land-basedexerciseinpatientswithkneeosteoarthritis.J RehabilMed.2008;40:137–44.
25.SilvaLE,ValimV,PessanhaAPC,OliveiraLM,MyamotoS, JonesA,etal.Hydrotherapyversusconventionalland-based exerciseforthemanagementofpatientswithosteoarthritis oftheknee:arandomizedclinicaltrial.PhysTher.
2008;88:12–21.
26.WyattFB,MilamS,ManskeRC,DeereR.Theeffectsofaquatic andtraditionalexerciseprogramsonpersonswithknee osteoarthritis.JStrengthCondRes.2001;15:337–40. 27.WangTJ,LeeSC,LiangSY,TungHH,WuSFV,LinYP.
Comparingtheefficacyofaquaticexercisesandland-based exercisesforpatientswithkneeosteoarthritis.JClinNurs. 2011;20:2609–22.
28.WallisJA,WebsterKE,LevingerP,FongC,TaylorNF.A pre-operativegrouprehabilitationprogrammeprovided limitedbenefitforpeoplewithseverehipandknee osteoarthritis.DisabilRehabil.2014;36:2085–90.
29.BresselE,WingJE,MillerAI,DolnyDG.High-intensityinterval trainingonanaquatictreadmillinadultswithosteoarthritis: effectonpain,balance,function,andmobility.JStrength CondRes.2014;28:2088–96.
30.WangT-J,BelzaB,ThompsonFE,WhitneyJD,BennettK. Effectsofaquaticexerciseonflexibility,strengthandaerobic fitnessinadultswithosteoarthritisofthehiporknee.JAdv Nurs.2007;57:141–52.
31.FiskenAL,WatersDL,HingWA,SteeleM,KeoghJW. Comparativeeffectsof2aquaexerciseprogramsonphysical function,balance,andperceivedqualityoflifeinolderadults withosteoarthritis.JGeriatrPhysTher.2015;38:17–27. 32.McAlindonTE,CooperC,KirwanJR,DieppePa.Kneepainand
disabilityinthecommunity.BrJRheumatol.1992;31:189–92. 33.HallMC,MockettSP,DohertyM.Relativeimpactof
radiographicosteoarthritisandpainonquadricepsstrength, proprioception,staticposturalswayandlowerlimbfunction. AnnRheumDis.2006;65:865–70.
34.PangJ,CaoY,ZhengY,GaoN,WangX,ChenB,etal.Influence ofpainseverityonhealth-relatedqualityoflifeinChinese kneeosteoarthritispatients.IntJClinExpMed.2015;8:4472–9. 35.TerweeCB,vanderSlikkeRMa,vanLummelRC,BeninkRJ,
MeijersWGH,deVetHCW.Self-reportedphysicalfunctioning wasmoreinfluencedbypainthanperformance-based physicalfunctioninginknee-osteoarthritispatients.JClin Epidemiol.2006;59:724–31.
36.RoperJ,TillmanMD,BresselE.Aquatictreadmillexercise improvesgaitmechanicsandmobilityforindividualswith unilateralkneeosteoarthritis.JGenInternMed.2012;27:691. 37.TsourlouT,BenikA,DiplaK,ZafeiridisA,KellisS.Theeffects
ofatwenty-fourweekaquatictrainingprogramonmuscular strengthperformanceinhealthyelderlywomen.JStrength CondRes.2006;20:811.
38.SuomiR,LindauerS.Effectivenessofarthritisfoundation aquaticprogramonstrengthandrangeofmotioninwomen witharthritis.JAgingPhysAct.1997;5:341–51.
39.NormanK,StobäusN,GonzalezMC,SchulzkeJ-D,PirlichM. Handgripstrength:outcomepredictorandmarkerof nutritionalstatus.ClinNutr.2011;30:135–42.
542
rev bras reumatol.2016;56(6):530–54241.BentoPCB,RodackiALF.Musclefunctioninagedwomenin responsetoawater-basedexercisesprogramandprogressive resistancetraining.GeriatrGerontolInt.2015;15:1193–2000. 42.SuomiR,CollierD.Effectsofarthritisexerciseprogramson
functionalfitnessandperceivedactivitiesofdailyliving measuresinolderadultswitharthritis.ArchPhysMed Rehabil.2003;84:1589–94.
43.JordanKM,ArdenNK,DohertyM,BannwarthB,BijlsmaJWJ, DieppeP,etal.EULARRecommendations2003:anevidence basedapproachtothemanagementofkneeosteoarthritis: ReportofaTaskForceoftheStandingCommitteefor InternationalClinicalStudiesIncludingTherapeuticTrials (ESCISIT).AnnRheumDis.2003;62:1145–55.
44.BartelsElseM,LundH,HagenKåreB,DagfinrudH, ChristensenR,Danneskiold-SamsøeB.Aquaticexercisefor
thetreatmentofkneeandhiposteoarthritis.Cochrane DatabaseSystRev.2007:CD005523.
45.RahmannAE.Exerciseforpeoplewithhiporknee osteoarthritis:acomparisonofland-basedandaquatic interventions.OpenAccessJSportMed.2010;1:123–35. 46.HazellT,KennoK,JakobiJ.Functionalbenefitofpower
trainingforolderadults.JAgingPhysAct.2007;15: 349–59.
47.BarryBK,CarsonRG.Theconsequencesofresistancetraining formovementcontrolinolderadults.JGerontolABiolSci MedSci.2004;59:730–54.