rev bras ortop.2017;52(3):242–250
SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Review
Article
Patient-specific
instrumentation
in
total
knee
arthroplasty.
Should
we
adopt
it?
夽
Ana
Sofia
Teles
Rodrigues
∗,
Manuel
António
Pereira
Gutierres
UniversidadedoPorto,FaculdadedeMedicina,DepartamentodeOrtopediaeTraumatologia,Porto,Portugal
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received9March2016 Accepted13June2016
Availableonline15September2016
Keywords:
Arthroplasty Replacement
Knee/instrumentation Patient-specificmodeling Kneeprosthesis
Prosthesisdesign
a
b
s
t
r
a
c
t
Totalkneearthroplasty(TKA)isasurgicalprocedureofparamountrelevancethatrestoresa substantialdegreeoffunctioninarthriticknees.Increasedconsiderationhasbeengivento theinfluenceoflimbalignmentonlongevityafterTKA,aserrorsincomponentplacement canbeassociatedwithinferiorfunctionandcompromisedlong-termperformance. Con-sequently,numerousstudiescomparingpatient-specificinstrumentation(PSI)tostandard instruments(SI)havebeenpublished.Patient-specificapproachesusepreoperativeimaging tocreatespecificmaterialsforeachpatient’sanatomyandweredesignedtoachieveahigher rateofsuccessinTKA,causingtheentireproceduretobemoreefficientandcost-effective. However,itisnotcleartowhatdegreethesestudiessupportthepotentialadvantagesof PSI.Thus,thepresentstudyaimed toreviewthecurrentevidencecomparingPSItoSI, concerningalignment,cost-effectiveness,andpostoperativefunctionalevaluation.
©2016PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeOrtopedia eTraumatologia.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
Instrumentac¸ão
personalizada
na
artroplastia
total
do
joelho.
Devemos
adotá-la?
Palavras-chave:
Artroplastia Substituic¸ão
Joelho/instrumentac¸ão
Modelagempersonalizada
Prótesedojoelho Desenhodeprótese
r
e
s
u
m
o
Aartroplastiatotaldojoelho(ATJ)éumprocedimentocirúrgicodefundamental relevân-cia que restaura boa parte da func¸ão de joelhos artríticos. Maior atenc¸ão tem sido
dada à influência do alinhamento do membro na longevidade após a ATJ, uma vez
queerros noposicionamentodos componentespodem estar associados àuma menor
func¸ãoecompromentimentododesempenhoalongoprazo.Consequentemente,vários
estudos compararam a instrumentac¸ão personalizada para cada paciente (IPP) com a instrumentac¸ãopadrão(IP).Asabordagenspersonalizadasusamimagenspré-operatórias paracriarmateriaisespecíficosparaaanatomiadecadapacienteeforamprojetadospara atingirumamaiortaxadesucessonaATJ,tornandotodooprocessomaiseficienteerentável. Noentanto,nãoestáclaroatéquepontotaisestudosrespaldamasvantagenspotenciaisda IPP.Assim,opresenteestudotevecomoobjetivoavaliarasevidênciasatuais,comparando
夽
WorkperformedintheUniversidadedoPorto,FaculdadedeMedicina,Porto,Portugal.
∗ Correspondingauthor.
E-mail:a.sofiateles@gmail.com(A.S.Rodrigues).
http://dx.doi.org/10.1016/j.rboe.2016.06.008
rev bras ortop.2017;52(3):242–250
243
IPPeIPemrespeitoaoalinhamento,relac¸ãocusto-benefícioeavaliac¸ãofuncional pós-operatória.
©2016PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileirade OrtopediaeTraumatologia.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND
(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Totalkneearthroplasty(TKA)isconsideredasuccessful
ortho-pedic procedure in the management ofdegenerative joint
disease based on the rate ofrevision. It representsone of
the most regularly performed musculoskeletal procedures,
restoring,inmostcases,asubstantialdegreeoffunctionin
arthritic knees. One can anticipate an increase in TKA in
thefuture, givenestimatedenlargementinpopulation size andlongevity.Therefore,perfectingsurgicaltechniqueisof
paramountrelevance,aserrorsincomponentplacementcan
beassociatedwithinferiorfunctionandcompromised long-termperformance.1,2
Forthepastfewyears,increasedconsiderationhasbeen
placedonthe influenceoflimbalignmentand component
position on longevity and outcomes after TKA,
review-ing the survivorship andpostoperative performanceofthe
procedure.3–5 Ithasbeen establishedthatneutral
mechani-calalignmentiscriticalintheoverallsuccessofthesurgical
technique.2,6 Consequently, tibial and femoral component
malalignmentremains a significant concern, as deviations
exceeding3◦ofvarus/valgusinthemechanicalaxishavebeen
relatedwithpoorsurvivorship duetotheaccelerated wear resultantofabnormalstressesatthebearingsurfaces. Accord-ingly,tibialandfemoralcomponentsareneededtobeplaced
asprecisely as possibleand preventing malalignmentmay
provetobecost-effective.
That being said, two technological advancements,
aim-ing at improving the likelihood of achieving neutral TKA
alignment,haveemerged:computer-assistednavigationand
patient-specific instrumentation(PSI).7 Recently,numerous
comparative studies and randomizedcontrolled trials that
compare patient-specific cutting blocks to conventional
instrumentshavebeenpublished.However,itisnotclearto whatdegreethesestudiessupportthepotentialadvantages ofPSI.8–10 Forthatreason,thepurposeofthepresentstudy
istoperformareviewofthecurrentevidencecomparingPSI toSI,concerningalignment,cost-effectivenessand postop-erativefunctionalevaluation.Existinginformationconcerning
computer-assisted navigation will not be assessed in this
review.
Patient-specific
instrumentation
Aimingatenhancingtheoutcomesofthesurgery,the
man-ufacturing process for knee implants has improved over
theyears,involving,lately,patient-specificapproaches.The purposewastogetthemostaccuratepositioningforthe tib-ialandfemoralcomponents.3,11Thistechnologyemploysthe
generationofapreoperativeimageofthe knee,along with hipandankleimagesfortheevaluationoftheoverall
align-mentofthelimb,mostcommonlycomputedtomography(CT)
ormagneticresonanceimaging(MRI).Computersoftwareis
usedtogenerateanidealthree-dimensional(3D)modelofthe patient’slowerlimbanatomy,allowingtheanatomical land-marksofthekneetobeeasilyidentified, andtocreatethe 3Dmodelsofthefemoralandtibialcomponentswithoptimal size,positionand alignment.Apreoperativeplan proposed withbonyresectionsisgeneratedandprovidedtothe operat-ingsurgeon,whoisthenabletoassessthe3Dplanningofthe kneeimplantwiththeproposedbonyresectionsandwiththe finalimplantsinplace.Atthispoint,thesurgeonisexpectedto approveorreviewthepreoperativeplan,adjustingasrequired bonyresection.Whenapproved,generallywithin3weeks,the manufacturerfabricatesacorrespondingsetofcustomcutting blocksindividualizedtothepatient’snativeanatomy.1,3These
cuttingjigs are expectedto notonlydeterminethe proper coronal orientation, but also set the depth offemoral and tibialresection,anteroposteriorposition,rotation,andslope basedonthepreoperativeprototype.Alterationsin preoper-ative schedulingare inevitable withthe implementationof PSI:first,theplanningprocesshastobeanticipated,since,as mentionedabove,atleast3weeksarenecessarytofabricate
the cuttingblocks;second,the 3Dimagingstudies
manda-torypreoperativelywerenottypicallyperformedpreviously forconventionalTKA.Atlast,manufacturerandsurgeonmust cooperatefortheelaborationandapprovalofthepreoperative plan,ensuringthattheguidesareavailablebythetimeofthe procedure.7,12
Patient-specificinstrumentationwasdesignedtoachievea higherrateofsuccessinTKA,decreasingtheoddsofrevision.
The anticipated benefitsof this technology are numerous,
causingthe entireprocedure tobemoreefficientand cost-effective.7,13,14
First, being the patient-matched technology potentially
morepreciseandaccurate,withareductioninthe number
of outliers expected to be significant, neutral
postopera-tive alignment would be more reproducible with the use
of patient-specific jigs when compared to standard
align-menttechniques.12Second,thesurgeonhaspreoperativedata
regardingthesizeandlocationofthebonyresections,along with implant sizing and rotation information. This way, it is possible to intraoperatively determine if the surgery is
proceeding as expected. Third, as fewer instruments trays
are requiredperprocedure, thesterilizationcostswouldbe reduced.12,15Fourth,amoreefficientsurgeryispredictedwith
reductionofthetimeoftheprocedure,oncedifferentsteps havealreadybeenperformed,alsominimizingintraoperative decision making.11,12,16 Finally, by notrequiring the use of
intramedullaryrodstodeterminealignment,PSIavoids vio-lationoftheintramedullarycanal,potentiallyenablingtothe incidenceoffatembolismandperioperativebloodloss.14,17
244
rev bras ortop.2017;52(3):242–250data to support its use. It remains controversial whether
advantagesovercome weaknesses.3,16,17 With the necessity
ofapreoperativeCTscan,theradiationexposureincreases. Additionally,it isunclearif theanticipated costsreduction offsetthoseofthepreoperativestudiesandmanufacturingto fabricatethematerials.15,17Moreover,surgeriesmayneedto
bedelayedduetothesubstantialamountoftimerequiredto obtainthesuitablepreoperativeimaging,formulatethe intra-operativeplan,andtofabricatethecuttingblocks.Lastly,the precisionofanatomiclandmarkinghasbeenfoundtobe cru-cialtothefinalaccuracyofthe technique.Deformitiesthat maymisrepresenttheexactnessoftheCTscanorMRI, possi-blywillleadtoacompromised3Dmodel.
Methods
A literature review was conducted related to the use of
PSIinTKAusingPubmeddatabase,onSeptember25,2015,
using the query “total knee arthroplasty/instrumentation”
AND(“patientspecific”OR“patientmatched”).Theliterature searchidentified100studies,whichwerethenlimitedto31 publishedbasedonthefollowinginclusioncriteria:(1)
com-parison ofpatients who underwent TKA withPSI tothose
whounderwentTKAwithconventionalinstrumentation;(2)
performedinvivo;(3)assessmentofpostoperativecoronal, sagittalorrotationalcomponentalignment,operativetime, cost and/orfunction scores. Review articles, editorials and techniquedescriptionswere excluded. Studiesthat didnot meetthecriteriaordidnotaddressthepurposeofthepresent reviewwereexcluded,aswerestudiespublishedinanother languagethanEnglishandbefore2010.Thebibliographiesof theselectedstudieswerenotsearchedadditionally.
Results
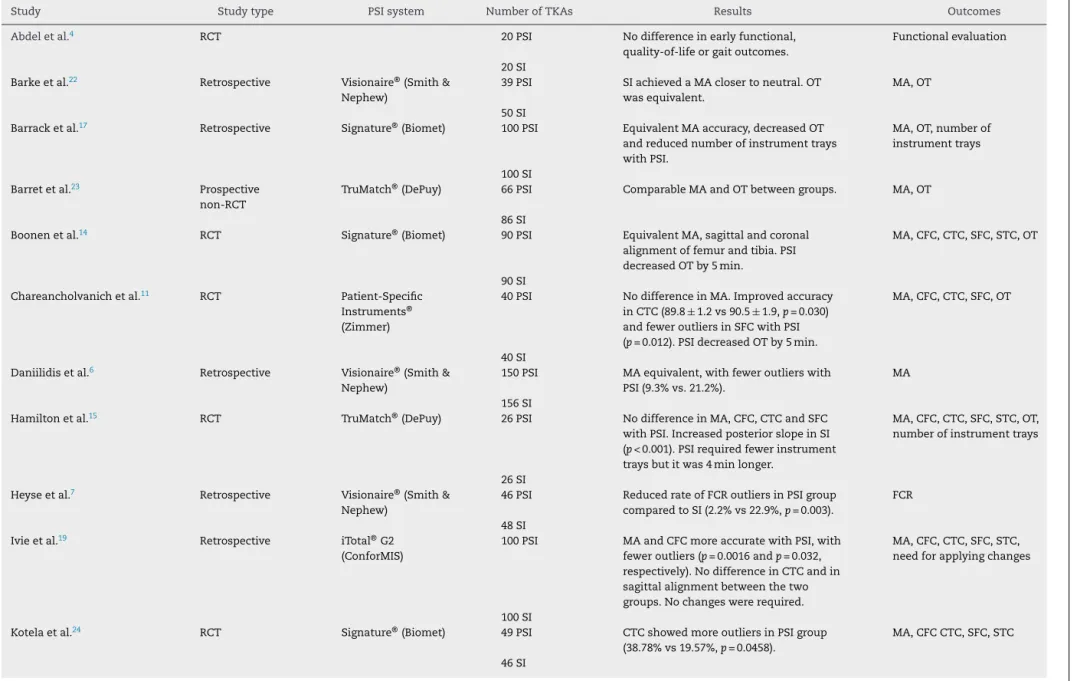
ThemainresultsaresummarizedinTable1.
Alignment
Achievingthemostpossibleaccuratealignmentatthe
com-pletion of TKA has been the upmost surgical goal for
the procedure, with numerous publications demonstrating
improvedsurvivorshipwiththisresult.Atleasttheoretically, patient-specific cutting blocks are believed to improve the accuracyoflimbalignmentbyguidingthecriticalbonecuts toward the hypothetically ideal position for each patient.
Despitemuchdebateontheusefulnessoftheinstruments,
therearestudiescomparing thevalueofthe new
mechan-icallyalignedPSIsystemtothatofstandardprocedurethat validatethesurgicalaccuracyofthetechniquetodate.
Fourrandomizedclinicaltrials(RTC)reportedresults sup-portingPSI.Withrespecttoachievingmechanicalalignment closertoneutral,Noble et al.12 favoredPSIover SI (1.7◦ vs
2.8◦; p=0.03). Chareancholvanich et al.11 and Vundelinckx
et al.3 reportedno difference inmechanicalalignment but
thefirstonedidnoteanimprovementinfrontaltibial compo-nentalignmentwithPSIbeingclosertoneutral(89.8◦versus
90.5◦;p=0.03),whilethesecondonefoundthatPSIwasmore
accurateinreproducingthedesiredtibiaposteriorslope(2.9◦
versus 5.0◦; p=0.0008).Silva et al.18 aimedatstudying the
rotationalalignmentandtheauthorsassumedthatthereis asmallerchanceofinternalmalrotationofthetibial compo-nentwithPSI,havingthetraditionalinstrumentationhigher
dispersion and amplitude ofthe tibialcomponent rotation
around the neutral position. Numerousretrospective
stud-ies noted similar results, with significant improvement in extremitymechanicalalignmentafterPSI.2,6,7,19AlsoRenson
etal.20 prospectivelyreportedmoreoutlierswithrespectto
mechanicalaxiswithSI(p=0.043).Additionally,femoral com-ponentfrontalplaneposition19 androtationalalignmentof
thefemoralcomponent7werealsoreportedtobeenhanced
withPSI.
Althoughproponentsofpatient-matchedinstrumentation
contendthatitimprovesalignment,otherwell-designed com-parativetrialshaverevealed noimprovementinalignment.
TheseauthorswerenotabletoshowimprovementwithPSI,
but the customized techniquedid notend upbeing worse
thantraditionalinstrumentation.TheaccuracybetweenTKAs
performedwithPSIandthose donewithSIwasconsidered
comparable.ArandomizedcontrolledtrialconductedbyRoh etal.9showednosignificantdifferenceneitherinthemean
alignmentinallparametersevaluated(mechanicalaxis,
sag-ittalandcoronalalignmentofeachcomponentandfemoral
component rotation) nor in the percentageof outliers. For Nunley etal.,16,21 inaretrospective study,bothgroupshad
the mean coronal alignment measurements falling within
theacceptedrangesandthemeanHKAandequivalentthe
number of outliers. The same results are shared by other
authors.5,10,17,22,23
Atlast,someauthorsnotonlyconcludedthatno
improve-ment in alignment was achieved with the use of PSI, but
alsoreporteddecreasedalignmentaccuracy.Inarecent ran-domizedcontrolledtrial,Victorelal.1comparedconventional
instrumentationwithpatient-specificguidesfromfour differ-ent implant suppliers: Signature® (Biomet Inc, Warsaw,IN,
USA), TruMatch® (DePuyInc,Warsaw,IN,USA),Visionaire®
(Smith&NephewInc,Memphis,TN,USA)andPatient-Specific Instruments®(ZimmerInc,Warsaw,IN,USA).TheuseofPSI
didnotreducethenumberofoutliers.Actually,theauthors foundmoreoutliersinthesagittalandcoronalalignmentof the tibialcomponent (23%vs17%;p=0.002and15%vs3%;
p=0.03,respectively)withtheuseofPSI.Deviationsfrom tar-getalignmentamongPSIsubgroupsweresimilar,exceptfor sagittalalignmentofthefemoralcomponent,whichwas sig-nificantlybetterforthePSIsubgroupusingVisionaire®system
(p=0.02)andhadfeweroutliers(p=0.001).Yet,thesame sys-temrevealedmoreoverallcoronalalignmentoutliers(p=0.04).
In anotherrecent RCTs,bothevaluating TruMatch® (DePuy
Inc, Warsaw, IN,USA) system,Hamilton e Parks.15 showed
improvedposteriortibialslopeinSIcases(p=0.001),whereas Woolsonetal.8reportedasignificantincreaseinthenumber
ofoutliersforthesameparameterinthePSIgroup. Addition-ally,Kotelaetal.24foundanincreaseinthenumberofoutliers
forcoronaltibialcomponentafterwithPSIhavingconducteda RCT.Similarly,Stronachetal.25retrospectivelyrevieweddata
r
e
v
b
r
a
s
o
r
t
o
p
.
2
0
1
7;
5
2(3)
:242–250
245
Table1–SummaryofthedataregardingtheresultsofPSIstudies.
Study Studytype PSIsystem NumberofTKAs Results Outcomes
Abdeletal.4 RCT 20PSI Nodifferenceinearlyfunctional,
quality-of-lifeorgaitoutcomes.
Functionalevaluation
20SI Barkeetal.22 Retrospective Visionaire®(Smith&
Nephew)
39PSI SIachievedaMAclosertoneutral.OT wasequivalent.
MA,OT
50SI
Barracketal.17 Retrospective Signature®(Biomet) 100PSI EquivalentMAaccuracy,decreasedOT andreducednumberofinstrumenttrays withPSI.
MA,OT,numberof instrumenttrays
100SI Barretetal.23 Prospective
non-RCT
TruMatch®(DePuy) 66PSI ComparableMAandOTbetweengroups. MA,OT
86SI
Boonenetal.14 RCT Signature®(Biomet) 90PSI EquivalentMA,sagittalandcoronal alignmentoffemurandtibia.PSI decreasedOTby5min.
MA,CFC,CTC,SFC,STC,OT
90SI Chareancholvanichetal.11 RCT Patient-Specific
Instruments® (Zimmer)
40PSI NodifferenceinMA.Improvedaccuracy inCTC(89.8±1.2vs90.5±1.9,p=0.030) andfeweroutliersinSFCwithPSI (p=0.012).PSIdecreasedOTby5min.
MA,CFC,CTC,SFC,OT
40SI Daniilidisetal.6 Retrospective Visionaire®(Smith&
Nephew)
150PSI MAequivalent,withfeweroutlierswith PSI(9.3%vs.21.2%).
MA
156SI
Hamiltonetal.15 RCT TruMatch®(DePuy) 26PSI NodifferenceinMA,CFC,CTCandSFC withPSI.IncreasedposteriorslopeinSI (p<0.001).PSIrequiredfewerinstrument traysbutitwas4minlonger.
MA,CFC,CTC,SFC,STC,OT, numberofinstrumenttrays
26SI Heyseetal.7 Retrospective Visionaire®(Smith&
Nephew)
46PSI ReducedrateofFCRoutliersinPSIgroup comparedtoSI(2.2%vs22.9%,p=0.003).
FCR
48SI Ivieetal.19 Retrospective iTotal®G2
(ConforMIS)
100PSI MAandCFCmoreaccuratewithPSI,with feweroutliers(p=0.0016andp=0.032, respectively).NodifferenceinCTCandin sagittalalignmentbetweenthetwo groups.Nochangeswererequired.
MA,CFC,CTC,SFC,STC, needforapplyingchanges
100SI
Kotelaetal.24 RCT Signature®(Biomet) 49PSI CTCshowedmoreoutliersinPSIgroup (38.78%vs19.57%,p=0.0458).
MA,CFCCTC,SFC,STC
246
r
e
v
b
r
a
s
o
r
t
o
p
.
2
0
1
7;
5
2(3)
:242–250
Table1–(Continued)
Study Studytype PSIsystem NumberofTKAs Results Outcomes
Marimuthetal.10 Retrospective Visionaire®(Smith& Nephew)
115PSI Nodifferencesintheevaluated parameters.Similarnumberofoutliers.
MA,CFC,CTC,SFC,STC, FCR
185SI
Ngetal.2 Retrospective Signature®(Biomet) 105PSI OverallMAsimilar,butfeweroutliers withPSI(9%vs22%,p=0.018);CFC(90.7 vs91.3,p<0.001)andCTC(89.9vs90.4,
p=0.005)closertoneutralinPSIgroup comparedtoSI.
MA,CFC,CTC
55SI Nobleetal.12 RCT Visionaire®(Smith&
Nephew)
15PSI MAclosertoneutralwithPSI(1.7vs2.8,
p=0.03).PSIshowedreductioninOT (7min)andnumberofinstrumenttrays needed.
MA,CFC,CTC,OT,number ofinstrumenttrays
14SI
Nunleyetal.16 Retrospective Signature®(Biomet) 57PSI Equivalentnumbersofoutlierswith respecttoMA.DecreasedOTby12min afterPSI.
MA,OT
57SI
Nunleyetal.21 Retrospective Signature®(Biomet) 50PSI Equivalentnumbersofoutlierswith respecttoMA.
MA
50SI Rensonetal.20 Prospectivecase
series
Signature®(Biomet) 71PSI FeweroutliersinMAwithPSIcompared toSI(13%vs29%,p=0.043).DecreasedOT timeby9minandthenumberof instrumenttraysbysixtrayswithPSI.
MA,CFC,CTC,SFC,STC,OT, numberofinstrumenttrays
60SI
Rohetal.9 RCT Signature®(Biomet) 42PSI Nodifferencegroupswithrespecttoall evaluatedparameters.Equivalentnumber ofoutliers.OTwas13minlongerwithPSI andPSIhadtobeabortedin16%ofknees.
MA,CFC,CTC,SFC,STC, FCR,OT,needforapplying changes
48SI Silvaetal.18 Prospective
randomized
Signature®(Biomet) 23PSI NosignificantdifferenceinFCRandTCR betweengroups,butlessdispersionand amplitudeofTCRaroundtheneutral positionwithPSI.
FCR,TCR
22SI
Stronachetal.25 Retrospective Signature®(Biomet) 58PSI NoimprovementinalignmentwithPSI. Worseningofaccuracyofthetibialslope withPSI(38%vs61%,p=0.01).Equivalent OT.
MA,CFC,CTC,SFC,STC,OT
r
e
v
b
r
a
s
o
r
t
o
p
.
2
0
1
7;
5
2(3)
:242–250
247
Table1–(Continued)
Study Studytype PSIsystem NumberofTKAs Results Outcomes
Stronachetal.26 Retrospective Signature®(Biomet) 66PSI EquivalentOTbutmultiplechanges requiredintraoperativelywithPSI (2.4changes/knee).
OT,needforapplying changes
62SI Tibeskuetal.13 Activity-based
costingmodel
Visionaire®(Smith& Nephew)
IncreasedefficacyinOTandutilizationof instrumenttrayswithPSI.PSIis economicallyeffective.
OT,numberofinstrument trays
Victoretal.1 RCT Signature®(Biomet) 61PSI NosignificantdifferencesbetweenPSI andSIwithrespecttocomponent alignment.PSIhadmoreoutliersthanSI inCTC(14.6%vs3.1%,p=0.03)andSTC (21.3%vs3.1%,p=0.002).Visionaire® subgrouphadmoreoverallcoronal alignmentoutliers(p=0.04)butfewerSFC outliers(p=0.001).PSIwasabandonedin 22%ofpatientsandmodifiedin28%of patients.
MA,CFC,CTC,SFC,STC, FCR,needforapplying changes
TruMatch®(DePuy) 64SI Visionaire®(Smith&
Nephew) Patient-Specific Instruments® (Zimmer)
Vundelinckxetal.3 RCT Visionaire®(Smith& Nephew)
31PSI EquivalentMA.ImprovedSTCwithPSI (2.9±2.39vs5.0±2.14,p=0.0008).No differenceinpain,patientsatisfaction,or functionaloutcomes(KOOS,Lysholm score).
MA,STC,functional evaluation
31SI
Woolsonetal.8 RCT TruMatch®(DePuy) 22PSI IncreasednumberofoutliersinPSIgroup withrespecttotibialslope(32%vs8%,
p=0.032).Nosignificantdifferencewith regardtoOTorKneeSocietyratingor functionscore.
MA,CFC,CTC,STC,FCR, OT,functionalevaluation
26SI Yaffeetal.5 Retrospective Patient-Specific
Instruments® (Zimmer)
44PSI NodifferenceinMA,SFCorSTC.No differenceinpain,motion,KneeSociety kneescores;PSIhadhigherKneeSociety functionscorespre-andpostoperatively
MA,SFC,STC,functional evaluation
40SI
248
rev bras ortop.2017;52(3):242–250Cost-effectiveness
Another source of conflict associated with the
implemen-tation of PSI is whether this technique will reveal itself cost-effectiveornot.ConsideringitwasconsensualthatPSI
iscomparabletoSI,equivalentoutcomeswithmore
expen-sivetechnologydonotfitintothecurrentcost-effectiveness paradigm.Multiplefactorsplayasubstantialroleintheoverall efficiencyandeconomicsofTKA.Theadvantagesclaimedby supportersofPSIinthesurgerytime,thenumberof
instru-ment trays used and the need for applying changes may
supportacumulativedecreaseinresourceuse.Currently,TKA representsalargeexpenseinthehealthbudgetandany reduc-tionintheexpensesitcarriesisofparticularinterestinrespect tothepresenthealtheconomicclimate.
Operative
time
DecreasedsurgicaltimewithPSIhasbeendescribed,allowing increasedoverallprocedureefficiencyandcost-effectiveness ofTKA.Still,itwasnotunanimouslyobserved.
ThereareavailabledatafromRCTssupportingareduction
ofthe operatingtimeusingPSIsystem. Chareancholvanich
etal.11randomized80patientstoundergoTKAwithPSIorSI
andreportedthatthisnewtechnologyreducedskin-to-skin operativetimebyamean5.1min(p=0.019).Additionally, com-parableresultswerereportedbyBoonenetal.,14havingthePSI
surgerytaken5minlessthantheprocedurewithSI(p<0.001) andNobleetal.12(PSItook6.7minless;p=0.048).Also
Ren-sonetal.,20inaprospectivestudy,showedthetimeofsurgery
woulddecreasewithPSI.
Usinganactivity-basedcostmodel,Tibeskuetal.13found
thatPSIcuttingblocksallowedamoreefficientuseoftime intheoperatingroom,leadingtoincreasedrevenuesforthe hospital.Theauthorsobservedadecreaseof10minincutting timeand20mininthepreparationoftheoperatingroom,per procedure.Theexplanationisgivenbytheuseoftheimplant guideasawaytoreducetimefordeterminationofthesize oftheimplantduringaprocedure.Byallowingthesurgeries toendearlier,theauthorsassumeitwouldenablethe hos-pitaltocarryoutadditionalprocedures.Moreover,the cost savingswasmatchedwiththeadditionalcostassociatedwith thenewtechnology.Theoverallcostswerealmostidentical, withPSIcostingjust59D more,indicatinghowthe
theoreti-calincreasedefficiencyoftheprocedureconductedwithPSI mayoffsetitsextracosts,especiallyaftersurgeonsgainmore experience.
Onthecontrary,afterhavingperformedafinancialanalysis incorporatingthecostofpreoperativeimagingandthecutting guide,aswellassparedoperatingroomtimeandinstrument processing,Barracketal.17showedthatPSIwasactuallymore
expensive than SI. As a resultof diminished surgerytime
and sterilization costs,a totalsavingof$322per casewas reportedwiththeuse ofPSI.Nonetheless, thecustom cut-tingguidewasestimatedtocost$950andpreoperativeMRI waspredictedtovaryfrom$400to$1250,basedoninsurance.
Itwasconcludedthatanysavingsbornebyoperatingroom
timegainedandinstrumentprocessingwereoverwhelmedby
theoverheadcostsdemandedbyPSI.AlsothreeRCTsfailedto showdecreasedoperativetimewithPSI.Theprimaryoutcome measuredbyHamiltoneParks15wastotalsurgicaltime
cal-culatedfrominitialskinincisiontoendofclosure.52patients wererandomizedtoeitherPSIorconventionalTKA.Whilethe PSIgrouptookanaverageof61:47min,themeantimeforSI groupwas57:27min(p=0.006),withthemostofthetime dif-ferenceoccurringduringfemoralpreparation.Similarly,Roh et al.9counted59.4minforPSIcomparedto46.6minforSI
(p<0.001).Atlast,Woolsonetal.8alsofailedtoshowany
differ-encebetweengroups.Comparableresultswerealsoobserved byotherauthors.22,25,26
Number
of
instrument
trays
PSI isalsoexpectedtodecreasethe number of
instrumen-tation trays used, given the abolition of steps such as IM alignmentguideplacement.Thecostsassociatedwith main-tenance,storageandsterilizationcouldpotentiallydecrease after fewer trays are needed to be opened. Noble et al.12
recorded the number of instrument trays opened for each
caseanddemonstratedasignificantreductioninthenumber ofinstrumenttraysused(mean4.3vsmean7.5;p<0.0001). Similarly,HamiltoneParks.15reportedasignificantlyhigher
numberofsurgicalinstrumenttraysusedintheSIcases, com-paredwiththetraysrequiredforthePSI(mean7.3vsmean 2.5;p<0.001).Additionalauthorsanalyzedthissamevariable andunanimouslysupportedtheclaimthatPSIdoesresultina decreasednumberofinstrumenttrays.16,17,20Tibeskuetal.13
intheiractivity-basedcostinganalysis,observedthatPSIledto utilizationof4traysless,whichwasestimatedtocorrespond to1400trayslessannually,comparedtoSI.Thisdecreasewas anticipatedtoresultinpotentialcostsavingsof160Dper
pro-cedure.
Need
for
applying
changes
OneofthetheoreticaladvantagesofPSIisdecreasedoperative timethroughminimizationofintraoperativedecisionmaking
andinstrumenthandling.Numerouspreoperativestepsmust
becompletedmeticulouslyfortheresultantguidestobe pre-cise.Theaccuracyofthepreoperativeplanaccompanyingthe PSIwasalsocalledintoquestionbydifferentauthors.
Recently,Ivieetal.,19inaretrospectivestudy,reportedall
thesurgeriestohaveproceededwithoutrequiringadditional surgeoninterventionorachangefromthepreoperative surgi-calplan,notbeingnecessaryanyconversiontoconventional TKA. This is in contrast to other investigations that have
shown frequent surgeon-directed changes during PSITKA.
According toVictoret al.,1 inarandomizedstudy withthe
inclusion offour different PSI systems, the custom
instru-mentsprocedure hadtobemodifiedin28%ofthepatients
and abandonedinmorethan 20%.Themostcommon
rea-son for modifyingthe use ofthe PSI was the necessityto
changethesize.AlsoRohetal.9soughttoevaluatethe
reli-ability ofPSI by intraoperatively investigatingwhether the surgerycouldbecompletedwithPSIalone.Actually,in8knees (16%),theprocedurecouldnotaccuratelybecompletedand
rev bras ortop.2017;52(3):242–250
249
Stronachetal.26showedthatonly23%ofthefemoraland47%
ofthetibialimplantedcomponentsizewasproperlypredicted byPSI.
Postoperative
functional
evaluation
Itisnoticeablealackofpublishedstudiesonthefunctional resultsandgaitparametersofpatientsthathaveundergone PSITKA.Especiallyafterthepopularizationofminimally inva-sivesurgicaltechniques,eventhoughlong-termsurvivorship ispertinent,early painreliefand improvedfunctional
out-comeshavebecomeincreasinglyimportanttopatientsand
surgeons.Itremains unknownwhetherPSI improves
func-tion and pain-related outcomes and gait. For that reason,
someauthorsdecidedtoappropriatelymeasurethese param-eters,inordertodeterminewhethertheycouldpotentiallybe improvedwithPSI.
Four ofthe selected studies addressed these questions,
resulting in conclusions substantially consensual.
Vun-delinckxet al.3 conducted a study with a mean follow-up
oflittlemorethan6months,randomizing62 patients,and reportedthatPSIdonotconferanyfunctiongainscompared tothetraditionalTKA.ThePSIdidnotshowitselfofgreater valuewithrespecttopostoperativepain(measuredusingthe visualanalogscale),patientsatisfaction,functionaloutcome,
basedonLysholmscoreand KneeinjuryandOsteoarthritis
OutcomeScore(KOOS),andgaitparameters.
Similarly,Abdel et al.4 performeda randomizedclinical
trialwith40 patients, evaluatingsubjective andobjectively
functionalandgaitoutcomes,preoperativelyand3months
postoperatively,usingpatient-reportedoutcomescores(new KneeSocietyScore(KSS),KOOSandSF-12)andgait parame-ters.At3monthspostoperatively,almostallfunctionalscores wereincreasedinbothgroupscomparedwithpreoperatively. However,therewere nostatisticalsignificantdifferences in postoperativefunctionalscoresbetweengroupsandthesame
occurred concerning the analyzed gait parameters. Hence,
theauthorsagreedthatnobenefitinpainorearlyfunction
and nocomparative improvementin gaitparameters were
conferredbyPSIwhencomparedwithconventionalTKA,as
assessedbytheKSS,KOOSandSF-12andcomprehensivegait analysis.
Yaffeetal.5alsofailedtoshowadifferenceinKSSorpain
scoreimprovementbetweenPSIandconventionaljigs,aftera 6monthfollow-upof122patients.Still,PSIdidshowa
signif-icantlyhigherKneeSocietyfunctionsubscoreimprovement
from thepreoperativeperiodtothe 6-monthpostoperative
period, when compared to conventional instrumentation.
Enhancedcomponentrotationandpositioningandimproved
component size accuracy may be the explanation for the
results.However,asthisisaretrospectivecase-controlstudy,
there was not randomization of the patients, introducing
potentialbias. Infact, PSI group hadhigher preoperatively
knee scores, function scores and pain scores than
man-ual instrumentationgroup. Consequently, firm conclusions
fromthis findingremain elusiveduetotheaffected ability ofthe authors todrawdefinitiveconclusionsfrom the raw postoperativelyscores,eventhoughthegroupsaresimilarin bodymassindex,gender,ageandpreoperativediagnosis.
Morerecently,Woolsonetal.,8inaRCT,reportedno
signif-icantdifferencewithregardtoKneeSocietyratingorfunction score.
Discussion
In order to gain acceptance into modern practice, new
technology must demonstrate either (1) increased efficacy
comparedtoexistingtechnologyor(2)equivalentoutcomes withreducedcost.
On the basis of their data, some authors showed
results that sustain of the value of customized cutting
blocks.2,7,12,13,19,20 Onecan expectthat this technologywill
assistinrestoringthemechanicalaxiswithaccuracy poten-tiallybetterthanconventionalinstrumentation.Infact,allthe selectedstudiesshowednoinferiormechanicalandfemoral
component alignment withPSI. Onlythe tibial component
revealedcontroversialresults.
However,differentexampleshaveshowndeficientguide
fit intraoperatively in which conventional instrumentation
was preferred rather than accepting the potential risk of
anundesirableresection.1,9,26Thispresurgicalprocessadds
complexity,time,expense,andmultiplestepstotheTKA pro-cess.Anerrormadeintheinitialstepsoftheprocesswilllead tocontinuedreproductionofthaterror.Thisraisesaconcern thatthepreoperativelyproposedimplantsizeandalignment fromPSImaynotbeanaccuratereflectionofpatientanatomy and,therefore,unreliable.Surgeonsmustbecautiousagainst
blind approval of PSI technology without supportive data.
Additionally, some authors claim that more intraoperative
decision-makingwasrequiredbyPSI,preventingittoreduce operativetime.9,15Accordingly,nodifferenceinsurgerytime
between thegroups wasestablished.This mayresultfrom
additionaltimetakentoevaluateeachstep,regularlyrepeated resectionsandrejectedblindacceptanceoftheproposedcuts, preventingtheauthorsfromimmediatelymakethecutsafter placingthesurgicalguides,whichcouldcompromisethe accu-racyofthecomponentssizeandposition.Nonethelessseveral authorsbelievethePSIcuttingjigstoachievelargerprogresses insurgerytimewithmoreexperience,asthestudieswereled duringtheearlylearningcurveforhigh-volumesurgeonswho haveperformedseveralthousandTKAsusingSI.1,2,16Lackof
expertisewiththePSImaybeenoughtobiastheresults. Sur-geonsareexpectedtoimprovethetechniqueandbeableto makefeweradjustments,reducingthesurgicaltimewithPSI, asthevolumeofperformancesincreases.
Final
remarks
Thevalueofanymedicaltechnologydependsonwhetheror
notitimprovesclinicaloutcomesandPSIoffersnumerous the-oreticaladvantagesthatmakeitanattractivealternativefor TKA.Asthistechnologystillremainsarelativelynewconcept, itisnotsurprisingthat,despiteitsincrease,thebodyof liter-atureremainslimited.Regardlessofwhetherthistechnology isfoundtobeacceptableinthefuture,thetruthisthat dif-ferent studiesassumedbothtechniquesare abletorestore
limbalignment andplace thecomponents withequivalent
250
rev bras ortop.2017;52(3):242–250supportthisinnovativetechnique, PSIhasnotconsistently beenshowntobecost-effectiveortoofferanyclinical ben-efitwithregardtofunctionalscoresassessed.Theextensive numberofanglesthatcanbemeasuredtoevaluatetheefficacy ofPSIalsomakesthecomparisonbetweendifferentstudies difficult.Additionally,ispossiblethatasix-monthfollow-up periodmaynotbesensitiveenoughtodetectPSI’seffecton
functionaloutcomesandcomponentsurvivorship.
PSImayhaveasmallandspecificroleincertaincases,such aswhentheuseofanIMorextra-medullaryrodwithmounted cuttingblock is impossible,for example after severe post-traumaticsequelsofdistalfemoralorproximaltibialfractures orforpatientswithIMhardwareorextra-articulardeformities, butadditionaljustifyingdataisvitalprioritsroutineuse.
Itispossiblethatmorepreciseconclusionsmayemerge.
Thatbeingsaid,additionalRCTsshouldbeconducted
com-paringtheclinicaloutcomesofPSItothetraditionaltechnique
with a longer postoperative follow-up period and a larger
samplebefore definitive conclusionsare made, concerning
functionalefficacyofthistechnologyandthepotential appli-cabilityofPSItospecialsituations.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. VictorJ,DujardinJ,VandenneuckerH,ArnoutN,BellemansJ.
Patient-specificguidesdonotimproveaccuracyintotalknee
arthroplasty:aprospectiverandomizedcontrolledtrial.Clin
OrthopRelatRes.2014;472(1):263–71.
2. NgVY,DeClaireJH,BerendKR,GulickBC,LombardiAVJr.
Improvedaccuracyofalignmentwithpatient-specific
positioningguidescomparedwithmanualinstrumentation
inTKA.ClinOrthopRelatRes.2012;470(1):99–107.
3. VundelinckxBJ,BruckersL,DeMulderK,DeSchepperJ,Van
EsbroeckG.Functionalandradiographicshort-termoutcome
evaluationoftheVisionairesystem,apatient-matched
instrumentationsystemfortotalkneearthroplasty.J
Arthroplasty.2013;28(6):964–70.
4. AbdelMP,ParratteS,BlancG,OllivierM,PomeroV,Viehweger
E,etal.Nobenefitofpatient-specificinstrumentationinTKA
onfunctionalandgaitoutcomes:arandomizedclinicaltrial.
ClinOrthopRelatRes.2014;472(8):2468–76.
5. YaffeM,LuoM,GoyalN,ChanP,PatelA,CayoM,etal.
Clinical,functional,andradiographicoutcomesfollowing
totalkneearthroplastywithpatient-specificinstrumentation,
computer-assistedsurgery,andmanualinstrumentation:a
short-termfollow-upstudy.IntJComputAssistRadiolSurg.
2014;9(5):837–44.
6. DaniilidisK,TibeskuCO.Acomparisonofconventionaland
patient-specificinstrumentsintotalkneearthroplasty.Int
Orthop.2014;38(3):503–8.
7. HeyseTJ,TibeskuCO.Improvedfemoralcomponentrotation
inTKAusingpatient-specificinstrumentation.Knee.
2014;21(1):268–71.
8. WoolsonST,HarrisAH,WagnerDW,GioriNJ.Component
alignmentduringtotalkneearthroplastywithuseofstandard
orcustominstrumentation:arandomizedclinicaltrialusing
computedtomographyforpostoperativealignment
measurement.JBoneJointSurgAm.2014;96(5):366–72.
9.RohYW,KimTW,LeeS,SeongSC,LeeMC.IsTKAusing
patient-specificinstrumentscomparabletoconventional
TKA?Arandomizedcontrolledstudyofonesystem.Clin
OrthopRelatRes.2013;471(12):3988–95.
10.MarimuthuK,ChenDB,HarrisIA,WheatleyE,BryantCJ,
MacDessiSJ.Amulti-planarCT-basedcomparativeanalysisof
patient-specificcuttingguideswithconventional
instrumentationintotalkneearthroplasty.JArthroplasty.
2014;29(6):1138–42.
11.ChareancholvanichK,NarkbunnamR,
PornrattanamaneewongC.Aprospectiverandomised
controlledstudyofpatient-specificcuttingguidescompared
withconventionalinstrumentationintotalknee
replacement.BoneJointJ.2013;95-B(3):354–9.
12.NobleJWJr,MooreCA,LiuN.Thevalueofpatient-matched
instrumentationintotalkneearthroplasty.JArthroplasty.
2012;27(1):153–5.
13.TibeskuCO,HoferP,PortegiesW,RuysCJ,FennemaP.Benefits
ofusingcustomizedinstrumentationintotalknee
arthroplasty:resultsfromanactivity-basedcostingmodel.
ArchOrthopTraumaSurg.2013;133(3):405–11.
14.BoonenB,SchotanusMG,KerensB,vanderWeegenW,van
DrumptRA,KortNP.Intra-operativeresultsandradiological
outcomeofconventionalandpatient-specificsurgeryintotal
kneearthroplasty:amulticentre,randomizedcontrolledtrial.
KneeSurgSportsTraumatolArthrosc.2013;21(10):2206–12.
15.HamiltonWG,ParksNL.Patient-specificinstrumentation
doesnotshortensurgicaltime:aprospective,randomized
trial.JArthroplasty.2014;29(7):1508–9.
16.NunleyRM,EllisonBS,RuhEL,WilliamsBM,ForemanK,Ford
AD,etal.Arepatient-specificcuttingblockscost-effectivefor
totalkneearthroplasty?ClinOrthopRelatRes.
2012;470(3):889–94.
17.BarrackRL,RuhEL,WilliamsBM,FordAD,ForemanK,Nunley
RM.Patientspecificcuttingblocksarecurrentlyofnoproven
value.JBoneJointSurgBr.2012;9411(Suppl.A):95–9.
18.SilvaA,SampaioR,PintoE.Patient-specificinstrumentation
improvestibialcomponentrotationinTKA.KneeSurgSports
TraumatolArthrosc.2014;22(3):636–42.
19.IvieCB,ProbstPJ,BalAK,StannardJT,CristBD,SonnyBalB.
Improvedradiographicoutcomeswithpatient-specifictotal
kneearthroplasty.JArthroplasty.2014;29(11):2100–3.
20.RensonL,PoilvacheP,VandenWyngaertH.Improved
alignmentandoperatingroomefficiencywithpatient-specific
instrumentationforTKA.Knee.2014;21(6):1216–20.
21.NunleyRM,EllisonBS,ZhuJ,RuhEL,HowellSM,BarrackRL.
Dopatient-specificguidesimprovecoronalalignmentintotal
kneearthroplasty?ClinOrthopRelatRes.2012;470(3):895–902.
22.BarkeS,MusanhuE,BuschC,StaffordG,FieldR.
Patient-matchedtotalkneearthroplasty:doesitofferany
clinicaladvantages?ActaOrthopBelg.2013;79(3):307–11.
23.BarrettW,HoeffelD,DaluryD,MasonJBB,MurphyJ,Himden
S.In-vivoalignmentcomparingpatientspecific
instrumentationwithbothconventionalandcomputer
assistedsurgery(CAS)instrumentationintotalknee
arthroplasty.JArthroplasty.2014;29(2):343–7.
24.KotelaA,KotelaI.Patient-specificcomputedtomography
basedinstrumentationintotalkneearthroplasty:a
prospectiverandomizedcontrolledstudy.IntOrthop.
2014;38(10):2099–107.
25.StronachBM,PeltCE,EricksonJA,PetersCL.Patient-specific
instrumentationintotalkneearthroplastyprovidesno
improvementincomponentalignment.JArthroplasty.
2014;29(9):1705–8.
26.StronachBM,PeltCE,EricksonJ,PetersCL.Patient-specific
totalkneearthroplastyrequiredfrequentsurgeon-directed