Artigo Original
Bianca Simone Zeigelboim1 Hélio Afonso Ghizoni Teive2 Rosane Sampaio Santos1 Walter Oleschko Arruda2 Ari Leon Jurkiewicz1 Heidi Mengelberg1 Denise França3 Jair Mendes Marques1
Descritores
Degenerações espinocerebelares Ataxias espinocerebelares Ataxia Audição Transtornos da audição Audiometria de resposta evocada Audiometria Potenciais evocados auditivos
Keywords
Spinocerebellar degenerations Spinocerebellar ataxias Ataxia Hearing Hearing disorders Audiometry, evoked response Audiometry Evoked potentials, auditory
Correspondence address: Bianca Simone Zeigelboim
R. Gutenberg, 99, 9º andar, Curitiba (PR), Brasil, CEP: 80420-030.
E-mail: [email protected] Received: 05/03/2012
Study carried out at the Universidade Tuiuti do Paraná – UTP – Curitiba (PR), Brazil. (1) Universidade Tuiuti do Paraná – UTP – Curitiba (PR), Brazil.
(2) Universidade Federal do Paraná – UFPR – Curitiba (PR), Brazil.
(3) Universidade do Centro-Oeste do Paraná – UNICENTRO – Irati (PR), Brazil. Conlict of interest: nothing to declare.
Avaliação audiológica na ataxia espinocerebelar
ABSTRACT
Purpose: To describe the audiological and electrophysiological results in patients with spinocerebellar ataxia (SCA). Methods: Retrospective and cross-sectional studies were performed. Forty-three patients were assessed using the following procedures: anamnesis and otolaryngologic exam, pure tone audiometry, acoustic immittance measures and brainstem auditory evoked potential (BAEP). Results: Patients showed gait abnormality (83.7%), speech disorder (48.8%), dizziness (41.8%) and dysphagia (39.5%). Hearing loss was referred in 27.9% of the cases; in the audiometric exams, 14 patients (32.5%) presented disorders; in SCA 3, 33.3%; in SCA 2, 12.5%; in SCA 4, 100.0%; in SCA 6, 100.0%; in SCA 7, 100.0%; in SCA 10, 50.0%; and in undetermined SCA, 21.4%. In BAEP, 20 patients (46.5%) were abnormal, being 58.3% in SCA 3, 62.5% in SCA 2, 100.0% in SCA 6, 100.0% in SCA 7, 66.7% in SCA 10 and 14.2% in undetermined SCA. While in acoustic immittance, 19 patients (44.1%) presented disorders, being 50.0% in SCA 3, 50.0% in SCA 2, 100.0% in SCA 4, 100.0% in SCA 6, 100.0% in SCA 7, 33.3% in SCA 10 and 28.5% in undetermined SCA. Conclusion: The most evident abnormalities in the audiological evaluation were the predominance of the down-sloping audiometric coniguration beginning at 4 kHz bilaterally and the bilateral absence of acoustic relex at the frequencies of 3 and 4 kHz. In the electrophysiological evaluation, 50% of the patients showed abnormalities with prevalence of an increase of the latency of waves I, II and V and of the interval in the interpeaks I-III, I-V and III-V.
RESUMO
INTRODUCTION
Spinocerebellar ataxia (SCA) is a disease that belongs to a heterogeneous group of neurodegenerative disorders that are characterized by the presence of progressive cerebellar ataxia(1). It can be classiied as sensitive, frontal, vestibular, and
cerebellar, with the latter being the object of this study(1). Out
of the 30 types of identiied SCAs, Types 2 and 3 are among the most prevalent(1,2).
There are about 3.0 to 4.2 cases of SCAs per 100,000,0 inhabitants(3), and the most common clinical manifestations are
gait and appendicular ataxia (dysmetria, dysdiadochokinesia, and intention tremor), dysarthria, nystagmus, ophthalmople-gia, dysphaophthalmople-gia, hearing loss (in some cases), pyramidal signs, lower motor neuron syndrome, cognitive dysfunction, epilepsy, visual disorders (retinitis pigmentosa), peripheral neuropathy, dementia, and movement disorders (including Parkinson’s, dystonia, myoclonus, and chorea)(1,3-5).
SCAs can be divided according to genetic inheritance: (a) autosomal recessive hereditary ataxia, (b) autosomal dominant hereditary ataxia, (c) hereditary ataxia related to the x chromo-some, and (d) mitochondrial hereditary ataxia(6).
Studies describe differences in the severity of clinical manifestations and the age of onset of symptoms, depending on which parent the expanded gene is inherited from. In the case of SCAs transmitted from the father, an increasing trend was observed in the number of repetitions in children, which is different when SCAs are transmitted from the mother. Therefore, when an SCA is transmitted from the father, it means more severe clinical manifestations in the children, who can even present the irst symptoms of ataxia before the father(7).
In Brazil, especially in the South region, a great number of families have been detected to carry SCAs(3,6). The
Machado-Joseph disease (MJD), also known as SCA 3, is the most com-mon form of autosomal dominant hereditary ataxia found in a number of epidemiological studies(3,6-8).
The exploration of peripheral and central auditory system is conducted by using behavioral, electroacoustic, and electro-physiological assessment methods.
Many authors(9-11) report that in neurodegenerative diseases,
the most common auditory dysfunctions are observed in the brainstem auditory-evoked potential (BAEP) test and occur in the inferior colliculus, lateral lemniscus, and cochlear nuclei.
SCAs are part of a group of diseases that present important changes in the speech-language ield. Such research is a key contributor in building knowledge as a substitute for cumber-some and elongated assessment and therapeutic procedures focusing on this disease.
The objective of this study was to assess the results of au-diological and electrophysiological evaluations in SCA patients.
METHODS
This study was approved by the Institutional Ethics Committee (Number: 058/2008) and authorized by the
patients who conirmed their acceptance by signing the in-formed consent form.
A retrospective cross-sectional study was conducted. A total of 43 patients were evaluated (17 female and 26 male) and referred to the clinical department of Hospital das Clínicas, who were also assisted at the otoneurology department of a teaching institution in the same city. The study participants were diagnosed with SCA (twelve with SCA 3, eight with SCA 2, one with SCA 4, one with SCA 6, one with SCA 7, and six with SCA 10).
The diagnosis of ataxia was performed by a genetic test, us-ing the polymerase chain reaction (PCR)(12-14). Fourteen patients
were genetically analyzed to discover the type of SCA, who were also part of the group of people with undetermined SCA.
The age of patients ranged from 18.0 to 70.0 years (mean age: 41.6 years, SD=13.0 years). Duration of disease was 1.0 to 15.0 years (mean duration: 7.9 years, SD=3.9 years; Table 1).
Patients with alterations that prevented their participation in examinations were excluded from the study.
The following procedures were performed:
• Anamnesis: A questionnaire with emphasis on otoneuro -logical signs and symptoms was applied.
• Otolaryngologic evaluation: Evaluation was carried out
with the objective of excluding any alteration that could interfere with the examination.
• Audiological evaluation: Patients were submitted to
pure-tone air conduction audiometry at frequencies ranging from 250 to 8 kHz, bone conduction at frequencies ranging from 500 to 4 kHz, and tests of speech recognition threshold (SRT) as well as the percentage index of speech recogni-tion (PISR). For these tests, the equipment used was Itera Madsen-GN Otometrics, TDH-39 headphones, from GN-ReSound, with thresholds expressed in dBNA and calibrated according to the ISO 8253 standard(15,16).
• BAEP: Two channels with 90-dBnHL click stimuli, polarity
alternated with presentation frequency of 21.1 c/s, 15-ms window, 30- to 3-kHz ilter, and at least 2,000 stimuli and two reproduction registers were used. Electrodes from Kendall Medtrace 2000 were placed in the right and left mastoid positions as well as in Fz (10-20 system), and the earth electrode was placed on the forehead. Clicks were presented with 3A insert earphones. The latency of Waves I, III, and V and the Interpeak intervals I-III, III-V, and I-V were analyzed. The equipment used was the Bio-logic’s Evoked Potential System, and the analysis criterion was proposed by the author(17).
• Acoustic immittance measures: This procedure was per -formed to assess the integrity of the tympanic ossicles, and the equipment used for this purpose was the Otolex middle-ear analyzer, TDH 39P headphones, from Gn-ReSound, and the author’s criteria were applied(18).
Statistical analysis
acoustic immittance measure, by analyzing results indicating normalcy and abnormalcy. Rejection level in the null hypothesis was ixated at 0.05 or 5%.
RESULTS
The most frequently mentioned complaints in anamnesis (Table 2) were as follows: gait imbalance (83.7%), trouble speaking (48.8%), dizziness (41.8%), dysphagia (39.5%), dysphonia (34.8%), and hearing loss (27.9%).
During the audiological evaluation, 14 patients (32.5%) presented changes in the examination – 2.3% in the right ear
(RE), 4.6% in the left ear (LE), and 25.6% bilaterally (B) –
which translated to 33.3% in SCA 3, 12.5% in SCA 2, 100.0% in SCA 4, 100.0% in SCA 6, 100.0% in SCA 7, 50.0% in SCA 10, and 21.4% in undetermined SCA (Table 3).
The application of the difference-in-proportions test proved there was signiicant difference between normal and abnormal
cases – RE (p<0.05), LE (p<0.05), and B (p=0.0001*). The
results of SRT and PISR were compatible with tone thresholds.
Table 1. Genetic aspects of spinocerebellar ataxias
Patient Age
(years) Gender
Spinocerebellar ataxias
Duration of
disease (years) Chromosome Gene Mutation Protein
1 42 M SCA 3 12 14q32.1 ATAXIN3 CAG Ataxin3
2 48 F SCA 3 15 14q32.1 ATAXIN3 CAG Ataxin3
3 43 M SCA 3 12 14q32.1 ATAXIN3 CAG Ataxin3
4 41 M SCA 3 8 14q32.1 ATAXIN3 CAG Ataxin3
5 48 F SCA 3 10 14q32.1 ATAXIN3 CAG Ataxin3
6 53 M SCA 3 13 14q32.1 ATAXIN3 CAG Ataxin3
7 50 F SCA 3 8 14q32.1 ATAXIN3 CAG Ataxin3
8 30 F SCA 3 9 14q32.1 ATAXIN3 CAG Ataxin3
9 42 M SCA 3 10 14q32.1 ATAXIN3 CAG Ataxin3
10 45 M SCA 3 15 14q32.1 ATAXIN3 CAG Ataxin3
11 51 M SCA 3 7 14q32.1 ATAXIN3 CAG Ataxin3
12 45 M SCA 3 3 14q32.1 ATAXIN3 CAG Ataxin3
13 54 F SCA 2 11 12q24.1 ATAXIN2 CAG Ataxin2
14 38 M SCA 2 8 12q24.1 ATAXIN2 CAG Ataxin2
15 41 M SCA 2 12 12q24.1 ATAXIN2 CAG Ataxin2
16 36 M SCA 2 3 12q24.1 ATAXIN2 CAG Ataxin2
17 18 M SCA 2 2 12q24.1 ATAXIN2 CAG Ataxin2
18 44 F SCA 2 3 12q24.1 ATAXIN2 CAG Ataxin2
19 30 F SCA 2 10 12q24.1 ATAXIN2 CAG Ataxin2
20 42 M SCA 2 12 12q24.1 ATAXIN2 CAG Ataxin2
21 43 M SCA 4 5 16q24.qter SCA4 PLEKHG4? —
22 57 F SCA 6 5 19q13.1 CACNA1A CAG CACNA1A
23 47 F SCA 7 10 3p14.1 ATAXIN7 CAG Ataxin7
24 49 F SCA 10 6 22q13.3 ATAXIN10 ATTCT Ataxin10
25 46 M SCA 10 10 22q13.3 ATAXIN10 ATTCT Ataxin10
26 27 F SCA 10 3 22q13.3 ATAXIN10 ATTCT Ataxin10
27 70 M SCA 10 13 22q13.3 ATAXIN10 ATTCT Ataxin10
28 54 M SCA 10 11 22q13.3 ATAXIN10 ATTCT Ataxin10
29 56 F SCA 10 12 22q13.3 ATAXIN10 ATTCT Ataxin10
30 24 M Und. 2 — — — —
31 27 M Und. 7 — — — —
32 20 M Und. 1 — — — —
33 32 M Und. 5 — — — —
34 22 M Und. 8 — — — —
35 22 M Und. 7 — — — —
36 62 M Und. 3 — — — —
37 66 M Und. 12 — — — —
38 18 F Und. 4 — — — —
39 23 M Und. 1 — — — —
40 37 F Und. 9 — — — —
41 48 F Und. 8 — — — —
42 48 F Und. 8 — — — —
43 51 F Und. 7 — — — —
In BAEP, 20 patients (46.5%) presented changes in the
examinations (11.6% in the LE and 34.9% in B), which
translated to 58.3% in SCA 3, 62.5 in SCA 2, 100.0% in SCA 6, 100.0% in SCA 7, 66.7% in SCA 10, and 14.2% in undetermined SCA (Table 3).
The application of the difference-in-proportions test proved there was a signiicant difference between the
pro-portions of normal and abnormal cases – LE (p<0.05) and B (p=0.0063*).
In the acoustic immittance measure, 19 patients (44.1%) registered changes in the examinations, especially bilaterally, which translated to 50.0% in SCA 3, 50.0% in SCA 2, 100.0% in SCA 4, 100.0% in SCA 6, 100.0% in SCA 7, 33.3% in SCA 10, and 28.5% in undetermined SCA (Table 4).
The application of the difference-in-proportions test further proved there was no signiicant difference between the propor-tions of normal and abnormal cases – B (p=0.2843).
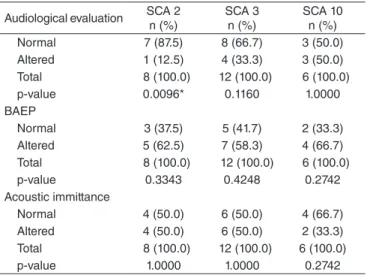
The results of audiological evaluation, BAEP, and acoustic immittance measure in relation to the proportions of normal and abnormal cases in SCAs 2, 3, and 10 are presented in Table 5.
The application of the difference-in-proportions test proved there was signiicant difference only in the audiological
evalu-ation and in SCA 2 (p=0.0096*).
DISCUSSION
Anamnesis revealed the predominance of gait disorders, which was expected in terms of SCA. Changes in speech, diz-ziness, dysphagia, dysphonia, and hearing loss are the most frequent symptoms as described in many past studies(1-4).
Changes in audiological evaluation were present in 30% of the patients with ataxia, especially those in the category of SCA 3 and SCA 10. The authors(19) assessed 18 patients with SCA and
observed normal hearing in all of them but found hearing changes using the BAEP test, with a 71% occurrence in Friedreich’s ataxia, in which only Wave I was found, and 71% in olivopontocerebellar atrophy, which does not refer to the type of alteration found. The authors pointed out to important abnormalities in the brainstem auditory pathways of patients with this disease.
In this study, 46.5% of patients presented alterations in BAEP, with increased Wave I latency only in SCA 3. An in-crease in Wave V latency was observed in SCAs 3, 6, 7, 10, and undetermined SCA; an increase in Wave III latency was observed in SCAs 2, 6, and 7; and an increase in Interpeak intervals I-III, I-V, and III-V occurred in SCAs 2, 3, 6, 7, 10, and the undetermined SCA. The authors(19-22) reported frequent
abnormalities in this examination. The prevalence of changes in SCAs 2 and 3 are in accordance with the authors(20,21), which is
due to higher prevalence of these types of SCA. Some studies(21)
have evaluated the BAEP test in 36 patients (eight with SCA 1, twelve with SCA 2, and sixteen with SCA 3) and observed re-sults indicating abnormalities in 50% of those with SCA 1, 42% with SCA 2, and 63% with SCA 3. Another group of research-ers(23) assessed 30 patients with spinocerebellar degeneration
and observed abnormalities in 30% of these patients after the BAEP test, with prolonged latencies and Interpeaks of waves I-III and I-V, which is in accordance with this study.
Some authors(24) conducted an anatomopathological
inves-tigation of brain in 12 patients with SCA (three with SCA 2, seven with SCA 3, and two with SCA 7), considering tissue cuts of auditory nuclei; they reported substantial damage to the central auditory system.
The study showed neural loss of the dorsal and ventral nuclei of the lateral lemniscus in two patients with SCA 2, in all of those with SCA 3, and in one patient with SCA 7. The superior olivary nucleus proved to be the most severely affected by degeneration, and the loss of myelinated ibers in brainstem pathways restricted to the lateral lemniscus was found in a patient with SCA 2, in ive patients with SCA 3, and in all of those with SCA 7. The trapezoid body was altered in a patient with SCA 2 and in two patients with SCAs 3 and 7. The involvement of these structures offered plausible explanations for the hearing damage observed in these patients.
Acoustic immittance measures were altered in 44.1% of these patients, and literature has no reference about this inding, so the results cannot be reconirmed. It is known that ibers leave from the anterior cochlear nuclei, via trapezoid body, and move toward the nuclei of the contralateral facial nerve and the superior olivary nucleus, which in turn forms synapses with the facial nerve nucleus. There are also homo-lateral ibers coming from the anterior cochlear nuclei, which establish such communications, and, in addition, axons inner-vate the stapedius muscle or the stapes. However, when there are multiple neurodegenerative diseases, the anterior cochlear nuclei are affected, which in turn renders impossible the task of making interferences in the acoustic relex mechanism(25,26).
Table 2. Frequency of symptoms in 43 patients with spinocerebellar ataxia
Symptoms Number of
patients
Frequency (%)
Gait imbalance 36 83.7
Trouble speaking 21 48.8
Dizziness 18 41.8
Dysphagia 17 39.5
Dysphonia 15 34.8
Hearing loss 12 27.9
Headache 11 25.5
Falling 11 25.5
Diplopia 10 23.2
Paresthesia in the extremities 7 16.2
Anxiety 6 13.9
Double vision 5 11.6
Tremor 5 11.6
Pain irradiated to the shoulder and arm 5 11.6
Insomnia 5 11.6
Depression 5 11.6
Pain and difficulty moving the neck 4 9.3
Migraine 4 9.3
Tinnitus 4 9.3
In the present study, a higher prevalence of alterations observed in the BAEP examination proved there were severe changes in the integrity of the brainstem auditory pathway. This inding is in accordance with many other research works(19-24), where the authors have observed
al-terations in many structures of the central auditory pathway,
demonstrating the greater sensitivity of this examination to detect changes in the path of acoustic impulse throughout the central auditory pathway.
The importance of studying the auditory system is empha-sized, especially in the context of electrophysiological control, together with clinical and genetic follow-ups.
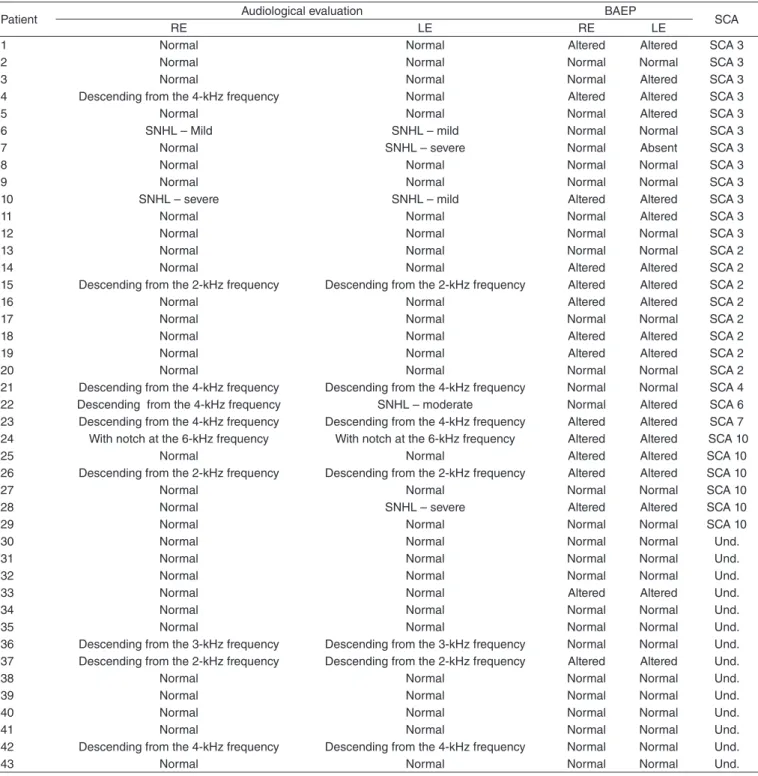
Table 3. Results of audiological and brainstem auditory-evoked potential evaluations in 43 patients with spinocerebellar ataxia
Patient Audiological evaluation BAEP SCA
RE LE RE LE
1 Normal Normal Altered Altered SCA 3
2 Normal Normal Normal Normal SCA 3
3 Normal Normal Normal Altered SCA 3
4 Descending from the 4-kHz frequency Normal Altered Altered SCA 3
5 Normal Normal Normal Altered SCA 3
6 SNHL – Mild SNHL – mild Normal Normal SCA 3
7 Normal SNHL – severe Normal Absent SCA 3
8 Normal Normal Normal Normal SCA 3
9 Normal Normal Normal Normal SCA 3
10 SNHL – severe SNHL – mild Altered Altered SCA 3
11 Normal Normal Normal Altered SCA 3
12 Normal Normal Normal Normal SCA 3
13 Normal Normal Normal Normal SCA 2
14 Normal Normal Altered Altered SCA 2
15 Descending from the 2-kHz frequency Descending from the 2-kHz frequency Altered Altered SCA 2
16 Normal Normal Altered Altered SCA 2
17 Normal Normal Normal Normal SCA 2
18 Normal Normal Altered Altered SCA 2
19 Normal Normal Altered Altered SCA 2
20 Normal Normal Normal Normal SCA 2
21 Descending from the 4-kHz frequency Descending from the 4-kHz frequency Normal Normal SCA 4
22 Descending from the 4-kHz frequency SNHL – moderate Normal Altered SCA 6
23 Descending from the 4-kHz frequency Descending from the 4-kHz frequency Altered Altered SCA 7 24 With notch at the 6-kHz frequency With notch at the 6-kHz frequency Altered Altered SCA 10
25 Normal Normal Altered Altered SCA 10
26 Descending from the 2-kHz frequency Descending from the 2-kHz frequency Altered Altered SCA 10
27 Normal Normal Normal Normal SCA 10
28 Normal SNHL – severe Altered Altered SCA 10
29 Normal Normal Normal Normal SCA 10
30 Normal Normal Normal Normal Und.
31 Normal Normal Normal Normal Und.
32 Normal Normal Normal Normal Und.
33 Normal Normal Altered Altered Und.
34 Normal Normal Normal Normal Und.
35 Normal Normal Normal Normal Und.
36 Descending from the 3-kHz frequency Descending from the 3-kHz frequency Normal Normal Und. 37 Descending from the 2-kHz frequency Descending from the 2-kHz frequency Altered Altered Und.
38 Normal Normal Normal Normal Und.
39 Normal Normal Normal Normal Und.
40 Normal Normal Normal Normal Und.
41 Normal Normal Normal Normal Und.
42 Descending from the 4-kHz frequency Descending from the 4-kHz frequency Normal Normal Und.
43 Normal Normal Normal Normal Und.
Legend: BAEP = brainstem auditory-evoked potential; SCA = spinocerebellar ataxia; RE = right ear; LE = left ear; SNHL = sensorineural hearing loss; Und = undetermined. The application of the difference-in-proportions test in audiological evaluation proves there was a significant difference between the proportion of normal and abnormal cases: RE (p<0.05), LE (p<0.05), and B (p=0.0001*)
CONCLUSION
The alterations that mostly appeared in the audiological evaluation include the prevalence of descending audiometric coniguration from the 4-kHz frequency, bilaterally, and the
absence of acoustic relex in 3- and 4-kHz frequencies, again bilaterally.
In the electrophysiological evaluation, 50% of the patients presented with changes, especially increased latencies in Waves I, III, and V and Interpeak intervals I-III, I-V, and III-V.
Table 4. Results of the immittance test in 43 patients with spinocerebellar ataxia
Patient
Acoustic immittance measure
SCA
RE LE
Tympanometric
curve Acoustic reflex
Tympanometric
curve Acoustic reflex
1 Type A Present Type A Present SCA 3
2 Type A Present Type A Present SCA 3
3 Type A Absent in the 4-kHz frequency Type A Absent SCA 3
4 Type A Absent in the 4-kHz frequency Type A Absent in the 4-kHz frequency SCA 3
5 Type A Absent in the 3- and 4-kHz frequencies Type A Absent in the 3- and 4-kHz frequencies SCA 3 6 Type A Absent in the 3- and 4-kHz frequencies Type A Absent in the 3- and 4-kHz frequencies SCA 3
7 Type A Absent in the 3- and 4-kHz frequencies Type A Absent SCA 3
8 Type A Present Type A Present SCA 3
9 Type A Present Type A Present SCA 3
10 Type A Absent Type A Absent in the 3- and 4-kHz frequencies SCA 3
11 Type A Present Type A Present SCA 3
12 Type A Present Type A Present SCA 3
13 Type A Present Type A Present SCA 2
14 Type As Absent Type As Absent SCA 2
15 Type A Absent in the 2-, 3-, and 4-kHz frequencies Type A Absent in the 2-, 3- and 4-kHz frequencies SCA 2 16 Type A Absent in the 3- and 4-kHz frequencies Type A Absent in the 3- and 4-kHz frequencies SCA 2 17 Type A Absent in the 3- and 4-kHz frequencies Type A Absent in the 3- and 4-kHz frequencies SCA 2
18 Type A Present Type A Present SCA 2
19 Type A Present Type A Present SCA 2
20 Type A Present Type A Present SCA 2
21 Type A Absent in the 4-kHz frequency Type A Absent in the 4-kHz frequency SCA 4
22 Type A Absent in the 4-kHz frequency Type A Absent SCA 6
23 Type A Absent in the 4-kHz frequency Type Ad Absent SCA 7
24 Type A Present Type A Present SCA 10
25 Type A Present Type A Present SCA 10
26 Type As Absent in the 3- and 4-kHz frequencies Type As Absent in the 3- and 4-kHz frequencies SCA 10
27 Type A Present Type A Present SCA 10
28 Type A Absent in the 3- and 4-kHz frequencies Type As Absent SCA 10
29 Type A Present Type A Present SCA 10
30 Type A Present Type A Present Und.
31 Type A Present Type A Present Und.
32 Type A Present Type A Present Und.
33 Type A Absent in the 3- and 4-kHz frequencies Type A Absent in the 3- and 4-kHz frequencies Und.
34 Type A Present Type A Present Und.
35 Type A Present Type A Present Und.
36 Type A Absent in the 3- and 4-kHz frequencies Type A Absent in the 3- and 4-kHz frequencies Und. 37 Type A Absent in the 3- and 4-kHz frequencies Type A Absent in the 3- and 4-kHz frequencies Und.
38 Type A Present Type A Present Und.
39 Type A Present Type A Present Und.
40 Type A Present Type A Present Und.
41 Type A Present Type A Present Und.
42 Type A Absent in the 4-kHz frequency Type A Absent in the 4-kHz frequency Und.
43 Type A Present Type A Present Und.
Legend: RE = right ear; LE = left ear; SCA = spinocerebellar ataxia; Und. = Undetermined.
ACKNOWLEDGEMENT
National Council for Scientific and Technological Development (CNPQ), Report n. 309965/2009-8.
*WOA collaborated with data collection and formatting; RSS collaborated with collection and bibliography; DF collaborated with collection and bibliography; HM collaborated with collection and bibliography; JMM collaborated with data analysis; HGAT was in charge of writing and inal review; ALI participated in the writing and inal review; BSZ was in charge of the project and study design as well as general orientation of the stages of execution and elaboration of the manuscript.
REFERENCES
1. Te ive H AG . S p i n o c e r e b e l l a r a t a x i a . A r q N e u r o p s i q u i a t r. 2009:67(4):1133-42.
2. Rüb U, Brunt ER, Deller T. New insights into the pathoanatomy of spinocerebellar ataxia type 3 (Machado-Joseph disease). Curr Opin Neurol. 2008;21:111-6.
3. Pulst SM. Spinocerebellar ataxia 2 (SCA 2). In: Pulst SM. Genetics of movement disorders. Amsterdam: Academic Press; 2003. p. 45-56.
4. Arruda WO, Carvalho Neto A. Late onset autosomal dominant cerebellar
ataxia. Neurobiologia. 1991;54(1):35-44.
5. Klockgether T. Recent advances in degenerative ataxias. Curr Opin Neurol. 2000;13(4):451-5.
6. Teive HAG. Avaliação clínica e genética de oito famílias brasileiras com ataxia espinocerebelar tipo 10 [tese]. Curitiba: Departamento de Medicina Interna do Setor de Ciências da Saúde da Universidade Federal do Paraná; 2004.
7. Freund AA. Diagnóstico molecular das ataxias espinocerebelares tipo 1, 2, 3, 6 e 7: estudo populacional e em indivíduos com suspeita clínica [tese]. Curitiba: Departamento de Medicina Interna do Setor de Ciências da Saúde da Universidade Federal do Paraná; 2007.
8. Jardim LB, Silveira I, Pereira ML, Ferro A, Alonso I, do Céu Moreira M,
et al. A survey of spinocerebellar ataxia in South Brazil – 66 new cases with Machado-Joseph disease, SCA7, SCA8, or unidentiied disease-causing mutations. J Neurol. 2001;248(10):870-6.
9. Webster WR, Garey LJ. Auditory system. In: Paxinos G (ed). The human
nervous system. San Diego: Academic Press; 1990. p. 889-944. 10. Nachmanoff DB, Segal RA, Dawson DM, Brown RB, De Girolami
U. Hereditary ataxia with sensory neuronopathy: Biemond’s ataxia. Neurology. 1997;48(1):273-5.
11. Biacabe B, Chevallier JM, Avan P, Bonfils P. Functional anatomy of auditory brainstem nuclei: application to the anatomical basis
of brainstem auditory evoked potentials. Auris Nasus Larynx.
2001;28(1):85-94.
12. Dueñas AM, Goold R, Giunti P. Molecular pathogenesis of spinocerebellar ataxias. Brain. 2006;129(Pt 6):1357-70.
13. Schöls L, Bauer P, Schmidt T, Schulte T, Riess O. Autosomal dominant cerebellar ataxias: clinical features, genetics, and pathogenesis. Lancet
Neurol. 2004;3(5):291-304.
14. Pearson CE, Edamura KN, Cleary JD. Repeat instability: mechanisms of dynamic mutations. Nat Rev Genet. 2005;6(10):729-42.
15. Davis H, Silverman SR. Hearing and deafness. 3ª ed. New York: Ed. Holt, Rinehart & Wilson; 1970.
16. Silman S, Silverman CA. Basic audiologic testing. In: Silman S, Silverman CA, Auditory diagnosis: principles and applications. San Diego: Singular Publishing Group; 1997. p. 38-58.
17. Hall JW. Handbook of auditory evoked responses. Boston: Allyn & Bacon; 1992.
18. Jerger J. Clinical experience with impedance audiometry. Arch Otolaryngol. 1970;92(4):311-24.
19. Knezevic W, Stewart-Wynne EG. Brainstem auditory evoked responses in hereditary spinocerebellar ataxias. Clin Exp Neurol. 1985;21:149-55.
20. Kondo H, Harayama H, Shinozawa K, Yuasa T, Miyatake T. Auditory brainstem response and somatosensory evoked potential in Machado-Joseph disease in Japanese families. Rinsho Shinkeigaku. 1990;30(7):723-7.
21. Abele M, Bürk K, Andres F, Topka H, Laccone F, Bösch S, et al.
Autosomal dominant cerebellar ataxia type I. Nerve conduction and evoked potential studies in families with SCA1, SCA2 and SCA3. Brain. 1997;120(Pt 12):2141-8.
22. Schöls L, Linnemann C, Globas C. Electrophysiology in spinocerebellar
ataxias: spread of disease and characteristic findings. Cerebellum. 2008;7(2):198-203.
23. Yokoyama J, Aoyagi M, Suzuki T, Kiren T, Koike Y. Three frequency component waveforms of auditory evoked brainstem response in spinocerebellar degeneration. Acta Otolaryngol Suppl. 1994;511:52-5.
24. Hoche F, Seidel K, Brunt ER, Auburger G, Schöls L, Bürk K, et al.
Involvement of the auditory brainstem system in spinocerebellar ataxia type 2 (SCA2), type 3 (SCA3) and type 7 (SCA7). Neuropathol Appl Neurobiol. 2008:34(5):479-91.
25. Jurkiewicz AL, Floriani A, Collaço LM, Zeigelboim BS. Anatomia funcional da orelha. In: Zeigelboim BS, Jurkiewicz AL (org).
Multidisciplinaridade na otoneurologia. São Paulo: Roca; 2012. p. 19-95.
26. Carvalho RMM. Imitância acústica. In: Zeigelboim BS, Jurkiewicz AL
(org). Multidisciplinaridade na otoneurologia. São Paulo: Roca; 2012. p. 122-30.
Table 5. Distribution of the results of the audiological, brainstem auditory evoked potential and acoustic immittance evaluations in spinocerebellar ataxias 2, e, and 10
Audiological evaluation SCA 2 n (%)
SCA 3 n (%)
SCA 10 n (%)
Normal 7 (87.5) 8 (66.7) 3 (50.0)
Altered 1 (12.5) 4 (33.3) 3 (50.0)
Total 8 (100.0) 12 (100.0) 6 (100.0)
p-value 0.0096* 0.1160 1.0000
BAEP
Normal 3 (37.5) 5 (41.7) 2 (33.3)
Altered 5 (62.5) 7 (58.3) 4 (66.7)
Total 8 (100.0) 12 (100.0) 6 (100.0)
p-value 0.3343 0.4248 0.2742
Acoustic immittance
Normal 4 (50.0) 6 (50.0) 4 (66.7)
Altered 4 (50.0) 6 (50.0) 2 (33.3)
Total 8 (100.0) 12 (100.0) 6 (100.0)
p-value 1.0000 1.0000 0.2742
Legend: SCA = spinocerebellar ataxias; BAEP = brainstem auditory-evoked potential