REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Effects
of
a
novel
method
of
anesthesia
combining
propofol
and
volatile
anesthesia
on
the
incidence
of
postoperative
nausea
and
vomiting
in
patients
undergoing
laparoscopic
gynecological
surgery
夽
Hiroaki
Kawano
∗,
Naohiro
Ohshita,
Kimiko
Katome,
Takako
Kadota,
Michiko
Kinoshita,
Yayoi
Matsuoka,
Yasuo
M.
Tsutsumi,
Shinji
Kawahito,
Katsuya
Tanaka,
Shuzo
Oshita
DepartmentofAnesthesiology,TokushimaUniversityHospital,Tokushima,Japan
Received20May2014;accepted3July2014 Availableonline30October2014
KEYWORDS
Postoperativenausea
andvomiting;
Propofol; Sevoflurane;
Generalanesthesia;
Laparoscopy
Abstract
Background: Weinvestigatedtheeffectsofanovelmethodofanesthesiacombining propo-folandvolatileanesthesiaontheincidenceofpostoperativenauseaandvomitinginpatients undergoinglaparoscopicgynecologicalsurgery.
Methods:Patientswererandomlydividedintothreegroups:thosemaintainedwithsevoflurane (GroupS,n=42),propofol(GroupP,n=42),orcombinedpropofolandsevoflurane(GroupPS, n=42).Weassessedcompleteresponse(nopostoperativenauseaandvomitingandnorescue antiemeticuse),incidenceofnauseaandvomiting,nauseaseverityscore,vomitingfrequency, rescueantiemeticuse,andpostoperativepainat2and24haftersurgery.
Results:ThenumberofpatientswhoexhibitedacompleteresponsewasgreaterinGroupsPand PSthaninGroupSat0---2h(74%,76%and43%,respectively,p=0.001)and0---24h(71%,76%and 38%,respectively,p<0.0005).Theincidenceofnauseaat0---2h(GroupS=57%,GroupP=26% andGroupPS=21%,p=0.001)and0---24h(GroupS=62%,Group P=29%andGroupPS=21%, p<0.0005)wasalso significantlydifferentamonggroups.However,therewerenosignificant differencesamonggroupsintheincidenceorfrequencyofvomitingorrescueantiemeticuse at0---24h.
Conclusion:Combined propofol and volatile anesthesia during laparoscopic gynecological surgeryeffectivelydecreasestheincidenceofpostoperativenausea.Wetermthisnovelmethod ofanesthesia‘‘combinedintravenous-volatileanesthesia(CIVA)’’.
©2014SociedadeBrasileiradeAnestesiologia.PublishedbyElsevier EditoraLtda.Allrights reserved.
夽 Presentedinpartatthe57thAnnualMeetingoftheJapaneseSocietyofAnesthesiologists,Fukuoka,Japan,3-5June2010.
∗Correspondingauthor.Presentaddress:DepartmentofAnesthesiology,TokushimaPrefecturalCentralHospital,Tokushima,Japan. E-mail:[email protected](H.Kawano).
http://dx.doi.org/10.1016/j.bjane.2014.07.005
PALAVRAS-CHAVE
Náuseaevômito
pós-operatórios; Propofol; Sevoflurano;
Anestesiageral;
Laparoscopia
Efeitosdeumnovométododeanestesiacombinandopropofoleanestesiavolátil sobreaincidênciadenáuseaevômitonopós-operatórioempacientessubmetidasà laparoscopiaginecológica
Resumo
Justificativa: Investigamososefeitosdeumnovométododeanestesia,combinandopropofole anestesiavolátil,sobreaincidênciadenáuseaevômitonoperíodopós-operatóriodepacientes submetidasàlaparoscopiaginecológica.
Métodos: As pacientes foram randomicamente divididas em três grupos: manutenc¸ão com sevoflurano(GrupoS,n=42),compropofol(GrupoP,n=42)oucomacombinac¸ãodepropofol esevoflurano(GrupoPS,n=42).Avaliamosasrespostascompletas(semnáuseaevômitono pós-operatórioesemusodeantieméticoderesgate),incidênciadenáuseaevômito,escore degravidadedanáusea,freqüênciadevômitos,usodeantieméticoderesgateedorno pós-operatórioem2e24hapósacirurgia.
Resultados: OnúmerodedoentesqueapresentouumarespostacompletafoimaiornosgruposP ePSquenoGrupoSem0-2h(74%,76%e43%,respectivamente,p=0,001)e0-24h(71%,a76%e 38%,respectivamente,p<0,0005).Aincidênciadenáuseaem0-2h(GrupoS=57%,GrupoP=26% eGrupoPS=21%,p=0,001)e0-24h(GrupoS=62%,GrupoP=29%egrupoPS=21%,p<0,0005) tambémfoisignificativamentediferenteentreosgrupos.Porém,nãohouvediferenc¸a significa-tivaentreosgruposemrelac¸ãoàincidênciaoufrequênciadevômitosouusodeantiemético deresgateem0-24h.
Conclusão:Acombinac¸ãodepropofoleanestesiavolátildurantealaparoscopiaginecológica efetivamentediminuiaincidênciadenáuseanopós-operatório.Denominamosestenovométodo deanestesia‘‘anestesiacombinadaintravenosavolátil(ACIV)’’.
©2014SociedadeBrasileira deAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Volatile anesthetics exert cardioprotective effects
medi-atedbythe activationofadenosine triphosphate-sensitive
potassium(KATP)channelsincardiacmyocytes.1,2Theyalso
affect coronary vasodilation by activating KATP channels
in vascular smooth muscle cells.3,4 Therefore, the use of
volatileanestheticsforclinicalanesthesiamaybebeneficial inpreventionofcoronaryarterydisease.
Total intravenous anesthesia (TIVA) with propofol also
hasmanyadvantages.Itdecreasestheincidenceof
postop-erativenauseaandvomiting(PONV),5,6decreasescerebral
bloodflowandintracranialpressure,7andattenuates
post-operativepain8andneuroendocrinestressresponse.9
Becauseofthesebenefitscombinedwiththerapidonset
andcessationofaction,bothvolatileanestheticsand propo-folareextensivelyusedforclinicalanesthesia.
We hypothesized that a novel method of anesthesia
combiningpropofolandvolatileanesthesiacanprovidethe
benefitsofbothwhiledecreasingthedisadvantagesofeach
anesthetic. In this study, we investigated the effects of
combinedpropofolandvolatileanesthesiaontheincidence
ofPONVinpatientsundergoinglaparoscopicgynecological
surgery.
Materials
and
methods
AfterobtainingapprovalforthisstudyfromtheEthics
Com-mitteeonHumanStudiesofTokushimaUniversityHospital,
written informedconsent wasobtained fromall patients.
All patients were scheduled for elective laparoscopic
gynecologicalsurgery(removalofovariantumorsandcysts,
adhesiolysis,myomectomy, salpingostomy, ovarian drilling
andoophorectomy)undergeneralendotrachealanesthesia,
withanAmericanSocietyof Anesthesiologists(ASA)
physi-calstatusofIandII.Thestudy’sexclusioncriteriawereas follows:obesity(bodymassindex>33kg/m2);neurological,
renal,orliverdisease;andtheuseofdrugswithantiemetic properties,includingcorticosteroids.Riskfactorsassociated
withPONVwererecorded.
Patientswererandomlyassignedtooneofthefollowing
threegroups bythesealedenvelopemethod:those
main-tained withsevoflurane (Group S), thosemaintained with
propofol(Group P), and thosemaintained with combined
propofolandsevoflurane(GroupPS).
No preanesthetic medication was administered. All
patientsweremonitored by electrocardiography,
noninva-sivearterialblood pressuremeasurement,pulseoximetry,
capnography,andthebispectralindex(BIS)monitoring.No
nasogastric tubes were inserted. General anesthesia was
inducedwithintravenousremifentanil,thiamylal(GroupS)
orpropofol(GroupsPandPS)androcuronium.Anesthesia
wasmaintainedwithremifentanilandsevoflurane,propofol,
orcombinedpropofolandsevofluranein2:1airandoxygen.
InGroupS,anesthesiawasmaintainedwithsevoflurane
(end-tidalconcentrationapproximately1minimumalveolar
concentration). In Group P, anesthesia was maintained
with an infusion of propofol (4---8mg/kg/h). In Group
PS, anesthesia was maintained with combined propofol
(2mg/kg/h) and sevoflurane (end-tidal concentration
approximately 0.5 minimum alveolar concentrations).
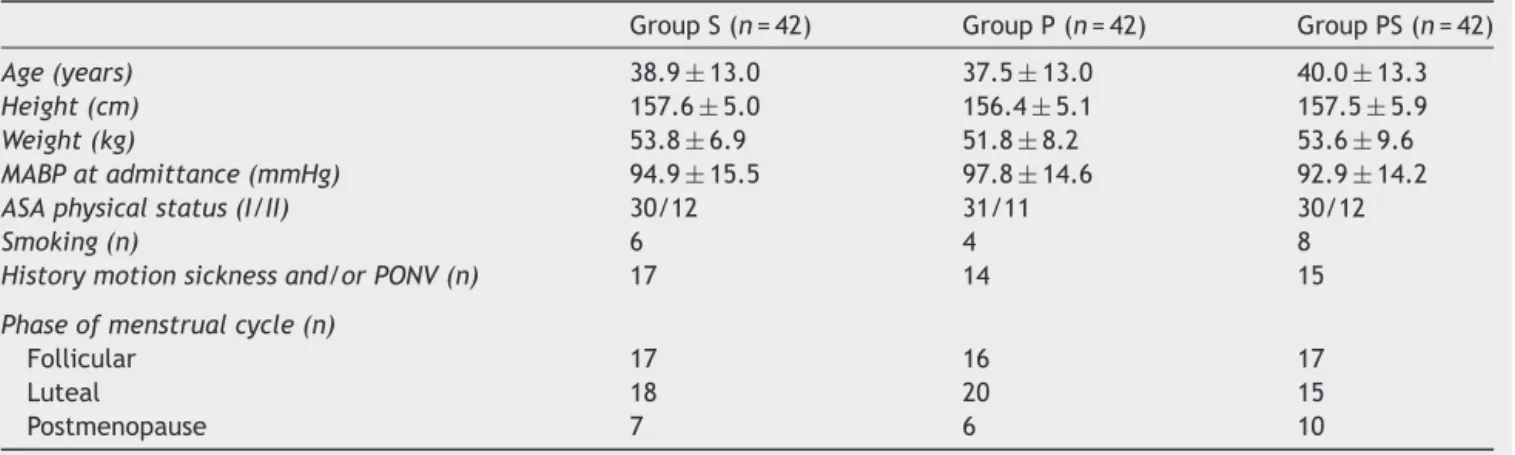
Table1 Patientdemographics.
GroupS(n=42) GroupP(n=42) GroupPS(n=42)
Age(years) 38.9±13.0 37.5±13.0 40.0±13.3 Height(cm) 157.6±5.0 156.4±5.1 157.5±5.9
Weight(kg) 53.8±6.9 51.8±8.2 53.6±9.6
MABPatadmittance(mmHg) 94.9±15.5 97.8±14.6 92.9±14.2 ASAphysicalstatus(I/II) 30/12 31/11 30/12
Smoking(n) 6 4 8
Historymotionsicknessand/orPONV(n) 17 14 15
Phaseofmenstrualcycle(n)
Follicular 17 16 17
Luteal 18 20 15
Postmenopause 7 6 10
MABP,meanarterialbloodpressure.
Datapresentedasmean±SDornumberofpatients.Anesthesiawasmaintainedwithsevoflurane (GroupS),propofol(GroupP), or combinedpropofolandsevoflurane(GroupPS).
rates (Group P) were titrated to achieve a target BIS
value of 40---60. In Group PS, propofol infusion rate and
sevofluraneconcentrationwerefixed.
Intraoperative analgesia was performed by titrating
remifentanil infusion at the discretion of the attending
anesthesiologist. Neuromuscularblockade wasmaintained
withintermittentrocuronium.Ringer’sacetatesolutionwas
administeredat10mL/kg/hforthefirsthourofanesthesia
andat5mL/kg/hforallsubsequenthours.Beforetheendof
surgery,allpatientsreceivedflurbiprofenaxetil(1mg/kg).
Attheendofsurgery,neuromuscularblockadewasreversed
withatropine(0.5mg)andneostigmine(1mg).
The incidence and severity of PONV were assessed by
blindedobservers at2and24haftersurgery.The severity
of nausea was recorded using the following scale: no
nausea,mildnausea,moderatenausea,andseverenausea.
AcompleteresponsewasdefinedasnoPONVandnorescue
antiemetic use. Intravenous metoclopramide (10mg) was
used as the rescue antiemetic. Postoperative pain was
evaluated using a numerical rating scale (0=no pain to
10=maximal pain). When a patient requested analgesia,
a diclofenac suppository (25mg) or intramuscular
penta-zocine (15mg) was administered. The 0---2h and 2---24h
intervalsweredefinedasearlyandlate,respectively. The
primaryendpoint wasthe complete responserate within
24hofsurgery.
Apreviousstudy10reportedacumulativePONVincidence
of70%at24h inpatientsundergoinglaparoscopic
gyneco-logicalsurgery.The samplesizewasdeterminedbypower
analysistoprovideapowerof0.8todetecta35%absolute
decreaseinthecumulativePONVincidence(˛=0.05).
Sta-tisticalanalysiswasperformedwithSPSS® version18(SPSS
Inc.,Chicago,IL,USA).Continuousvariableswerecompared
byone-wayanalysisofvariance, withBonferroniposthoc
testsformultiple comparisons.Categoricalvariableswere
analyzed using the 2 or Fisher’s exact tests, with
cor-rectionfor multiple comparisons whereappropriate. Data
are expressed as number of patients or mean±standard
deviation. Ap-value of <0.05 was considered statistically significant.
Results
Of130patients,fourwereexcludedfromthisanalysis:two
who convertedtolaparotomy and twoviolated the study
protocol. Therefore,42 patients wererandomly allocated
toGroupS,42toGroupP,and42toGroupPS.
Demographic data were similar with respect to age,
weight,height,ASAphysicalstatus,smokinghistory,history
ofmotionsicknessand/orPONV,andmenstrualcyclephase
(Table1).Similarly,therewerenosignificantdifferencesin
intraoperativevariables,includingthedurationof
anesthe-siaandsurgery,totaldosesofremifentanilandrocuronium,
surgery type, temperature, blood loss, and intravascular
fluidvolume(Table2).
A complete response at 24h (primary end point) was
achievedin38%patientsinGroupS,71%inGroupPand76%
inGroupPS(p<0.0005)(Table3).GroupsPandPSdiffered significantly from Group S (p=0.012 and<0.002,
respec-tively),butnosignificant differencewasevident between
GroupsPandPS(Table3).Theincidenceofnauseaat24h wasalsosignificantlydifferent(GroupS=62%,GroupP=29% andGroupPS=21%,p<0.0005).Thesignificantnausearate wasalsolowerinGroupPandPSthaninGroupS(p=0.003).
However,therewerenostatisticallysignificantdifferences
amonggroupsintheincidenceorfrequencyofvomitingor
rescueantiemeticuseat24h(Table3).
In the early postoperative period, the proportion of
patientswhoexperiencedacompleteresponsewas
signifi-cantlyhigherinGroupsP(74%)andPS(76%)thaninGroup
S (43%) (p=0.001). The incidence of nauseawasalso
sig-nificantly lower in Groups P (26%) and PS (21%) than in
Group S (57%) (p=0.001).However, therewere no
statis-ticallysignificantdifferencesamonggroupsintheincidence orfrequencyofvomitingatthistime(Table3).
Inthelatepostoperativeperiod,althoughtheincidence
ofnauseawaslowerinGroupsP(12%)andPS(10%)thanin
GroupS(26%),thedifferencewasnotstatisticallysignificant (p=0.078).Theproportionofpatientsexhibitingacomplete
response,theincidenceandfrequencyofvomiting,severity
ofnausea,andrescueantiemeticusedidnotdifferamong
Table2 Surgery/anesthesia-relatedparameters.
GroupS(n=42) GroupP(n=42) GroupPS(n=42)
Durationofanesthesia(min) 171.2±58.6 167.9±67.1 155.5±48.7 Durationofsurgery(min) 124.7±54.5 122.1±65.3 111.5±48.7
Anesthetics
Remifentanil(mg) 3.082±1.884 3.197±1.856 3.055±1.420
Rocuronium(mg) 54.8±13.2 53.1±13.4 50.6±13.0
Typeofsurgery(n)
Ovariancystectomy/tumorectomy 31 24 32
Adhesiolysis 2 5 2
Myomectomy 6 9 3
Salpingostomy 1 0 2
Ovariandrilling 1 0 1
Oophorectomy 1 4 2
Temperature(◦C) 36.6±0.4 36.4±0.4 36.6±0.6 Bloodloss(mL) 28.8±54.5 65.4±142.7 31.4±58.8 Fluidvolume(mL) 1059.0±312.3 1109.8±440.9 1036.0±341.1
Datapresentedasmean±SDornumberofpatients.
Anesthesiawasmaintainedwithsevoflurane(GroupS),propofol(GroupP),orcombinedpropofolandsevoflurane(GroupPS).
Table3 Incidenceofpostoperativenauseaandvomiting.
GroupS(n=42) GroupP(n=42) GroupPS(n=42) p-Value
0---2postoperativehours
Nausea 24(57) 11(26)b 9(21)b 0.001a
Significantnausea(moderateorsevere) 16(38) 7(17) 3(7)b 0.001a
Vomiting 4(10) 5(12) 3(7) 0.759
Vomitingepisodesinpatientswhovomited 2.3±1.5 1.2±0.4 2±1.7 0.155
Postoperativenauseaand/orvomiting 24(57) 11(26)b 9(21)b 0.001a
Rescueantiemetic 8(19) 1(2) 2(5) 0.014a
Completeresponse 18(43) 31(74)b 33(76)b 0.001a
2---24postoperativehours
Nausea 11(26) 5(12) 4(10) 0.078
Significantnausea(moderateorsevere) 1(2) 3(7) 2(5) 0.592
Vomiting 2(5) 4(10) 2(5) 0.586
Vomitingepisodesinpatientswhovomited 1.5±0.7 2.3±1.5 3±0 0.530
Postoperativenauseaand/orvomiting 11(26) 5(12) 4(10) 0.078
Rescueantiemetic 2(5) 3(7) 0(0) 0.233
Completeresponse 31(74) 36(86) 38(90) 0.108
0---24postoperativehours
Nausea 26(62) 12(29)b 9(21)b <0.0005a
Significantnausea(moderateorsevere) 17(40) 8(19) 4(10)b 0.003a
Vomiting 4(10) 6(14) 3(7) 0.549
Vomitingepisodesinpatientswhovomited 3±2.2 2.5±1.2 4±3 0.651
Postoperativenauseaand/orvomiting 26(62) 12(29)b 9(21)b <0.0005a
Rescueantiemetic 9(21) 4(10) 2(5) 0.052
Completeresponse 16(38) 30(71)b 33(76)b <0.0005a
Datapresentedasmean±SDornumberofpatients(%).
Anesthesiawasmaintainedwithsevoflurane(GroupS),propofol(GroupP),orcombinedpropofolandsevoflurane(GroupPS).
a Statisticallysignificantdifference(p<0.05).
Table4 Postoperativepaindata.
GroupS(n=42) GroupP(n=42) GroupPS(n=42)
Numericalratingscale(0---10) Postoperativeat
2h 6.4±2.5 5.6±2.3 5.9±3.0
24h 4.1±2.3 3.7±1.9 3.8±2.4
Postoperativediclofenacsodium(mg) 17.3±18.7 16.7±18.0 17.9±18.5
Postoperativepentazocine(mg) 7.9±8.9 8.6±13.7 4.6±7.4
Datapresentedasmean±SD.
Anesthesiawasmaintainedwithsevoflurane(GroupS),propofol(GroupP),orcombinedpropofolandsevoflurane(GroupPS).
Therewasnodifferenceamonggroupsinthenumerical
ratingscaleoranalgesiause(Table4).Nopatientsreported
intraoperativeawareness.
Discussion
Thisstudydemonstratesthattheuseofcombinedpropofol
andsevofluraneanesthesiaduringlaparoscopic
gynecologi-calsurgerydecreasesPONVincidence.Thisisthefirststudy,
asper ourknowledge, to assess the effects of combined
propofolandvolatileanesthesiaonPONVincidence.
The use of volatile anesthetics such as isoflurane
and sevoflurane has many benefits. The representative
beneficial effect is cardioprotection. Volatile
anesthet-ics have been shown to protect the myocardium against
myocardialischemia andreperfusion injurythrough a
sig-nal transduction pathway that includes protein kinase
C and mitochondrial and sarcolemmal KATP channels.1,2
Reportedly,3,4 volatile anesthetics also cause coronary
vasodilatationby activatingvascular KATP channels.
Ran-domized clinical trials in patients undergoing coronary
arterysurgeryhavedemonstratedthatvolatileanesthetics
decreasetroponin release, the duration of intensive care
unit stay, and the incidence of late cardiac events and
enhance leftventricularfunction.11 On the basis ofthese
trials,theAmericanCollegeofCardiology/AmericanHeart
Association2007guidelinesonperioperativecardiovascular
evaluationandcarefornoncardiacsurgery11recommendthe
useofvolatileanestheticagentsduringnoncardiacsurgery
formaintenanceofgeneralanesthesiainhemodynamically
stablepatients at risk for myocardial ischemia (Class IIa,
levelofevidenceB).Theadditionalbenefitsofvolatile anes-thesiaincludealowerincidenceofintraoperativeawareness duringgeneralanesthesia12andabronchodilatoryeffect.13
TIVA with propofol is associated with a lower PONV
incidence.5,6 In addition, TIVA has many advantages over
volatileanesthesia.Severalstudies7haveshownthat
propo-folcauses adose-relateddecrease incerebral bloodflow,
the rateof cerebral metabolism of oxygen, and
intracra-nial pressure. Animal studies14 have demonstrated that
volatileanestheticsinhibithypoxicpulmonary
vasoconstric-tion(HPV)inadose-dependentmanner,althoughpropofol
doesnotseemtoaffectHPV.15Althoughitremains
contro-versialwhetherpropofolcaninducemalignanthyperthermia
(MH),16 Sumitani et al.17 reporteda relatively low
preva-lence of MH in propofol users. Previous studies8 have
demonstrated that patients anesthetized with propofol
experiencelesspainthanthoseanesthetizedwithvolatile
anesthetics. Furthermore, TIVA was shown to be more
effective in inhibiting the neuroendocrine stress response
comparedwithvolatileanesthesia.9Propofolmayalso
pre-venttissuedamageresultingfromoxidativestress18through
itsantioxidantproperties.19
Propofol and volatile anesthetics such as sevoflurane
and desflurane are extensively used for clinical
anesthe-sia because of the rapid onset and cessation of action.
The use of each anesthetic has both advantages and
dis-advantages. We developed a novel method of anesthesia
combiningpropofol andvolatile anesthesiatoreceive the
benefitsanddecreasethedisadvantagesofeachanesthetic.
However,thiswasjustahypothesis,andtheactualeffects
ofcombination remainunknown.Therefore,weevaluated
theeffectsofcombinedpropofolandvolatileanesthesiaon
PONV incidenceinpatients undergoinglaparoscopic
gyne-cologicalsurgery.
Theresultsofthisstudyshowedthattheuseofcombined
propofolandvolatileanesthesiaduringlaparoscopic
gyneco-logicalsurgerycauseda66%reductioninPONV(from62%to
21%),aneffectthatwasmorepronouncedintheearly
post-operativeperiod.Surprisingly,thiseffectiscomparablewith thatofTIVAwithpropofol(a66%decreaseinGroupPSversus
a53%decreaseinGroupP).ThePONVincidenceinGroupS
(62%)wassimilartothepreviouslyreportedPONVincidence
undergoinglaparoscopicgynecologicalsurgery.10,20
PatientsinGroupPSreceivedsignificantlysmallerdoses
of sevoflurane during anesthesia, which may explain the
decreasedPONVincidence.Apfeletal.21 reportedthatthe
degree of exposure to volatile anesthetics is the primary
causeof PONV inthe early postoperativeperiod.Another
reason for the decreased PONV incidence could be the
antiemeticeffectsofpropofol.Theantiemeticpropertiesof
propofolwerefirstdemonstratedbyBorgeatetal.22and
sub-sequently byseveralother authors.23 However,itsprecise
mechanismofactionremainsunclear.Propofolmayactasa
dopaminereceptorantagonist.24 Ithasalsobeenshownto
possessaweakantagonisticeffectagainstserotonin.
How-ever, the precise mechanism by which propofol exerts its
antiemeticeffectsremainundetermined.Reportedly,25 the
effect is associated with a defined plasma concentration
range;the plasma propofolconcentration associatedwith
a50%decreaseinnauseascoreswasfoundtobe343ng/mL.
According tothe pharmacokineticsimulation(TIVAtrainer
8,Frank Engbers,Leiden,The Netherlands),155min after
an induction dose of 1.5mg/kg and maintenance with
Simulationdataalsodemonstratethattheplasmapropofol
concentrationdropsbelow350ng/mLwithinapproximately
170min oftheendofinfusion.These simulationdata
sug-gestthattheplasmaconcentrationofpropofolusedinour
methodwillabovetherangeeffectiveforantiemesisuntil
approximately170minaftertheendofsurgery.This
prob-ably explains why patients in Group PS exhibiteda lower
incidenceof PONV,particularly inthe early postoperative
period.
Limitationsofthestudy
Our study has some limitations. First, there is increasing
consensus that better PONV prophylaxis can be achieved
throughtheuse ofa combination ofagents actingon
dif-ferent receptors, considering that multiple receptors are
involvedintheetiologyofPONV.Inhigh-riskpatients,a
mul-timodalapproachtopreventPONVhasbeenrecommended.
However,wedidnotadministeranyprophylacticantiemetic
or combined agents to prevent PONV. This is because
we wanted to investigate the baseline risk, which could
havebeen masked byprophylacticantiemetic.Decreasing
thebaseline riskhas been recommended26 becauseit can
significantlydecreasePONVincidence.27,28Inaddition,
pro-phylacticantiemeticareassociatedwithanincreaseinboth costsandadverseeffects.29,30 Therefore,weconsideredit
important to study the pure incidence of PONV for each
method of anesthesia. Second, only one combination of
propofol infusion rate and sevoflurane concentration was
studied, and the effects of other combinations were not
assessed in this study. Therefore, the optimal
combina-tionofpropofolinfusionrateandsevofluraneconcentration
remainstobedetermined.
Conclusions
In conclusion, combined propofol and volatile
anesthe-sia during laparoscopic gynecological surgery effectively
decreases PONV incidence in the absence of
prophylac-tic antiemetic. Although further experimental researchis
required to clarify its efficacy in a clinical context, we
believe that combined propofol and volatile anesthesia
offerspotentialclinicalbenefits.Wetermthisnovelmethod
of anesthesia ‘‘combined intravenous-volatile anesthesia
(CIVA)’’.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Tanaka K, Weihrauch D, Ludwig LM, et al. Mitochondrial adenosinetriphosphate-regulatedpotassiumchannel opening acts as a trigger for isoflurane-induced preconditioning by generatingreactiveoxygen species. Anesthesiology.2003;98: 935---43.
2.Tanaka K, Ludwig LM, Kersten JR, et al. Mechanisms of cardioprotection by volatile anesthetics. Anesthesiology. 2004;100:707---21.
3.CrystalGJ, GureviciusJ, SalemMR,etal.Roleofadenosine triphosphate-sensitivepotassiumchannelsincoronary vasodi-lationbyhalothane,isoflurane,andenflurane.Anesthesiology. 1997;86:448---58.
4.ZhouX,AbboudW,ManabatNC,etal.Isoflurane-induced dila-tionofporcinecoronaryarteriolesismediatedbyATP-sensitive potassiumchannels.Anesthesiology.1998;89:182---9.
5.HabibAS,WhiteWD,EubanksS,etal.Arandomized compari-sonofamultimodalmanagementstrategyversuscombination antiemetics for the prevention of postoperative nausea and vomiting.AnesthAnalg.2004;99:77---81.
6.MukherjeeK,SeavellC,RawlingsE,etal.Acomparisonoftotal intravenouswithbalancedanaesthesiaformiddleearsurgery: effectsonpostoperativenauseaandvomiting,pain,and condi-tionsofsurgery.Anaesthesia.2003;58:176---80.
7.PinaudM,LelausqueJN,ChetanneauA,etal.Effectsof propo-foloncerebralhemodynamicsandmetabolisminpatientswith braintrauma.Anesthesiology.1990;73:404---9.
8.ChengSS,YehJ,FloodP.Anesthesia matters:patients anes-thetizedwithpropofolhavelesspostoperativepainthanthose anesthetized withisoflurane.Anesth Analg. 2008;106:264---9, tableofcontents.
9.MaranaE,ColicciS,MeoF,etal.Neuroendocrinestressresponse ingynecologicallaparoscopy:TIVAwithpropofolversus sevoflu-raneanesthesia.JClinAnesth.2010;22:250---5.
10.BoehlerM,MitterschiffthalerG,SchlagerA.Koreanhand acu-pressurereducespostoperativenauseaandvomitingafter gyne-cological laparoscopic surgery.Anesth Analg.2002;94:872---5, tableofcontents.
11.Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2007 guidelinesonperioperativecardiovascularevaluationandcare for noncardiacsurgery: a reportof theAmerican Collegeof Cardiology/AmericanHeartAssociationTaskForceonPractice Guidelines (Writing Committee to Revise the 2002 Guide-linesonPerioperativeCardiovascularEvaluationforNoncardiac Surgery):developedincollaborationwiththeAmericanSociety ofEchocardiography,AmericanSocietyofNuclearCardiology, HeartRhythmSociety,SocietyofCardiovascular Anesthesiolo-gists,SocietyforCardiovascularAngiographyandInterventions, SocietyforVascularMedicineandBiology,andSocietyfor Vas-cularSurgery.Circulation.2007;116:e418---99.
12.Ghoneim MM. Awareness during anesthesia. Anesthesiology. 2000;92:597---602.
13.PabelickCM,PrakashYS,KannanMS,etal.Effectsofhalothane onsarcoplasmicreticulumcalciumreleasechannelsinporcine airwaysmoothmusclecells.Anesthesiology.2001;95:207---15.
14.IshibeY,GuiX,UnoH,etal.Effectofsevofluraneonhypoxic pulmonaryvasoconstrictionintheperfusedrabbitlung. Anes-thesiology.1993;79:1348---53.
15.SchwarzkopfK,SchreiberT,PreusslerNP,etal.Lungperfusion, shuntfraction,andoxygenationduringone-lungventilationin pigs:theeffectsofdesflurane,isoflurane,andpropofol.J Car-diothoracVascAnesth.2003;17:73---5.
16.MigitaT,MukaidaK,HamadaH,etal.Effectsofpropofolon cal-ciumhomeostasisinhumanskeletalmuscle.AnaesthIntensive Care.2009;37:415---25.
17.SumitaniM,UchidaK,YasunagaH,etal.Prevalenceof malig-nanthyperthermiaandrelationshipwithanestheticsinJapan: datafromthediagnosisprocedurecombinationdatabase. Anes-thesiology.2011;114:84---90.
18.Nakahata K, Kinoshita H, Azma T, et al. Propofol restores brainmicrovascularfunctionimpairedbyhighglucoseviathe decreaseinoxidativestress.Anesthesiology.2008;108:269---75.
19.Murphy PG, Myers DS, Davies MJ, et al. The antioxidant potential of propofol (2,6-diisopropylphenol). Br J Anaesth. 1992;68:613---8.
undergoingoutpatientgynecologicallaparoscopy.AnesthAnalg. 1996;82:533---8.
21.ApfelCC,KrankeP,KatzMH,etal.Volatileanaestheticsmaybe themaincauseofearlybutnotdelayedpostoperativevomiting: arandomizedcontrolledtrialoffactorialdesign.BrJAnaesth. 2002;88:659---68.
22.BorgeatA,Wilder-SmithOH,SaiahM,etal.Subhypnoticdoses ofpropofolpossessdirectantiemeticproperties.AnesthAnalg. 1992;74:539---41.
23.Gan TJ, GinsbergB, Grant AP, et al. Double-blind, random-ized comparison of ondansetron and intraoperative propofol topreventpostoperativenauseaandvomiting.Anesthesiology. 1996;85:1036---42.
24.DiFlorio T. Is propofola dopamine antagonist? AnesthAnalg. 1993;77:200---1.
25.GanTJ, GlassPS,HowellST, etal.Determination ofplasma concentrations of propofol associated with50% reduction in postoperativenausea.Anesthesiology.1997;87:779---84.
26.Gan TJ, Meyer T, Apfel CC, et al. Consensus guidelines for managing postoperativenausea and vomiting. Anesth Analg. 2003;97:62---71,tableofcontents.
27.Tramer MR. A rational approach to the control of post-operative nausea and vomiting: evidence from systematic reviews.PartI.Efficacyandharmofantiemeticinterventions, andmethodologicalissues.ActaAnaesthesiolScand.2001;45: 4---13.
28.Tramer MR. A rational approach to the control of post-operative nausea and vomiting: evidence from systematic reviews.PartII. Recommendationsfor prevention and treat-ment,andresearchagenda.ActaAnaesthesiolScand.2001;45: 14---9.
29.ScholzJ, Steinfath M, Tonner PH. Postoperative nauseaand vomiting.CurrOpinAnaesthesiol.1999;12:657---61.