www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Hearing
health
network:
a
spatial
analysis
夽
Camila
Ferreira
de
Rezende
a,
Sirley
Alves
da
Silva
Carvalho
b,∗,
Fernanda
Jorge
Maciel
c,
Raimundo
de
Oliveira
Neto
d,
Darlan
Venâncio
Thomaz
Pereira
e,
Stela
Maris
Aguiar
Lemos
baUniversidadeFederaldeMinasGerais(UFMG),BeloHorizonte,MG,Brazil
bDepartmentofPhonoaudiology,UniversidadeFederaldeMinasGerais(UFMG),BeloHorizonte,MG,Brazil cEscoladeSaúdePúblicadoEstadodeMinasGerais,BeloHorizonte,MG,Brazil
dSecretariaMunicipaldeSaúde,JuntaReguladoradaSaúdeAuditiva,Brazil eSecretariadeEstadodeSaúdedeMinasGerais,BeloHorizonte,MG,Brazil
Received18September2013;accepted12January2014 Availableonline28August2014
KEYWORDS
Healthcare(public health);
Audiology; Healthservices evaluation; Publichealth administration; Healthsurveys
Abstract
Introduction:Inordertomeetthedemandsofthepatientpopulationwithhearingimpairment, theHearingHealthCareNetworkwascreated,consistingofprimarycareactionsofmediumand highcomplexity.Spatialanalysisthroughgeoprocessingisawaytounderstandtheorganization ofsuchservices.
Objective:ToanalyzetheorganizationoftheHearingHealthCareNetworkoftheStateofMinas Gerais.
Methods:Cross-sectional analyticalstudy usinggeoprocessing techniques. Theabsolute fre-quency and the frequency per 1000 inhabitants of the following variables were analyzed: assessmentand diagnosis, selection and adaptationofhearing aids, follow-up,and speech therapy.Thespatialanalysisunitwasthehealthmicro-region.
Results:Theassessmentanddiagnosis,selection,andadaptationofhearingaidsandfollow-up hadahigherabsolutenumberinthemicro-regionswithhearinghealthservices.Thefollow-up procedureshowed thelowest occurrence.Speech therapyshowedhigher occurrenceinthe state,bothinabsolutenumbers,aswellasperpopulation.
Conclusion:Theuse ofgeoprocessingtechniquesallowed theidentificationofthecareflow asafunctionoftheprocedureperformancefrequency,populationconcentration,andterritory distribution.AllproceduresofferedbytheHearingHealthCareNetworkareperformedforusers ofallmicro-regionsofthestate.
© 2014Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
夽 Pleasecitethisarticleas:deRezendeCF,CarvalhoSAS,MacielFJ,deOliveiraNetoR,PereiraDVT,LemosSMA.Hearinghealthnetwork: aspatialanalysis.BrazJOtorhinolaryngol.2015;81:232---9.
∗Correspondingauthor.
E-mail:[email protected](S.A.S.Carvalho). http://dx.doi.org/10.1016/j.bjorl.2014.01.003
PALAVRAS-CHAVE
Atenc¸ãoàsaúde; Audiologia;
Avaliac¸ãodeservic¸os desaúde;
Saúdepública; Sistemaúnicode saúde
Rededesaúdeauditiva:umaanáliseespacial
Resumo
Introduc¸ão: Paraatenderàsdemandasdapopulac¸ãocomdeficiênciaauditiva,oSUScriouas RedesEstaduaisdeAtenc¸ãoàSaúdeAuditiva,compostasporac¸õesnaatenc¸ãobásica,médiae altacomplexidade.Umaformadesecompreenderaorganizac¸ãodessesservic¸osnosterritórios desaúdeéutilizando-seanáliseespacial,realizadapormeiodogeoprocessamento.
Objetivo: Analisaraorganizac¸ãodaRedeEstadualdeAtenc¸ãoàSaúdeAuditivaemMinasGerais.
Método: Estudo analítico transversal, utilizando-se técnicas de geoprocessamento. Foram analisadasafrequênciaabsolutaefrequênciapormilhabitantesdasvariáveis:avaliac¸ãoe diag-nóstico,selec¸ãoeadaptac¸ãodeAASI,acompanhamentoeterapiafonoaudiológica.Aunidade deanáliseespacialfoiamicrorregiãodesaúde.
Resultados: Osprocedimentosavaliac¸ãoediagnóstico,selec¸ãoeadaptac¸ãodeAASIe acompan-hamentotiverammaiornúmeroabsolutonasmicrorregiõesondeháServic¸osdeSaúdeAuditiva credenciados.OprocedimentodeacompanhamentoapresentouamenorocorrêncianoEstado. Oprocedimentoterapiafonoaudiológicaapresentoumaiorocorrência,tantoemvalorabsoluto quantoporpopulac¸ão.
Conclusão:A utilizac¸ão do geoprocessamento permitiu identificar o fluxo do atendimento em func¸ão da frequência de realizac¸ão dos procedimentos, concentrac¸ão populacional e distribuic¸ãoterritorial.Todososprocedimentosanalisadossãorealizadosemusuáriosemtodas asmicrorregiõesdoEstado.
©2014Associac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicado por ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Hearingloss characterizesa sensorydeficit thatlimitsthe subject’sperformance atany ageand hasadverse effects onqualityoflife,cognitivefunction,andontheemotional, behavioral,andsocialwell-being.1,2
According to data from the WorldHealth Organization
(WHO),hearinglossisthethirdmostcommondisabilityin
Brazil.Halfofallcasesofhearinglossareavoidablethrough
prevention,earlydiagnosis,andmanagementprocedures.3
Tomeetthedemandsofthispopulation,oneofthe
strate-giesofthehealthcare systemwasthecreationofaState
HearingHealthNetworkintheBrazilianUnifiedHealth
Sys-tem(SistemaÚnicodeSaúde---SUS),establishedby
Ministe-rialDecreeNo.587ofOctober7,2004,whichdeterminesthe
organizationandimplementationofactionsinprimarycare
bymediumandhigh-complexitycareservicesinthese
net-works.Theseactionsseektoofferanintegratedapproachto
care,hearinghealthpromotion,prevention,andearly
iden-tificationofhearingproblemsinthecommunity,aswellas
informationalandeducationalservices,familycounseling,
andreferralstotheHearingHealthService.4
Consideringtherecentprocessofcreationofthispolicy,
theevaluationofhealthinitiativesgainsimportanceinthe
sector,5asitprovidesrelevantinformationtotheprocessof
decision-makingbasedonevidence.6Onewaytounderstand
howtheseservicesareorganizedintheterritoriesof
health-careistousespatialanalysisoftheelementsthatcomprise
thecarenetwork,conductedbymeansofgeoprocessing,a
setoftechnologiesthatanalyzesandevaluatesinformation
regardingageographicalspacewithacertainobjective.7
For such purposes, it is necessary to establish the
geographicallocationofevents,associatinggraphical
infor-mation (maps) to the health database and using tools to
manipulate spatially presented information.8 Among the
many information systems, a geographic information
sys-tem(GIS)facilitatesthecollection,storage,manipulation,
analysis, visualization, and production of geographically
referenceddata,9 allowingthe qualificationand
organiza-tionof health services according to the particularities of
eachgeographicarea,10whichcontributestoabetter
under-standingofcurrenthealthproblems.
Geoprocessing techniques have been applied topublic
and collective health, as they allow analyzing the
asso-ciationsbetween environment and health-related events,
assistingtheplanning,monitoring,andevaluationofhealth
actionsandcontributingtothestructuringandanalysisof
environmentalrisks.8,11Moreover,theuseofsuchtechniques
aimstospatiallyidentifyareaswithspecificcharacteristics
inordertosubsidizeprogramsorpoliciesaimedat health
careimprovement, increasingtheefficiencyof theuse of
publicresourcesanddefiningpriorityareas.12
The present study aimed to analyze the organization
ofthe StateHearing HealthNetwork in thehealth
micro-regionsofthestate ofMinasGerais andassessthespatial
pattern between procedures of evaluation and diagnosis,
selection and adaptation of the individual sound
amplifi-cation device (ISAD), follow-up, and speech/audiological
therapyperformedathealthcareservices.
Methods
Thepresentstudyispartoftheproject‘‘Evaluationofthe
HearingHealthNetworkImplementation:Acasestudyofthe
micro-regionsof Sete Lagoas andCurvelo, MinasGerais’’,
fundedbytheFundac¸ãodeAmparoàPesquisadoEstadode
MinasGerais(FAPEMIG)andapprovedbytheEthics
Table1 Descriptionofproceduresconsideredforcalculationofthestudyvariables.
Code Proceduredescription
Variable1:Evaluationanddiagnosis
021107009-2 Evaluationforhearinglossdiagnosis.
021107010-6 Evaluationfordifferentialdiagnosisofhearinglossinpatientyoungerthan3 yearsorwithassociateddisorder.
Variable2:SelectionandadaptationofIndividualSoundAmplificationDevice(ISAD)
070103012-7 ExternalretroauriculartypeAISAD 070103013-5 ExternalretroauriculartypeBISAD 070103014-3 ExternalretroauriculartypeCISAD 070103003-8 Externalintra-auriculartypeAISAD 070103004-6 Externalintra-auriculartypeBISAD 070103005-4 Externalintra-auriculartypeCISAD 070103006-2 ExternalintracanaltypeAISAD 070103007-0 ExternalintracanaltypeBISAD 070103008-9 ExternalintracanaltypeCISAD 070103011-9 Externalmicro-canaltypeCISAD
070103001-1 ExternalconventionalboneconductiontypeAISAD 070103002-0 ExternalretroauricularboneconductiontypeAISAD 070103010-0 ExternalMicro-canaltypeBISAD
Variable3:Follow-up
021107029-7 Diagnosticreassessmentofhearinglossinpatientsolderthan3years. 021107030-0 Diagnosticreassessmentofhearinglossinpatientsyoungerthan3yearsor
withassociateddisorder.
030107003-2 Follow-upofpatientadaptedwithuni/bilateralISAD---adult/child.
Variable4:Speechandaudiologicaltherapy
030107011-3 Speechandaudiologicaltherapy
This is a cross-sectional analytical study using geopro-cessingtechniques. Datafromthe Outpatient Information System(SIA/SUS)were usedforthe constructionof varia-bles per health micro- and macro-region, considering the MasterPlanforRegionalizationofthestateofMinasGerais andthecityofresidenceofthenetworkusers.Thefollowing variableswereused:evaluationanddiagnosis,selectionand adaptationoftheISAD,follow-up,andspeech/audiological therapy for the year 2010 (Table 1), to allow the
assess-mentofthepatientsitineraryatthemainpointsofthecare
network.
Thesevariables weresubsequentlyconvertedinto
indi-cators by incorporating the relative population variation
totheoriginal data magnitude,using datafromthe 2010
censusbytheInstitutoBrasileirodeGeografiaeEstatística
(IBGE).Thevariablesrepresentedinchoroplethmapswere
comprehended fromsix classintervals defined bya
natu-ralbreaksdistribution,whichestablishestheintervallimits
usingactual breaks inthe histogram throughvisualization
by the researchers. After the representation of variables
asindexes(1000inhabitants/year),aspecificcartographic
representationoftheabsolutefrequency wasestablished.
Thismethodologicalprocedureusedfourclassintervals,also
definedbythemethodofnaturalbreaksdistribution.
Results
In2010,thestateofMinasGeraishad15accreditedHearing
HealthServices,distributedover14micro-regions,ofwhich
eightarehighlycomplexity(locatedinthemunicipalitiesof
BeloHorizonte,Uberlândia,Alfenas,PousoAlegre, Montes
Claros,GovernadorValadares,PonteNova,andJuizdeFora)
andseven aremediumcomplexity (locatedinthe
munici-palitiesofFormiga, SantaLuzia,Uberaba,PatosdeMinas,
Diamantina,andTeofiloOtoni).Allproceduresanalyzed in
allstatehealthmicro-regionswereperformed,althoughthe
frequencyofoccurrencewasnothomogeneousthroughout
theterritory,mainlywhencomparingthefourmomentsof
careprovidedtopatientsinthenetwork(fromdiagnosisto
speech/audiologicaltherapy)(Figs.1---4).
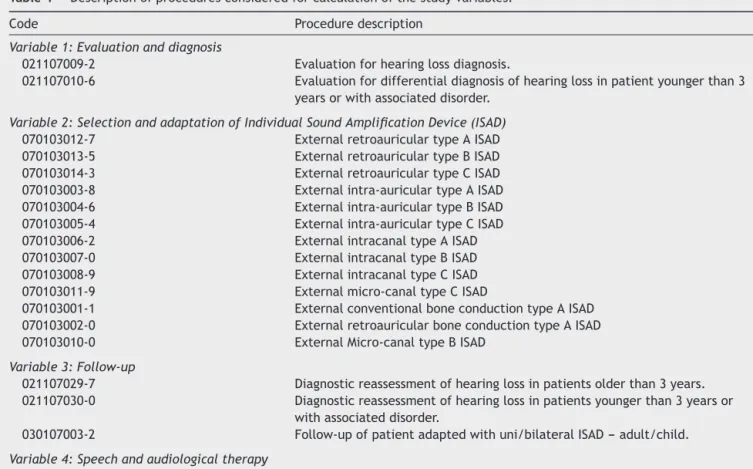
Thevariableevaluationanddiagnosisoccurredathigher
absolute frequency in the micro-regions of Belo
Hori-zonte/Nova Lima/Caeté, Juiz de Fora/Lima Duarte/Bom
JardimMinas,Uberlândia/Araguari,GovernadorValadares,
andPatosdeMinas,andthe lattertwoalsohada greater
number of individuals who underwent this procedure,
togetherwiththemicro-regionsofPonteNovaandVic¸osa.
Althoughitshowedahighervalueofabsolutefrequencyof
evaluationsand diagnoses, themicro-region of Belo
Hori-zonte/Nova Lima/Caetéwasindicated onthe mapasone
of themicro-regionswithlowervalue perpopulation that
performedsuchprocedures(Fig.1).
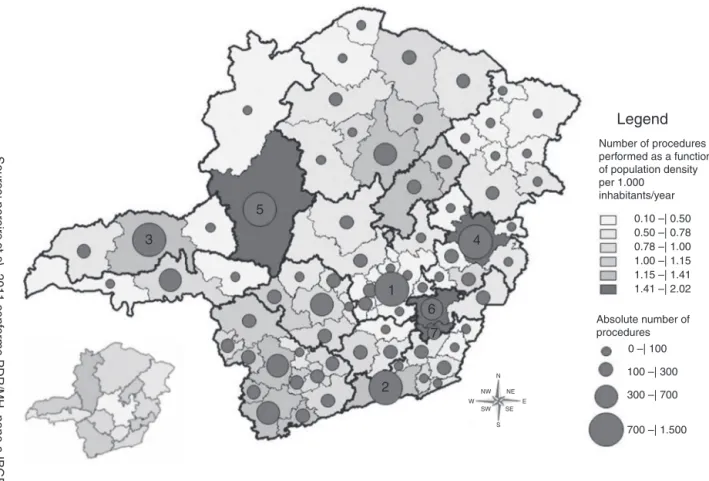
The spatial distribution of the procedure ‘‘selection
and adaptation of the ISAD’’ showed a higher number of
procedures as a function of population density per 1000
inhabitants in the micro-regions of Ponte Nova, Vic¸osa,
Formiga,Alfenas/Machado,Itajubá,GovernadorValadares,
Patos de Minas, Montes Claros/Bocaiúva, Pouso Alegre,
Number of procedures performed as a function of population density per 1.000
inhabitants/year
Absolute number of procedures
Source:
pereir
a
et al
, 2011 conf
or
me PDR/MH, nono e IBGE.
0 –| 100 0.10 –| 0.50 0.50 –| 0.78 0.78 –| 1.00 1.00 –| 1.15 1.15 –| 1.41 1.41 –| 2.02
N
NE E SE
S SW W
NW
100 –| 300
300 –| 700
700 –| 1.500
Legend
3
5
6 7
4
1
2
Figure 1 Spatial distributionaccording to micro-and macro-regionofthe ‘‘Assessmentand Diagnosis’’ procedure per 1000 inhabitants/yearandfrequency.
had higher absolute frequency value of this procedure.
In addition to the abovementioned, the micro-regions of
Belo Horizonte/Nova Lima/Caeté and Juiz de Fora/Lima
Duarte/BomJardimMinasshowedahighabsolutefrequency
value for selection and adaptation of ISAD performed in
2010. Ahigher numberper 1000 inhabitants andabsolute
frequency of this procedure was observed between the
micro-regionswhencomparedtothevariableevaluationand
diagnosis(Fig.2).
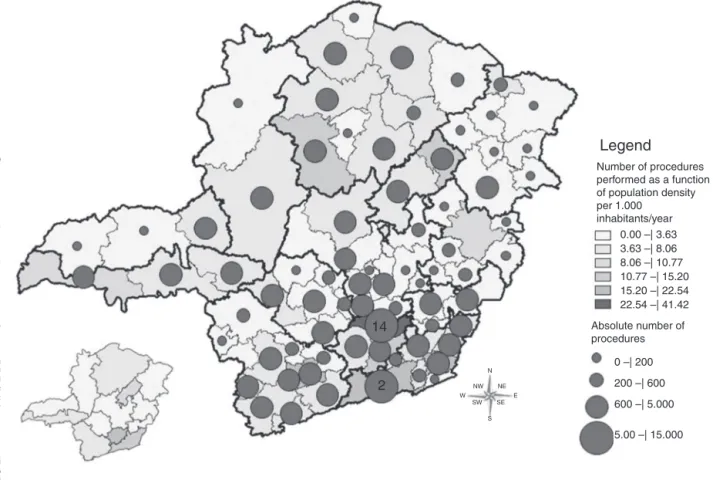
The follow-up procedure occurredat the highest
abso-lute frequency in the regions of Belo Horizonte/Nova
Lima/Caeté,JuizdeFora/LimaDuarte/BomJardimMinas,
and Pouso Alegre, whereas the micro-regions of Itajubá,
PocosdeCaldas,andPousoAlegreshowedhighervalueper
populationsubmittedtosuchprocedure.The map
demon-strated large areaswithlow production of thisprocedure
per1000inhabitants,aswellaslowvaluesofabsolute
fre-quency of this procedure, with this variable showing the
lowestoccurrenceinthestate(Fig.3).
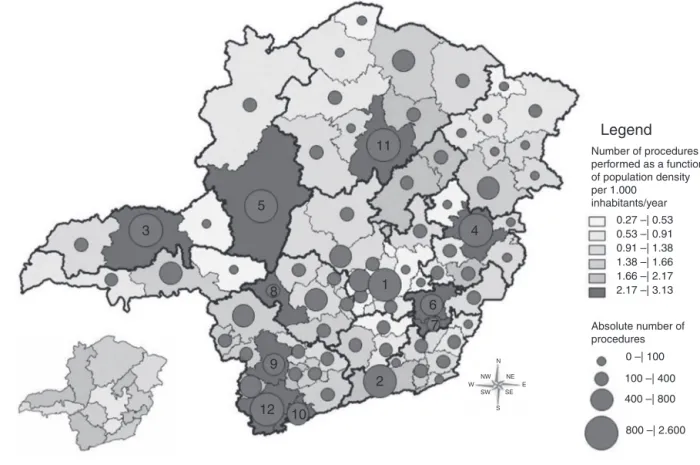
The speech/audiological therapy procedure occurred
at greater absolute numbers in the regions of Juiz de
Fora/LimaDuarte/BomJardimMinasandConselheiro
Lafai-ete/Congonhas,withthelatterbeingtheonlymicro-region
highlightedperpopulation.The mapshowedthatthis
pro-cedureoccurredatgreatestfrequencyper1000inhabitants,
anditsmaximumvaluewas41.42speech/audiological
ther-apysessions/1000inhabitants(Fig.4).
A directly proportional association was not observed
betweentheabsolutenumberofproceduresoftheanalyzed
variablesand the number of procedures per 1000
inhabi-tants,i.e.,thehealthregionswithhigherproductionrelated
tothevariablesdidnotnecessarilyhaveahighernumberof
proceduresin relation topopulation. Moreover,no
micro-regionwashighlightedregardingallanalyzedvariables.
Tables2and3showtheminimum,maximum,mean,and
standard deviation values for each analyzed variableand
theirrespectivemicro-region of occurrenceregarding the
numberof proceduresasa functionof population density
per1000inhabitants/yearandtheabsolutenumberof
pro-cedures,respectively.
Discussion
Albeitheterogeneously, allproceduresrelatedtothefour
momentsofthehearinghealthcareservicewereperformed
in users residing in all health micro-regions of the state.
TheprincipleofSUSregionalizationguaranteesthathealth
servicesareorganizedintolevelsofincreasing
technologi-calcomplexity,arrangedinadelimitedgeographicareaand
aimedata populationtobetreated.13 Thus,usersshould
findsecondarycareserviceswithinthemicro-region
corre-spondingtothemunicipalityofresidence.14
Althoughallthehealthmicro-regionsdemonstrated
pro-duction, none showed significant production values per
populationatthefourmomentsofcaretoindividualswith
hearingloss,asshowninFigs.1---4.Thismayindicatethat
Number of procedures performed as a function of population density per 1.000
inhabitants/year
Absolute number of procedures
Source:
pereir
a
et al
, 2011 conf
or
me PDR/MH, nono e IBGE.
0 –| 100 0.27 –| 0.53 0.53 –| 0.91 0.91 –| 1.38 1.38 –| 1.66 1.66 –| 2.17 2.17 –| 3.13
N
NE E SE
S SW W
NW 100 –| 400
400 –| 800
800 –| 2.600
Legend
3
5
8
9
12 10
6 7
4
1 11
2
Figure2 Spatialdistributionaccordingtomicro-andmacro-regionofthe‘‘SelectionandAdaptationofISAD’’procedureper 1000inhab./yearandfrequency.
Number of procedures performed as a function of population density per 1.000 inhabitants/year
Absolute number of procedures
Source:
pereir
a
et al
, 2011 conf
or
me PDR/MH, nono e IBGE.
0 –| 100 0.02 –| 0.17 0.17 –| 0.36 0.36 –| 0.51 0.51 –| 0.82 0.82 –| 1.40 1.40 –| 2.11
N
NE E SE
S SW W
NW 100 –| 400
400 –| 800
800 –| 1.200
Legend
12 10 13
1
2
Number of procedures performed as a function of population density per 1.000
inhabitants/year
Absolute number of procedures
Source:
pereir
a
et al
, 2011 conf
or
me PDR/MH, nono e IBGE.
0 –| 200 0.00 –| 3.63 3.63 –| 8.06 8.06 –| 10.77 10.77 –| 15.20 15.20 –| 22.54 22.54 –| 41.42
N
NE E SE
S SW W
NW 200 –| 600
600 –| 5.000
5.00 –| 15.000
Legend
14
2
Figure4 Spatialdistributionaccording tomicro- andmacro-regionofthe‘‘Follow-up’’procedure for 1000inhab./year and frequency.
Table2 Minimum,maximum, mean,andstandarddeviationvaluesasafunction ofthenumber ofproceduresperformed consideringthedemographicdensityof1000inhabitants/yearinthestateofMinasGerais.
Variable Micro-region
(minimumvalue)
Micro-region (maximumvalue)
Mean SD
Evaluationanddiagnosis PedraAzul(0.10) GovernadorValadares(2.02) 0.74 0.41 Selectionandadaptation PedraAzul(0.27) PatosdeMinas(3.13) 1.27 0.67 Follow-up Alfenas/MachadoeTrês
Pontas(0.02)
PousoAlegre(2.11) 0.38 0.42
Speechandaudiological therapy
Itabira.Vespasiano.Unaí eItuiutaba(0.00)
Conselheiro
Lafaiete/Congonhas(41.42)
5.29 6.42
SD,standarddeviation.
Table 3 Minimum, maximum, mean, andstandard deviation values as a function of the absolute number ofprocedures performedinthestateofMinasGerais.
Variable Micro-region
(minimumvalue)
Micro-region (maximumvalue)
Mean SD
Evaluationanddiagnosis PedraAzul(5) BeloHorizonte/Nova Lima/Caeté(1453)
199.32 251.04
Selectionandadaptation PedraAzul(14) BeloHorizonte/Nova Lima/Caeté(2549)
338.55 428.41
Follow-up TrêsPontas(3) BeloHorizonte/Nova Lima/Caeté(1143)
112.03 211.79
Speechandaudiologicaltherapy Itabira,Vespasiano,Unaí eItuiutaba(0)
JuizdeFora/LimaDuarte/Bom JardimdeMinas(14410)
1337.68 2276.50
ofthestatemicro-regionsasrecommendedbythe Ministe-rialDecreeNo.587ofOctober 7,2004.The formusedby healthmanagersforthepurposeofaccreditationofMiddle and High-Complexity Audiology services4 evaluates
struc-turalissuesthatcanbeenoughforqualificationofcenters,
but can lead to erroneous conclusions when used as the
soleinstrumentforaccreditationofexistingservices,asthis
formdoesnotevaluatetheserviceperformanceintermsof
providingtheserviceandthedemandfortheserviceinthe
micro-region.Thus,thereitisnecessarytoestablish
objec-tiveindicatorstoassessthelevelofimplementationofthe
HearingHealthNetworkinthestatemicro-regions.
Although in 2010 the micro-region of Belo
Hori-zonte/NovaLima/Caetéwastheonlycenterthat hadtwo
hearinghealthcareservicesthatwereaccreditedand
asso-ciatedtoeducationalinstitutions.Thismicro-regionshowed
low values per population submitted to the procedure of
assessmentanddiagnosis,incomparisontotheother
micro-regions.
Theincreaseintheuseofhealthservicesmayberelated
toincreasedsupply,15,16whichmakespossibletheexistence
of pent-up demands and needs suppressed by insufficient
supplyofpublichealthactionsandservices.Thesedata
sug-gesttheexistenceofapent-updemandandaninadequate
supplyofservices,consideringthepopulationof3,186,312
inhabitantswhichwasencompassedbythismicro-regionin
2010.
The micro-regions highlighted asthosewiththehigher
absolutenumberofevaluationanddiagnosis,selectionand
adaptation of ISAD, and follow-up procedures are
micro-regions that have middle- or high-complexity accredited
Hearing Health Services, which may be due to easier
accessofusersconsideringtheshortestdistancesfromthe
residence to the service. It is the responsibility of the
municipalitytoensureaccessofusersundergoingoutpatient
treatmenttootherlocations,whenthemunicipalityof
ori-gindoesnotofferthedegreeofcomplexityrequiredbythe
user.13
However,the Health Care StateTransportation System
(SETS) offered by the Health Secretariat of Minas Gerais
covered only 21 (27.63%) of the 76 micro-regions of the
Statein 2009. In 2010, it waspredicted that 41 (53.94%)
ofthemicro-regionswouldbecoveredbytheSETS,17which
canmakeitdifficultorevenimpossibleforuserstoaccess
HearingHealthCareservices.Onlythespeech/audiological
therapyprocedurewasalsohighlightedinthemicro-region
of Conselheiro Lafaiete/Congonhas, which does not have
accreditation for this service. However, this fact is
justi-fied by the availability of speech/audiological therapy in
a decentralized manner, which can be performed by the
MunicipalHearingHealthReferrals.18
ThehigherfrequencyofselectionsandadaptationofISAD
procedureinrelationtotheevaluationanddiagnosis
proce-durecanbejustifiedconsideringthat themostuserswith
hearingloss undergo binaural ISAD adaptation, and so,in
thesecases,theprocedureisconsideredtwiceforthesame
individual,whereastheassessmentanddiagnosisprocedure
isconsideredonlyonce,regardlesswhetherhearinglossis
unilateralorbilateral.
However,theconfirmationofthishypothesisisnot
pos-sible,as the dataprovided in the Outpatient Information
System show no separation regarding the selection and
adaptationofmonauralorbinauralISADperuser.
Addition-ally,thereisalsothepossibilitythattheuserwillundergo
the evaluation and diagnosis procedure through a private
healthcareservice/insuranceorprivateconsultations,with
interpositionofuserswhouse publicandprivateservices,
asis thecase of thosepatients whoseekthe health care
centeronlytoundergovaccinations,accordingtotheir
pri-vate physician’s indication, but when they need medical
consultationsorexaminationsfordiagnosisandtherapeutic
support,theyusetheirhealthinsurance.19
Thisstudyshowedthatfollow-upistheprocedurewith
the lowest occurrence in the state. Patient follow-up is
essentialfortheeffectiveuseofISADandconsequent
suc-cessinitsadaptation,20 whichbecomesfeasiblebymeans
of periodic returns to the Hearing Health Program,
aim-ing to monitor hearing loss and verify effectiveness of
the ISAD use.4 It has been observed that outpatient
vis-its related to patient follow-up have decreased over the
years,21 withlowerspontaneousratesofreturnfor
follow-up than the abandonment rates of the Health Hearing
Program.22
Lowpatientadherencetotheauditoryrehabilitation
pro-cess can bethe resultby several factors, suchaslack of
awarenessaboutthefactthatadaptationtotheISADisonly
one stepinthe process,or thedifficulty of accesstothe
service,incasesofpatientswhoneedtoundergotreatment
at a service outside the city of residence.23 Additionally,
thefollow-upprocedureshouldoccuratleastonceayear;
therefore,itisexpectedthatitwouldoccurathigher
abso-lutefrequency andinalargernumberofthepopulation.4
Althoughitisnotsufficient,theactivesearchforusersofthe
HearingHealthServiceforreturnconsultationsand
follow-upprocedureshasbeenshowntobeeffective22andcanbe
analternativetoincreaseserviceadherence.
Incontrasttothelownumberoffollow-upproceduresin
thestate,itwasobservedthatspeech/audiologicaltherapy
occursfrequentlyinalltheregions,whichisalsoobserved
atthenationallevel,where61.77%oftheperformed
proce-duresrefertospeech/audiologicaltherapy,withadecrease
inoutpatientservicesrelatedtofollow-upobservedoverthe
years.21
Thehighvalueofoccurrenceperabsolutefrequencyand
perpopulationofthisprocedureisjustifiedbythefactthat
speech/audiological therapy can be indicated more than
once,takingintoaccounttheindividualcharacteristicsand
needsoftheuser,andalsoduetothepossibilityof
perform-ingthisprocedureaccordingtotheHearingHealthMunicipal
References,18 whichreducespotentialdifficultiesofaccess
to the service. Such justificationsalso explain the higher
valueofthisprocedureinrelationtoother evaluated
pro-cedures.
Severalfactors,suchasaccess,pent-updemand,and
dif-ficultyoftreatmentadherence,amongotherfactors,seem
toinfluencethewayexistingservicesareusedbythe
popu-lation.Thesefactspointstotheneedtobetterunderstand
theassociationamongthesefactorsandtheuseofhearing
healthservices,aswellastodefineprocessindicatorsthat
allowmonitoringandevaluationofthenetwork
implemen-tationprocessinthestate.
Itis necessarytoconduct furtherevaluationstudies of
the Hearing Health Network, both at the state and the
requiregreaterresourcestooptimizethenetworkand
con-sequently,improvequalityoflifeofthepopulation.
Conclusions
Theassessmentanddiagnosis,selection andadaptationof
hearingaids,monitoring,andspeechtherapy/audiology
pro-ceduresofferedbyHearingHealthNetworkwereperformed
in allregions ofthe state, withspeech/audiological
ther-apyandfollow-upproceduresrepresentingthemostandthe
leastoftenperformed,respectively.Therewasalackof
sys-tematicspatialdistributionpatternbetweentheprocedures
inthehealthcaremicro-regionsatthefourmomentsofcare
offered to individuals with hearing impairment. Although
hearinghealthservicesareavailable,accordingtothe
orga-nizationalpolicyofregionalization,theuseofthisnetwork
stillshowsveryheterogeneouspatternswhencomparingthe
healthmicro-regionsinthestate.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
We would like to thank Fundac¸ão de Amparo à Pesquisa
do Estado de Minas Gerais (FAPEMIG) for the financial
support for the development of the project ‘‘Evaluation
of Hearing Health Network implementation: A case
study of the micro-regions of Sete Lagoas and Curvelo,
Minas Gerais’’, process: A PQ-03622-10, Edict: PPSUS
MS/CNPq/FAPEMIG/SES2008---2009.
References
1.Butugan O, Santoro PP, Rezende E, Silveira JA, Medicis JA, Grasel SS. Diagnóstico precoce da deficiência auditiva no primeiro ano de vida de crianc¸as com alto risco através de audiometria de tronco cerebral. Pediatria (Santiago). 2000;22:115---22.
2.Reis ATPS, Silva FGF, Farias RB. Perfil epidemiológico dos pacientesatendidosnocentroauditivodePetrolina---PE.Rev CEFAC.2012;14:79---83.
3.World Health Organization. Deafness and hearing impair-ment;2006.Availablefromhttp://www.who.int/mediacentre/ factsheets/fs300/en/index.html[accessed14.11.11]. 4.PupoAC,MendesBCA,ManzoniCRCT,LewisDR,MachadoMAMP,
MartinezMANS,etal.Guiadeorientac¸ãoparafonoaudiólogos sobreaimplantac¸ãoedesenvolvimentodasaúdeauditivana atenc¸ãoprimária.ConselhoFederaldeFonoaudiologia.2011. 5.BosiMLM, UchimuraKY. Avaliac¸ãodaqualidadeouavaliac¸ão
qualitativa do cuidado em saúde? Rev Saúde Publica. 2007;41:150---3.
6.Soárez PC, Padovan JL, Ciconelli RM. Indicadores de saúde no Brasil: um processo em construc¸ão. Rev Adm Saúde. 2005;7:57---64.
7.BarcellosC,RamalhoWM,GracieR,MagalhãesMAFM,Fontes MP,SkabaD.Georreferenciamentodedadosdesaúdenaescala submunicipal:algumas experiências noBrasil.EpidemolServ Saúde.2008;17:59---70.
8.HauLC,NascimentoLFC,TomaziniJE.Geoprocessamentopara identificarpadrõesdeperfildenascimentosnaregiãodoVale doParaíba.RevBrasGinecolObstet.2009;31:171---6.
9.GrahamAJ,AtkinsonPM,DansonFM.Spatialanalysisfor epi-demiology.ActaTrop.2004;91:219---25.
10.BonfimC,MedeirosZ.Epidemiologiaegeografia:dos primór-dios ao geoprocessamento. Rev Espac¸o apara a Saúde. 2008;10:53---62.
11.CamaraG,MonteiroAMV.Geocomputationtechniquesfor spa-tial analisys: are they relevant to health data? Cad Saúde Pública.2001;17:1059---81.
12.HayesMV.Ontheepistemologyofrisk:language,logicandsocial science.SocSciMed.1992;35:401---7.
13.ConselhoNacionaldeSecretáriosdeSaúde---Brasil.Legislac¸ão do SUS/Conselho Nacionalde Secretáriosde Saúde. Brasília: CONASS;2003.
14.PlanoDiretordeRegionalizac¸ãodeMinasGerais---Brasil,2010. Available from: http://www.saude.mg.gov.br/politicasde saude/plano-diretor-de-regionalizacao-pdr [accessed 14.05.12].
15.OliveiraEXG,Travassos C,CarvalhoMS.Acessoà internac¸ão hospitalar nos municípios brasileiros em 2000: territórios do Sistema Único de Saúde. Cad Saude Publica. 2004;20 Supl.2:298---309.
16.Castro MSM, Travassos C, Carvalho MS. Efeito da oferta de servic¸osdesaúdenousodeinternac¸õeshospitalaresnoBrasil. RevSaudePublica.2005;39:277---84.
17.Borges JF. As redes de protec¸ão social e a reduc¸ão das desigualdadesregionaisemMinasGerais.In:BrandãoE,editor. Reduc¸ãodasdesigualdadesregionais:umadasfacesdochoque degestão.BeloHorizonte:SEVAN/IDENE;2009.Availablefrom: http://www.bibliotecaidene.org/arquivos/album/381/arq
2535.pdf[accessed14.05.12].
18.Minas Gerais. Ministério da Saúde, Secretaria de Atenc¸ão à Saúde. Resoluc¸ãoSES n◦1669de 19de novembro de2008
---AprovaofluxodeinclusãonaRedeEstadualdeSaúdeAuditiva deMinasGeraisedefineatribuic¸õesdoFonoaudiólogo Descen-tralizado,daJuntadeSaúdeAuditivaMicrorregionaledaJunta ReguladoradaSaúdeAuditiva.Brasília,DF;2008.
19.AssisMMA,VillaTCS,NascimentoMAA.Acessoaosservic¸osde saúde: uma possibilidade a ser construída naprática. Ciênc SaúdeColetiva.2003;8:815---23.
20.Ribas A, Rosa M, Dante G, Martins-Bassetto J. SOS prótese auditiva: relato de um estudo de caso realizado na clínica de fonoaudiologia da UTP. Ciência e Cultura. 2006;38: 9---18.
21.BevilacquaMC,MorettinM,MeloTM,AmantiniRCB,Martinez MANS.Contribuic¸õesparaanálisedapolíticadesaúdeauditiva noBrasil.RevSocBrasFonoaudiol.2011;16:252---9.
22.Lanzetta BP, Frota S, Goldfeld M. Acompanhamento da adaptac¸ãodeprótesesauditivasemcrianc¸assurdas.RevCEFAC. 2010;12:360---70.