www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Imbalance
in
the
diurnal
salivary
testosterone/cortisol
ratio
in
men
with
severe
obstructive
sleep
apnea:
an
observational
study
夽
Cristina
Mihaela
Ghiciuc
a,1,
Lucia
Corina
Dima-Cozma
b,1,
Raluca
Mihaela
Bercea
c,1,
Catalina
Elena
Lupusoru
a,
Traian
Mihaescu
c,
Sebastian
Cozma
d,
Francesca
Romana
Patacchioli
e,∗aUniversityofMedicineandPharmacyGrigoreT.Popa,DepartmentofPharmacology,Iasi,Romania
bUniversityofMedicineandPharmacyGrigoreT.Popa,SchoolofMedicine,DepartmentofInternalMedicine,
Iasi,Romania
cUniversityofMedicineandPharmacyGrigoreT.Popa,ClinicofPulmonaryDiseases,Iasi,Romania dUniversityofMedicineandPharmacyGrigoreT.Popa,DepartmentofOtorhinolaryngology,Iasi,Romania eSapienzaUniversityofRome,DepartmentofPhysiologyandPharmacology‘‘V.Erspamer’’,Rome,Italy
Received24June2015;accepted8September2015 Availableonline17December2015
KEYWORDS
Obstructivesleep apnea;
Saliva; Cortisol; Testosterone
Abstract
Introduction:Thecomplexrelationshipbetweensleepdisordersandhormonescouldlead to
alterations inthe productionofcortisol and testosteroneinobstructive sleep apnea (OSA)
patients.
Objective: Thepurposeofthisstudywastodeterminethediurnaltrajectoriesofsalivary
free-testosterone,free-cortisolandtheirratio(T/C).
Methods:TensubjectsnewlydiagnosedwithOSA,basedonnocturnalpolysomnography
eval-uation and excessive daytime sleepiness, and seven matched controls were consecutively
recruited.Cortisolandtestosteroneweremeasuredinsalivarysamplescollectedupon
awaken-ing,atnoonandintheevening.Thepsychometricevaluationofanxiety/depressionandreferred
sexualfunction disturbanceswasperformedtoevaluatethepresenceofneuropsychological
comorbidities.
夽 Pleasecitethisarticleas:GhiciucCM,Dima-CozmaLC,BerceaRM,LupusoruCE,MihaescuT,CozmaS,etal.Imbalanceinthe
diur-nal salivary testosterone/cortisolratio in men withsevere obstructive sleepapnea: anobservational study. Braz JOtorhinolaryngol. 2016;82:529---35.
∗Correspondingauthor.
E-mail:[email protected](F.R.Patacchioli). 1 Theseauthorscontributedequallytothiswork.
http://dx.doi.org/10.1016/j.bjorl.2015.09.004
Resultsandconclusion: ThemainfindingwasthatOSAsubjectsdisplayedhypocortisolismupon
awakeningandasignificantreductionintestosteroneconcentrationintheeveningin
compar-isonwiththecontrolgroup,whichhasmaintainedthephysiologicaltestosteroneandcortisol
diurnalfluctuation,withhigherhormoneconcentrationsinthemorningandlower
concentra-tionsintheevening.Theuseofdatafrommultiplediurnalmeasurementsratherthanasingle
pointallowedthedetectionofT/Cratiochangesofoppositesignsatthebeginningandendof
theday:theOSAsubjectshadahigherT/Cratiothanthecontrolsinthemorning,whiletheir
T/Cratiowassignificantlylowerthanthatofthecontrolsintheevening.Theimbalancesin
theanabolic-catabolicdiurnalequilibriumsuggestthatOSAisassociatedwithadysregulation
ofthehypothalamic---pituitary---adrenalandhypothalamic---pituitary---gonadalaxes,potentially
anunderlyingcauseofsomeoftheneuropsychologicalcomorbiditiesobservedinOSApatients.
© 2015 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published
by Elsevier Editora Ltda. This is an open access article under the CC BY license (http://
creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE
Apneiaobstrutiva dosono;
Saliva; Cortisol; Testosterona
Desequilíbrionaproporc¸ãosalivardiurnadetestosterona/cortisolemhomens comapneiaobstrutivadosonograve:umestudoobservacional
Resumo
Introduc¸ão:A relac¸ão complexa entre os distúrbios do sono e os hormônios pode levar a
alterac¸õesnaproduc¸ãodecortisoletestosteronaempacientescomApneiaobstrutivadosono
(AOS).
Objetivo:Oobjetivodesteestudofoideterminarascurvasdiurnasdetestosteronaecortisol
livresnasalivaesuaproporc¸ão(razãoT/C).
Método: Dezindivíduosrecém-diagnosticadoscomAOScombasenaavaliac¸ãopor
polissono-grafia noturna e sonolência diurna excessiva e sete controles pareados foram recrutados,
consecutivamente.Cortisoletestosteronaforammedidosemamostrasdesalivacoletadasao
acordar,aomeio-diaeànoite.Aavaliac¸ãopsicométricadosdistúrbiosdeansiedade/depressão
efunc¸ãosexualmencionadosfoirealizadaparadetectarapresenc¸adecomorbidades
neurop-sicológicas.
Resultados: OachadoprincipalfoiqueosindivíduoscomAOSapresentamhipocortisolismoao
acordareumareduc¸ãosignificantenaconcentrac¸ãodetestosteronaànoite,emcomparac¸ão
comogrupo controle, quemanteve avariac¸ãofisiológica diurna detestosterona e cortisol
comconcentrac¸õeshormonaismaiselevadaspelamanhãeconcentrac¸õesmaisbaixasdurante
anoite.Ousodedadosde váriasmensurac¸ões diurnas,em vezdeuma únicamensurac¸ão,
permitiudetectar asalterac¸ões narazão T/Cdesinais opostos noinícioe nofinal dodia:
osindivíduos comAOS apresentaram razãoT/Cmaiorqueoscontrolesnapartedamanhã,
enquantoquearazãoT/Cfoisignificantementeinferioràdoscontrolesduranteanoite.
Conclusão:Osdesequilíbriosnobalanc¸oanabólico-catabólicodiurnosugeremqueaAOSestá
associada auma desregulac¸ão dos eixoshipotálamo-hipófise-adrenal e
hipotálamo-hipófise-gonadal,potencialmenteacausasubjacentedealgumasdascomorbidadesneuropsicológicas
observadasempacientescomAOS.
© 2015 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado
por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http://
creativecommons.org/licenses/by/4.0/).
Introduction
Obstructive sleep apnea (OSA) is a chronic respiratory disturbance that can be diagnosed with an overnight polysomnography(PSG).Itisaserioushealthproblemwith prevalence greater than 26% in the general middle-aged population.1---3
Excessive daytime sleepiness and snoring are often associated with neuropsychological symptoms, includ-ing concentration difficulties and cognitive disturbances. Hypoxia,sleep fragmentation,obesity, and ageing in OSA
patientswerefoundtobeassociatedwithlowserum testos-terone levels.Luboshitzkyet al.4 demonstratedthat men
withsleepapneahaddecreasedlevelsoftestosteroneand luteinizinghormoneduringnightlysleep,whichispossibly causedbythecombinedeffectsofhypoxiaandsleep frag-mentation.Morerecently,Berceaandco-workersreported thatthemorningserumtestosteroneconcentrationinobese patientswithsevereOSAwasassociatedwithincreased anx-iety/depressionandsleepefficiencydisturbances.5
could lead toalterations in the production of cortisol.6---9
Testosterone and cortisol, major end products of the hypothalamic---pituitary---gonadal (HPG) axis and the HPA axis, respectively, are part of a biological balance that modulatespsychologicallyandphysicallyintegratedhuman responses.Theinterrelationshipbetweensexandstress hor-mones has been extensively investigated in the context ofsports medicineby measuringthe testosterone/cortisol (T/C) ratio as a marker of anabolic/catabolic activities connectedwithathleteperformanceandovertraining.10---11
Furthermore,theT/Cratiohasbeenproposedasahormonal markerofpsychopathologies,12,13andaspecificassociation
betweenareductionoftheT/Cratioandischemicdisease hasalsobeenreported.14
The purposeofthisstudywastodeterminethediurnal fluctuation of salivary free-testosterone (T) and free-cortisol(C)andtostudytheirinterrelationshipbymeasuring diurnal variationsintheT/C ratioofpatients withsevere OSA. This analysis will expand upon previous studies that providedonlypartialdatafromsingle-pointhormonal mea-surements.
Interestingly,sexhormoneimbalanceisoftenassociated withdepressiveand anxiousmood disordersin men15 and
bidirectionallyinteractswitherectilefunction.16Therefore,
toassessthepresenceofcomorbidities,theHamilton Inven-toryQuestionnairesforDepression(HDS)andAnxiety(HAS) andtheInternationalIndexforErectileFunction(IIEF) ques-tionnairewereadministeredtothestudypopulation.
Materials
and
methods
Studypopulation
This prospective study was conducted over 6 months betweenMay 2011andDecember2012 intheSleep Labo-ratoryintheClinicofPulmonary Diseases(Iasi,Romania). ThestudywasformallyapprovedbythelocalEthics Commit-tee(Protocoln◦14,April29th,2011).AllCaucasiansubjects
wererecruitedamongpatientsvisitingtheCentreforSleep Disturbancesandprovided theirwritten informedconsent beforethestartofthestudy.
We previously estimated that at least 14 subjects (7 per group) were required to detect a mean absolute dif-ferencecorrespondingtoa 50%variationontheexpected peakof T/C ratioin healthy subjects(40.00±20.00 arbi-trary unit) witha two-tailed ˛of 0.05 and 80% of power analyses.Thus,10patients(OSAgroup)wereselectedbased onthefollowinginclusioncriteria:male, 40---60yearsold, non-smoker,withbodymassindex(BMI)>30kg/m2(obese)
and newly diagnosed with severe OSA based on noctur-nal polysomnography (PSG) evaluation (apnea-hypoapnea index, AHI≥30h−1) and excessive daytime sleepiness
(EpworthSleepinessScale,ESS≥10).17 Theexclusion
crite-ria included the following: acute or chronic associated diseases,smoking,useofanychronicmedicationand non-cooperative attitude. Patients with suspected OSA were hospitalized for 4 consecutive days. On the morning of admittance,bloodsampleswerecollectedfor biochemical-hematological parameter determinations, and pulmonary functionassessment (spirometry)and psychometric evalu-ationswiththeHamiltonRatingScaleforDepression,18with
theHamiltonAnxietyRatingScaleandwiththeInternational Index Erectile Function questionnaire (IIEF)19 were
per-formed.Abaselinerestingelectrocardiogram(ECG),heart rate(HR)(BTL-08USA)andsystolicanddiastolicblood pres-sure were recorded (M3 --- Omron, Japan). Conventional
sleep recordings (SOMNOlab V2.01, Weinmann, Germany) were obtained from 10:00 pm to 7:00 am (day 2) and AHI,arterial oxygensaturation (SpO2),desaturationindex
(ODI)andmicroarousalindex,werescoredapplyingstandard criteria.20AccordingtoAmericanAcademyofSleepMedicine
2007,theAHIwascalculatedasthemeannumberofapneas plushypopneasperhourofsleep;apneaswerescoredwhen theabsenceofairflowwaslastingatleast10sand hypop-neas whenthere wasat least a 30% drop in the oronasal airflow,withcoincidentoxygendesaturationofatleast4%, lastingatleast10s.7,20
Theparticipantswereinstructedonhowtocollectsaliva andaskedtoavoid food,coffeeandalcohol consumption, teethbrushingandanyphysicalexerciseforatleast30min beforeeachsalivacollection.21 Thus,onthedayafter(day
3),salivawascollecteduponawakening(between6:30hand 7:30h),atnoon(beforelunch)andintheeveningat19:00h beforedinner,for measuringthe dailycortisoland testos-teronefluctuation. The exacttimeof salivasampling was monitoredbyastaffmember.Amongthepatients hospital-izedwithsuspectedOSA,weselected7adultmalesubjects forthecontrolgroupwhohadthesamesomatic characteris-ticsoftheOSAsubjectsbutdidnotsufferfromsleepapnea (AHI<5h−1,ESS<10).
Salivarysamplingprocedure,testosteroneand cortisolassay
Saliva was collected using the Salivette (Sarstedt, Italy) samplingdevice,whichallowsforquickandhygienicsaliva recoverythroughcentrifugationat3000rpmfor15min.22
For each sample, duplicate measurements were per-formed for the direct assay of testosterone on 100L of saliva (inter-assay coefficient of variation was <10%, and intra-assay coefficient of variation <7% with a minimum detectable concentration of 3.5pg/mL at the 95% confi-dencelimitusingcommercialimmunoenzymatickitsandfor thedirect assayof cortisolon25Lof saliva (inter-assay coefficientofvariationwas<10%,andintra-assaycoefficient ofvariation<7%withaminimumdetectableconcentration of0.5ng/mLatthe95%confidencelimit(Diametra,Italy).
Dataanalysis
Alldatawerereportedasthe mean±SEM. The statistical
analyseswereperformed andthe graphicswereproduced using the SigmaPlot 11 software package (SxST.it, Italy). Normal distribution of the data was tested using the Kolmogorov---Smirnovtest.Whereappropriate,Student’st -test or the Mann---Whitney Utest was usedas parametric andnon-parametrictests,respectively,forthecomparisons betweengroups.
Table1 Somatic,polysomnographic,andpsychometricvariablesinthestudypopulation.
Control(n=7) OSA(n=10) Statistics p-Value
Age(years) 51±3 53±3 T=58.000 0.66
BMI(kg/m2) 32.2±0.6 32.3±0.7 T=69.000 0.591
Waistcircumference(cm) 105±2 109±2 t=−1.623 0.125
Polysomnographyparameters
AHI(h−1) 2.57±0.48 63.5±9.3 T=28.000 <0.001
MinimumSpO2(%) 87.6±1.49 68.5±4.27 T=95.000 0.002
ODI(h-1) 4.86±0.83 58.4±9.35 T=28.000 <0.001
Sleepduration(min) 419.3±8.5 395.3±7.5 t=2.088 0.054
Sleepefficiency(%) 79.9±0.7 78.6±0.7 t=1.370 0.191
Microarousal(h-1) 9.9±0.94 46.7±6.31 T=28.000 <0.001
ESS 4.0±0.83 12.9±1.23 t=−4.910 <0.001
SystemicbloodpressureandHR
SBP(mmHg) 117±3 127±2 t=−2.744 <0.05
DBP(mmHg) 69±4 76±2 t=−1.657 0.118
Heartrate(beats/min) 67±1 75±2 T=48.000 0.156
Psychometricscores
HDS 5±1 10±0.54 t=−5.073 <0.001
HAS 2±1 5.3±1 T=38.000 <0.05
EF 27.9±0.7 16.0±0.9 T=98.000 <0.001
OF 9.0±0.2 6.9±0.3 T=97.000 <0.001
SD 9.1±0.1 6.9±0.2 T=98.000 <0.001
IS 14.0±0.2 6.5±0.2 t=18.190 <0.001
OS 10.0±0 8.5±0.2 T=98.000 <0.001
Dataareexpressedasthemean±SEM.BMI,bodymassindex;AHI,apnea-hypopneaindex;minimumSpO2,minimumoxygensaturation; ODI,oxygendesaturationindex;ESS,EpworthSleepinessScale;SBP,systolicbloodpressure;DBP,diastolicbloodpressure;HDS,Hamilton DepressionScore;HAS,HamiltonAnxietyScore;EF,erectilefunction,OF,orgasmicfunction;SD,sexualdesire;IS,intercoursesatisfaction; OS,overallsatisfaction.
T,C,and theT/C ratiomeasured in both groups at 7:00, 12:00,and19:00onthesamplingday.
Theareaunderthecurve(AUC)wascalculatedfromthe AUCdeterminedforeachsubjectbythetrapezoidalmethod usingthethreesalivarytestosteronevaluesmeasuredduring thesamplingday(morning,noon,andevening).23
Statisticalsignificancewassetatp<0.05.
Results
Characteristicsofthestudypopulation
As reportedin Table1, thetwogroups were matched for age,and there wereno significant differences in theBMI values;themeanwaistsizewassimilarforbothgroupsand washoweverabovethenormalrangeformen.
Theresultsofthepulmonaryfunctiontests(spirometry), forcedexpiratoryvolume(FEV),andvitalcapacity(FEV/VC ratio)were withinthe normal limits for subjects in both groups (data not reported). As shown in Table 1, all PSG parameterswerewithinnormalrangesinthecontrolgroup. Incontrast,theOSAgrouphadsignificantlyhigherAHIvalues andasignificantdecreaseintheminimumSpO2,whichisa
characteristicofsevereOSA.TheODIwasalsosignificantly increasedintheOSAgroup.Theshorterdurationofsleepin OSAsubjectsdoesnotreachstatisticalsignificanceandno changeshave been detectedin the sleepefficency. More-over, thenumber of microarousal events wassignificantly
higherintheOSAgroupthaninthecontrolgroup.In addi-tion,excessivedaytimesleepiness,asevaluatedbytheESS, wassignificantlyhigherintheOSAgroupthaninthecontrol group.
Table1alsoshowsthatthemeansystolicbloodpressure wasslightlyelevatedintheOSAgroupcomparedtothe con-trol group,with nochange in diastolic blood pressure. In addition, the OSA patients showed a tendency toward an increasedHR.
TheHamiltonInventoryScoresforDepression(HDS)and Anxiety(HAS)andtheIIEFresultsforthestudypopulation arealsoreportedinTable1.OSApatientshadsignificantly higherpsychometricscoresforanxietyanddepressionthan thecontrols.Thepsychometricscoresofthecontrolgroup indicatednosignsofdepressionoranxiety.Furthermore,the OSApatientsweresignificantlymorelikelytohaveerectile functiondisordersthanthecontrols.
Individualhematologicalandserumbiochemicalmarkers of glycemiaandlipids(totalcholesterol andtriglycerides) were within the normal ranges for both groups (data not shown).
Diurnaltrajectoriesofsalivaryfree-testosterone andsalivaryfree-cortisolinthestudypopulation
160
120
80
40
0
8
6
4
0 2
Saliv
ar
y cor
tisol (ng/ml)
Saliv
ar
y testosterone (pg/ml)
Awak ening
(6.30-7.30am)
12pm 7pm
Day time
Control (n = 7) OSA (n = 10)
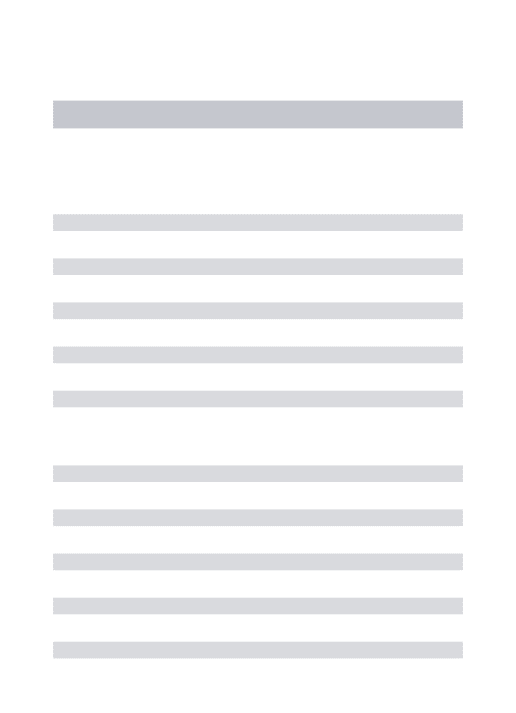
Figure 1 Diurnal trajectories of salivary free-testosterone and salivary free-cortisol in the study population. The data arepresentedasthemean±SEM.Statistical analysis:a two-wayANOVAfollowedbypost-hoctestformultiplecomparisons: * and**: p<0.05 andp<0.01, respectively, vs. thevalue at 07:00; †, ††, and†††:p<0.05, p<0.01, andp<0.001,
respec-tively,vs. the value at12:00;§ and§§:p<0.05andp<0.01,
respectively,vs.thecontrol.
Atwo-wayANOVAanalysisshowedthattherewere signif-icantdifferencesinthesalivarytestosteroneconcentrations measuredatdifferenttimesoftheday(GROUP:F1,50=0.184,
p=0.670; TIME: F2,50=15.350, p<0.001; GROUP×TIME
interaction: F2,50=3.701, p=0.032). The post-hoc test for
multiplecomparisonsshowedthattheTestosterone concen-tration measured in the evening for the control group (91±4pg/mL)wassignificantlylowerthanthevalueinthe
morning(124±10pg/mL, p<0.05).Thesamediurnal fluc-tuation was detected in the OSA group; the Testosterone in theevening(54±5pg/mL) wassignificantlylower than
that in the morning (136±14pg/mL, p<0.001). In addi-tion, the Testosteroneconcentration in the OSA group at 19:00wassignificantlylower(p<0.01)thantheTestosterone concentration in the control group. Finally, no signifi-cant differencewas detected between the control group and the OSA group in the AUC computed from the diur-nal total Testosterone production (1240±53pg/mL/h and 1222±108pg/mL/h,respectively).
TheCconcentrationsinthecontrolandOSAgroupsare reportedinFig.1.Atwo-way ANOVAdemonstrated signif-icant differences between and within the subject groups (GROUP: F1,50=9.594, p=0.003; TIME: F2,50=33.152,
p<0.001; GROUP×TIME interaction: F2,50=3.753,
p=0.031).
50
40
30
20
10
0
T/C r
atio
Awak ening
(6.30-7.30am)
12pm 7pm
Day time
Control (n = 7) OSA (n = 10)
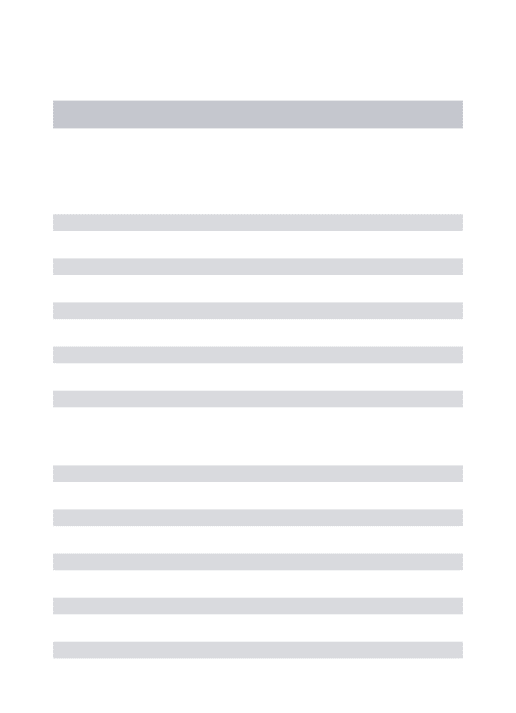
Figure2 Diurnaltrajectories oftheT/Cratiointhe study population.Thedataarepresentedasthemean±SEM. Statis-ticalanalysis:atwo-wayANOVAfollowedbypost-hoctestfor multiplecomparisons,*p<0.001vs.thevalueat7am;†p<0.05
vs.thevalueat12pm;§p<0.05vs.thecorrespondingcontrol.
In both the control and OSA groups, the salivary Cortisol concentration in the morning (7.2±0.6ng/mL
and4.6±1.0ng/mL, respectively)wassignificantlyhigher
than that in the evening (2.5±0.4ng/mL, p<0.001 and 2.1±0.1ng/mL, p<0.001, respectively). Furthermore, in themorning,theCortisolconcentrationintheOSAgroupwas significantlylowerthanthatinthecontrolgroup(p<0.05).
DiurnaltrajectoriesofsalivaryT/Cratiointhe studypopulation
Fig. 2 depicts the diurnal trajectories of the T/C ratio in the study population. A two-way ANOVA demonstrated significant differences in the T/C ratio measured dur-ing the sampling day (GROUP: F1,50=0.633, p=0.431;
TIME: F2,50=3.880, p=0.028; GROUP×TIME interaction:
F2,50=5.347, p=0.008). In the control group,there wasa
progressiveandstatisticallysignificant increaseintheT/C ratioduringthesamplingday(7:00=18±9;12:00=27±3;
19:00=43±5).Incontrast,therewerenosignificantdiurnal
fluctuationsintheT/CratiointheOSAgroup(7:00=28±3;
12:00=34±4;19:00=27±4).Additionally,theT/Cratioin
theOSAgroupwassignificantlyhigherthanthatinthe con-trolgroupin themorning(p<0.05)andsignificantlylower thanthatinthecontrolgroupintheevening(p<0.05).
Discussion
disturbances.The majorfindingof thisstudy isthat male obeseOSA patientshaveareducedTconcentrationinthe eveningandareducedCconcentrationinthemorning com-paredwithnon-apneicobesecontrols. Furthermore,male obeseOSApatientshaveanimbalanceintheT/Cratio mea-suredinthemorningandintheevening.
Sexhormonesarebelieved tobeinvolvedinthe patho-genesis of OSA in adult male subjects who present with reducedlevelsof circulatingandrogens.5,16 Inthe present
study,therewerenodifferencesbetweenthecontroland OSAgroupsinthefluctuationofthediurnalTtrajectory;the eveningTconcentrationwastypicallylowerthanthe morn-ingconcentrationsinbothexperimentalgroups.24,25Salivary
testosteroneconcentrationlowerthan controlsalso trans-latesin an increase incomorbidities (fatigue, depression, general reduction of the well-being sense, sleep distur-bances,etc.)16affectingourOSAsubjects.SinceBMIabove
thenormalrangewaspresentinbothexperimentalgroups, OSA itself, rather than obesity, seems to be the cause of the drop of salivary testosterone concentration in the presentstudy.Ithasbeen suggestedthatthemorningrise intestosterone productionis derived fromanendogenous testosterone circadian rhythm and is not directly related toanyofthesleepstages.26 However,theOSApatientsin
thisstudy experienceda decreasein thelead tostressful modificationsofthesleeppatternswithadecreasedsleep efficiency.26
Inthisstudy,wedemonstratedthatOSAsubjects main-tainphysiologicalcircadianactivityintheHPAaxis,withthe highestcortisolconcentrations presentinthemorningand thelowestpresentintheevening.Themaintenanceof reg-ularcircadian cortisolproductionin OSAsubjects hasalso beenreportedinapreviousstudy27;however,theseauthors
didnotdetectanydifferencebetweentheOSApatientsand controlsinthemorningcortisolconcentration.This discord-ancemayberelatedtothefactthatinthepresent study is detected in the saliva only the ‘‘bioactive’’ free frac-tion,whichcorrespondstotheunboundfreeplasmafraction of thehormone.7 Indeed, morninghypocortisolism in OSA
patientshas been recentlyconfirmed.8 The highest Tand
Cconcentrations occurat thebeginning ofthe day, while thelowestlevelsoccurintheevening.25,28Inourstudy,we
useda three-pointdiurnal sampling schedule for thefirst timeandwereabletodetectagradualincreaseintheT/C ratiothroughouttheday.Achangeinthebalancebetween thetwosteroidhormonesmayputanindividualatriskfor abreakdowninhomeostasis.Inthepresentstudy,theOSA subjectshadahighermorningT/Cratiothanthecontrols; however, in the evening, the T/C ratio was significantly lowerintheOSAsubjectscomparedwiththecontrolgroup. Thisimbalanceintheanabolic-catabolicequilibriumcould beattributedtothe morninghypocortisolismthat charac-terizessevere OSA7,8;the resultant flattened response to
chronicallyrepeatednocturnalchallengesreflectsa dysreg-ulationoftheHPAaxis.29Incontrast,thedecreaseintheT/C
ratiointheOSAgroupintheeveningcouldbearesultofthe sharpandmarkeddropintheTconcentrationat19:00.
Obesity in men is associated with reduced androgen secretion.30 However,inthepresentstudy,obesitywasnot
considered a confounding factor in the T concentration reductionbecauseobesity occurredin bothgroups. Treat-mentof moderatetosevere OSA withcontinuouspositive
airway pressure (CPAP) does not reliably increase testos-terone levels in most studies. In contrast, a reduction in weightdoessopredictablyandlinearlyinproportiontothe amountofweightlost.16
Compared with the control group, the OSA patients demonstrated either a mild anxious-depressive disorder or excessive daytime sleepiness. Recently, a relationship between a depressive mood and obesity wasdescribed.31
However,thecontributionoftheT/Cratioimbalancetothe development of anxious-depressive symptoms in patients withsevere OSAandthekeyrolethatobesityplaysinthe pathogenesisofOSAcomorbiditiesneedstobefurther stud-ied.
OSA is a recognized cause of sexual disturbances in men.16,32,33 In this study,we confirmed that OSA patients
sufferfrommildtomoderatesexualdysfunctionasassessed bytheIIEFquestionnaire.19
Conclusions
ThemainfindingofthisstudyisthatmaleobeseOSApatients havesignificantchangesintheTandCdiurnaltrajectoriesin comparisonwithnon-apneicobesecontrols.Hypocortisolism was particularly pronounced in the morning. Conversely, the Tconcentrationwaslowest in theevening. Moreover, althoughOSApatientsmaintainedthephysiologicaldiurnal T/C ratiofluctuation, they exhibitedan imbalance in the diurnalT/Cratiotrajectory.
Thisstudy improved onother previous studies byusing salivaryhormonemeasurementstodetectthefreefraction ofsteroidhormonesintheplasma34andbyemployinga
tar-getedprotocol.Inparticular,theuseofdatafrommultiple diurnal measurements rather than a single point permit-ted the detection of T/C ratio changes of opposite signs at the beginningand end of theday, allowing for a more accuratestudyoftheHPGandHPAaxes.Finally,itislikely thatinOSAsubjects,poorsleepquality,tiredness,and psy-chological distress areamong the comorbidities affecting theresponsescrucialtothemaintenanceofthe physiolog-icalanabolic-catabolichormonalbalance.However,wedid notestablish a causalrelationship between thesefactors. In fact, a limitationof this study is that we only demon-stratedtheco-existenceofimbalancedTandCproduction andOSA comorbidities.To fullyaddress thispossible rela-tionship,furtherresearch,withsamplesizesadequatefora correlativestudydesign,isnecessary.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
ScientificBilateralAgreementbetweenSapienzaand Grig-oreT.PopaUniversities.
References
1.HiestandDM,BritzP,GoldmanM,PhillipsB.Prevalenceof symp-tomsandriskofsleepapneaintheUSpopulation:resultsfrom thenationalsleepfoundationsleepinAmerica2005poll.Chest. 2006;130:780---6.
2.JennumP,RihaRL.Epidemiologyofsleepapnoea/hypopnoea syndrome and sleep-disordered breathing. Eur Respir J. 2009;33:907---14.
3.YoungT,PeppardPE,GottliebDJ.Epidemiologyofobstructive sleepapnea:apopulationhealthperspective.AmJRespirCrit CareMed.2002;165:217---39.
4.LuboshitzkyR,LavieL,Shen-OrrZ,HerrerP.Alteredluteinizing hormoneandtestosteronesecretioninmiddle-agedobesemen withobstructivesleepapnea.ObesRes.2005;13:780---6.
5.BerceaRM,PatacchioliFR,GhiciucCM,CojocaruE,Mihaescu T.SerumtestosteroneanddepressivesymptomsinsevereOSA patients.Andrologia.2013;45:345---50.
6.TomfohrLM, Edwards KM, Dimsdale JE. Is obstructive sleep apneaassociatedwithcortisollevels?Asystematicreviewof theresearchevidence.SleepMedRev.2012;16:243---9.
7.GhiciucCM,Dima-CozmaLC,BerceaRM,LupusoruCE,Mihaescu T,SzalontayA,etal.Restoringofsalivarycortisolawakening response(CAR) bynasal continuous positiveairway pressure (CPAP) therapy in obstructive sleep apnea. Chronobiol Int. 2013;30:1024---31.
8.KaracaZ, IsmailogullariS, Korkmaz S, CakirI, Aksu M, Bay-demirR,etal.Obstructivesleepapnoeasyndromeisassociated with relative hypocortisolemia and decreased hypothalamo-pituitary-adrenal axis response to 1 and 250g ACTH and
glucagonstimulationtests.SleepMed.2013;14:160---4.
9.Patacchioli FR, Tabarrini A, Ghiciuc CM, Dima-Cozma LC, PreteA, Bianchini C,et al. Salivary biomarkers of obstruc-tive sleep apnea syndrome in children. Pediatr Pulmonol. 2014;49:1145---52.
10.BrownleeKK, Moore AW, Hackney AC. Relationship between circulatingcortisolandtestosterone:influenceofphysical exer-cise.JSSM.2005;4:76---83.
11.PeeriM,ZamaniM,FarzanegiP,RakhshanizadehA,PiriE.Effect ofsleepdisorderonthelevelsoftestosterone,cortisolandT/C ratioinyoungfootballplayers.AnnBiolRes.2012;3:3798---804.
12.GlennLA,RaineA,SchugRA,GaoYD,GrangerDA.Increased testosteronetocortisolratioinpsychopathy.JAbnormPsychol. 2011;120:389---99.
13.Terburg D, Morgan B, van Honk J. The testosterone-cortisol ratio:ahormonal markerfor proneness tosocial aggression. IntJLawPsychiatry.2009;32:216---23.
14.Smith GD, Ben-Shlomo Y, Beswick A, Yarnell J, Lightman S, ElwoodA.Cortisol,testosterone,andcoronaryheartdisease: prospectiveevidence from the CaerphillyStudy. Circulation. 2005;112:332---40.
15.Fernández-Guasti A, Fiedler JL, Herrera L, Handa RJ. Sex, stress,andmooddisorders:attheintersectionofadrenaland gonadalhormones.HormMetabRes.2012;44:607---18.
16.AndersonML,TufikS.Theeffectsoftestosteroneonsleepand sleep-disorderedbreathinginmen:itsbidirectionalinteraction witherectilefunction.SleepMedRev.2008;12:365---79.
17.JohnsMW.Anewmethodformeasuringdaytimesleepiness:the EpworthSleepinessScale.Sleep.1991;14:50---5.
18.HamiltonM.Aratingscalefordepression.JNeurolNeurosurg Psychiatry.1960;23:56---62.
19.RosenRC,RileyA,WagnerG,OsterlohIH,KirkpatrickJ,Mishra A.Theinternationalindexoferectilefunction(IIEF)a multidi-mensionalscaleforassessmentoferectiledysfunction.Urology. 1997;49:822---30.
20.IberC,Anoni-Israel S,ChessonAL,QuaSF.TheAASMmanual forthescoringofsleepandassociatedevents.Westchester,IL: AmericanAcademyofSleepMedicine;2007.
21.HackneyAC,ViruA.Researchmethodology:endocrinology mea-surementsinexercisescienceandsportsmedicine.JAthlTrain. 2008;43:631---9.
22.GröschlM,KhölerH,TopfHG,RupprechtT,RauhM.Evaluation ofsaliva collectiondevicesfortheanalysisofsteroids, pep-tides andtherapeutic drugs. JPharm BiomedAnal.2008;47: 478---86.
23.Pruessner JC, Kirschbaum C, Meinlschmid G, Hellhammer DH. Two formulas for computation of the area under the curve represent measures of total hormone concentration versus time-dependent change. Psychoneuroendocrinology. 2003;28:916---31.
24.Cooke RR, McIntosh JE, McIntosh RP. Circadian variation in serumfreeandnon-SHBG-boundtestosteroneinnormalmen: measurements,andsimulationusingamassactionmodel.Clin Endocrinol(Oxf).1993;39:163---71.
25.Plymate SR, Tenover JS, Bremmer WJ. Circadian variation in testosterone, sex hormone-binding globulin, and calcu-lated non-sex hormone-binding globulin bound testosterone in healthy young and elderly men. J Androl. 1989;10: 366---71.
26.AxelssonJ,IngreM,ÅkerstedtT,HolmbäckU.Effectsofacutely displaced sleep on testosterone. J Clin Endocrinol Metab. 2005;90:4530---5.
27.RaffH,EttemaSL,EastwoodDC,WoodsonBT.Salivary corti-solinobstructivesleepapnea:theeffectofCPAP.Endocrine. 2011;40:137---9.
28.GhiciucCM, Dima-CozmaCL, PasqualiV,RenziP,Simeoni S, LupusoruCE,etal.Awakeningresponsesanddiurnal fluctua-tionsofsalivarycortisol,DHEA-Sand␣-amylaseinhealthymale
subjects.NeurondocrinolLett.2011;32:475---80.
29.Nater UM, Maloney E, Roumiana S, Gurbaxani BM, Lin JM, JonesJF, etal.Attenuated morningsalivarycortisol concen-trationsin apopulation-based studyof persons withchronic fatiguesyndromeandwell controls.JClinEndocrinolMetab. 2008;93:703---9.
30.FeldmanHA,LongcopeC,DerbyCA,JohannesCB,AraujoAB, CovielloAD,etal.Agetrendsinthelevelofserumtestosterone andotherhormonesinmiddle-agedmen:longitudinalresults fromMassachusettsMaleAgingStudy.JClinEndocrinolMetab. 2002;87:589---98.
31.deWit LM,Fokkema M,vanStratenA, LamersF,CuijpersP, PenninxBW.Depressiveandanxietydisordersandthe associa-tionwithobesity,physicalandsocialactivities.DepressAnxiety. 2010;27:1057---65.
32.PetersenM,Kristensen E,BergS,MidgrenB.Sexualfunction inmalepatientswithobstructivesleepapnoea.ClinRespirJ. 2010;4:186---91.
33.BerceaRM,Mihaescu T,Cojocaru C,BjorvatnB. Fatigueand serum testosterone inobstructive sleepapnea patients. Clin RespirJ.2015;9:342---9.