REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Reduced
fasting
time
improves
comfort
and
satisfaction
of
elderly
patients
undergoing
anesthesia
for
hip
fracture
Luiz
Eduardo
Imbelloni
a,∗,
Illova
Anaya
Nasiane
Pombo
b,
Geraldo
Borges
de
Morais
Filho
baDepartmentofAnesthesiology,FaculdadedeMedicinaNovaEsperanc¸a,ComplexoHospitalarMangabeira,JoãoPessoa,PB,Brazil bComplexoHospitalarMangabeiraGov.TarcisioBurity,JoãoPessoa,PB,Brazil
Received25August2013;accepted16October2013
Availableonline2January2015
KEYWORDS
Spinalanesthesia; Fasting;
Satisfaction
Abstract
Backgroundandobjectives: Patient’ssatisfactionisastandardindicatorofcarequality.The aimofthisstudywastoevaluatewhetherapreoperativeoralingestionof200mLofa carbo-hydratedrinkcanimprovecomfortandsatisfactionwithanesthesiainelderlypatientswithhip fracture.
Method: Prospective randomizedclinicaltrialconducted inaBrazilianpublichospital,with patientsASAI---IIIundergoingsurgeryforhipfracture.Thecontrolgroup(NPO)received noth-ingbymouthafter9:00p.m.thenightbefore,whilepatientsintheexperimentalgroup(CHO) received 200mL ofacarbohydrate drink2---4h before the operation. Patients’ characteris-tics,subjectiveperceptions,thirstandhungerandsatisfactionweredeterminedinfoursteps. Mann---WhitneyU-testandFisherexacttestwereusedforcomparisonofcontroland experi-mentalgroups.Ap-value<0.05wasconsideredsignificant.
Results:A total of100 patients were includedinone ofthetwo regimens ofpreoperative fasting.Fastingtimedecreasedsignificantlyinthestudygroup.Patientsdrank200mL2:59h beforesurgeryandshowednohunger(p<0.00)andthirstonarrivaltoOR(p<0.00),resulting inincreasedsatisfactionwiththeperioperativeanesthesiacare(p<0.00).
Conclusions: Thesatisfactionquestionnaireforsurgicalpatientcouldbecomeausefultoolin assessingthequalityofcare.Inconclusion,CHOsignificantlyreducespreoperativediscomfort andincreasessatisfactionwithanesthesiacare.
© 2014SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
∗Correspondingauthor.
E-mail:[email protected](L.E.Imbelloni).
http://dx.doi.org/10.1016/j.bjane.2013.10.019
PALAVRAS-CHAVE
Raquianestesia; Jejum;
Satisfac¸ão
Adiminuic¸ãodotempodejejummelhoraoconfortoesatisfac¸ãocomanestesiaem
pacientesidososcomfraturadequadril
Resumo
JustificativaeObjetivos:Asatisfac¸ãodopacienteéindicadorpadrãodaqualidadeda assistên-ciaprestada.Oobjetivodesteestudofoiavaliarseaingestãode200mLoralpré-operatória deumabebidadecarboidratospodemelhoraroconfortoeasatisfac¸ãocomaanestesiano pacienteidosocomfraturadequadril.
Método: Ensaio clínico prospectivo e randomizado realizado em hospital público de saúde brasileiro,pacientesestadofísicoASAI-IIIsubmetidosàcirurgiadefraturadequadril.Ogrupo controle(NPO)nãorecebeunadapelaboca,apósas21horasdanoiteanterior,enquantoqueos pacientesnogrupoexperimental(CHO)recebeu200mLdeumabebidadecarbohidratosde2a 4horasantesdaoperac¸ão.Característicasdospacientes,percepc¸õessubjetivas,presenc¸ade sedeefomeesatisfac¸ãodospacientesfoiapuradoemquatroetapas.TestedeMann-Whitney U-testeexatodeFisherforamutilizadosentreogrupocontroleeogrupoexperimental.Valor dep<0,05foiconsideradosignificativo.
Resultados: Umtotalde100pacientesforamincluídosemumdosdoisregimesdejejum pré-operatório.Tempodejejumdiminuiusignificativamentenogrupodeestudo.Pacientesbeberam 200mL2:59hantesdacirurgiaenãoapresentaramfome(p<0,00)esedenachegadaàSO(p< 0,00),resultandoemaumentodasatisfac¸ãocomocuidadoperioperatórioanestesia(p<0,00).
Conclusões:O questionário de satisfac¸ão do paciente cirúrgico poderia tornar-se um instrumento útil naavaliac¸ão daqualidade de atendimento.Em conclusão, CHO reduz sig-nificativamenteodesconfortopré-operatórioesatisfac¸ãocomoscuidadosdaanestesia. ©2014SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
There is an increasing number of studies on patient sat-isfaction. Satisfaction is the judgment of the quality of patient care and one of the main objectives during any hospitalization.1Itisalsoacontributingfactortothe out-come,assatisfiedpatientsaremorelikelytocooperatewith
theproposedtreatment.2Comfortandsatisfactionare
rel-evanteconomicimpactcriteriaduringtreatment.1,2
Patient satisfaction is a widely used measure of the
healthcarequalityandhasbeenassociatedwithother
out-comemeasuresandbehavioralintentionsofthepatient.In
general,satisfactionseemstobehigherinolder patients1 andthosewithabetterglobalhealthperspective.3
Measure-ment and understanding of treatment satisfactionshould
alsobepresentinelderlypatients.
Thestandardpracticeof‘‘nothingbymouth’’hasbeen
appliedfordecadesinpatientsundergoingelective
surger-ies. However, recent data indicate that a liberal fasting
scheme does not increase the risk in these patients.4,5
Acarbohydrate-richdrink(CHO) significantlyreduces
pre-operative discomfort without affecting gastric contents.6
Decreased fasting time was related to a lower incidence
ofnauseaandvomitinginpatientsundergoinglaparoscopic
cholecystectomy.7The patientsatisfactionassessmenthas
been used as a measurement of clinical trial outcomes,8
consultations,9 and workload.10 However, little is known
aboutitsbenefit,particularlyonanesthesiacare
satisfac-tionof patients whoreceiveda drinkin the preoperative
andpostoperativeperiods.
Anxiety is a state of imminent danger, which involves
a lot of tension and suffering and may cause increased
heart rate, increased blood pressure, sweating, tremors,
heavybreathing,andmuscletension.11Itmaybeinfluenced
byinternal (personal)andexternal (environment)factors.
The hospitalizationprocessitselfmaybringanxietytothe
patient.Depressionisalsoapossiblereactioninhospitalized
patients. Itis closelyrelated tostressand anxietybefore
surgery.12 Therefore,minimizingthefactorsthatcancause
anxiety is important to avoid physical and psychological
healthconsequences.
The nutritional status increases the risk of
post-operative complications and mortality in patients with
hip fracture.13 In Brazil, the IBRANUTRI study found
that, among patients admitted to hospitals of the
Brazilian public health system (SUS), malnutrition was
present in 48.1% and severe malnutrition in 12.5% of
patients.14
The evaluation of medical treatments, services, and
interventions is increasingly focusing on patient
satisfac-tion. The elderly arethe fastest growing segment of the
population and are responsible for a large portion of the
useofhealthcareservices.Theaimofthisprospective
ran-domized clinical trial wasto investigate --- as part of the
ACERTORPE (Acelerando a Recuperac¸ão Total em
Ortope-dia---AcceleratingTotalRecoveryinOrthopaedics)protocol
implementation --- if the ingestion of a carbohydrate-rich
drinkbeforesurgerycould improvepostoperativecomfort
Method
The protocol was approved by the Ethics Research
CommitteeandregisteredinPlataformaBrasil.During
pre-anestheticvisit, thestudy objectiveandprocedures were
explained in detail to each patient and family members,
andallpatientsprovidedwritteninformedconsent.Thisis
acase---controlstudy.The significancelevelof5% and80%
powerwasused.Thehospitalperformsabout700surgeries
permonth,70%areorthopedicpatients.Ofthose70%,over
50% of patients undergomajor orthopedic surgery (femur
andknee)permonth.Thesamplesizecalculationindicated
47patientsineachgroup.Threepatientswereincludedfor
safety,whichamountedtoasampleof50pairs.
One hundred consecutive patients of both sexes, ASA
physicalstatusI---III,withhipfracture,agedover60years, scheduledforsurgicalrepairwereincludedinthestudy.All inpatientswereSUSpatientsandreceivedspinalanesthesia. Lipschitz classification13 wasusedtoassess the elderly
nutritional status. Inclusion criteria were patients with
normalbloodvolumeandthosewithoutpre-existing
neuro-logicaldisease,coagulationabnormalities,infectionatthe
lumbarpuncturesite,agitationand/ordelirium,notusing
indwellingcatheters,withhemoglobinlevel>10g%,andnot
admittedtotheICU.
Beforeinductionofanesthesia,thepatientwasroutinely
monitored (electrocardiogram,pulseoximetry,and
nonin-vasivebloodpressure);forearmveinwaspuncturedwitha
18Gvenouscatheter.Noadditionalfluidwasintravenously
administeredbeforetheoperationineachgroup.
Perioper-ativevolumereplacementwas4mLkg−1ofcrystalloidand
500mL 6% hydroxyethyl starch (130/0.4) in 0.9% sodium
chloride(Voluven®)inbothgroups.Hypotension(decreased
SBP<30%)wastreatedwithintravenousetilefrine(2mg)and bradycardia(HR<50bpm)withatropine(0.50mg).
After sedation withintravenousketamine (0.1mgkg−1)
andmidazolam(0.5---1mg),skincleaningwithchlorhexidine
andexcessremoval,spinalpuncturewasperformedwiththe
patientinthesittingposition,inthemidlineofL2---L3
inter-space usinga 27G Quincke needle.After the appearance
ofcerebrospinalfluid(CSF),0.5% bupivacaine(10mg)was
administeredatarateof1mL15s−1.Patientswere
imme-diatelyplacedinasupinepositionforthestartofsurgery.
Postoperative analgesia was achieved by anterior
(inguinal)orposteriorlumbarplexusblock(psoas
compart-ment), witha 50mm (inguinal) or 100mm (psoas) needle
(B. Braun) connected to a peripheral nerve stimulator
(Stimuplex®,B. BraunMelsungen AG)prepared torelease
a 0.5mA pulsed square wave with 2Hz frequency,
look-ing for the contraction of the quadriceps muscle. After
theexpectedcontraction,40mLof0.25%bupivacainewere
injected.
Control groupreceivednilperos(NPO)after9o’clock
the night before surgery. Experimental group (CHO) took
200mL of 12.5% dextrinomaltose 2---4h beforesurgery. To
allpatients, 200mLof 12.5%dextrinomaltosewasoffered
immediatelyafterthemotorblockade.
Patients’ characteristics and subjective assessment of
well-being were recorded four times: (1) after the
anes-thesiologist visit; (2)before surgery;(3) beforedischarge
fromthepost-anesthesiarecoveryunit(PACU);and(4)on
themorningofthefirstpostoperativedayintheward.All
patientswereaskedtoevaluatethefollowingitems:hunger, thirst,agitation,postoperativenauseaandvomiting(PONV),
satisfaction, and postoperative analgesia. All evaluations
wereclassifiedasyesorno.
Statisticalanalysis
Mann---WhitneyandFisher’sexacttestswereusedfor statis-ticalanalyses.Ap-value<0.05wasconsideredsignificant.
Results
A total of 100 elderly patients ASA physical status I---III
scheduledfororthopedichipsurgerywereincludedinthis
singlecenterstudy(SUShospital).Patientswererandomly
assignedtooneofthe twopreoperative fastingregimens.
Allpatientscompletedthetrial,andallquestionnaireswere
analyzed.Nopatientwaswithdrawnfromthestudy.
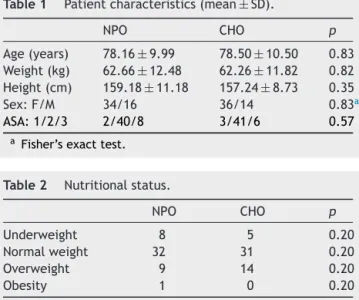
The mean age of patients was78 years and 70% were
female.Patientsincontrolgroup(n=50)andexperimental
group(n=50) weresimilar regardingage, weight,height,
gender,andphysicalstatus(Table1).
In nutritional assessment, 13 patients (13.4%) were
underweight, 63 patients (60.9%) had normal weight, 23
patients (24.7%) were overweight, and only one patient
(0.9%) was obese. There was no significant difference
betweengroups(Table2).
There was no significant difference between groups
regardinganyoftheitemsevaluatedinpre-anestheticvisit (Table3).
Incontrolgroup,35patients(70%)werehungryand45
patients(90%)werethirstyonarrivaltotheoperatingroom.
Inexperimentalgroup,nopatientcomplainedofhungerand
only2patients(10%)reportedbeingthirsty(Table4).There
wasasignificantdifferencebetweengroups.
The evaluation of differenttimes is shown in Table 5.
Meanfastingtimewasof13:30hincontrolgroupand2:59h inexperimentalgroup,withsignificantdifference.All
sur-gerieswereperformedunderspinalanesthesia,withamean
Table1 Patientcharacteristics(mean±SD).
NPO CHO p
Age(years) 78.16±9.99 78.50±10.50 0.83 Weight(kg) 62.66±12.48 62.26±11.82 0.82 Height(cm) 159.18±11.18 157.24±8.73 0.35 Sex:F/M 34/16 36/14 0.83a
ASA:1/2/3 2/40/8 3/41/6 0.57
a Fisher’sexacttest.
Table2 Nutritionalstatus.
NPO CHO p
Underweight 8 5 0.20
Normalweight 32 31 0.20
Overweight 9 14 0.20
Table3 Questionnaireresultsinpre-anestheticvisit.
NPO Yes/No
CHO Yes/No
p
1.Wereyousatisfiedwiththeanesthesiologist’svisitbeforesurgery? 50/0 50/0 a
2.Wastheanestheticprocedurefullyexplained? 50/0 50/0 a
3.Wasitexplainedthatyouwereparticipatinginastudyprotocol? 50/0 50/0 a
4.Didtheanesthesiologistmentionpreoperativefasting? 50/0 50/0 a
5.Doyouthinkitisimportantnottodrinkandeatbeforeanesthesia? 29/21 26/24 0.69
6.WouldyouliketoingestaliquidbeforebeingtakentotheOR? 50/0 50/0 a
7.Wouldyoumindbeingwokentoingestthisliquid? 21/29 26/24 0.69
aNotstatisticallyevaluatedbecausethevariablesareconstant.
Table4 Questionnaire results on arrival at the surgical theatre.
NPO Yeas/No
CHO Yeas/No
p
1.Areyouhungry? 35/15 0/50 0.00 2.Areyouthirsty? 45/5 2/48 0.00
durationof1:59h,withnosignificant differencebetween groups.DextrinomaltosewasorallyadministeredinthePACU (1:58h, on average); there was no significant difference betweengroups.ThelengthofPACUstaywas2:23h, practi-callythesamebetween groups.The durationofanalgesia was 22h, with no significant difference between groups. None of the patients in both groups experienced brady-cardia. Four patients in control group and 2 patients in experimentalgroupdevelopedhypotension,whichwas cor-rectedwithasingledoseofvasopressor,withnosignificant difference.
Theeffectoflessthirstandhungerintheexperimental groupwasdetected beforesurgery.In contrast,therewas nodifferencebetweenthetwogroupsinthePACUregarding thesatisfactionofhavingtakendextrinomaltose,onsetof nauseaandvomiting,satisfactionofnotbeingtransferredto theICU,andbeingwithoutintravenoushydration(Table6).
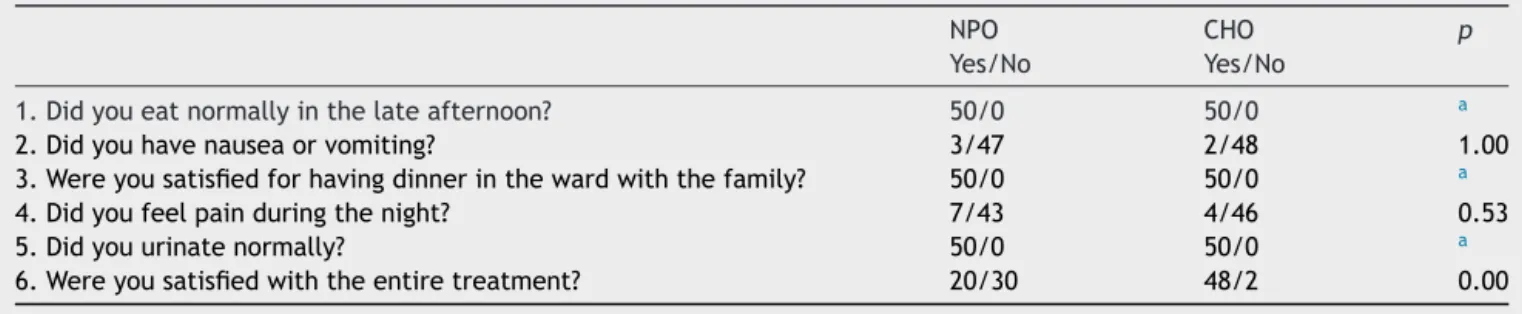
Intheward,thesubjectiveassessmentofhunger,thirst,
nausea and vomiting, postoperative pain, and bladder
catheterizationwassimilarinbothgroups(Table7).
Satisfaction with preoperative visit was
compara-ble between groups. The satisfaction with the overall
anesthetic management, assessed before hospital
dis-charge, washigher in the experimental group (90%) than
inthecontrolgroup(40%),withasignificantdifference.
Discussion
This study clearly confirms that the preoperative intake
of200mLofacarbohydratedrink(12.5%dextrinomaltose)
decreased hunger and thirst preoperatively, resulting in
greatercomfortandsatisfactionwithanesthesiainelderly
patientsundergoingsurgicalrepairofhipfracture.
Hipfractureisacommoninjuryandtheleadingcauseof
deathamongelderlypatients,withsignificantratesof
mor-talityat30daysandoneyear.14---16Thesepatientsrepresent
a significant workload, not just for the operating
depart-mentandsurgicalwards,butfortheentirehealthsystem.
Perioperativecareisalsobecomingmorecomplex,withan
increasingnumberofpatientstakingseveralspecificdrugs
for concomitant diseases. The anesthesiologist must take
thisintoaccountwhenplanningtheanestheticandanalgesic
techniques. Allpatientswere operatedunderspinal
anes-thesia,andanalgesiawasperformed withalumbarplexus
block,withameandurationof22h.
Unlikemulticenterstudywithpatientsfromthe
Brazil-ianpublichealthsystem,17theincidenceofwell-nourished
patientsinthisstudywas60%.Theclassificationusedinthis
studyshowedagoodcorrelationwithmortality;itiseasily
applied,18 wassuggestedforelderlypatients,19 andthatis
whyitwasused.
The questionnaire used for preoperative evaluation
provedtobeequalbetweenthetwogroups.Remembering
Table5 Fastingtime,durationofsurgery,lengthofPACUstay,dextrinomaltoseadministrationtimeaftersurgery,andduration ofanalgesia(mean±SD).
NPO CHO p
Fastingtime(h:min) 13:53±2:05 2:59±0:36 0.00
Durationofsurgery(h:min) 2:00±0:41 1:58±0:32 0.82 DextrinomaltoseinPACU(h:min) 1:52±0:42 2:03±0:43 0.35
PACUstaytime(h:min) 2:18±0:41 2:29±0:43 0.57
Table6 QuestionnaireresultsinPACU.
NPO Yes/No
CHO Yes/No
p
1.WereyousatisfiedtohavetakenthejuicestillinthePACU? 50/0 50/0 a
2.Didyougetqueasywhentookthejuice? 0/50 0/50 a
3.Didyouvomitaftertakingthejuice? 0/50 0/50 a
4.AreyoupleasedtogotothewardratherthantotheICU? 50/0 50/0 a
5.AreyousatisfiedforbeingwithoutintravenoushydrationwhenleavingthePACU? 50/0 50/0 a
a Notstatisticallyevaluatedbecausethevariablesareconstant.
Table7 Questionnaireresultsontheward.
NPO Yes/No
CHO Yes/No
p
1.Didyoueatnormallyinthelateafternoon? 50/0 50/0 a
2.Didyouhavenauseaorvomiting? 3/47 2/48 1.00
3.Wereyousatisfiedforhavingdinnerinthewardwiththefamily? 50/0 50/0 a
4.Didyoufeelpainduringthenight? 7/43 4/46 0.53
5.Didyouurinatenormally? 50/0 50/0 a
6.Wereyousatisfiedwiththeentiretreatment? 20/30 48/2 0.00
a Notstatisticallyevaluatedbecausethevariablesareconstant.
whattheyhavebeeninformedpreoperativelyaboutfasting,
manypatientssaidtheyprefertofollowthedoctor’sorders
toavoidsuspensionoftheirsurgeries.
In 2006, it wasreportedthat the average timeof
fas-tingfromallsolidsandliquidswas16h,andadultpatients
presenting for elective surgerywiththis longtime of
fas-tingiscommon.20ThefastingtimeinNPOgroupwasslightly
shorter,about 14hcomparedtoother study,20 and80%of
patients reported feeling thirsty or hungry. However, the
fastingtimeinexperimentalgroupwasabout3h,withonly
tworeportsofthirst,whichresultedingreatersatisfaction forpatients.InarecentCochranesystematicreview
involv-ing 22 studies, it was found that there was no evidence
thatashorterfastingtimeincreasedtheriskofaspiration,
regurgitation,or morbiditycomparedwithastandardNPO
regimen.21OurresultsconfirmthatCHOintake(200mL)did
notincreasemorbiditycomparedwithNPO.
Thirstandhungerarethemostimportantfactorsfor
pre-operativediscomfort,followedbyanxiety.22Inourstudy,the
intakeof200mLofabeveragewithCHObeforesurgerynot
only reducedthepreoperative thirstandhunger, but
pro-videdgreatersatisfactiontopatients.ThesameCHOvolume
takenonthePACUdidnotprovidetheonsetofnauseaand
vomiting,andalsoincreasedthesatisfactionofallpatients
whowenttotheward.
Forthisstudy,astandardcarbohydratebeverage(12.5%
dextrinomaltose) was selected to be orally administered
preoperativelytotheexperimentalgroupandtobothgroups
inthePACU.Thisstudywasconductedwithelderlypatients
withhipfracture,astheyrepresentagroupofpatientsin
whichthegastrointestinaltractistotallyfree.Becauseno
patienthadnauseaandvomitinginthePACU,allpatients
werefedin thelateafternoonofthesurgerydayandthis
providedanadditionalsatisfactionforpatientsandfamilies.
Abbreviationofpreoperativefastingwiththeadministration
of CHO in coronary artery bypass grafting was safe and
reducedboth ICU andhospital stay times.23 Even in
high-riskpatients(ASAIII---IV)undergoingelectivecardiacsurgery,
preoperativeintakeofupto400mLCHOappearstobesafe,
providinggreatercomfortforpatients.24
Psychologicalpreparationofpatientsundergoingsurgery
decreased the length of hospital stay and reduced the
needforpostoperativeanalgesics.25Informationprovidedby surgeons,anesthesiologists,andnursesonthesurgical pro-cedure,andbetterqualityofpostoperativeanalgesiareduce anxietyandimproverecovery.25,26Allinformationprovided
topatientsandfamiliesduringthepreanestheticprovided
decreaseinpatientanxietyandallowedafaster recovery,
withdischargeconditionsonthefirstdayaftersurgery. Feelingthirstyisarealdiscomfortandcausesgreat
suf-feringtopatient.27 Severalstudies have shownthat thirst
is intense and results in increased anxiety, dehydration,
irritability,weakness,anddespair.28Inthisstudy,therewas ahighincidenceofthirstintheNPOgroupversusnopatient
intheexperimentalgroup.
Theappropriatefluidreplacementisobviouslyimportant
whenthenormalintakeisprohibited,takinganimportant
roleinoptimizingthecardiovascularfunctionduringsurgery.
In both groups, patients receivedperioperative hydration
withcrystalloidandcolloid,resultinginalowincidenceof hypotension.
Satisfactionisdefinedasapleasantsensationcausedby
thefulfillmentof expectations.29 Satisfactionisthe result
of psychological processes, which involves comparing the
perceivedperformanceofaspecifictreatmentfortheinitial expectationsofthepatient.29,30Themainobjectiveofthis
studywastodevelopaquestionnairetoassesssatisfaction
withthepreferenceforpreoperativefastinginorthopedic
Traditionally,directand indirectmeasures were
devel-opedtoassesshealth carefromtheperspective ofhealth
professionals. Patient satisfaction is one of the measures
used,asshown intheincreasingnumberoftoolsdesigned
toassesssatisfactioninrecentyears.Someauthorsgosofar astoconsiderpatientsatisfactionasoneoftheprimary
out-comesofhealthcare.31Patientsatisfactionquestionnaires
must,amongotherrequirements,havesomepsychometric
properties,especiallyifthegoalistogeneralizethe
infor-mationtothetargetpopulation.32 The study involvedthe
applicationof thequestionnairein fourstagestopatients
with more than 60 years, which shows that satisfaction
increasedwiththedecreaseinfastingtime.
In a study of patients undergoing gynecologic
laparoscopy, it was reported that the intake of CHO
twohoursbeforesurgerydecreasedthirstbeforeandafter
theoperation,andthattherewasnodifferenceregarding
hunger.33 Inourstudy,CHO200mLdecreasedboth hunger
andthirstcomparedwiththeNPOgroup.
Theroleoftheanesthesiologisthasevolvedgreatly,since
in addition to providing optimal surgical conditions, they
wanttominimizethepainrightaftersurgery.Theperipheral
nerveblockimprovedpostoperativeanalgesiaandreduced
sideeffectsofopioids,34therebyfacilitatingafastrecovery
process.The meandurationof analgesiawas22h, similar
to other studies with the same type of surgery.34 At the
doseused,allpatientshadresidualanalgesiathenextday,
withoutanydegreeofmotorblock.
The surgical patient satisfaction questionnaire could
becomeausefultoolforassessingthequalityofcare.In gen-eral,satisfactionseemstobehigherinolderpatients.1For elderlypatientsatthehospital,alimitedliquidoralregimen of2---4hbeforeanoperationcaneasilybeimplemented.Itis
onlyamatteroforganizationandadministration.However,
theanesthesiologistsmustfirstensurethesafetyand
com-fortofthepatients.Inthissense,ourdataclearlyshowthat
theliberaluseofCHOinelderlyinpatients isan easyand
practicalwaytoincreasepatientcomfortandsatisfaction
withanesthesiacare.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.LinnMW,LinnBS,SteinSR.Satisfactionwithambulatorycare andcomplianceinolderpatients.MedCare.1982;20:606---14.
2.KinceyJ,BradshawP,LeyP.Patient’ssatisfactionandreported acceptanceofadviceingeneralpractice.JRCollGenPract. 1975;25:558---66.
3.YoungGJ,MeterkoM,DesalKR.Patientsatisfactionwith hospi-talcare.MedCare.2000;38:325---34.
4.LewisSJ,EggerM,Sylvester PA,et al.Earlyenteralfeeding versus‘‘nilbymouth’’aftergastrointestinalsurgery: system-atic reviewand meta-analysisofcontrolledtrials. BrMedJ. 2001;323:1---5.
5.OliveiraKGB,BalsanM,OliveiraSS,etal.Doesabbreviationof preoperativefastingtotwohourswithcarbohydratesincrease theanestheticrisk?RevBrasAnestesiol.2009;59:577---84.
6.HauselJ, Nygren J, Lagerkranser M, et al. A carbohydrate-richdrinkreducespreoperativediscomfortinelectivesurgery patients.AnesthAnalg.2001;93:1344---50.
7.HauselJ,NygrenJ,ThorellA,etal.Randomizedclinicaltrialof theeffectsoforalpreoperativecarbohydratesonpostoperative nauseaandvomitingafterlaparoscopiccholecystectomy.BrJ Surg.2005;92:415---21.
8.BollamMJ,McCarthyM,ModellM.Patient’sassessmentofout ofhourscareingeneralpractice.BrMedJ.1988;296:829---32.
9.MorrellDC,EvanME,MorrisRW,etal.Thefiveminute consul-tation:effectoftimeconstraintonclinicalcontentandpatient satisfaction.BrMedJ.1986;292:870---3.
10.Kaim-CaudlePR,MarshGN.Patientsatisfactionsurveyin gen-eralpractice.BrMedJ.1975;1:262---4.
11.DavidoffLL.Introduc¸ãoàPsicologia. MakronBooks;2001. p. 559.
12.Angerami-CamonVA,TrucharteFAR,KnijnikRB,etal.Psicologia Hospitalar---TeoriaePrática.CengageLearn.2010;27:34.
13.Koval KJ, Maurer SG, Su ET, et al. The effects of nutri-tionalstatusonoutcomeafterhipfracture.JOrthopTrauma. 1999;13:164---9.
14.GoldacreMJ,RobertsSE,YeatesD.Mortalityafteradmissionto hospitalwithfracturedneckoffemur:databasestudy.BrMed J.2002;325:868---9.
15.ParkerM,JohasenA.Hipfracture.BrMedJ.2006;333:27---30.
16.Morrison RS, Chassin MR, Siu AL. The medical consultant’s roleincaringforpatientswithhipfracture.AnnInternMed. 1998;128:1010---20.
17.Waitzberg DL, Caiaffa WT, Correia MITD. Hospital malnutri-tion:theBraziliannationalsurvey(IBRANUTRI):astudyof4000 patients.Nutrition.2001;17:573---80.
18.LipschitzDA.Screeningfornutritionalstatusintheelderly.Prim Care.1994;21:55---67.
19.CerviA, Franceschini SCC, Priore SE. Análise crítica do uso doíndicedemassacorporalparaidosos.RevNutrCampinas. 2005;18:765---75.
20.Aguilar-NascimentoJE,SalomãoAB,CaporossiC,etal.Acerto pós-operatório: avaliac¸ão dos resultados da implantac¸ão de umprotocolomultidisciplinardecuidadosperi-operatóriosem cirurgiageral.RevColBrasCir.2006;33:181---7.
21.BradyM,KinnS,StuartP.Preoperativefastingforadultsto pre-ventperioperativecomplications.CochraneDatabaseSystRev. 2003:CD0004423.
22.Kindler CH, Harms C, Amsler F, et al. The visual analog scale allows effective measurement of preoperativeanxiety anddetectionofpatients’anestheticconcerns.AnesthAnalg. 2000;90:706---12.
23.FeguriGR,LimaPRL,LopesAM,etal.Clinicalandmetabolic results of fasting abbreviation with carbohydrates in coro-nary artery bypass graft surgery. Rev Bras Cir Cardiovasc. 2012;27:7---17.
24.BreuerJP,vonDossowV,vonHeymannC,etal.Preoperativeoral carbohydrateadministrationtoASAIII---IVpatientsundergoing electivecardiacsurgery.AnesthAnalg.2006;103:1099---108.
25.CarrDB,GoudasLC.Acutepain.Lancet.1999;353:2051---8.
26.KehletH,WilmoreDW.Multimodalstrategiestoimprove surgi-caloutcome.AmJSurg.2002;183:630---44.
27.AroniP,NascimentoLA,FonsecaLF.Assessmentstrategiesfor themanagementofthirstinthepost-anestheticrecoveryroom. ActaPaulEnferm.2012;25:530---6.
28.CrenshawJT,WinslowEH.Preoperativefasting:oldhabitsdie hard.AJNAmJNurs.2002;102:37---44.
29.OliverRL.Cognitive,affective,andattributebasesofthe sat-isfactionresponse.JConsumRes.1993;20:418---30.
31.DonabedianA.Evaluatingthequalityofmedicalcare.Milbank MemFundQ.1996;44:166---203.
32.DoeringER.Factorsinfluencinginpatientsatisfactionwithcare. QRBQualRevBull.1983;9:291---9.
33.MeisnerM,ErnhoferU,SchmiditJ.Liberalisationof preopera-tivefastingguidelines:effectsonpatientcomfortandclinical practicabilityduringelectivelaparoscopicsurgeryofthelower abdomen.ZentralblChir.2008;133:479---85.