_
D
iscussions
Washington, D. C. September-October 1970
4
2 Provisional A_enda Item 16 CSP18/DT/1 EN
9 September 1970
ORIGINAL: SPANISH
VENEREAL DISEASES AS A NATIONAL AND
CSPI8/DT/I, Rev. i (Eng.)
I. INTRODUCTION
After the decrease in the incidence of venereal disease observed in
the years following World War II, the recrudescence of the disease that
commenced toward the end of 1950 in all regions of the world again focused
the attention of the public health authorities in the majority of the
coun-tries on the health problem posed by syphilis and gonorrhea.
4
Reflecting this general concern, in October of 1965 the Pan American
Sanitary Bureau, in cooperation with the United States Public Health Service,
" held a seminar which was attended by 40 public health experts representing
25 countries and territories of the Hemisphere, most of whom were directors
and chiefs of departments in ministries of health.
The purpose of the seminar was to exchange ideas and experiences on
the venereal disease problem and to discuss control methods, and its aim was
to direct the attention of the Governments to the situation and to the need
to conduct control programs.
Since then, there has been an increase in the interest of the
coun-tries, as evidenced by the requests for assistance received by the Bureau,
including fellowships to study laboratory techniques and control methods
abroad, national courses and projects at the country level, and advisory
ser-vices and program evaluation.
Another indicator of the growing interest in the problem is the
increasing number of countries that participate in the evaluation of the
performance of laboratory tests which the WHO Serological Reference Laboratory,
at the National Communicable Disease Center in Atlanta, Georgia, United States
of America, makes each year. Seven countries participated in 1963, and 18
participated in 1969.
Even more significant than the foregoing, the selection of the topic,
"Venereal Diseases as a National and International. Health Problem," for the
Technical Discussions at the XVIII Pan American Sanitary Conference Shows the
high interest and concern of the Governments in ascertaining the facts of the
situation and in seeking solutions to the problem.
Venereal diseases are widespread in every country of the world, and,
while it is generally recognized that they constitute an important problem,
its true magnitude is as yet not definitely known.
Various attempts to study them in different regions of the world point
up the gaps in our knowledge of their extent and importance.
The ma:ln difficulties stem from incomplete and deficient case
notifica-tion and lack of uniformity in the notification and registration practices
CSPI8/DT/I, Rev. i (Eng.)
Page 2
For this reason, comparability and collation of statistical data on
the incidence and prevalence of this group of diseases is a problem in itself,
and the authorities are forced to resort to estimates to obtain an idea of
the situation.
Guthe and Hume, in 1948, estimated that there were at least 2 million
new cases of syphilis, acquired by venereal contact, each year and that the ¥
annual prevalence of the disease was as high as 20 million in the world
popu-lationover15 yearsof age. i
If population increases since 1948, the changes in the factors that
influence the spread of the disease, and the trend to increasing incidence
observed in all regions of the world in the decade of the 1950' s, are taken
into account, the annual incidence of new cases of syphilis in the 1960's
may be estimated at not less than 3 million, and the prevalence at 30 million
cases,
Using the same type of calculation, it would be possible to make a
cautious prediction that we are entering the decade of the 1970's with an
annual incidence of 4 million cases of early syphilis, of which 370,000 will
occur in the Americas.
The annual incidence of gonorrhea can be calculated by applying to the
world incidence of syphilis the ratio of cases of syphilis and gonorrhea that
seek medical treatment, which shows that for each case of the former there
are four of the latter. Accordingly, the annual incidence of gonorrhea would
have been 12 million in the 1960's, and we can expect 16 million at the
begin-ing of the present decade, with 1.5 million cases in the Americas.
A study of this problem, based on the notified cases of venereal
dis-ease since 1950, shows that infectious syphilis has increased in many
coun-tries, has remained at approximately the same level in others, and has
diminished in some.
Increase in gonorrhea has been much more widespread and in some
coun-tries has approached epidemic proportions.
Chancroid, !ymphosranuloma venereum, and granuloma inguinale appear
to be less important, while nongonocoecal urethritis, in those countries in
which it is distinguished from gonorrhea, is more prevalent. &
A world survey made by the World Health Organization in 1962 showed
that 76 of the 106 countries (72 per cent) reported a steady increase in the
incidence of early syphilis. Of the 106 countries, 21 were in the Western
Hemisphere and 15 of them (59 per cent) reported an increase.
The situation revealed by this survey has continued; and, even though
around the mid-1960's some countries (France, Italy, the United Kingdom, and
the United States of America) reported a new decrease, this trend did not
CSPI8/DT/I, Rev. i (Eng.)
Page 3
T the Americas, 9 out of 12 countries responding to a questionnaire
sent out by the Bureau in the early part of 1969 reported either an increase
or no significant change for the period from 1960 to 1967, 1968 or 1969.
The increase in gonorrhea is still more marked than that of early
syphilis. A survey of a similar nature conducted by WHO in 1961 showed that
4 53 out of the iii countries (48 per cent) reported a steady increase from
1950 to 1960. In the Americas, in ii out of the 21 countries (52.4 per cent)
the same phenomenon was observed and the trend has not been reversed since
• that date.
In the 1969 survey, 13 of the 24 countries in the Americas reported
an increase.
There can no longer be any doubt that we are witnessing an increase in
the incidence of syphilis and gonorrhea in an important number of the countries
that have adequate reporting procedures, and it may be assumed that the same
thing is also occurring in those countries where the reporting procedures are
not reliable.
II. THE PROBLEM OF VENEREAL DISEASE IN THE AMERICAS
In order to obtain an overall picture of the venereal disease problem
in the Hemisphere, all countries and territories were asked to complete a
questionnaire and the information received is the basis of the description
presented herein. However, in some cases it was necessary to complete this
information with data derived from regular reports of the countries to the
Bureau and to estimate rates when the countries failed to do so, using the
population estimates of the United Nations.
All countries and some territories replied to the questionnaire, but
the information from most of the latter is incomplete and, accordingly, the
presentation is limited to the situation in the 26 countries of the Hemisphere.
It is, of course, well known to all and can easily be observed, that
the data are frequently incomplete and we cannot be certain of their
compara-bility. In some cases the figures furnished in the questionnaire do not
coincide with others previously reported to the Bureau.
Because of such deficiencies in basic information, the overall
descrip-tion must be viewed with caution and no definitive conclusions can be drawn.
• Despite these inadequacies, the data collected can be used to give some
general idea of the situation.
Information from Brazil for the period 1965-1969, appearing in Table I,
CSPI8/DT/I, Rev. 1 (Eng.)
Page 4
TABLE I
CASES OF VENEREAL DISEASE IN THE MUNICIPALITIES
OF THE CAPITALS, NOTIFIED TO THE HEALTH
AUTHORITIES, FOR THE PERIOD
1965-1969
BRAZIL
Years
Disease 1965 1966 1967 1968 1969
Syphilis,all forms 11,718 8,603 -* 6,759 -*
Syphilis, primary and
secondary 2,123 2,847 2,469 2,798 1,881
Syphilis,early latent 804 284 250 691 197
Syphilis,late 1,344 909 751 1,062 461
Syphilis, congenital 283 181 82 556 55
Gonorrhea 13,337 13,254 9,707 13,849 6,176
Chancroid 2,811 2,856 2,409 3,483 2,119
Lymphogranulomavenereum 793 624 606 590 483
Granulomavenereum 190 128 25 32 14
* Information not available
I
RecordedMorbidityfor Syphilis- All Stages
Tables II and III show cases of syphilis, all stages, and the rates
per i00,000 population in 25 countries, for the years 1950 and 1960-1969. o
The rates for all stages of syphilis are in general much higher than
those for early syphilis, and in many countries the great difference results
from the fact that many of the cases notified are discovered and reported as
CSPI8/DT/I , Rev. i (Eng.)
Page 5
In 1969 the total rate per I00,000 population for syphilis was ii.0
in Canada and 45.4 in the United States of America; in Middle America, the
highest rate was 242.3 in E1 Salvador, and lowest was 13.7 in Panama. The
Dominican Republic had the highest rate of the Caribbean Islands, 330.3, and
Cuba, the lowest, 7.2, in the zone and in the Continent. In South America
the rate varied from 98.8 in Venezuela to 8.0 in Bolivia.
4
Data are available for 1950 from 18 out of 26 countries (Bolivia,
Canada, Colombia, Dominican Republic, E1 Salvador, Guatemala, Guyana, Haiti,
° Jamaica, Mexico, Nicaragua, Panama, Paraguay, Peru, Trinidad and Tobago,
United States of America, Uruguay, and Venezuela) and from 16 countries for
the years 1950-1960. The rates dropped 97 per cent in Panama and 20 per cent
in Haiti. Only those for Trinidad and Tobago and for Uruguay rose by 203 per
cent and 12 per cent respectively in this period.
Although the downward trend continued between 1960 and 1969, it was
not too generalized. Of the 25 countries, 17 (Argentina, Barbados, Canada,
Chile, Costa Rica, Cuba, Dominican Republic, E1 Salvador, Haiti, Honduras,
Jamaica, Mexico, Panama, Paraguay, Peru, United States of America, and
Venezuela) reported lower rates. The greatest decrease was observed in
Jamaica (80 per cent) and the smallest in Venezuela (6 per cent). In eight
countries (Bolivia, Colombia, Ecuador, Guyana, Guatemala, Nicaragua, Trinidad
and Tobago, and Uruguay) there was an increase varying from one per cent in
Nicaragua to 82 per cent in Uruguay. In Costa Rica, where data are not
avail-able prior to 1962, a decrease of 16 per cent was recorded between 1962 and
1969 (Table IV).
The foregoing data, with the limitations imposed by their quality and
the variations in the efficiency of case detection and the prompt discovery
of early cases, would indicate that even though the decline observed between
1950 and 1960 continued over the next decade, it is not as general or as
marked.
Recorded Morbidity for Early Syphilis
Early syphilis (primary and secondary), in addition to being the
in-fectious stages of the disease, also constitutes recently acquired syphilis
and hence the rate for early syphilis is the best incidence indicator,
de-spite the fact that it is subject to the effects of variations in the number
of cases diagnosed and notified.
Thirteen countries had data available for 1968 or 1969 (Argentina,
Canada, Colombia, Ecuador, E1 Salvador, Jamaica, Mexico, Nicaragua, Peru,
Trinidad and Tobago, United States of America, Uruguay, and Venezuela). In
North America the rate per i00,000 population was 4.4 in Canada and 9.4 in
the United States of America. In Middle America, the highest rate, 70.2,
was recorded in E1 Salvador and the lowest, 3.5, in Guatemala. In the
Caribbean Area, Jamaica and Trinidad and Tobago had similar rates, 29.4
and 31.8, respectively; in Cuba it was 2.7; in South America the rates ranged
CSPI8/DT/I, Rev. 1 (Eng.)
Page 6
Figures for 1950 were available from only seven countries (Canada,
Colombia, Guyana, Mexico, Trinidad and Tobago, United States of America, and
Venezuela). From 1950 to 1960, all showed a decrease, ranging from 43 per
cent in the United States of America to 97 per cent in Guyana.
In contrast, in the 13 countries for which the rates for 1960 and 1969
can be compared, the decrease was not generalized. Eight countries (Canada,
Colombia, Ecuador, Guyana, Trinidad and Tobago, United States of America,
Uruguay, and Venezuela) recorded increases ranging from 28.8 per cent in
Trinidad and Tobago to 5 per cent in Colombia. In the five countries in
which there was a decrease, the sharpest drop was in Argentina (90 per cent)
and the smallest in Jamaica (3 per cent) (Tables IV, V, and VI and Chart I).
The change in the trend for early syphilis from 1950 to 1960, and from
1960 to 1969, and the predominance of countries in which the rates showed an
increase, support the assumption that we are witnessing a recrudescence of the
syphilis problem, due to an increase in incidence.
Despite the increase shown in the comparison of rates for 1960 and
1969 in the United States of America, the upward trend that began in 1959
reversed direction in 1965. In 1969 the latter trend was continuing, with
the rate for that year 7.4 per cent under that of 1968. No other country in
the Hemisphere shows this phenomenon so clearly, and it could be attributed
to the renewal or intensification of the control program in that country.
Recorde d Morbidity for Early Latent Syphilis
Tables VII and VIII show the known cases and the rates per i00,000
population for early latent syphilis in ten countries (Colombia, Ecuador,
E1 Salvador, Guyana, Honduras, Jamaica, Mexico, Trinidad and Tobago, United
States of America, and Venezuela). The rates for 1968 and 1969 for Cuba,
Guatemala, Nicaragua, and Paraguay may be seen in Table V.
In 1968 or 1969 the rates varied from 0.8 in Cuba to 84.2 in
El Salvador.
In five countries (Colombia, Guyana, Mexico, United States of America,
and Venezuela) the information for 1950 and 1960 reveals a decrease in the
rates for all these countries ranging from 74 per cent in the United States
of America to 34 per cent in Guyana, while between 1960 and 1969 only Jamaica,
Mexico, and the United States of America had a decrease, which amounted to
55 per cent, 87 per cent, and 24 per cent respectively. All other coun- •
tries with data for those years (Colombia, Ecuador, E1 Salvador, Trinidad and
Tobago, United States of America and Venezuela) showed increases ranging from
8 per cent in Venezuela to 166 per cent in Colombia. This change in the trend
CSPI8/DT/I, Rev. 1 (Eng.)
Page 7
Identification of early latent syphilis is made almost entirely as a
result of serological tests, and the rate therefore depends on the tests that
are made; despite this fact, the trend in the rates of early latent syphilis
is an indicator of the prevalence of the first period of latency of the
dis-ease that is the result of the incidence of two to four years earlier. For
this reason, it also reflects failure to detect cases in the early stages.
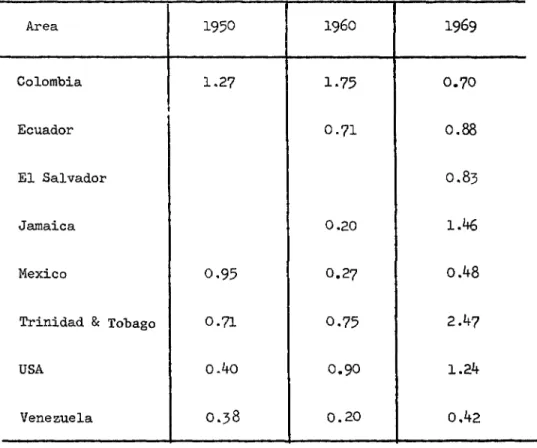
The ratio between early syphilis and early latent syphilis, expressed
in terms of the average number of early syphilis cases for each case of latent
- syphilis, constitutes an index of efficiency in the detection of infectious
cas es.
Table IX gives these indices for 1950, 1960, and 1969 in Colombia,
Ecuador, E1 Salvador, Mexico, Trinidad and Tobago, United States of _America,
and Venezuela.
Recorded Morbidity for Late Syphilis and Late Latent Syphilis
The rate per i00,000 population for late and late latent syphilis is
an indicator of the prevalence resulting from infections occurring 5 to
20 years earlier, and in general, because of the lack of notification of
symp-tomatic late syphilis, the majority of the cases included are due to late
latency and, accordingly, are much affected by the number of serological
examinations carried out.
Data are available for 1968 or 1969 for 13 countries (Colombia, Cuba,
Ecuador, El Salvador, Guatemala, Honduras, Jamaica, Mexico, Nicaragua, Peru,
Trinidad and Tobago, United States of America, and Venezuela). The highest
rate was recorded for E1 Salvador (59.3) and the lowest for Cuba (1.3).
From 1950 to 1960 in all countries for which we have data (Colombia,
Guyana, Mexico, Trinidad and Tobago, United States of America, and Venezuela)
the rates dropped, with the sharpest decrease in Trinidad and Tobago (69 per
cent) and the smallest in Guyana (12 per cent).
From 1960 to 1969 in the same countries the rates increased in Ecuador
(180 per cent) and in Guyana (55 per cent) from 1960 to 1966) and declined
in Colombia (50 per cent), Mexico (58 per cent) United States of America
(41 per cent) and Venezuela (68 per cent) (Tables IV, X, XI).
• Recorded Morbidity for Consenital Syphilis
In North America the rates for congenital syphilis per i00,000
popula-tion were 0.2 in Canada and 1.0 in the United States of America.
In the Caribbean Area, the rate for Cuba was 0.i per cent and that for
CSPI8/DT/I, Rev. i (Eng.)
Page 8
In Middle America, the highest rate was recorded in E1 Salvador (1.6)
and the lowest in Honduras and Mexico (0.i).
In South America, the rate in Argentina was less than 0.i; in Ecuador
it was 0.3; in Colombia, 0.8; in Uruguay, 1.3; in Venezuela 1.6; and the highest
wasinParaguay,2.0.
Five countries (Canada, Colombia, Trinidad and Tobago, United States
of America and Venezuela) submitted data permitting comparison of the rates
in 1960 with 1950 and all recorded decreases ranging from 87.0 per cent in
Canada to 39 per cent in Venezuela.
Between 1960 and 1968 or 1969 the decrease in the prevalence of cases
of congenital syphilis seems to be continuing even though it remains
rela-tively high in some countries, especially if it is kept in mind that in all
probability the notified cases reflect only a part of the problem.
Five count¢ies furnished age-specific morbidity rates for congenital
syphilis (Colombia, E1 Salvador, Jamaica, United States of America, and
Venezuela). Table XIV shows that in Colombia the rate for the group under
one year decreased from 8.8 to 7.0 from 1963 to 1967; while in the United
States of America it increased from 5.0 to 8.8, despite the fact that in both
countries the rate for all age groups decreased. The increase may be
inter-preted as the result of improved diagnoses, or as a consequence of an increase
in the disease in pregnant women or deficiencies in the maternal and child
health programs.
The rates for the 10-year-and-over group dropped 55.2 per cent in the
United States of America over the period 1960 to 1968 or 1969, and since
cases in persons over one year of age reflect incidence i0 or more years
earlier, the observed decrease is an indicator of the changes in the
situa-tion before 1950 and from 1950 to 1960.
Mortality from Syphilis
Death rates from syphilis are conditioned by the prevalence of the
disease, the prompt treatment of early cases, and the diagnosis of syphilis
as the cause of death. Tables XV and XVI show the notified deaths and the
ratesfor1950and for1960-1969.
In Guyana, Haiti, and Paraguay such mortality figures are not
avail-able, and in Cuba and Peru there are no comparable data for 1950.
A comparison of the rates for the most recent year (1967, 1968, or
1969) for which mortality data are available in each country shows that, in
North America, Canada reported a rate of 0.4 and the United States of America_
1.2. In Middle America, Mexico and E1 Salvador reported the highest rates (0.5
in both) and Guatemala and Nicaragua, the lowest (0.i). In the Caribbean
Area, the rate varied from 3.2 in Jamaica to 0.5 in Cuba_ in South America,
CSPI8/DT/I, Rev. 1 (Eng.)
Page 9
In most countries the decrease in the syphilis mortality rate from
1950 to 1960 continued between 1960 and 1969.
From 1950 to 1960 the decrease in rates ranged from 75.6 per cent in
Paraguay to 33.3 per cent in Trinidad and Tobago. From 1960 to 1969, in
contrast to the decrease observed in all other countries, increases were
4 recorded in Argentina (15.4 per cent) Paraguay (20.7 per cent), and Trinidad
and Tobago (i00 per cent). The greatest decrease was in El Salvador
(75.4 per cent) and the smallest in the United States of America (25 per cent).
©
Chart No_ 2 shows the trend in mortality rates for the several regions
of the Hemisphere.
Enfant Mortality from Syphilis
Mortality rates from syphilis per i00,000 live births, for 1969 or the
most recent year for which data are available, show that Paraguay recorded
the highest (97 per cent in 1968). No deaths from syphilis were reported in
Barbados, Canada, Costa Rica, and Trinidad and Tobago in the last year for
which data were reported.
Only Barbados and the United States of America presented data on which
a comparison of rates for 1950 or 1951 could be made with data for 1960. Both
countries showed a decrease, 95 per cent in Barbados and 88 per cent in the
United States of America.
For the period 1960-1969, five countries experienced an increase in
infant mortality from syphilis, with the greatest increase recorded in the
Dominican Republic (173 per cent) and the smallest in Colombia (66 per cent).
The sharpest decline was in Mexico (70 per cent) (Tables XVII and XVIII).
The foregoing data suggest that, despite the decreasing trend, infant
mortal-ity continues to be a problem in many countries and indicates deficiencies
in maternal and child care programs.
Recorded Morbidity from Gonorrhea
The number of cases of gonorrhea continues to increase, reaching
epi-dermic proportions in some countries and constituting the principal venereal
4
disease problem in many areas.
In 1969 or the most recent year reported, for each reported case of
" early syphilis there were 73 cases of gonorrhea in Jamaica, 29 in Canada,
23 in the United States of America, 16 in Argentina, i0 in Colombia and Mexico,
8 in Ecuador, 6 in Peru, 3 in Nicaragua and 2 each in E1 Salvador, Honduras,
CSPIS/DT/I, Rev. i (Eng.)
Page I0
The rates per i00,000 population in North America were 128.6 in Canada
and 263.2 in the United States. In Middle America, rates ranged from 199.2
in Costa Rica to 20.2 in Mexico. In the Caribbean Area tbe highest rate
(2,147.2), was recorded in Jamaica with the lowest (2.9) in Cuba. In South
America, the range was 265.5 in Venezuela and 5,0 in Bolivia (Tables IV,
XIX,andXX andChartNo.3).
The trend from 1950 to 1960 was downward in i0 countries (Bolivia,
Canada, Costa Rica, El Salvador, Haiti, Mexico, Panama, Trinidad and Tobago,
United States of America, and Venezuela). The sharpest decrease was recorded in
Bolivia(94 per cent) and the smallest in IIaiti (20 per cent). In five countries
(Colombia, Dominican Republic, Guyana, Peru and Uruguay) increases in the
rates ranged from 161 per cent in the Dominican Republic to 16 per cent in
Peru.
In ii countries (Argentina, Barbados, Dominican Republic, Guyana, Haiti,
Honduras, Jamaica, Mexico, Peru, Panama, and Uruguay), the rates for gonorrhea
in 1969 were less than in 1960. The decrease ranged from 62 per cent in
Argentina to 0.4 per cent in Uruguay.
In the same period, 13 countries (Bolivia, Canada, Colombia, Costa Rica,
Ecuador, E1 Salvador, Guatemala, Jamaica, Nicaragua, Paraguay, Trinidad and
Tobago, United States of America, and Venezuela) recorded an increase. The
greatest increase was observed in Ecuador and the lowest in E1 Salvador.
In Cuba a comparison of the rate for 1969 with the 1961 rate shows an
increase of 9.7 per cent.
The picture revealed by these figures indicates that the problem of
gonorrhea is out of control and that a concerted effort must be made to find
solutions.
Other Venereal Diseases
Tables XXI, XXII, XXIII, and XXIV show the notified cases of Chancroid,
lymphogranuloma venereum, and granuloma inguinale and the rates for chancroid
per i00,000 population.
Cases of granuloma inguinale are relatively rare and in general are
decreasing; in 1969 the greatest number of cases (168) was reported by Colombia.
The same thing seems to be happening to lymphogranuloma venereum, even
though the total number of cases is somewhat higher. The highest figure for
notified cases (722) was reported by the Dominican Republic.
Chancroid, on the other hand, still constitutes a problem; in 1969 the
CSPI8/DT/I, Rev. i (Eng.)
Page ii
The highest ratio of cases of chancroid to each notified case of early
syphilis (0.5) was recorded in Venezuela and in E1 Salvador in 1969; in
Honduras in 1967 the ratio was 1.2.
III. CONTRIBUTORY FACTORS IN THE RECRUDESCENCE OF VENEREAL DISEASES
There is a worldwide recrudescence of venereal diseases which has
occurred despite modern control techniques and availability of treatment that
" is effective and easy to administer and that offers adequate means of control.
Under these circumstances it is essential to identify the causes of
this apparent paradox so as to organize, or accelerate (as the case may be),
national control programs based on the elimination or control of the factors
that are causing or contributing to this increase. Given the importance of
venereal diseases as a health problem and their impact on society, such
na-tional progrs_ms should have a permanent character and should be carried on
without interruption.
This paradox which involves an increase instead of a decrease in
venereal diseases, in the face of the progress made in availability of
treat-ment, has come about in a changing environment that is characterized by:
The expansion and increasing rapidity of communications between
different countries, and within each country, that facilitates travel
for cultural, commercial, and touristic purposes, and thereby favors
the spread of contacts and venereal diseases which are no longer
confined to limited areas;
An increase in urbanization and industrialization. Both the
developed and the developing countries, with the consequent mobility
of population groups attracted by urban life and new sources of
em-ployment within one country and between different countries;
High birth rates with a great increase in youthful populations,
limited in some countries by family planning and population control;
High population density in certain areas, with overcrowding along
with a process of homogenization of ideas and cultures, especially
among the young who change their traditional ideas and values without
fully replacing them, which in turn gives rise to the co-existence
of different groups with different values and cultural standards
. within the same community.
In this si1:uation of change, epidemiological and social factors that
are favorable for the spread of venereal diseases are intensified, while at
the same tim_ as a result of effective medical action, there is less fear of
venereal diseases coupled with a reduced immunity to reinfection, which
CSPI8/DT/I, Rev. 1 (Eng.)
Page 12
The increase in the diseases at the same time brings about an increase
in the demand for control services that are not being adequately provided by
the health authorities.
In this general framework, various factors conditioning the present
situation stand out. They may be grouped into behavioral factors and medical
andpublichealthfactors.
i. Factors Related to Behavior and Its Changing Nature
Venereal diseases are typical of the ills that have been called
behav-ioral diseases; they continue to spread, despite the fact that adequate
methods of control and treatment are available, because their basic causes
are linked to individual and con_nunity behavior.
Human conduct plays a predominant role in these diseases, and hence
they are closely interrelated to intellectual, emotional, and sociocultural
factors. Even though the effects of these social, economic, and psychosocial
influences on the incidence and spread of the diseases have long been known,
few studies have been made to pinpoint the relative importance of the several
factors, and even fewer to point out ways of controlling venereal disease by
changing behavioral patterns.
The changing environment that characterizes the present situation
con-stitutes the ecological background to venereal diseases, in which one or more
of the factors influences the balance that can inhibit or facilitate
transmission.
The factors most frequently cited as contributing to changes in sexual
behavior are increased promiscuity, changes in sexual habits, increased sexual
activity in the younger age groups, and increased sexual contacts resulting
from the increased migration and interchange between population groups and
areas.
Promiscuity
Promiscuity is not basically a sexual problem but is rather a
manifes-tation of deep psychic disturbances. A study made in the United States of
America by the Public Health Service on sexual life in urban and social
envir-onments brought out very clearly the comon factors in promiscuity that cut
across the borders of social, educational, and age groups, and that were related
toignorance.
Changes in ethical, moral, and behavioral standards resulting from
rapid social, economic, and technological changes have been diffused with
great rapidity and have, in turn, led to increased sexual activity. The
effect of transition from rural to urban environment is the production of
emotionally maladjusted adolescents, as destruction of basic social
CSPI8/DT/I, Rev. 1 (Eng.)
Page 13
subjecting them to an environment in which a large number and variety of
social ills can flourish, and thereby creating foci of venereal diseases
in the large urban centers.
Traditionally, the problem of female promiscuity has been identified
with prostitution. Even today, when the type of prostitution that originated
in poverty and the need for a living has been abolished in principle by
4
international action, it still plays a large part in the spread of venereal
diseases, particularly gonorrhea, in many countries. In the Region of the
Western Pacific, a great many countries reported that more than 80 per cent
of the infection in males can be traced to this source.
According to the replies received, prostitution in the Americas is
regulated in five countries and two territories (Ecuador, Guatemala, Uruguay,
Honduras, and Panama, and the Bahamas and the Netherlands Antilles); it has
been eradicated in Cuba. In seven countries it is illegal (Canada, E1 Salvador,
Guyana, Mexico, Paraguay, Trinidad and Tobago, and the United States of America);
in the remainder it is tolerated, whatever may be its legal status.
Never-theless, in the seven countries that reported prostitution illegal, one
(Guyana) commented that it exists in fact, while in Mexico there appears to
be a provision under which the municipalities may permit it, and in Trinidad
and Tobago, although it has been outlawed, it is reported to play a major
role in the spread of venereal diseases.
Nine countries (Colombia, Costa Rica, Dominican Republic, E1 Salvador,
Honduras, Nicaragua, Peru, Trinidad and Tobago, and Venezuela) consider
pros-titution to be an important factor in the spread of venereal disease, and
Costa Rica holds it responsible for 80 per cent of the problem.
Only Cuba, Jamaica, and the United States of America reported that
prostitution plays no part, or is of little importance, in the venereal
dis-ease problem in those countries.
The picture drawn by these data appears to indicate that prostitution
itself is still a problem, as well as an important factor in the spread of
venereal diseases, and that it is probably being overlaid with new aspects
of clandestine se_mal traffic in an environment of a changing social ecology.
Following the postwar period, prostitution has reappeared in the
devel-oped countries and in many of the developing countries, with changed
charac-" teristics attributable to the improved social and economic situation,
indus-trialization, and the emancipation of women, and stimulated by the search for
pleasure and benefits and luxuries of the improved economic situation. Hence,
" this intensification of hidden sexual traffic is a reflection of higher income
and an increasingly complacent attitude of society toward sexual freedom.
It is stimulated by communications media and advertising and has its roots
in mental aberrations, hereditary factors, traits of ethnic and other minority
groups, and family and educational background that give rise to social
dislo-cations and impair the ability of the individual to face the complexities of
CSPI8/DT/I, Rev. 1 (Eng.)
Page 14
Whether or not it is a question of commercialized promiscuity or
pro-miscuity stimulated by changes in sexual behavior arising from the other
causes discussed, the theory has been advanced that the introduction and
in-creasing use of oral contraceptives has contributed to increased sexual
activ-ity and the consequent spread of venereal diseases.
Few studies have been made to explore this problem, and the majority
of opinions offered are subjective. However, one study, made in Upsala,
Sweden, from 1967 to 1968, revealed that among patients receiving treatment
for gonorrhea and their contacts, 70 per cent of the female students and
51 per cent of the females who were not students were using contraceptive pills,
while the respective percentages for similar groups in 1966 were 48 and 18 per
cent thus evidencing a considerable increase in use of the pill. But what is
more significant is the fact that the average number of sexual pairs was 36 per
cent higher among the group using the pill than in the group not using it.
The average frequency of sexual contacts in the first-named group was 47 per
cent higher than in the second. Moreover, 36 per cent of the females had
increased both the frequency of sexual relations and the number of pairs by
25 per cent after beginning to use oral contraceptives.
If the results of this study were generalized, we would have to accept
the fact that the use of oral contraceptives plays a part by causing the
pro-miscuous woman to expose herself much more frequently. The lack of replies
on this point indicates a lack of precise information that can be generally
applied to all factors relating to changes in conduct. In effect, 14
coun-tries responded in one way or another to the question: What role is played
in the dissemination of venereal diseases by changes in standards of conduct
observed in the last decade? None was able to describe such effects or to
supply objective data.
Increased Sexual Activity and Venereal Diseases in Younger Age Groups
It is evident that there is an increase in sexual activity among younger
age groups and in the number of contacts, and that this increase is conditioned
by psychological, educational, and social and cultural factors in the
environ-ment which encourage greater promiscuity in these groups.
While in some countries there is still the belief that venereal
dis-eases are not a problem among the young, in the majority of the world regions
it appears to be increasing among adolescents and the under-20 age group and
in many instances has been responsible for the recrudescence of venereal
dis-eases as a problem. Reports from the different countries do not agree in
their conclusions. If we consider the increase in the number of persons who
are now seeking treatment, and only the conduct of those who seek treatment
is known, it is difficult to affirm that the observed situation is due to
CSPI8/DT/I, Rev. 1 (Eng.)
Page 15
Nevertheless, in countries where this increase in the under-20 age
group has been observed, the factors contributing to the increase seem to
be early maturity, industrialization and urbanization which attract young
people to the cities where they are free of family control, living in crowded
housing, the rebellion of the young people to the authoritarian ideas of
their parents and teachers, and the greater tolerance of society to sex.
An increase in venereal diseases in the under-20 age group was observed
in the United States of America, where rates for early syphilis in that group
rose from 10.1 to 24.2 per i00,000 population between 1956 and 1965. An
" increase has also been recorded in Canada, the Federal Republic of West Germany,
France, Italy, and the Scandinavian countries.
Five countries in the Americas (Ecuador, Mexico, Peru, United States
of America, and Venezuela) submitted data on which a comparison of the
inci-dence of early syphilis in 1960,with data for 1968 or 1969, was possible for
the age groups 10-19 and 15-19 (Table XXV).
If the percentage differences between rates for this group in the two
years are compared with the differences for all ages in the same years, we
find that in Mexico, where the decrease was general, the rates for males and
females in the 15-19 group decreased less (9.3 and 18.7 per cent, than the
rates for all ages (28.4 and 30 per cent).
In Peru, the decrease in rates for all ages was 17.9 per cent, and in
the age group 10-19 it was only 3.7 per cent. In the United States of America
a comparison of the figures for 1960 and 1968 also shows that the decrease in
the 15-19 age group for males was 10.3 per cent, while in females there was an
increase of 5.7 per cent. The rates for all ages decreased 2.4 per cent in
males and increased 27.2 per cent in females.
In Venezuela, the increase for males in the 10-19 age group was
53.1 per cent, while the increase for all ages was i0 per cent. In females,
where an imcrease was also recorded, this increase was greater for all ages,
351.7 per cent, than the 192.3 per cent recorded for the 10-19 age group.
In Ecuador_ in the same age group there was an increase of 66.6 per cent
in males and 61.2 per cent in females.
The foregoing data are not consistent, since in the countries where
there was a decrease this was in general less among youthful groups of both
sexes, and in Venezuela, where there was an increase in both sexes, and
espe-cially in women of all ages, the increase observed among the young was less.
Only two countries, the United States of America and Venezuela, can
be used to study the trends of gonorrhea infection in the younger groups.
In both countries the rates for both sexes and all age-groups increased. The
United States of America reported a 74.2 per cent increase for males and 35.1
per cent increase for females, while the figures for Venezuela were,
CSPIS/DT/I, Rev. I (Eng.)
Page 16
the United States of America was less, 62.9 per cent in males and 26.7 per cent
in females, while in Venezuela the increase of 160 per cent in males and
161 per cent in females in the 10-19 age group is virtually the same as that
observed for all age groups (Table XXVI).
The available data, therefore, are not such as to permit general
con-clusions about the increase in sexual activity and venereal diseases among
the younger age groups.
Influence of Homosexuality
In recent years male homosexuality has gained in importance in the
transmission of infectious syphilis in many of the developed countries of the
world where a large proportion of primary infections occur in this group.
This is in contrast with the traditional belief, still prevalent in the
devel-oping countries, that homosexuality plays a very small part in the spread of
venereal disease.
Data available from some studies made in European countries, the United
States of America, Canada, m_d Ceylon show that different groups of patients
who have contracted infectious syphilis identify male contacts in percentages
that range from 8.4 to 93 per cent. The average shown in these studies is
around 20 to 25 per cent, in which is included the data found in a survey
made by the American Social Health Association covering the years 1965 and
1966. There are no figures of this nature in the other American states, and
the replies to the questionnaire indicate that no country in the Hemisphere
could supply any objective information.
It is important to point out that homosexual prostitution results
more from the desire for money and immorality than to intersexuality, and
that homosexuals also have heterosexual contacts, thus playing a significant
role in the spread of venereal disease to other groups.
Population Mobility
Increased population mobility with the greater number of contacts and
their frequency between countries, and between different areas within the
same country, facilitated by the expansion and rapidity of communications,
is another identifiable factor among the causes of venereal disease recrudescence.
As an indicator of the importance of the problem, it is observed that
in Sweden, 24 per cent of recent syphilis cases acquired the infection abroad.
In the United Kingdom, 40 per cent of the infected males and 60 per cent of
[
CSPIS/DT/I, Rev. i (Eng.)
Page 17
2. Medical and Public Health Factors
The introduction of penicillin in the treatment of venereal diseases,
its widespread use, and the results initially obtained,changed the public
attitude toward this group of diseases. The fear of the consequences of
vene-real diseases was replaced by a certain lack of concern on the part of the
i public, and gave rise to a false sense of security among health authorities.
Government interest in control programs began to decrease, and in
almost every part of the world the majority of venereal disease patients came
to be treated by private physicians. The simPle , rapid treatment thereby passed
out of the hands of the trained venereologist to the general practitioner, and
the idea was lost that the latter required any special preparation for the new
tasks. Accordingly, their training for the new responsibility is largely
defi-cient because at the same time the changing image of these diseases was reflected
in the medical schools where instruction in the field either deteriorated or
was neglected.
Nevertheless, the role of private physicians inthe diagnosis and
treatment of venereal diseases is, and must continue to be, extremely
impor-tant, if the work of investigating contacts and educating the patient and the
community in prophylaxis is to be carried on.
The proportion of patients who resort to private physicians and receive
treatment from them depends on social and economic conditions, the
availabil-ity of public services, and the attitudes of the public.
The proportion of patients treated by private physicians varies in the
different countries according to the organization and coverage provided by
the health services. In the United Kingdom, where there is a single health
service, more than 75 per cent of the patients receive treatment in public
clinics. In Scotland, particularly, 90 per cent of the gonorrhea patients
receive such treatment.
In contrast, ten times as many cases as are reported are treated by
private physicians.
The availability and ease of administration of the treatment lends
itself to self-medication, as well as treatment by nonmedical people of all
types (pharmacists, witch doctors, amateurs, etc.). Free distribution of
antibiotics, which is the practice in many countries, contributes to this
situation.
Antibiotics can be obtained without medical prescription in 15 of the
26 countries in the Americas (Bolivia, Chile, Colombia, Dominican Republic,
Ecuador, E1 Salvador, Guatemala, Honduras, Mexico, Nicaragua, Panama, Paraguay,
Peru, Uruguay, and Venezuela).
Although there is no evidence that the treponemicidal efficacy of
CSPI8/DT/I, Rev. i (Eng.)
Page 18
therapy seems to have been reached. At the same time, it is known that many
strains of N. $onorrheae in various parts of the world are showing increasing
resistance to penicillin and other antibiotics used for its control, and,
for this reason, its treatment is becoming more complex, requiring
special-ized and up-to-date knowledge in the selection of drugs and treatment schedules.
Preventive effects that might have been derived from use and abuse of
antibiotics in the first decade after their introduction, if in fact this was
the case, seem to have disappeared. In the case of syphilis, the prescribed
treatment eliminates relative immunity, leads to the reinfection of
individ-uals forming part of those groups that have high rates of exposure, and causes
changes in the volume of susceptibles.
Eradication or control of yaws in countries where it was once prevalent
may also have contributed to the increase of the susceptible population.
The initial optimism created by the successful use of penicillin has
given rise to a de-emphasis of the attention given to control programs.
Measures earlier in effect were not continued, or at least new procedures
were not developed, nor were adequate funds assigned to the work, since it
was considered to be no longer a program requiring high priority.
However, with the present recrudescense of the diseases, many countries
have introduced new programs and have renewed their interest in the control
and study of the venereal disease problem.
IV. VENEREAL DISEASE CONTROL PROGRAMS IN THE AMERICAS
It is true that the multiplicity of ecological forces affecting the
dissemination of venereal diseases is not within the control of the
tradi-tional public health measures, and behavioral factors have a determining
influence that makes it essential to promote social and educational techniques
based on multidisciplinary studies. Nevertheless, venereal diseases do not
for that reason cease to be a cormnunicable disease to which the control
pro-cedures appropriate to their specific epidemiological behavior can and must
be applied.
Measures for the control of gonorrhea and syphilis are known and easy
to define. They consist primarily in early detection and prompt treatment
of cases.
In the absence of an irmnunizing agent and because of the manner in
which they are transmitted, through venereal contact between infected and
non-infected individuals, control depends on locating the infected persons
as promptly as possible, especially those in the infectious stages, and
treat-ing them before they can become focis of infection.
Control depends on diagnosis and treatment of cases, their detection,
CSPI8/DT/I, Rev. i (Eng.)
Page 19
work is to be done, the existence of a well-organized and dynamic health
service, working for a well-organized society, is essential.
The establishment of control programs and their application depend
on a great many factors, among which an important role is played by the
attitude of its medical profession, the authorities and workers in the health
services, and the community attitude toward the diseases which determine the
priority of the work and the funds that will be made available for it.
i. Venereal Disease Control Programs
Nineteen countries of the Americas (Bolivia, Brazil, Canada, Chile,
Costa Rica, Cuba, Dominican Republic, Ecuador, E1 Salvador, Guatemala, Jamaica,
Mexico, Nicaragua, Paraguay, Peru, Trinidad and Tobago, United States of America,
Uruguay, and Venezuela) have reported that they have officially organized control
programs. Twelve of this group (Brazil, Canada, Chile, Costa Rica, Dominican
Republic, Ecuador, Guatemala, Mexico, Nicaragua, Trinidad and Tobago, United
States of America and Venezuela) could identify all or a part of the financial
resources allocated for venereal disease control activities. Two countries
(Argentina and Honduras), although ha_ing no officially organized control
programs, were also able to report the funds available to combat these
diseases.
Except for Cuba and Guatemala, all countries with venereal disease
control programs indicated that they had programs for the control of gonorrhea,
and three - Barbados, Guyana, and Honduras - had gonorrhea control programs
even though they did not report official venereal disease control programs.
All countries except Colombia and Panama furnished free treatment for
syphilis and gonorrhea.
2. Venereal Disease Notification
The increase in venereal diseases that can be observed in countries
with the more highly developed reporting systems seems to indicate that it
is a universal problem.
, It frequently appears that syphilis and gonorrhea are more prevalent
than is revealed by available statistics, even in those countries having the
best notification procedures. Apart from the fact that case notification
. from all possible sources ought to be obligatory, efforts to promote timely
and efficient reporting should not be curtailed.
It is essential to encourage regular notification of all cases
diag-nosed and treated by private physicians and by both private and public
institutions, both for gonorrhea and for syphilis in each and every one of
CSPIS/DT/], Rev. i (Eng.)
Page 20
Limited knowledge of venereal disease derives from a series of facts.
In many cases the patient resorts to self-treatment_ to the amateur
practi-tioner_ to the curer, to the witch doctor, or to nonmedical professionals who
do not report the cases that come to their attention. At the same time, the
medical profession reports only a small proportion, if they do so at all_ of
the cases among their patients.
In addition to the foregoing, variations in the forms and the standards
for classification of syphilis that are employed, often within the same country,
are not comparable and make it difficult to correlate early syphilis cases
reported by one country with the figures for another.
A national survey on incidence of venereal diseases made in the United
States of America in 1968 showed that private doctors reported to the
Depart-ment of Health only about ii per cent of the infectious syphilis cases,
38 per cent of the cases of other stages, and ii per cent of the cases of
gonorrhea. Nevertheless, four out of five of the reported cases were treated
by private physicians.
As a result of poor notification procedures, data on gonorrhea have
little validity. Even when data for syphilis are more reliable, notification
of these cases is also very deficient. In the WHO surveys of 126 countries,
57.2 per cent of the countries reported that notification was obligatory. In
the Americas, however, notification is obligatory in 22 countries.
Data on early syphilis since 1950 were available in only twelve
coun-tries, eight in Europe and four in the Americas (Canada, E1 Salvador,
United States of America and Venezuela)
In replies to the questionnaire sent out by the Bureau this year,
21 countries (Argentina, Bolivia, Brazil, Canada, Chile, Colombia, Costa Rica,
Cuba,Dominican Republic, Ecuador, E1 Salvador, Guatemala, Honduras, Mexico,
Nicaragua, Panama, Paraguay, Trinidad and Toba_o. United States of America,
Uruguay, and Venezuela) reported that case notification of venereal diseases
to the health authorities is obligatory.
However, notification of positive serological reaction is obligatory
in ii countries (Argentina, Bolivia, Brazil, Canada, Cuba, Dominican Republic,
Honduras, Mexico, Panama, United States of America (all but 12 states), and
Venezuela_.
Although this picture appears encouraging, examination of the data
supplied reveals substantial deficiencies in both quantity and quality, which
makes it difficult to describe and interpret the situation.
3. Serological Examinations
Serological examinations constitute an important tool in the diagnosis
CSPIS/DT/1, Rev. i (Eng.)
Page 21
Screening procedures tend to lose their value and the cost increases
to the extent that the incidence of the disease decreases; at the same time,
they are very useful in population groups that are especially vulnerable, and
the majority of public health authorities and workers consider that this
pro-cedure should be used for premarital testing, for pregnant women, as a routine
test in hospitals, in health examinations, and in any other group that is
¢
particularly exposed to the diseases.
The serological tests that are most recommended and that are considered
perfectly feasible in a well-organized program are VDRL as a nontreponemal test
to be used as a routine, primarily as a screening technique, and a treponemic
test which, because it is more specific, could be employed whenever the diagnosis
has to be based on the serological result. The VDRL test is already being used
as a nontreponemic test in all countries of the Hemisphere; Cuba reported that
it is using the Kahn test, and Chile and Haiti both use VDRL and Kahn.
Ten countries (Canada, Colombia, Costa Rica, Ecuador, Jamaica, Mexico,
Trinidad and Tobago, United States of America, Uruguay, and Venezuela) report
at least one laboratory in the country that performs serological tests for
treponema.
Eleven countries (Argentina, four provinces of Canada, Costa Rica,
E1 Salvador, Guatemmla, Honduras , Mexico, Panama9 Paraguay, Peru and the
United States of America, with the exception of five states) have laws or
provisions requiring premarital serological tests, and in five of the
remain-ing countries (Cuba, Dominican Republic, Ecuador, Haiti, and Venezuela) it is
customarily perfo creed.
Serological tests for pregnant women are required by law or regulation
in 14 countries (Bolivia, Chile, Colombia, Costa Rica, Ecuador, E1 Salvador,
Haiti, Honduras, Mexico, Panama, Paraguay, Peru, United States of America, and
Vemezuela), and such testing is customary in ten (Argentina, Barbados, Canada,
Cuba, Dominican Republic, Guatemala, Guyana, Jamaica, Trinidad and Tobago, and
Uruguay).
In Brazil, serological tests are made in both groups in the maternity
hospitals.
Table XXVIII shows serological tests made in 1969 with the percentage
" positivity. The lowest percentage, 2.1, was recorded in the United States of
America and the highest, 45, in the Dominican Republic, followed by Jamaica with
22.2.
• Five other countries submitted data on the number of cases treated in
1969 as result of serological tests (Bolivia, Ecuador, Jamaica, Mexico and
CSPIS/DT/I, Rev. i (Eng.)
Page 22
4. Diasnosis of Gonorrhea
Up to the present date no satisfactory serological technique is available
that will detect cases of gonorrhea. The Gram stain and culture methods are
relied upon for diagnosis and detection.
In women, and especially in the asymptomatic cases that constitute the
principal reservoir of infection, culture is the basic technique.
The Gram stain technique is employed in all countries in the Americas,
but it is used in all clinics in only twelve countries (Brazil, Canada,
Costa Rica, Ecuador, Guatemala, Jamaica, Nicaragua, Peru, Trinidad and Tobago,
United States of America, Uruguay, and Venezuela). Thirteen countries have
facilities for culture (Brazil, Canada, Costa Rica, Dominican Republic,
E1 Salvador, Guatemala, Nicaragua, Paraguay, Peru, Trinidad and Tobago, United
States of America, Uruguay, and Venezuela).
5. Investigation of Contacts
Identification of contacts, their location, examination_ and treatment
is essential if the spread of the disease is to be halted.
In recent years, particularly in the United States of America,
tech-niques and procedures have been developed and highly encouraging results have
been obtained through their application in syphilis control. In contrast, it
is much more difficult to trace the source of infection and halt transmission
of gonorrhea, because of its very short incubation period. Experience shows
that control methods must take into consideration the differences in the
behav-ior of the two diseases and that new methods specifically applicable to gonorrhea
must be found.
Whatever the method employed and the level of training of personnel
used in contact investigation, the information collected shows that contact
investigation is carried throughout the entire country in ten countries
(Argentina, Barbados, Canada, Costa Rica, E1 Salvador, Panama, Trinidad and
Tobago, Uruguay, United States of America, and Venezuela). In twelve countries
(Bolivia, Chile, Colombia, Cuba, the Dominican Republic, Guyana, Ecuador, Jamaica,
Mexico, Nicaragua, Paraguay and Peru), this work is performed only in the large
cities.
Nevertheless, only five of the first-named ten countries (Costa Rica, •
E1 Salvador, Trinidad and Tobago, United States of America, and Venezuela)
have available data for 1967 and 1968 on the number of primary and secondary
cases of syphilis interviewed. In the second group, where interviews are carried
out only in the large cities, data were submitted by only six countries (Bolivia,
Chile, Dominican Republic, Ecuador, Jamaica, and Mexico).
Five countries of the eleven in which the number of cases of primary and
secondary syphilis interviewed is known also have data for 1960 (Costa Rica,
CSPI8/DT/I, Rev. I (Eng.)
Page 23
Tables XXVlII and XXIX show the activities and the results of contact
investigation in the countries that have data. Table XXX shows indices of
these activities and the results.
The contact index, i.e., the average number of sexual contacts reported
for each case of infectious syphilis interviewed, ranged from 0.47 in El Salvador
to 4.35 in Venezuela in the figures for 1968.
Comparison of the contact index for 1968 with the same data for 1960
" shows that it decreased from 4.11 to 2.58 in Costa Rica, from 0.92 to 0.47 in
E1 Salvador, and from 3.39 to 2.95 in the United States of America. In Mexico
and Venezuela it increased from 1.17 and 1.23 to 1.72 and 4.35 resoectively.
These differences can be interpreted as a function of changes in the number of
sexual pairs, or in the techniques and ability of the investigators in
obtain-ing names of contacts from the persons interviewed.
The percentase of contacts interviewed reflects the ability of the staff
to locate them as well as the availability of funds for the work, and varied
from 17 per cent in Ecuador to 90 per cent in Costa Rica. The comparison of
these percentages for 1960 and 1968 shows that Costa Rica experienced an increase
from 20 to 80 per cent, and Ecuador from 32 to 84 per cent, while no change
appeared in the United States of America, and Mexico and Venezuela had a
decrease from 50 to 47 per cent and from 75 to 53 per cent, respectively.
The index of syphilis cases treated, which is the average number of cases
discovered and treated as a result of investigation of contacts of each case of
infectious syphilis interviewed, is known only for E1 Salvador, the United
States of America_ and Venezuela. It was 0.43 for the United States of America
in 1960 and 0.43 in 1968. The figures for Venezuela in the same years were
0.43 and 2.11 respectively; and for E1 Salvador it was 0.17 in 1969.
The index of earl}_ syphilis cases treated (lesion-to-lesion) represents
the average number of infectious cases of syphilis for each case of early
syphilis interviewed. It ranged from 0.16 in Mexico to 0..72 in Chile in 1968.
The comparison between the figures for 1960 and 1968 shows that it rose in
Venezuela from 0.I to 0.66, and in E1 Salvador from 0.13 to 0.28; it remained
stationary in Mexico, and decreased from 0.27 to 0.22 in the United States of
America.
• 6o International Control Measures
Attention has been concentrated on the epidemiological control of
emigrants and tourists, in the venereal disease control centers of the
maritime health authorities recommended by the Brussels Agreement, and on
the international exchange of epidemiological information, in the control
of the spread of venereal diseases from one country to another, which has
CSPIS/DT/I, Rev. I (Eng.)
Page 24
The number of venereal disease control centers in the Americas in
1961 was 387.
With regard to the exchange of epidemiological information, the
information provided by the countries shows that in 1969 only Mexico, the
United States of America, and Venezuela notified other countries in the
Hemisphere of the number of contacts obtained that had their domicile in the
country notified. The number of for_q sent by Mexico was 147, the United
States of America, 411, and Venezuela, 22. Mexico sent one and the United
States of America sent 396 to countries in other continents.
V. THE COST OF VENEREAL DISEASES
Even though only in general terms, it is important to have an idea
of the burden imposed on the community by the presence of these diseases in
order to arrive at an estimate of the benefits that might be obtained
through their control or eradication, a benefit that in turn justifies, in
economic terms, the health programs and the resources required to carry
them out.
The cost of venereal diseases in terms of morbidity has been pointed
out in the presentation of estimates of new cases of early syphilis and
gonorrhea. But in addition to the magnitude of the problem of the acquired
infection and its recrudescence on a worldwide basis, it is also important
to estimate the disability and premature death that may be expected among
patients who are not treated.
Under present conditions of technical knowledge and given the fact
that effective drugs are available for treatment of the diseases, it is
difficult if not impossible on ethical grounds to carry out studies to
measure the varying degrees of disability and death between the treated and
untreated groups. Probably the only source of information that could be
used for this purpose, either today or in the future, would be the classic
material collected by Beck and Brunsgaard in Oslo and the study made at
Tuskogee in Alabama.
It has been estimated on the basis of these two studies that for
every 200 patients not receiving treatment, one will become blind; four
will develop dementia; eight,consumption; and seven, cardiovascular syphilis.
At the same time untreated syphilis reduces life expectancy by 17 per cent,
and in 30 per cent of the deaths it has been determined on autopsy that the
principal cause of death was syphilitic involvement of the cardiovascular
or the central nervous system.
Moreover, apart from the emotional and social problems caused by the
disease that are measured in terms of human suffering, untreated syphilis
results in enormous e,:onomic losses and the burden of the expense required
to treat the disease and its complications and disabilities, and in the
diminution of productivity resulting from man-hours of work lost either by
CSPI8/DT/I , Rev. i (Eng.)
Page 25
It has been estimated that in the United States of America 24,000
patients with psychoses as a result of syphilis, interned in mental hospitals,
represent an expense of $49 million. The cost of maintaining 12,200 persons
incapacitated by blindness amounts to $5 million each year, and the loss of
man-years resulting from the lowered life expectancy can be calculated as a
loss in productivity equivalent to $48 million annually.
This total of $102 million, although a substantial sum, represents
only a part of the problem; it does, however, serve as an indicator to
assess the economic importance of venereal diseases and can be used as a
• yardstick to measure the benefits that might be obtained by their control.
Vl. OUTLOOK AND REQUIREMENTS
Venereal diseases and especially gonorrhea have increased to a
significant extent in the decade of the 1960's and the programs to control
these diseases have not been adequate.
Medical and public health efforts have been neutralized and
out-weighed by ecological influences and rapid physical and social changes in
the environment that have favored, and are continuing to favor, its spread.
All that can be expected of individual therapy in the treatment of
gonorrhea and syphilis seems to have been achieved, and there is little hope
that new advances in treatment would effect any change in that situation.
Since the disease is so intimately related to the behavior of
indi-viduals and societies, the psychological, educational, and sociocultural
factors affecting its spread must be taken into consideration so as to be
sure they are made a part of the control programs. However, we have very
little knowledge of these factors and even less of the processes by which
they may be changed.
It is probable that, as a consequence of this situation, venereal
diseases will continue to be a national and international problem of
impor-tance, unless it is possible to develop vaccines and preventive methods or
technical developments are found that can offset the effects of the
indi-vidual and environmental factors now contributing to their incidence. Both
aspects need to be studied, and the necessary attention and funds must be
made available for this purpose.
The impact of health education programs does not seem to be very
• promising, and new techniques must be designed to produce the required
impact on individuals and groups most at risk. Social research and
CSPIS/DT/I, Rev. 1 (Eng.)
Page 26
to identify with some precision those who are most exposed to the risk and
what characteristics they have. Even when epidemiology is showing
increas-ing interest in psychological, cultural, and social factors that influence
patients, and some social scientists are becoming concerned in turn with
epidemiology, much still remains to be done and very few studies have so
far been made to clarify the problem.
The need for coordinated research is imperative, and the importance of
behavior in the venereal disease problem is obvious. However, this should not
be used as an excuse for abandoning control activities. In the present state
of knowledge, these are essential and they must be intensified since, at least
in the case of syphilis_they have demonstrated their effectiveness when
prop-erly applied.
Accordingly, each country must perfect and develop its control programs,
giving them a permanent basis by effective incorporation into the health
ser-vices so as to assure their continuity.
The programs must be based on a diagnosis of the situation and the
epi-demiological behavior of the disease in different communities and sectors of
the communities. There must be an adequate register of cases completed by a
system of analysis and interpretation that facilitates surveillance on the
trends of venereal diseases in different areas and in different population
groups. This is not possible without obligatory notification that is properly
enforced. It is essential that redoubled efforts be made to improve the
ex-isting conditions.
A program, to be effective, must include the necessary activities
de-signed to improve the general state of health, to provide specific protection,
and to limit the consequences of the disease.
Health education and sex education are fundamental requirements if a
program is to be effective in improving the general health situation in
rela-tion to venereal diseases. Despite the limitations on the available
tech-niques, an effort must be made to extract the best possible advantage from
them, to perfect them, and to seek new methods.
Provision of specific protection requires individual and collective
prophylaxis, diagnosis and early treatment of cases, and identification of
contacts so as to close off the reservoirs and halt or limit spread of the
disease.
Research in preventive methods now in progress must be expanded and
intensified with the objective of finding a satisfactory syphilis vaccine and
immunizing agents or other types of preventive measures for gonorrhea. The
study of preventive techniques could be incorporated in programs for family
planning and maternal and child care, which at the same time can be used for
epidemiological research in behavioral aspects that encourage the spread of