REVIEW ARTICLE
Association between physical activity and quality of life in
the elderly: a systematic review, 2000-2012
Gislaine C. Vagetti,
1,2Valter C. Barbosa Filho,
3Nata´lia B. Moreira,
1Valdomiro de Oliveira,
1Oldemar Mazzardo,
1Wagner de Campos
11Exercise and Sports Research Center, Graduate Program in Physical Education, Universidade Federal do Parana´ (UFPR), Curitiba, PR, Brazil.2Faculdade de Artes do Parana´, Curitiba, PR, Brazil.3Sports Center, Graduate Program in Physical Education, Universidade Federal de Santa Catarina (UFSC), Floriano´polis, SC, Brazil.
Objective:To review information regarding the association of physical activity (PA) with quality of life (QoL) in the elderly and to identify the study designs and measurement instruments most commonly used in its assessment, in the period 2000-2012.
Methods: Relevant articles were identified by a search of four electronic databases and cross-reference lists and by contact with the authors of the included manuscripts. Original studies on the association between PA and QoL in individuals aged 60 years or older were examined. The quality of studies as well as the direction and the consistency of the association between PA and QoL were evaluated.
Results:A total of 10,019 articles were identified as potentially relevant, but only 42 (0.42%) met the inclusion criteria and were retrieved and examined. Most studies demonstrated a positive association between PA and QoL in the elderly. PA had a consistent association with the following QoL domains: functional capacity; general QoL; autonomy; past, present and future activities; death and dying; intimacy; mental health; vitality; and psychological.
Conclusion:PA was positively and consistently associated with some QoL domains among older individuals, supporting the notion that promoting PA in the elderly may have an impact beyond physical health. However, the associations between PA and other QoL domains were moderate to inconsistent and require further investigation.
Keywords: Quality of life; motor activity; elderly; aged; physical activities
Introduction
As the size of the elderly population continues to increase, health maintenance and physical independence in this population have become widely discussed topics in the literature. An important component in determining the health status of an individual, especially during the aging process, is quality of life (QoL). However, concepts of QoL are very widespread and diverse.
Most definitions of QoL involve domains such as functional ability, socioeconomic status, emotional state, intellectual activity, cultural and ethical values, religiosity, health, living environment, and daily activities.1-4 From this perspective, QoL in the elderly consists of physical, psychological, social, cultural, mental, and spiritual domains.5
QoL can also be divided into general QoL (QoL) or health-related QoL (HRQoL). The former is based on a broad definition that encompasses a sense of well-being and happiness, without reference to health problems or
disorders. HRQoL, on the other hand, is part of a multidimensional approach that considers physical, men-tal, and social-related symptoms, as well as limitations that are caused by illness.6
According to the World Health Organization (WHO), participation in physical activity (PA) may play a key role in healthy aging and thus in promoting good QoL.7 Previous studies have suggested that elderly patients with adequate PA levels live healthier lives and are at lower risk for cardiovascular disease.8-10Additionally, PA
has positive effects on psychological,11physical,12,13and emotional14well-being. However, there is still a need for studies on the benefits of PA for domains of well-being and QoL.
Several reviews have been conducted to synthesize information regarding the relationship between PA and domains of mental health and QoL.15-18Some of these reviews have suggested an association between PA and QoL.15-17 However, the results appear to be dependent on the instruments used to measure PA and QoL, as well as on the type of study design (i.e., most studies use cross-sectional designs). Additionally, many studies do not restrict their research to the elderly, making it difficult to assess the extent of the relationship between PA and QoL for this specific population. Finally, these reviews do not identify the consistency or direction of the association
Correspondence: Gislaine Cristina Vagetti, Centro de Pesquisa em Exercı´cio e Esporte (CEPEE), Universidade Federal do Parana´, Rua Corac¸a˜o de Maria, 92, BR 116, km 95 Jardim Botaˆnico, CEP 80215-370, Curitiba, PR, Brasil.
E-mail: [email protected]
Submitted May 23 2012, accepted Apr 28 2013.
ß2014 Associac¸a˜o Brasileira de Psiquiatria
of PA with different domains of QoL in the elderly. Thus, it is important to conduct a review to systematize informa-tion regarding the associainforma-tion between PA and QoL domains specifically in the elderly.
Understanding the way in which PA influences general and specific domains of QoL is an important factor for promoting health in the elderly. A review of the associa-tion between PA and QoL in the elderly will also identify gaps in the literature and allow for the development of new research on QoL in this population. With these factors in mind, the present study aims to systematically review information regarding the association of PA with specific domains of QoL in the elderly and to identify the study designs and measurement instruments most commonly used for the assessment of PA and QoL in the elderly in the literature published between 2000 and 2012.
Methods
Search strategy
Relevant articles for this review were identified by searching four electronic databases: MEDLINE/ PubMed, SPORTDiscus, SciELO, and LILACS. The search was limited to articles that were published between 2000 and 2012, in Portuguese, English, or Spanish. Keywords that characterized components of PA (physical activity, exercise, motor activity, functional capacity, and functionality) and the population of interest (elder, senior, elderly, older adults, and aged) were used in combination with the keyword for QoL (quality of life). Queries were performed in English and Portuguese. Keywords were combined using the Boolean operators ‘‘AND’’ and ‘‘OR.’’ We decided not to include theses, dissertations, or monographs, as conducting a systematic search of these would be logistically unfeasible.
The search was initially conducted in 2010 and updated on November 20, 2012. All of the selection processes and article evaluations were conducted in pairs (GCV, VCBF), and if there was disagreement between reviewers on the inclusion and exclusion criteria, the article in question was specifically discussed until a final consensus was reached. An initial analysis was performed on the basis of the titles of the manuscripts, and a second evaluation was carried out on the basis of the abstracts of all articles that met the inclusion criteria or could not be clearly ruled out. After examining the abstracts, all of the selected articles were retrieved and subsequently examined using the established inclusion criteria. A manual search of the reference lists of selected articles was also performed, and the principal authors of the manuscripts were contacted to identify other publications that met the inclusion criteria.
Inclusion and exclusion criteria
The following inclusion criteria were considered: i) original articles published in peer-reviewed journals that aimed to test for an association between PA and domains of QoL; ii) studies published between January 2000 and
November 2012; iii) samples with individuals aged 60 years or older or samples with a mean age in this age group. Intervention, cross-sectional, and longitudinal studies were considered in this review. However, we chose to restrict the review to intervention studies that had a sample size equal to or greater than 50 individuals and cross-sectional/longitudinal studies that had a sam-ple size equal to or greater than 100 individuals. This approach has been adopted in previous systematic reviews19,20with the aim of obtaining greater statistical power for detecting associations between variables and higher reliability in the interpretation of findings.
Several indicators of PA in elderly patients were included: self-administered scales for PA participation and electronic devices that objectively evaluated PA (e.g., accelerometers, pedometers, and heart rate monitors). Due to the direct relationship between PA and physical fitness, objective measures of physical or functional fitness (e.g., treadmill test) were also considered to be indicators of PA.
For QoL assessment, we decided that the search for studies should not be limited to those that used a generic instrument to assess QoL (e.g., WHOQoL-100 or SF-36), as this could exclude important intervention and cohort studies that examine the association between PA and domains of QoL. Therefore, we included studies that utilized self-reported QoL questionnaires, inventories, and well-being scales which contained QoL or HRQoL domains (well-being, life satisfaction, self-rated health) and the specific domains that comprise QoL or HRQoL (physical, psychological, social, cultural, mental, and spiritual domains).1-5
Quality assessment
Two independent reviewers (GCV, VCBF) evaluated the quality of the intervention studies using the Downs & Black checklist.21 This spreadsheet contains 27 items that assess information quality, internal validity (biases and confounders), study power, and external validity. Due to the difficulties in evaluating the quality of cross-sectional and observational articles, we decided to use the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE)22 checklist to evaluate the quality of articles with these designs. This checklist consists of 22 items and contains recommendations about what should be included for a more accurate and complete description of observational studies. All of the questions were coded as zero (representing poor quality) or one (representing adequate quality). Study quality scores could range from zero to 27 points in intervention studies and from zero to 22 points in cross-sectional and cohort studies; on both scales, the higher the score, the better the methodological quality of the study. In the event of differences in article evaluations between the two reviewers, the article was reassessed until they reached an agreement. The studies were classified into three groups according to their methodological quality. For this purpose, each study score was compared to the maximum score of the STROBE (22 points) or Downs &
Physical activity and quality of life in the elderly 77
Black (27 points) checklists. This strategy was used to stratify studies as being of high quality (o 70% total
score), moderate quality (50-69% total score), or low quality (, 50% total score).23 The instruments used to assess PA and QoL in the studies included in the review are described in Box 1.
Consistency and direction of the association between PA and QoL
An evaluation was performed to determine the consis-tency of the association between PA and domains related to QoL in the reviewed studies. Consistency was defined as the proportion of studies that displayed a positive association between PA measures and QoL measures. This strategy derived a classification of the PA-QoL associations into three groups: consistent (o 60%); moderate (30-59%); and inconsistent (f30% of studies
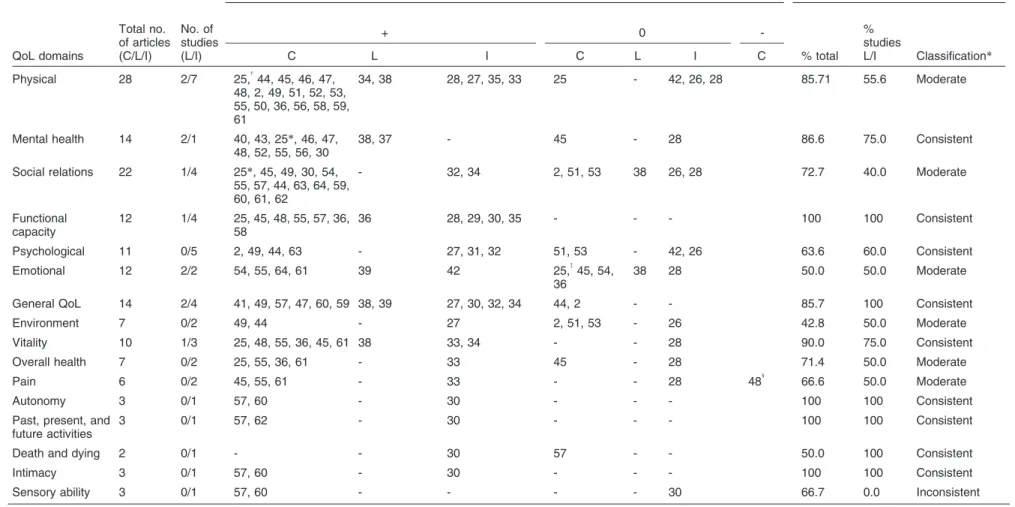
with positive associations). This classification has pre-viously been used elsewhere.23 The percentage of studies indicating a significant association between PA and QoL was calculated for the three types of study designs (intervention, longitudinal, and cross-sectional). For longitudinal and intervention studies, however, only the percentage was analyzed to determine the consis-tency of the association between PA and QoL. The direction of the association between PA and QoL domains was classified as positive, zero, or negative (Table 1).
Table 1 had the purpose to identify the association between PA and QoL domains, independently of the instrument used to assess QoL. Domains with similar contents were grouped into the same class, as follows: functional capacity: physical limitation,39 functional fit-ness35; social relationships: social function-ing,34,42,44,47,54,61,64 social engagement,53 social support,32 social participation29,56,60,62; and, physical: physical functioning,33,34,37,44,49,54,59,61physical health,46
physical role.54,61
Data extraction
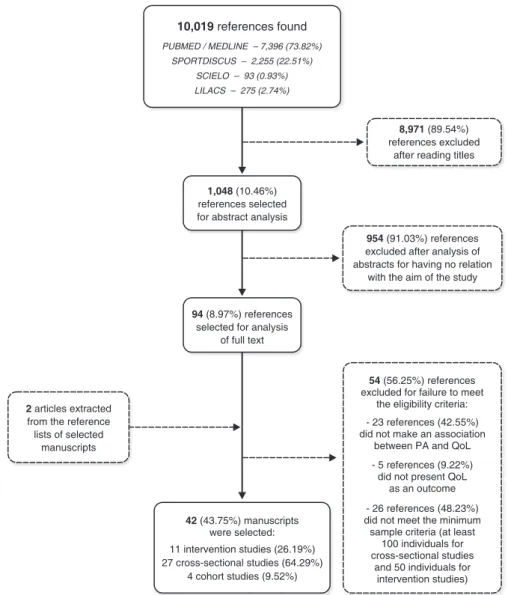
The following data were extracted from each of the included studies: study site, country, type and size of the sample, age of participants, application mode for the PA and QoL measurement instruments, adjustment vari-ables, and main results. The articles were arranged chronologically based on the year of publication and according to the methodological design that was used (intervention, longitudinal, or cross-sectional) (Figure 1). To evaluate the effect size for the QoL outcomes of each PA intervention, Cohen’s f was calculated using G*
Power statistical software version 3.1.2 (Franz Faul, Universitat Kiel, Germany).
Results
The detailed characteristics and main results of the studies reviewed are shown in a Supplementary Table online. A total of 10,019 articles were identified as
potentially relevant to this review. After analysis of titles, 1,048 studies were selected for the abstract reading process. Ninety-four studies were considered to be relevant after the abstract reading and were thus selected for a full-text reading. Two additional studies24,42 were included from the references of the selected articles; thus, 96 studies were considered relevant for this review. Of these, 54 studies (56.25%) were excluded because they did not meet the eligibility criteria: 23 (42.55%) did not address the association between PA and QoL variables, five (9.22%) did not present QoL as an outcome, and 26 (48.23%) had a sample of less than 100 individuals (in the case of cross-sectional studies) or less than 50 individuals (in the case of intervention studies). Therefore, the electronic search generated 42 studies (43.75%) deemed relevant for this systematic review.
Quality of studies
None of the studies achieved a maximum score (27 points) on the Downs & Black checklist;21the scores of
intervention studies ranged from 18 points2,25,29,40,54,58to 22 points.32,33,34,53 Using the STROBE checklist,22 only
three of the studies32-34,53achieved a maximum score of 22 points, and six studies2,25,29,40,54,58 obtained the minimum score (18 points). Based on the proposed cutoff points,2395.24% of the studies were classified as high-quality, and only two studies (4.76%) as being of medium quality.25,29
General characteristics of the studies
Eleven intervention studies and 31 observational studies were included. Twenty-seven of the observational studies were cross-sectional, and four were prospective cohorts. With the exception of three studies (7.14%),39,41,45the
included studies had a sample that was composed exclusively of the elderly (60 years or older). Most studies (73.81%) included participants of both sexes, and 11 studies (26.19%)2,25,27,33,35,36,40,46,54,56,62 only included
women. The majority of studies included healthy, elderly individuals who were living independently (92.86%), while others included institutionalized elderly subjects (7.14%)30,47,57 or elderly subjects with health problems.
These health problems included dizziness (2.38%),51 depression (2.38%),57 hypertension (2.38%),45 cancer (9.52%),28,33,49,59and osteoarthritis (2.38%).58
Evaluation of PA and QoL
Box 1 Instruments used to assess physical activity and quality of life in the studies included in the review (instruments listed by acronym; see full names in a footnote to the Supplementary Table online)
Physical activity
- Accelerometer: measures minutes and counts per day in moderate and vigorous physical activity.
- Andersen’s behavioral model: in this model, contextual and individual characteristics are conceptualized as factors that impede or enhance the individual’s health behaviors, most notably health care utilization and subsequent other outcomes related to health and satisfaction.
- Barthel Index: evaluates the functional potential of the individual, assessing the degree of assistance required in 10 independent activities, such as feeding, personal hygiene, dressing, bladder and bowel control, walking, climbing stairs, and transferring from wheelchair to bed.
- CHAMPS: assesses weekly frequency and duration of various physical activities typically undertaken by older people. - ECOG scale: a scale that ranges from 0 (able to perform physical activity without restriction) to 4 (completely unable to
perform physical activity, confined to bed or wheelchair).
- FES-I: composed of 10 items rated on a Likert scale (1 = no concern, 4 = very concerned) to estimate the level of concern about falling during physical activity and social events within and outside the home in the elderly.
- GLTEQ: an instrument of habitual physical activity during the last 7 days. It includes three items measuring the frequency of light, moderate, and vigorous physical activity.
- HAP: Brazilian version consisting of 94 items addressing participation in physical activity, which can be categorized according to the International Classification of Functioning, Disability and Health.
- IPAQ: composed of items related to frequency and duration of physical activity at different intensities (light, moderate, vigorous), in periods of at least 10 minutes in habitual week days.
- Johnson Space Center physical activity scale: composed of a Likert scale on participation in physical activity in the last month, ranging from 0 (avoid physical activity) to 7 (participates in vigorous physical activity regularly, for 3 or more hours/week). Considered active when reporting scores 3 or higher on the Likert scale.
- LL-FDI: composed of items scored on a Likert scale (1 = not, 5 = no limitations) to assess functional limitations in older adults.
- PASE: 10 items designed to assess frequency and duration of physical activity in the elderly, in areas such as leisure, family, and professional activity.
- Pedometer: analyzes the number of steps per day.
- PSW: composed of five items scored on a Likert scale (1 = strongly disagree, 7 = strongly agree) to assess the overall judgment of the individual’s life satisfaction.
- Exercise Self-Efficacy Scale: measures an individual’s belief in his or her ability to perform physical activity three times per week, at moderate intensity, for 40 min or more. For each item, participants indicate their confidence in completing the physical activity, ranging from 0% (no confidence) to 100% (highly reliable).
- Questionnaire developed to assess physical activity for the BRFSS: six questions on participation in moderate/vigorous physical activity in a typical week.
- Self-Efficacy for Walking Scale: investigates the individual’s belief in his or her physical ability to successfully complete a given distance in 4 minutes. For each item, participants indicate their confidence in performing the behavior on a percentage scale ranging from 0% (no confidence) to 100% (highly confident).
- The Activity-Specific Balance Confidence Scale: assesses the individual’s confidence in performing various daily activities without compromising their balance.
- The Older American Resources and Services Scale: composed of 14 daily activities and work. The subjects were grouped into four categories: independent (maximum score on the physical activity scale), lightly dependent (to perform one to three activities), moderately dependent (to perform four to six activities), and severely dependent (to perform seven or more physical activity).
- YPAS: list of work and recreational physical activity performed during a habitual week.
Quality of life
- EORTC-QLQ-C30: measures physical, role, emotional, social and cognitive functioning, as well as global quality of life and three symptom types: fatigue, pain, and nausea/vomiting.
- GDS: used to identify symptoms of depression in the elderly. Respondents may be classified as ‘‘normal’’ (0-9 points), ‘‘mildly depressed’’ (10-19 points), or ‘‘severely depressed’’ (20-30 points).
- HRQL: questionnaire consisting of 12 domains that cover a range of psychological and physical functions: functional status, vitality, social function, physical pain, emotions, general health, and mental health.
- IADL: composed of eight items to assess independent living skills and aspects of quality of life related to physical
Physical activity and quality of life in the elderly 79
scales. Four studies (9.52%)26,31,37,47 used a direct measure of PA (accelerometer and/or pedometer).
The most widely used questionnaire to assess QoL was the Short Form-36 (SF-36) (33.33%),27,28,33,37,
40,42,44,47,49,54,57,58,61,64
followed by the World Health Organization Quality of Life Assessment –– Abbreviated Version (WHOQoL-Bref) (19.04%),2,26,43,48,50,52,63,64 the Short Form-12 (SF-12) (7.14%),36,46,51the World Health Organization Quality of Life Assessment –– Module for Older Adults (WHOQoL-Old) (9.52%),29,56,60,62 the Satisfaction with Life Scale (SWLS) (7.14%),36,46,55 a questionnaire developed for the Behavioral Risk Factor Surveillance System (BRFSS) (7.14%),39,41,45 and the World Health Organization Quality of Life 100 (WHOQoL-100)(4.76%).25,32The following instruments were used in one (2.38%) study each: Medical Outcomes Study (MOS),24 Neuropsychiatric Inventory (NPI),30 Instru-mental Activities of Daily Living Scale (IADL),31 Lund Gerontology Centre Life Quality Questionnaire (LGC),53 European Organization for Research and Treatment of Cancer Quality of Life questionnaire, version C30 (EORTC-QLQ-C30),59 and Health-Related Quality of
Life Questionnaire (HRQL).34 Due to the variability of
PA and QoL assessment tools, a meta-analysis could not be performed.
Characteristics of the intervention studies
Of the intervention studies, three (27.27%)25,29,32 were conducted in Brazil, and the rest in the following countries: United States (9.1%),24England (9.1%),26the Netherlands (9.1%),27 Australia (9.1%),28 France (9.1%),30 Japan (9.1%),31 Canada (9.1%),33 and Iceland (9.1%).34
The duration of the 11 intervention studies ranged from 329to 1224,26,31,33 months, but only six of these studies were randomized. The duration of each PA session ranged from 3030 to 90 minutes,31 and the weekly frequency (number of sessions) ranged from one31 to five33sessions per week.
Twelve different exercise programs were employed in the analyzed intervention studies. Five studies (45.45%)24,26,29,31,32 used programs focused on muscle strength, three (27.27%)27,29,34used programs focused on muscle endurance exercises, and four (36.36%)24,26,31,33
focused on aerobic endurance exercises. Four studies
function. Scores range from 0 (low function, dependent) to 8 (high function, independent) for women, and 0 to 5 for men. This instrument is intended to be used among non-institutionalized elderly.
- LGC questionnaire: a subscale of a previously validated questionnaire consisting of nine items that seek to evaluate factors related to quality of life in the elderly, especially well-being and social engagement.
- MOS: composed of 116 items that assess structural social support (social network), functional support, and physical, mental, and general health. It consists of seven components of health-related quality of life (physical functioning, pain, emotional well-being, energy/fatigue, sleep problems, sense of mastery, and self-esteem).
- MUNSH: comprises 24 items designed to evaluate ‘‘happiness’’ in the elderly. This instrument consists of four subscales: positive affect (PA), negative affect (NA), positive experiences (EP), and negative experiences (EN). The total score is obtained by the formula (PA - NA) + (EP - EN), and ranges from 0 to 48 points.
- NPI: composed of 12 neuropsychiatric symptoms (for example, delusions, hallucinations, agitation/depression, and aggression), with scores ranging from 0 to 144 points. Higher scores indicate greater behavioral problems and poorer quality of life.
- PGC morale scale: designed to measure the dimensions of emotional adjustments in people aged 70 to 90, providing an assessment of psychological well-being of older people.
- Physical Self-Perception Profile: developed for self-perceptions related to a ‘‘physique’’ based on a hierarchical model. In this model, global self-esteem is at the peak of the physical hierarchy, self-esteem and competence as a field of sports, physical strength and condition as subdomains.
- Questionnaire developed for the BRFSS to assess quality of life: composed of four questions related to number of days during the 30 days preceding the study, in which the individual did not have a good health status (general, physical, and mental).
- SF-12: a version of the SF-36 with a small number of items (only 12) that can be grouped into two components (physical and mental health).
- SF-36: a shortened version of the MOS questionnaire comprising 36 items covering eight components (domains): functional capacity, physical aspects, pain, general health, vitality, social, emotional aspects, mental health.
- SWLS: composed of five items that seek to estimate overall life satisfaction.
- TMIG-IC: this scale, comprising 13 items, enables estimation of the competence of elderly individuals to perform everyday physical activity, with scores ranging from 0 to 13 points.
Table 1 Summary of the association of PA and different aspects of QoL
QoL domains
Total no. of articles (C/L/I)
No. of studies (L/I)
Direction of association with PA (numbers are the study reference number) Consistency of the association with PA
+ 0
-% total % studies
L/I Classification*
C L I C L I C
Physical 28 2/7 25,{44, 45, 46, 47, 48, 2, 49, 51, 52, 53, 55, 50, 36, 56, 58, 59, 61
34, 38 28, 27, 35, 33 25 - 42, 26, 28 85.71 55.6 Moderate
Mental health 14 2/1 40, 43, 25*, 46, 47, 48, 52, 55, 56, 30
38, 37 - 45 - 28 86.6 75.0 Consistent
Social relations 22 1/4 25*, 45, 49, 30, 54, 55, 57, 44, 63, 64, 59, 60, 61, 62
- 32, 34 2, 51, 53 38 26, 28 72.7 40.0 Moderate
Functional capacity
12 1/4 25, 45, 48, 55, 57, 36, 58
36 28, 29, 30, 35 - - - 100 100 Consistent
Psychological 11 0/5 2, 49, 44, 63 - 27, 31, 32 51, 53 - 42, 26 63.6 60.0 Consistent
Emotional 12 2/2 54, 55, 64, 61 39 42 25,{45, 54, 36
38 28 50.0 50.0 Moderate
General QoL 14 2/4 41, 49, 57, 47, 60, 59 38, 39 27, 30, 32, 34 44, 2 - - 85.7 100 Consistent
Environment 7 0/2 49, 44 - 27 2, 51, 53 - 26 42.8 50.0 Moderate
Vitality 10 1/3 25, 48, 55, 36, 45, 61 38 33, 34 - - 28 90.0 75.0 Consistent
Overall health 7 0/2 25, 55, 36, 61 - 33 45 - 28 71.4 50.0 Moderate
Pain 6 0/2 45, 55, 61 - 33 - - 28 481 66.6 50.0 Moderate
Autonomy 3 0/1 57, 60 - 30 - - - 100 100 Consistent
Past, present, and future activities
3 0/1 57, 62 - 30 - - - 100 100 Consistent
Death and dying 2 0/1 - - 30 57 - - 50.0 100 Consistent
Intimacy 3 0/1 57, 60 - 30 - - - 100 100 Consistent
Sensory ability 3 0/1 57, 60 - - - - 30 66.7 0.0 Inconsistent
C = cross-sectional studies; I = intervention studies; L = longitudinal studies; PA = physical activity; QoL = quality of life. *Classification previously adopted, considering only the percentage of longitudinal and intervention studies (Strong et al.24) {Guallar-Castillo´n et al.,42only in men.
{Guallar-Castillo´n et al.,42in light PA. 1
Lobo et al.47: higher pain scores reflect lower QoL; therefore, this was also considered in estimating the consistency of association between PA and QoL.
Studies that sought to identify a common specific QoL domain, independently of the instrument used to assess QoL, were grouped into the same class of the evidence summary, as follows: functional capacity: physical limitation,39functional fitness35; social relationships: social functioning,34,42,44,47,54,61,64social engagement,53social support,32social participation29,56,60,62; and
physical: physical functioning,33,34,37,44,49,54,59,61physical health,46physical role.54,61
Physical
activity
and
quality
of
life
in
the
elderly
81
Rev
B
ras
Psiquiatr.
(36.36%)24-26,31 focused on exercises for developing flexibility, and two (18.18%)30,31used a program focused
on the development of body awareness.
The majority of the intervention studies (81.81%)22,26-31, 33,34
employed programs based on moderate-to-vigorous PA. Only one study (9.09%)25developed an intervention
program consisting of low-intensity PA.
Four intervention studies (36.36%)28,30,33,34used
sta-tistical approaches that allowed for the inclusion of possible confounding variables. The most commonly used variables were age, gender, and number of comorbidities/diseases.
Regarding the effect size, the intervention studies showed values between 0.1425and 0.7027in the physical domain, 0.0225and 0.2725 in the psychological domain, 0.2033and 1.0627in the bodily pain domain, 0.0934and 0.6329 in the social domain, 0.1825 and 0.2025 in the environmental domain, 0.1834 and 0.2233 in vitality, 0.4129 and 0.6029 in autonomy, 0.1125 and 0.2525 in
spiritual, 0.3629and 0.4529in intimacy, 0.3629and 0.7729
in past, present, and future activities, and, finally, 0.5629 and 1.1329in the general QoL domain.
Characteristics of the longitudinal (cohort) studies
Of the four longitudinal studies, three (75%)35,36,38 were conducted in the U.S. and one (25%)37in Japan. Of these studies, one (25%)37had subjects who were followed for 1 year, two (50%)35,36for 2 years, and one (25%)38for 5 years. Only one study (25%)37used a direct measure of PA (pedometers), while the rest used the PASE.35,36,38 Three studies (75%)35,36,38 used self-efficacy as a mediating variable between PA and QoL.
All longitudinal studies35-38used the covariance model for data analysis, but one study (25%)37also used linear regression. Three studies (75%)35-37included
confound-ing variables into the model. The most commonly used variables were age, race, education level, and chronic health conditions.
Characteristics of cross-sectional studies
Of the 27 cross-sectional studies, 11 (40.74%)2,48,50,52,54,
56,58,60-63 were conducted in Brazil, eight (29.63%)39,41, 44-46,49,55,64
in the U.S., two (7.40%)51,53in Sweden, two (7.40%)42,57in Spain, and one (3.70%) each in China,43 Portugal,47England,59and Australia.40
Of these 27 studies, only one (3.70%)47 used a direct
measure of PA (accelerometer). Five (18.52%)40,42,51,53,61 used a questionnaire developed for the study itself, seven (25.92%)2,54,56,58,60,62,63used the IPAQ, three (11.11%)39,
41,45
used the questionnaire developed for the BRFSS, and 11 (40.74%) used other instruments. To evaluate QoL, the majority of the studies (37.04%)40,42,44,47,49,54,57,58,61,64used the SF-36. Five studies (25.92%)2,43,48,50,52,63,64 used the
WHOQoL-Bref, three (11.11%)39,41,45 used the BRFSS scale, three others (11.11%)56,60,62 used the WHOQoL-Old, two (7.40%)46,51 used the SF-12, and three (11.11%)53,55,59used other instruments.
The majority of the studies (59.26%)2,37,39,40,
42,43,45,51,53,56,58,59,61-64 used regression analysis. Six
studies (22.22%)47,48,50,52,54,57used analysis of variance, and five (18.55%),44,46,49,55,60 analysis of covariance. Sixteen studies (59.26%)39,41,42,44,45,49,51-53,55,59-64 used statistical approaches that allowed for the inclusion of possible confounding variables. The most commonly used variables were age, race/ethnicity, gender, educa-tional level, and health problems.
Summary of evidence for the association between PA and QoL
Table 1 summarizes the main results regarding the association between PA and QoL domains. Different instruments were used to obtain QoL scores, which resulted in a wide variety of QoL domains being evaluated in the studies included in this review. The most commonly evaluated domains were physical health, mental health, functional capacity, psychological, emotional, social relationships, environment, pain, overall health, general QoL, and vitality.
The consistency of the associations was assessed in longitudinal and intervention studies. The results of this review showed a consistent and positive association between PA and the functional capacity (100%), general QoL (100%), autonomy (100%), past, present, and future activities (100%), death and dying (100%), intimacy (100%), mental health (75%), vitality (75%) and psycho-logical (60%) domains. There was a moderate associa-tion between PA and the following domains: physical (55.6%), social relations (40%), emotional (50%), overall health (50%), pain (50%), and environment (50%). The results showed an inconsistent association between PA and the sensory ability domain.
Discussion
Characteristics of the study
There was a strong concentration of studies in some countries, especially the U.S. and Brazil, which together
accounted for 61.90% of the included studies. This characteristic makes it difficult to generalize the results to populations with socio-cultural characteristics that are different from those of the countries in which the studies were conducted. Most studies were performed in devel-oped countries, although Brazil is a developing nation and had a fairly large number of studies on this topic. The development of Brazilian and international literature on the importance of PA for the promotion of QoL in the elderly is also supported by the significant increase in the number of publications since 2005 (see Supplementary Table online). This progression should be accompanied by the conduction of research of a higher level of methodological quality to confirm the causal relationship between PA and QoL15and to understand the mechan-isms of this relationship.38
Regarding participant age, the WHO defines the elderly as individuals aged 65 years or older in developed countries and 60 years or older in developing countries.65 However, some studies did not follow this guideline for inclusion in their samples. Additionally, some studies had samples consisting exclusively of elderly women. Many scientific studies involving this age group typically have a greater number of female participants,18 possibly because i) women have a longer life expectancy (6 years longer on average), ii) women have a higher level of social support, are more likely to seek new sources of support, have a greater ability to form bonds, enjoy affectionate relations, and assemble in a group, and iii) women have lower biological vulnerability, as the rate of lethal diseases is higher among men.66
This review shows some variability among the studies regarding how PA is measured. Only three studies31,37,47 used direct measures to assess PA. The remainder used subjective measures of PA, and in some cases, these measures were created by the authors themselves without assessing the validity and reliability of PA estimates based on these instruments. The use of questionnaires offers low cost and ease of application; however, information reported by individuals has limited accuracy, as they tend to overestimate participation in PA.67A good test of reliability and validity of self-reported measures of PA may be to compare data from the same population, thus facilitating the identification of temporal changes in participation in PA and its possible influences on health factors.16
QoL assessment in the elderly was also performed using different methods. Among the studies included in this review, the most widely used instrument for measur-ing QoL was the SF-36. This questionnaire was devel-oped to assess HRQoL based on the MOS, which is a questionnaire that was published in 1990. The SF-36 contains 36 items that are divided into eight scales and can also be grouped into physical and mental compo-nents. The SF-36 has been translated into several languages and validated for several cultures. Research has been conducted using the SF-36 in over 40 countries.68The instrument allows for the measurement of health dimensions and can assess the impact of disease and the benefits of treatment. It is also a good
Physical activity and quality of life in the elderly 83
predictor of mortality.69 In Brazil, the instrument was translated and validated by Ciconelli et al.70 The
popularity of the SF-36 may be due to the year of its development, in the early 1990s. Additionally, the SF-36 allows for the assessment of HRQoL and its specific domains, which represents an outcome of interest in the research models included in this review (e.g., studies of institutionalized elderly or those with health problems).
Another instrument used in the studies was the QoL assessment questionnaire developed by the WHO, which is widely used in research and clinical practice.5 This questionnaire was used in nine of the studies included in this review in the WHOQoL-100, WHOQoL-Bref and WHOQoL-Old versions. This prevalence demonstrates the importance of these instruments for evaluating QoL in cases in which general QoL and its specific domains is an outcome of interest.
It bears stressing that different instruments and QoL domains have specific properties (e.g., some instruments assess general QoL while other assess HRQoL, but both evaluate QoL in different ways, implying different concepts of QoL). Therefore, the lack of data limits the general-ization and comparison of the results of different studies, since QoL domains are also affected by a number of factors related to culture, physical, and social environment of communities and societies.71,72Standardization of QoL assessment instruments in studies with elderly participants is essential for future research that seeks to identify the causal relationship between PA and QoL.
Association between PA and QoL
In general, the studies included in this review showed a positive association between PA and QoL in the elderly. However, the consistency of the association varied across different samples, as did the type of intervention/ observation and the instruments used to measure the dependent variable. Only a few of the studies in which associations between PA and QoL domains were observed were methodologically robust (with sample randomization or adequate control for confounders). Furthermore, the effect sizes for the associations derived from experimental studies were generally small or medium and usually highly variable between studies. Therefore, the consistency of findings, by itself, does not define the possible causal association between PA and QoL domains as clinically robust.
The summary of the study evidence (see Table 1) indicates that PA is consistently associated with the following QoL domains: functional capacity; general QoL; autonomy; past, present, and future activities; death and dying; intimacy; mental health; vitality; and psychological. These associations suggest that PA may promote physical independence as well as essential mental aspects of QoL. However, this review showed that the associations between PA and the physical, emotional, overall health, social relations, pain, and environment domains of QoL are moderate. These associations may be related to the fact that PA promotes physical independence by improving functional capacity and
physical health, which are essential for individual auton-omy. These positive changes in life may induce increases in the states of mental health and general QoL.
Finally, only one domain presented an inconsistent association with PA: the sensory ability domain (see Table 1). Conflicting results regarding the association of PA and different domains are present in a number of studies.2,25,26,29,31,44,50,52,53,55This inconsistency may be due to the nature of PA and to the use of different methodologies and instruments for assessment of PA and QoL. The nature of PA programs for the elderly (aerobic, anaerobic, strength training, stretching exercises, social leisure activities, and others) may relate to QoL domains in a unique way, resulting in different associations. Standardization of methodologies for intervention and long-itudinal studies is required, as is standardization of the instruments of QoL and type of PA used in these studies.
Other systematic reviews that were conducted with the general population have shown a positive association between PA and QoL,71but further studies are needed to evaluate the consistency of this association. It is important to note that not all of the studies included in the present review used statistical approaches that could control for potential confounding variables in the associa-tion between PA and QoL.
The present review provides evidence for a causal relationship between PA and some domains of QoL in the elderly. We cannot sustain that a causal relationship exists for all domains of QoL, because most studies that showed significant associations used cross-sectional designs, thus precluding any inferences about causality. The studies included in this review proposed to elucidate and provoke further discussion about the association between PA and QoL in the elderly. First, some studies sought to identify possible explanatory variables for the association between PA and QoL, primarily testing the importance of self-efficacy for PA as a mediating variable in this association.35,46 Second, other studies examined the dose-response relationship between PA and QoL (i.e., analysis of PA frequency and intensity and the impact of these factors on QoL). These studies will be discussed in greater detail in the following sections. Third, the lack of agreement among studies investigating the association between PA and specific QoL domains demonstrates the need for standardization of methodologies and instru-ments in future studies. These studies may guide the development of actions for the promotion of PA, QoL, and other health factors in the elderly.
Association between PA and QoL: the mediating role of self-efficacy for PA
In this area of study, mediating variables are mechanisms that can show the connection between PA and QoL in the elderly and may influence the consistency and direction of this relationship.15Although the results of recent literature
typically described in the literature, and appears to involve a number of variables. Self-efficacy for PA appears to be an initial step in the study of variables that mediate the association between PA and QoL.15
Previous studies have suggested that self-efficacy for PA has a mediating impact on the association between PA and QoL. For example, the cross-sectional study by McAuley et al.46 presented evidence to support such a position, arguing that self-efficacy, the central component of social cognitive theory, has been consistently shown to be a determining factor in PA participation. The authors concluded that elderly women who were more active had greater self-efficacy, which was associated with more positive states of both physical health and mental health. An intervention study38 showed that self-efficacy and affect are important mediators of the effectiveness of a PA program to promote QoL. This study indicated that changes in PA practice 5 years after intervention are associated with increased affect, which, in turn, is associated with increased QoL. Participation in PA may influence individual assessments of cognitive abilities, i.e., self-efficacy and affect, during exercise. This is the main theoretical basis for the mediating role of these variables in the association between PA and QoL.73 In their examination of the literature, Rejeski et al.15used similar arguments to explain the relationship between PA and QoL, proposing, for example, that self-efficacy is an important mediator in this relationship.
The evidence of these and other studies15,35,36,38 represents the first attempts to test potential mediators of the relationship between PA and QoL. These analyses are based on theoretical models and have important implications for how PA promotion programs can be structured for improvement of QoL in the elderly. This research highlights the need for the study of other variables that might explain the relationship between PA and QoL (e.g., enjoyment of PA), as well as the mediating role of these variables in the relationship between PA and other domains of QoL (e.g., the psychological domain). Nonetheless, current evidence suggests that PA inter-ventions and programs should orient their activities toward providing experiences, comments, and informa-tion that serve to increase awareness of the percepinforma-tion of cognitive abilities of the elderly in relation to their participation in PA.
Intensity and frequency of PA
The dose-response relationship between PA and QoL domains was also examined in some studies (i.e., different frequencies and intensities of PA and the impact of these factors on QoL).28,33,34,37,41,42,45,50,51,53,56,59,63
One study included in this review highlighted that light PA was associated with the following SF-36 scales: general health, vitality, social function, and mental health.42 In
another study, light PA was associated with 40% lower odds of having low scores in the physical and mental domains of HRQoL.51
In a study by Vareja˜o et al.,25in which an intervention program consisting of low-intensity PA was implemented,
no significant improvements were found in QoL domains. A previous longitudinal study demonstrated that the practice of moderate PA was predictive of an improvement in the functional capacity domain of QoL.74 Active individuals maintain or improve their physical abilities and are better prepared to perform any kind of work in their daily lives, which, in turn, can promote this domain of QoL.36,75
Other cross-sectional studies showed that moderate and/or vigorous intensity PA was also associated with the following QoL domains: functional capacity,42,47,57,59,76
global QoL,59 pain,47,76 physical,59 vitality,42,44,47,57,76 mental health,76 and general health.42,57 Vigorous PA was associated with 50-70% lower odds of having low scores in the physical and mental domains51and a 15% increase in the odds of experiencing social engagement and emotional support.53Non-participation in moderate or vigorous PA increased the odds of experiencing 14 or more unhealthy days (physical or mental HRQoL domains) when compared to performing moderate or vigorous PA.39,41
Thus, studies suggest that different PA intensities contribute to different domains of QoL. It should be noted, however, that most of these studies are cross-sectional, making it difficult to draw conclusions about the associa-tion between different PA intensities and qualities and specific QoL domains.
Other studies have sought to test the impact of the frequency of PA on QoL domains. For example, Alexander et al.50 used the Human Activity Profile
(HAP) and WHOQoL-Bref to assess QoL and found that a greater weekly frequency of PA was associated with higher values in the physical domain of QoL. Likewise, Grimmett59found that practicing at least five PA sessions per week was associated with higher scores in several QoL domains, such as global QoL and the physical, functional capacity, and social domains.
In another study, elderly patients who performed moderate PA with low weekly frequency (1 or 2 days) had a 30% greater chance of experiencing 14+ unhealthy days when compared to those who performed moderate PA 5 or 6 days a week.41 Analysis of the relationship between PA frequency and QoL domains is even rarer.
On the basis of the studies included in this review, it is clear that the evidence is contradictory regarding the dose-response relationship between PA and QoL, and that this relationship may be dependent on the QoL domain assessed (e.g., the impact of PA frequency on the physical domain of QoL may be different from its impact on the psychological domain). More intervention studies are required to investigate the impact of the intensity and frequency of PA on QoL. It is also important that future studies seek approaches that permit the inclusion of confounding variables in the statistical models. Such approaches will help establish the cause and effect relationship between PA and QoL by control-ling for possible intervening variables.
Limitations of the study
This review had some limitations that should be high-lighted. The first limitation concerns the possibility that
Physical activity and quality of life in the elderly 85
some relevant studies were not included. The electronic search was limited to studies published between 2000 and 2012 and indexed in the PubMed/MEDLINE, SPORTDiscus, SciELO, and LILACS databases. It is possible that relevant studies published prior to that period or indexed in other databases are missing. The search for studies was also limited to the peer-reviewed literature; therefore, unpublished data, theses, dissertations, and institutional position papers were not included. It is important to emphasize that the study of the association between PA and QoL is a topic of relatively recent interest, as the main instruments for assessing QoL were only developed in the 1990s. Additionally, major original studies are published in the peer-reviewed literature. Therefore, it is believed that the most important studies examining the association between PA and QoL and published in this period are summarized in this review.
A second limitation is the small number of studies that evaluated the different domains of QoL. For example, the domains past, present, and future activities, death and dying, intimacy, and sensory ability were only evaluated in three studies,29,60,62and the pain domain of QoL was only evaluated in seven studies.27,33,37,44,47,57,61 Other QoL domains were assessed in several studies (e.g., physical domain). However, the vast majority of studies were cross-sectional. This type of design has important limitations in seeking to establish the causal relationship between PA and QoL. Longitudinal and intervention studies are needed to assess different domains of QoL and the impact of PA on these outcomes.
Conclusions
The literature on the association between PA and QoL in the elderly is mainly composed of cross-sectional studies. Different questionnaires are used to assess PA, and the long and short versions of SF-36 and WHOQoL-Bref are the most used questionnaires to assess QoL. There was a consistent positive association between PA and the following QoL domains: functional capacity; general QoL; autonomy; past, present, and future activities; death and dying; intimacy; psychological; vitality; and mental health. This evidence supports the notion that promoting PA in the elderly may have an impact beyond functional capacity and mental health, as it was associated with a positive perception of general QoL. PA had a positive association, albeit moderate or inconsistent, with other domains of QoL in the elderly. The results also showed that PA may not be associated with some QoL domains (e.g., sensory ability), but further investigations are needed.
Evidence on the impact of the frequency and intensity of PA on QoL domains is still limited. Longitudinal and intervention studies are needed to better understand the dose-response relationship between PA and QoL. The association between PA and QoL is clearly more complex than is generally stated in the literature, and seems to involve some mediating variables, such as self-efficacy for PA and affect. Further studies are needed to support this hypothesis.
Acknowledgements
This study has received grants from Fundac¸a˜o Arauca´ria and Coordenac¸a˜o de Aperfeic¸oamento de Pessoal de Nı´vel Superior (CAPES).
Disclosure
The authors report no conflicts of interest.
References
1 Irigaray TQ, Trentini CM. Qualidade de vida em idosas: a importaˆncia da dimensa˜o subjetiva. Estud Psicol (Campinas). 2009;26:297-304.
2 Mazo GZ, Mota J, Gonc¸alves LHT, Matos MG, Carvalho J. Atividade fı´sica e qualidade de vida de mulheres idosas da cidade de Floriano´polis, Brasil. Rev Port Cien Desp. 2008;8:414-23. 3 Spirduso WW, Cronin DL. Exercise dose-response effects on quality
of life and independent living in older adults. Med Sci Sports Exerc. 2001;33:S598-608.
4 Bowling A. Ageing well. Quality of life in old age. Maidenhead: Open University; 2005. p. 139.
5 The World Health Organization Quality of Life Assessment (WHOQoL): position paper from the World Health Organization. Soc Sci Med. 1995;41:1403-9.
6 Seidl EMF, Zannon CMLC. Qualidade de vida e sau´de: aspectos conceituais e metodolo´gicos. Cad Saude Publica. 2004;20:580-8. 7 World Health Organization (WHO). Recomendaciones mundiales sobre
actividad fı´sica para la salud [Internet]. 2010. [cited 2013 Oct 16]. http:// whqlibdoc.who.int/publications/2010/9789243599977_spa.pdf 8 Paterson DH, Jones GR, Rice CL. Ageing and physical activity:
evidence to develop exercise recommendations for older adults. Can J Public Health. 2007;98:S69-108.
9 Ro´z˙an´ska-Kirschke A, Kocur P, Wilk M, Dylewicz P. The fullerton fitness test as an index of fitness in the elderly. Med Rehabil. 2006;10:9-16.
10 American College of Sports Medicine, Chodzko-Zajko WJ, Proctor DN, Fiatarone Singh MA, Minson CT, Nigg CR, et al. American College of Sports Medicine position stand. Exercise and physical activity for older adults. Med Sci Sports Exerc. 2009;41:1510-30. 11 Bowling A, Banister D, Sutton S, Evans O, Windsor J. A
multi-dimensional model of the quality of life in older age. Aging Ment Health. 2002;6:355-71.
12 Stewart KJ, Turner KL, Bacher AC, DeRegis JR, Sung J, Tayback M, et al. Are fitness, activity, and fatness associated with health-related quality of life and mood in older persons? J Cardiopulm Rehabil. 2003;23:11-21.
13 Morimoto T, Oguma Y, Yamazaki S, Sokejima S, Nakayama T, Fukuhara S. Gender differences in effects of physical activity on quality of life and resource utilization. Qual Life Res. 2006;15:537-46. 14 Lee C, Russell A. Effects of physical activity on emotional well-being among older australian women: cross-sectional and longitudinal analyses. J Psychosom Res. 2003;54:155-60.
15 Rejeski WJ, Mihalko SL. Physical activity and quality of life in older adults. J Gerontol A Biol Sci Med Sci. 2001;56:23-35.
16 Bize R, Johnson JA, Plotnikoff RC. Physical activity level and health-related quality of life in the general adult population: a systematic review. Prev Med. 2007;45:401-15.
17 Oliveira AC, Oliveira NMD, Arantes PMM, Alencar MA. Qualidade de vida em idosos que praticam atividade fı´sica - uma revisa˜o sistema´tica. Rev Bras Geriatr Gerontol. 2010;13:301-12.
18 Guimara˜es JMN, Caldas CP. A influeˆncia da atividade fı´sica nos quadros depressivos de pessoas idosas: uma revisa˜o sistema´tica. Rev Bras Epidemiol. 2006;9:481-92.
19 Chen X, Beydoun MA, Wang Y. Is sleep duration associated with childhood obesity? A systematic review and meta-analysis. Obesity (Silver Spring). 2008;16:265-74.
21 Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52:377-84.
22 Elm EV, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP, Strobe iniciative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Rev Esp Salud Publica. 2008;82:251-9.
23 Strong WB, Malina RM, Blimkie CJ, Daniels SR, Dishman RK, Gutin B, et al. Evidence based physical activity for school-age youth. J Pediatr. 2005;146:732-7.
24 King AC, Pruitt LA, Phillips W, Oka R, Rodenburg A, Haskell WL. Comparative effects of two physical activity programs on measured and perceived physical functioning and other health-related quality of life outcomes in older adults. J Gerontol A Biol Sci Med Sci. 2000;55:M74-83.
25 Vareja˜o RV, Dantas EHM, Matsudo SM. Comparac¸a˜o dos efeitos do alongamento e do flexionamento, ambos passivos, sobre os nı´veis de flexibilidade, capacidade funcional e qualidade de vida do idoso. R Bras Ci Mov. 2007;15:87-95.
26 Fox KR, Stathi A, McKenna J, Davis MG. Physical activity and mental well-being in older people participating in the better ageing project. Eur J Appl Physiol. 2007;100:591-602.
27 de Vreede PL, van Meeteren NL, Samson MM, Wittink HM, Duursma SA, Verhaar HJ. The effect of functional tasks exercise and resistance exercise on health-related quality of life and physical activity. A randomised controlled trial. Gerontology. 2007;53:12-20. 28 Morey MC, Sloane R, Pieper CF, Peterson MJ, Pearson MP,
Ekelund CC, et al. Effect of physical activity guidelines on physical function in older adults. J Am Geriatr Soc. 2008;56:1873-8. 29 Rocha CAQC, Paixa˜o JA, Tucher G, Botaro CA, Bruno RX. Efeitos
de um programa de forc¸a e resisteˆncia muscular na qualidade de vida de idosos. Braz J Biomotricity. 2009;3:271-80.
30 Dechamps A, Diolez P, Thiaudie`re E, Tulon A, Onifade C, Voung T, et al. Effects of exercise programs to prevent decline in health-related quality of life in highly deconditioned institutionalized elderly persons: a randomized controlled trial. Arch Intern Med. 2010;170:162-9.
31 Taguchi N, Higaki Y, Inoue S, Kimura H, Tanaka K. Effects of a 12-month multicomponent exercise program on physical performance, daily physical activity, and quality of life in very elderly people with minor disabilities: an intervention study. J Epidemiol. 2010;20:21-9. 32 Pernambuco C, Rodrigues B, Bezerra J, Carrielo A, Fernandes A, Vale R, et al. Quality of life, elderly and physical activity. Health. 2012;4:88-93.
33 Courneya KS, Tamburrini AL, Woolcott CG, McNeely ML, Karvinen KH, Campbell KL, et al. The Alberta Physical Activity and Breast Cancer Prevention Trial: quality of life outcomes. Prev Med. 2011;52:26-32.
34 Geirsdottir OG, Arnarson A, Briem K, Ramel A, Tomasson K, Jonsson PV, et al. Physical function predicts improvement in quality of life in elderly Icelanders after 12 weeks of resistance exercise. J Nutr Health Aging. 2012;16:62-6.
35 Mcauley E, Morris KS, Doerksen SE, Motl RW, Liang H, White SM, et al. Effects of change in physical activity on physical function limitations in older women: mediating roles of physical function performance and self-efficacy. J Am Geriatr Soc. 2007;55:1967-73. 36 McAuley E, Doerksen SE, Morris KS, Motl RW, Hu L, Wo´jcicki TR, et al. Pathways from physical activity to quality of life in older women. Ann Behav Med. 2008;36:13-20.
37 Aoyagi Y, Park H, Park S, Shephard RJ. Habitual physical activity and health-related quality of life in older adults: interactions between the amount and intensity of activity (the Nakanojo Study). Qual Life Res. 2010;19:333-8.
38 Elavsky S, McAuley E, Motl RW, Konopack JF, Marquez DX, Hu L, et al. Physical activity enhances long-term quality of life in older adults: efficacy, esteem, and affective influences. Ann Behav Med. 2005;30:138-45.
39 Brown DW, Balluz LS, Heath GW, Moriarty DG, Ford ES, Giles WH, et al. Associations between recommended levels of physical activity and health-related quality of life. Findings from the 2001 behavioral risk factor surveillance system (BRFSS) survey. Prev Med. 2003;37:520-8.
40 Cassidy K, Kotynia-English R, Acres J, Flicker L, Lautenschlanger NT, Almeida OP. Association between lifestyle factors and mental health measures among community-dwelling older women. Aust N Z J Psychiatry. 2004;38:940-7.
41 Brown DW, Brown DR, Heath GW, Balluz L, Giles WH, Ford ES, et al. Associations between physical activity dose and health-related quality of life. Med Sci Sports Exerc. 2004;36:890-6.
42 Guallar-castillo´n P, Peralta PS, Ramo´n J, Lo´pez E, Me´todo SUY. Actividad fı´sica y calidad de vida de la poblacio´n adulta mayor en Espan˜a. Med Clin. 2004;123:606-10.
43 Lai KL, Tzeng RJ, Wang BL, Lee HS, Amidon RL, Kao S. Health-related quality of life and health utility for the institutional elderly in Taiwan. Qual Life Res. 2005;14:1169-80.
44 Acree LS, Longfors J, Fjeldstad AS, Fjeldstad C, Schank B, Nickel KJ, et al. Physical activity is related to quality of life in older adults. Health Qual Life Outcomes. 2006;4:37.
45 Brown DW, Brown DR, Heath GW, Moriarty DG, Balluz L, Giles WH. Relationships between engaging in recommended levels of physical activity and health-related quality of life among hypertensive adults. J Phys Act Health. 2006;3:137-47.
46 Mcauley E, Konopack JF, Motl RW, Morris KS, Doerksen SE, Rosengren KR. Physical activity and quality of life in older adults: influence of health status and self-efficacy. Ann Behav Med. 2006;31:99-103.
47 Lobo A, Santos P, Carvalho J, Mota J. Relationship between intensity of physical activity and health-related quality of life in Portuguese institutionalized elderly. Geriatr Gerontol Int. 2008;8:284-90.
48 Rossato DD, Rosa PV da, Rosa LHT da, Bianchi PD. Qualidade de vida e capacidade funcional de idosos adscritos em um PSF da cidade de Cruz Alta - RS. Fisioter Bras. 2008;9:338-42.
49 Johnson BL, Trentham-Dietz A, Koltyn KF, Colbert LH. Physical activity and function in older, long-term colorectal cancer survivors. Cancer Causes Control. 2009;20:775-84.
50 Alexandre Tda S, Cordeiro RC, Ramos LR. Factors associated to quality of life in active elderly. Rev Saude Publica. 2009;43:613-21. 51 Ekwall A, Lindberg A, Magnusson M. Dizzy –– why not take a walk? Low level physical activity improves quality of life. Gerontology. 2009;55:652-9.
52 Paskulin L, Vianna L, Molzahn AE. Factors associated with quality of life of Brazilian older adults. Int Nurs Rev. 2009;56:109-15. 53 Rennemark M, Lindwall M, Halling A, Berglund J. Relationships
between physical activity and perceived qualities of life in old age. Results of the SNAC study. Aging Ment Health. 2009;13:1-8. 54 Toscano JJO, Oliveira ACC. Qualidade de vida em idosos com
distintos nı´veis de atividade fı´sica. Rev Bras Med Esp. 2009;15:169-73.
55 White SM, Wo´jcicki TR, McAuley E. Physical activity and quality of life in community dwelling older adults. Health Qual of Life Outcomes. 2009;7:10.
56 Carvalho ED, Valadares ALR, Costa-Paiva LH, Pedro AO, Morais SS, Pinto-Neto AM. Atividade fı´sica e qualidade de vida em mulheres com 60 anos ou mais: fatores associados. Rev Bras Ginecol Obstet. 2010;32:433-40.
57 Salguero A, Martı´nez-Garcı´a R, Molinero O, Ma´rquez S. Physical activity, quality of life and symptons of depression in community-dwelling and institutionalized older adults. Arch Gerontol Geriatr. 2011;53:152-7.
58 Figueira HA, Figueira AA, Cader SA, Guimara˜es AC, DevOliveira RJ, Figueira JA, et al. Effects of a physical activity governmental health programme on the quality of life of elderly people. Scand J Public Health. 2012;40:418-22.
59 Grimmett C, Bridgewater J, Steptoe A, Wardle J. Lifestyle and quality of life in colorectal cancer survivors. Qual Life Res. 2011;20:1237-45. 60 Guedes DP, Hatmann AC, Martini FA, Borges MB, Bernadelli R Jr. Quality of life and physical activity in a sample of Brazilian older adults. J Aging Health. 2011;24:212-26.
61 Lima MG, Barros MBA, Ce´sar CLG, Goldbaum M, Carandina L, Alves MCGP. Health-related behavior and quality of life among the elderly: a population-based study. Rev Saude Publica. 2011;45:485-93. 62 Valadares ALR, Carvalho ED, Costa-Paiva LH, Morais SS,
Pinto-Neto AM. Association between different types of physical activities and quality of life in women aged 60 years or over. Rev Assoc Med Bras. 2011;57:450-5.
Physical activity and quality of life in the elderly 87
63 Porto DB, Guedes DP, Fernandes RA, Reichert FF. Perceived quality of life and physical activity in Brazilian older adults. Motricidade. 2012;8:33-41.
64 Baernholdt M, Hinton I, Yan G, Rose K, Mattos M. Factors associated with quality of life in older adults in the United States. Qual Life Res. 2012;21:527-34.
65 World Health Organization (WHO). Envelhecimento ativo: uma polı´tica de sau´de [cited 2013 Oct 16]. Brası´lia: Organizac¸a˜o Pan-Americana da Sau´de (Opas). 2005. http://bvsms.saude.gov.br/bvs/ publicacoes/envelhecimento_ativo.pdf
66 Garrido GE, Furuie SS, Buchpiguel CA, Bottino CM, Almeida OP, Cid CG, et al. Relation between medial temporal atrophy and functional brain activity during memory processing in Alzheimer’s disease: a combined MRI and SPECT study. J Neurol Neurosurg Psychiatry. 2002;73:508-16.
67 Reis RS, Petroski EL, Lopes A da S. Medidas da atividade fı´sica: revisa˜o de me´todos. Rev Bras Cineantropom Desempenho Hum. 2000;2:89-96.
68 Ware JE Jr. SF-36 health survey update. Spine (Phila Pa 1976). 2000;25:3130-9.
69 Tsai SY, Chi LY, Lee CH, Chou P. Health-related quality of life as a predictor of mortality among community-dwelling older persons. Eur J Epidemiol. 2007;22:19-26.
70 Ciconelli RM, Ferraz MB, Santos W, Meina˜o I, Quaresma MR. Traduc¸a˜o para a lı´ngua portuguesa e validac¸a˜o do questiona´rio gene´rico de avaliac¸a˜o de qualidade de vida SF-36. Rev Bras Reumatol. 1999;39:143-50.
71 Pucci GCMF, Rech CR, Fermino RC, Reis RS. Associac¸a˜o entre atividade fı´sica e qualidade de vida em adultos. Rev Saude Publica. 2012;46:166-79.
72 Pucci G, Reis RS, Rech CR, Hallal PC. Quality of life and physical activity among adults: population-based study in Brazilian adults. Qual Life Res. 2012;21:1537-43.
73 Diener E, Emmons RA, Larsen RJ, Griffin S. The satisfaction with life scale. J Pers Assess. 1985;49:71-5.
74 Wang L, Larson EB, Bowen JD, van Belle G. Performance-based physical function and future dementia in older people. Arch Intern Med. 2006;166:1115-20.
75 Brach JS, Simonsick EM, Kritchevsky S, Yaffe K, Newman AB, Health, Aging and Body Composition Study Research Group. The association between physical function and lifestyle activity and exercise in the health, aging and body composition study. J Am Geriatr Soc. 2004;52:502-9.