rev bras ortop.2014;49(4):405–408
w w w . r b o . o r g . b r
Case
Report
Lumbar
stenosis:
clinical
case
夽,夽夽
Pedro
Sá,
Pedro
Marques,
Bruno
Alpoim,
Elisa
Rodrigues,
António
Félix,
Luís
Silva,
Miguel
Leal
∗UnidadeLocaldeSaúdeAltoMinho,VianadoCastelo,Portugal
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received7March2013 Accepted8October2013 Availableonline3May2014
Keywords:
Spine
Spinalstenosis Laminectomy
a
b
s
t
r
a
c
t
Lumbarstenosisisanincreasinglycommonpathologicalconditionthatisbecomingmore frequent withincreasingmeanlife expectancy,withhighcostsforsociety.Ithasmany causes,amongwhichdegenerative,neoplasticandtraumaticcausesstandout.Mostofthe patientsrespondwelltoconservativetherapy.Surgicaltreatmentisreservedforpatients whopresentsymptomsafterimplementationofconservativemeasures.Here,acaseof severestenosisofthelumbarspineatseverallevels,inafemalepatientwithpathological andsurgicalantecedentsinthelumbarspine,ispresented.Thepatientunderwenttwo differentdecompressiontechniqueswithinthesameoperation.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Estenose
lombar:
caso
clínico
Palavras-chave:
Colunavertebral Estenoseespinal Laminectomia
r
e
s
u
m
o
Aestenoselombaréumapatologiacadavezmaisfrequente,queacompanhaoaumentoda esperanc¸amédiadevidaequecomportacustoselevadosparaanossasociedade.Apresenta inúmerascausas,entreasquaisdestacam-seadegenerativa,aneoplásicaeatraumática. Amaioriadospacientesrespondebemàterapêuticaconservadora.Otratamentocirúrgico estáreservadoparaaquelesdoentesqueapresentemsintomatologiaapósaimplementac¸ão demedidasconservadoras.Éapresentadoum casodeestenosegravedacolunalombar emváriosníveis,numadoentedosexofemininocomantecedentespatológicos/cirúrgicos dacolunalombar,naqualforamaplicadasduastécnicasdistintasdedescompressão,no mesmoatocirúrgico.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevierEditora Ltda.Todososdireitosreservados.
夽
Pleasecitethisarticleas:SáP,MarquesP,AlpoimB,RodriguesE,FélixA,SilvaL,etal.Estenoselombar:casoclínico.RevBrasOrtop. 2014;49:405–408.
夽夽
WorkperformedintheAltoMinhoLocalHealthcareUnit,VianadoCastelo,Portugal. ∗ Correspondingauthor.
E-mail:[email protected](M.Leal).
2255-4971/$–seefrontmatter©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
406
rev bras ortop.2014;49(4):405–408Introduction
Lumbarstenosisisdefinedasapathologicalnarrowingofthe vertebralcanaland/orintervertebralforamensthatleadsto compressionofthethecalsacand/orthenerveroots.Itmaybe confinedjusttoonesegment(twoadjacentvertebraeandthe intervertebraldisc,jointfacetsandcorrespondingligaments) or,insituationsofgreaterseverity,itmayencompasstwoor moresegments1andpresentseveraletiologies.
As mean life expectancy increases, people of greater agearepresentingactivelifestyles.Consequently,functional limitation and pain caused by symptomatic degenerative pathologicalconditionsofthespinehavebecomemore fre-quentandlumbarstenosishasbecomeanimportantdisease. Themainclinicalmanifestationsarelumbalgia,generally associatedwithirradiationtothelowerlimbs,andneurogenic claudication.
Radiologicalexaminations,especiallylumbarX-rays, com-puted tomography (CT) and magnetic resonance imaging (MRI),areusefulandessentialtoolsfordiagnosingand char-acterizinglumbarstenosis.
Therapyforthisconditioncontinuestobeaclinical chal-lenge,withvariousoptionsavailable.
Case
report
Thepatientwasa53-year-oldwhitefemalewhowasobserved inanorthopedicoutpatientconsultationwithacomplaintof lumbalgiaintheL5–S1regioninsituationsofconstantloading, withirradiationtobothlegs.Theconditionhadbeenevolving foraround twoyears,despiteconservativetherapy consist-ingofanalgesia,NSAIDs,musclerelaxantsandphysiotherapy, whichhadbeeninstitutedbythefamilydoctor.Thepatient reportedhavingneurogenicclaudication.Shedidnothaveany previoushistoryoftrauma.
Shereportedhavingpersonal antecedentsofadisc her-nia,whichwaspresentintwosegmentsofthelumbarspine (L3–L4 and L4–L5),and havingundergoing classical lumbar discectomy.
Onphysical examination,shepresented painon palpa-tionofthelumbarspineapophysesandparavertebralmasses. ShewasbilaterallypositiveforLasègue’ssign.Aneurological examinationrevealedafootinclinedtotheright.
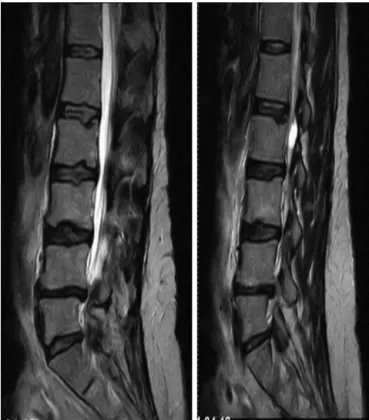
LumbarMRIshowedabulgingintervertebraldisc, hyper-trophyofthejointfacetsandyellowligamentsatthelevels L2–L3,L3–L4,L4–L5andL5–S1,whichcausednarrowingofthe spinalcanal,withimpairmentoftherootsofL4,L5 andS1
Fig.1–MRIofthelumbarspine(sagittalslice),inwhich lumbarstenosiscanbeseenatL2–S1.
(Figs.1and2AandB).Electromyographywasalsoperformed onthelowerlimbs,andthisrevealedsevereradiculopathyat L5andS1.
Fromthis,adiagnosisoflumberstenosisatL2–L3,L3–L4, L4–L5andL5–S1wasestablished,associatedwith neurologi-caldeficits,andsurgicaltreatmentwasproposed.Thepatient underwentlumbarrecalibrationofL2–L3andL3–L4bymeans oftheSenegastechniqueatL4–L5andL5–S1with laminec-tomyandfixationusingtranspedicularscrewsand postero-lateralarthrodesis,withanautologousbonegraft(Fig.3).
The patient presented regression of the neurological deficits aftertheoperation.Currently,sheisbeingfollowed upasanoutpatientandisasymptomatic.
Discussion
Theincidenceoflumbarstenosisinthegeneralpopulationis between1.7%and8%,anditincreasesfromthefifthdecade oflifeonwards.2
rev bras ortop.2014;49(4):405–408
407
Fig.3–X-rayofthelumbarspineaftersurgerywith arthrodesisatL4–S1.
Itcanbeclassifiedaccordingtoeitherits etiology orits anatomy.Theetiologicalclassificationisdividedinto congen-italstenosisandacquired/degenerativestenosis.Congenital stenosisischaracterizedbynarrowingofthevertebralcanal thatiseitheridiopathicorsecondarytobonedysplasiasuchas achondroplasia.Acquired/degenerativestenosismayoccuras aresultofmetabolicdisease(suchasPaget’sdisease),tumors, infections, osteoarthritic alterations or instability with or without spondylolisthesis. The anatomical classification is usedtoidentifyspecificareas ofstenosisand isusedas a “guide”tosurgicaldecompression.Fourtypesofstenosiscan bedefined:(1)central;(2)lateralrecess;(3)foraminal;and(4) extraforaminal.
Adultdegenerative lumbar stenosis, which was present inthisclinicalcase,isalmostalwaysassociatedwith osteo-phytic/degenerativeincreases inthejoint facets,andthese alterationsarecausedbysegmentalinstability.Itisbelieved thatthis entire degenerative process startswith degenera-tion of the intervertebral disc, followed by collapseof the disc space.3 This givesrise to abnormal movement
kinet-ics,withconsequentosteoarthrosis/hypertrophyofthejoint facets,whichresultsindiminutionofthecentraland inter-vertebralportionofthe vertebralcanal.Becauseofthe loss ofdisc heightand hypertrophyofthejointfacets, shorten-ingandthickeningoftheyellowligamentisseen,whichalso contributestowarddiminishingthecentralspaceofthe ver-tebralcanal.Insomepatients,degenerativecystscanalsobe seeninthesynovialregionofthejointfacets,whichcausea “mass”effectandcontributetowardagreaterdegreeoflumbar stenosis.
The classical clinical presentation of lumbar stenosis consists of bilateral neurogenic claudication, along with chroniclumbalgiawithirradiationtothelowerlimbs,which
worsens with standing up for prolonged periods, physi-cal activity and lumber extension. Some patients describe improvementofthesymptomswhen theysit downand/or flex thelumbarspine.Neurogenicclaudication needstobe distinguishedfromvascularclaudication.Thelatterdoesnot presentworseningwhilethepatientisstandingupforalong time, and it is not alleviated through flexion of the lum-barspine,unlikewhatisseenwithneurogenicclaudication. Objectiveexaminationonpatientswithvascularclaudication showsthattheygenerallypresentabnormalitiesofthearterial pulse,alongwithtrophicalterations(thinnerandshinierskin). Efforttestsmaybeusefulindistinguishingbetweenthesetwo clinicalentities.Asmallnumberofpatientspresentpriapism and/orsphincterdysfunctioninassociationwithneurogenic claudication,whichrevealsamoreseveredegreeoflumbar stenosis.Alterationstothesensitivityofthelowerlimbsand tendonreflexesmayalsobepresent.
There are several pathological conditions that present similar symptoms, and it is necessary to make a differ-ential diagnosis. It is important to rule out tumors (both primarytumorsandmetastases),Paget’sdisease,infections, trochantericbursitisandcoxarthrosis/gonarthrosis.4
Thediagnosisoflumbarstenosiscanbeconfirmedthrough using computed tomography (CT) and magnetic resonance imaging(MRI).CTistheexaminationthatpresentsbetter cost-efficacy,anditprovidesanexcellentlevelofdetailingofthe bonestructures,especiallyintheregionofthelateralrecess. MRIprovidesabetterviewofthesofttissues,whichisvery usefulinevaluatingthepathologyoftheintervertebraldisc, anditsefficacy isbetterthanthatofCTandmyelography.5
Electromyography,whichteststhevelocityofnerve conduc-tionandassessestheevokedsomatosensorypotentials,does notformpartofthe routineevaluationoflumbarstenosis. Itis usefulfor distinguishingradiculopathy because ofthe lumbarcompressionanddiabeticneuropathythataffectthe peripheralsensory-motornerves.
There are two main variants of treatments for lumbar stenosis:conservativeandsurgical.
Thepillarsofconservativeconsistofuseofdrugs, phys-iotherapy,corsetryandepiduralinjectionsofcorticosteroids. Use of non-steroidal anti-inflammatory drugs provides an improvement in the symptoms, though diminishing the inflammatoryresponseassociatedwithcompressionofneural elements.Physiotherapyisbasedonstretchingand strength-ening exercises for the lumbar spine, along with aerobic exercises(staticbicycle).Corsetrymaybeusefulfor alleviat-ingthesymptoms,throughdiminishinglumbarlordosis,and itpresentsbetterresultsinpatientswithspondylolisthesis.6
Injectionofcorticosteroidsfortreatinglumbarpathological conditions, notably lumbar stenosis, remains a controver-sialprocedure.7Todate,severalstudieshavebeenunableto
demonstrateanyeffectiveresponsefrominjectionsfor resolv-ingradiculopathy.7
408
rev bras ortop.2014;49(4):405–408approachenablesdirectviewingofthenerverootsandtheir decompressionalong theentirepath.Lessinvasive decom-pressive surgical techniques that preserve posterior bone andligamentstructureshaverecentlybeendevelopedinan attempttodiminishthepostoperativeinstability.These tech-niquesinclude laminectomywith angular resection ofthe anteriorandlateralportionsofthelamina,selective unilat-eral/bilaterallaminectomy,partiallaminectomyandlumbar laminoplasty.8–10Incertaincases,itispossibletoapplyseveral
surgicaltechniquesatdifferentvertebrallevelsinthesame patientand toreservestandard laminectomyforthelevels thatpresentstenosisofgreaterseverity.5Theclinicalresults
from surgicaldecompressionoflumber stenosishavebeen favorable,11withremissionofthesymptoms,althoughrecent
studieshaveindicatedthattheinitialclinicalimprovement tendstodeterioratewiththepassageoftime.12
Spondylolis-thesisfollowingdecompressionwithoutlumbararthrodesisis oneofthecommonestcomplications.Therefore,arthrodesis ofthelumbarspinewithautologousgraftsandfixationwith transpedicular screws shouldbe performed onall patients who present instabilitydue toresectionofthe joint facets during decompression.13 It is essential to perform lumbar
arthrodesisonpatientswithlumbarstenosisand spondylolis-thesisordegenerativescoliosis.13
Through presenting this case, the aim is to highlight the fact that this was a patient with pathological/surgical antecedentsinthelumbarspine,whopresentedsevere steno-siswithinvolvementofthelumbarspineatdifferentlevels, and towhom twodistinct decompression techniqueswere appliedinthesamesurgicalprocedure,withgoodresults.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.SpivakJM.Currentconceptsreview.Degenerativelumbar spinalstenosis.JBoneJointSurgAm.1998;80(7):1053–66. 2.LiebermanJR,PensakMJ.Preventionofvenous
thromboembolicdiseaseaftertotalhipandknee arthroplasty.JBoneJointSurgAm.2013;95(19):1801–11. 3.Kirkaldy-WillisWH,WedgeJH,Yong-HingK,ReillyJ.
Pathologyandpathogenesisoflumbarspondylosisand stenosis.Spine(PhilaPA1976).1978;3(4):319–28.
4.JönssonB,StrömqvistB.Symptomsandsignsindegeneration ofthelumbarspine.Aprospective,consecutivestudyof300 operatedpatients.JBoneJointSurgBr.1993;75(3):381–5. 5.PostacchiniF,AmatrudaA,MoraceGB,PerugiaD.Magnetic
resonanceimaginginthediagnosisoflumbarspinalcanal stenosis.ItalJOrthopTraumatol.1991;17(3):327–37. 6.WillnerS.Effectofarigidbraceonbackpain.ActaOrthop
Scand.1985;56(1):40–2.
7.RydevikBL,CohenDB,KostuikJP.Spineepiduralsteroidsfor patientswithlumbarspinalstenosis.Spine(PhilaPA1976). 1997;22(19):2313–7.
8.KanamoriM,MatsuiH,HiranoN,KawaguchiY,KitamotoR, TsujiH.Trumpetlaminectomyforlumbardegenerative spinalstenosis.JSpinalDisord.1993;6(3):232–7.
9.AryanpurJ,DuckerT.Multilevellumbarlaminotomies:an alternativetolaminectomyinthetreatmentoflumbar stenosis.Neurosurgery.1990;26(3):429–32.
10.TsujiH,ItohT,SekidoH,YamadaH,KatohY,MakiyamaN, etal.Expansivelaminoplastyforlumbarspinalstenosis.Int Orthop.1990;14(3):309–14.
11.TurnerJA,ErsekM,HerronL,DeyoR.Surgeryforlumbar spinalstenosis.Attemptedmeta-analysisoftheliterature. Spine(PhilaPa1976).1992;17(1):1–8.
12.PostacchiniF,CinottiG,GuminaS,PerugiaD.Long-term resultsofsurgeryinlumbarstenosis.8-yearreviewof64 patients.ActaOrthopScandSuppl.1993;251:78–80. 13.BoothJrRE,SpivakJ.Thesurgeryofspinalstenosis.Instr