ww w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Rheumatoid
arthritis
and
sleep
quality
Ana
Claudia
Janiszewski
Goes,
Larissa
Aparecida
Busatto
Reis,
Marilia
Barreto
G.
Silva,
Barbara
Stadler
Kahlow,
Thelma
L.
Skare
∗HospitalUniversitárioEvangélicodeCuritiba,UnidadedeReumatologia,Curitiba,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received10November2015 Accepted15June2016
Availableonline12August2016
Keywords:
Rheumatoidarthritis Sleep
Sleepapnea Depression Pain
a
b
s
t
r
a
c
t
Background:Sleepdisturbancesarecommoninrheumatoidarthritis(RA)patientsand con-tributetolossoflifequality.
Objective:Tostudyassociationsofsleepqualitywithpain,depressionanddiseaseactivity inRA.
Methods:Thisisatransversalobservationalstudyof112RApatientssubmittedto mea-surementofDAS-28,Epworthscalefordailysleepiness,indexofsleepqualitybyPittsburg index,riskofsleepapneabytheBerlinquestionnaire anddegreeofdepressionbythe CES-D(CenterforEpidemiologicStudiesDepressionscale)questionnaire.Wealsocollected epidemiological,clinical,serologicalandtreatmentdata.
Results:Only18.5%ofRApatientshadsleepofgoodquality.Inunivariateanalysisabad sleepmeasuredbyPittsburgindexwasassociatedwithdailydosesofprednisone(p=0.03), DAS-28(p=0.01),CES-D(p=0.0005)andshowedatendencytobeassociatedwithBerlinsleep apneaquestionnaire(p=0.06).Inmultivariateanalysisonlydepression(p=0.008)andBerlin sleepapneaquestionnaire(p=0.004)keptthisassociation.
Conclusions:MostofRApatientsdonothaveagoodsleepquality.Depressionandriskof sleepapneaareindependentlyassociatedwithsleepimpairment.
©2016ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Artrite
reumatoide
e
qualidade
do
sono
Palavras-chave:
Artritereumatoide Sono
Apneiadosono Depressão Dor
r
e
s
u
m
o
Antecedentes:Osdistúrbiosdosonosãocomunsempacientescomartritereumatoide(AR) econtribuemparaaperdadaqualidadedevida.
Objetivo:Estudarasassociac¸õesentreaqualidadedosonoeador,depressãoeatividadeda doenc¸anaAR.
Métodos:Estudo observacional transversal com 112 pacientes com AR submetidos à avaliac¸ãodoDAS-28,escaladeEpworthparasonolênciadiurna,qualidadedosonopelo índicedePittsburg,riscodeapneiadosonopeloquestionáriodeBerlimegraudedepressão peloquestionárioCES-D(CenterforEpidemiologicStudiesDepression).Tambémforamcoletados dadosepidemiológicos,clínicos,sorológicosedetratamento.
∗ Correspondingauthor.
E-mail:[email protected](T.L.Skare). http://dx.doi.org/10.1016/j.rbre.2016.07.011
Resultados: Apenas18,5%dospacientescomARtinhamumaboaqualidadedosono.Na análiseunivariada,umsonoruimmedidopeloíndicedePittsburgesteveassociadoàdose diáriadeprednisona(p=0,03),DAS-28(p=0,01),CES-D(p=0,0005)emostrouumatendência aestarassociadoàapneiadosonopeloquestionáriodeBerlim(p=0,06).Naanálise mul-tivariada,somenteadepressão(p=0,008)eaapneiadosonopeloquestionáriodeBerlim (p=0,004)mantiveramessaassociac¸ão.
Conclusões: AmaiorpartedospacientescomARnãotemumaboaqualidadedesono.A depressãoeoriscodeapneiadosonoestãoindependentementeassociadosao comprome-timentodosono.
©2016ElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCC BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Patients’well-beingisamajorconcerninrheumatoidarthritis (RA).PatientswithRAsufferfromavarietyofsymptomssuch asjointpain andswelling,stiffness,fatigueand functional disability,thatimpairtheirqualityoflife.Sleepdisturbances are alsocommon in this population and contribute tothe problem.1Severalstudieshavefoundsleepfragmentation,low
sleepefficiency,frequentawakeningsandpoorsleepquality inthisgroupofpatients.1–3
Nicassio et al.4 consider pain and sleep disturbance to
becloselylinked.Howeveritisdifficulttoknowwhichone istheprimaryproblem.Althoughtheinflammatoryprocess broughtbyRAactivityisresponsibleforpaininitiation, inves-tigators have found that, in some patients, pain intensity maybeout ofproportiontothe severityofinflammation.5
Itisbelievedthatthisisduetocentralnervoussystempain amplification, mainly due to diminished conditioned pain modulation.5 Psychological distress, most notably
depres-sion and/or anxiety is another variable implicated in this relationship.1,4
Tolookfurtherintothisissue,wehavestudiedasample ofRABrazilianpatientsinordertoclarifytheassociationsof sleepqualitywithpain,depressionanddiseaseactivity.
Methods
AfterapprovalofthelocalCommitteeofEthicsinResearch andsignedconsentfrompatientswestudied112RApatients fromasingleUniversityCenter.Thiswasaconvenience sam-ple of patients that came for regular consultations in the periodofoneyearandacceptedtoparticipateinthestudy. Allsubjectshadtofulfillatleastfour1987ACRcriteriaforRA classification.6Weexcludedpatientswithageunder18years,
with disease beginning before 16 years, pregnant women, thosewithuncontrolledthyroiddiseaseorwithotherchronic inflammatoryconditionandthoseusingsleepinductor med-ications.Wecollected demographic,clinicaland serological data,valuesofhemoglobin,ESR(erythrocytesedimentation rate),CRP(Creactiveprotein)andDAS-28.Diurnalsomnolence wasevaluatedbytheEpworthscale,7theindexofsleep
qual-itybythePittsburgindex,8andtheriskofsleepapneabythe
Berlinquestionnaire.9DepressionwasmeasuredbytheCES-D
QuestionnaireorCenterforEpidemiologicStudiesDepression
scale.10Alltheappliedinstrumentsweretranslatedand
vali-datedforthePortugueselanguage.Fatigueandglobalhealth weremeasuredbyavisualanalogicscalefrom0(none)to100 (maximal).
Patientsweredividedinthosewithgoodandpoorsleep qualityaccordingtothePittsburgindex(equalorlowerthan 5=good sleep; >5=sleep disorder) and these two samples were compared. For this comparison we used Fisher and chi-squaredtestsfornominaldataandMannWhitney and unpairedttestfornumericaldata.Associationswithp≤0.10 were studiedthroughlinearregression totestthevariables independence.Significanceadoptedwasof5%.
Results
Overviewofstudiedsampleandprevalenceofsleep disturbances
In the 112 RA patients, 83.1% were female, with age ran-gingfrom21to77years(mean55.4±10.9years)anddisease duration from 9monthsto53 years (median11 years;IQR orinterquartilerate=5–18).AutodeclaredAfrodescendants were19.6%;1.7%Asiaticdescendantsand78.5%Caucasians. Tobacco exposure occurred in 39.2% while 60.3% never smoked.Thebodymassindexvariedfrom17.3to46.4kg/m2 (medianof27.5;IQR=24.3–31.5kg/m2).Rheumatoidfactor(RF) was present in59.6%; anti-CCP in47.6%;ANA (antinuclear antibody)in34.9%.
Treatmentprofileatthetimeofstudyshowedthat pred-nisonewasusedin71.4%(dosesfrom5.0to60.0mg;median 5.0; IQR=5.0–10.0); methotrexate in 73.2%, antimalarial in 21.4%,leflunomidein43.7%,antiTNF-alphain5.3%and abat-aceptin2.6%.
Table1showstheresultsoflaboratorytestsandapplied questionnaires.
ComparisonstudyofRApatientswithgoodandpoor
sleepquality
Studyingthecomparisonofpatientswithandwithoutgood sleepqualityaccordingtothePittsburgindexweobtainedthe resultsinTable2.
Table1–Laboratoryandquestionnairesresultsin112rheumatoidarthritispatients.
Studiedvariable Values
Erythrocytesedimentationrate(mm/h) 1–103(median35.0;IQR=19.7–58.0)
Creactiveprotein(mg/dL) 0.15–80.0(median10.9;IQR=5.0–20.7)
Hemoglobin 10.9–16.9(mean13.3±1.2)
VASglobal 0–100(median30.0;IQR=30.0–60.0)
VASpain 0–100(median60.0;IQR30.0–80.0)
VASfatigue 0–100(median50.0;IQR0–80.0)
Bodymassindex(kg/m2) 17.3–46.4(median27.5;IQR=24.3–31.5)
•Underweight(<18.5)–4/112=3.5%
•Normal(18.6–24.9)–29/112=25.8%
•Overweight(25–29.9)–43/112=38.3%
•Obesity(≥30)–36/112=32.1%
DAS-28(ESR) 0.28–7.38(mean3.75±1.28)
Epworthsleepinessscale 0–24.0(median6.0;IQR3.0–12.0)
•Normal=79/112(70.5%)
•Pathologicalsomnolence=12/112(10.7%)
•Significantsomnolence=21/112(18.7%) Berlinorsleepapneascreeningquestionnaire 0–3.0(median1.0;IQR=3.0–2.0)
•Lowriskofsleepapnea=58/112(51.7%)
•Highriskofsleepapnea=54/112(48.2%)
Pittsburgsleepqualityindex 1–18(median9.0;IQR5.0–18.0)
•Sleepofgoodquality=21/112(18.5%)
•Sleepdisturbance=47/112(41.9%)
•Badsleep=44/112(39.2%) CenterforEpidemiologicStudiesDepressionScale(CES-D) 0–60(median13.0;IQR=6.0–22.0)
•Normal–63/112=56.1%
•Depressive–49/112=43.7%
VAS,visualanalogicscale;DAS-28,DiseaseActivityScoreCalculator.
ThecomparisonofVASfatigue,Epworthsleepinessscale
and Berlin sleep apnea screening questionnaire showed
respectivelyp=0.04,p=0.84andp=0.06(MannWhitney).The
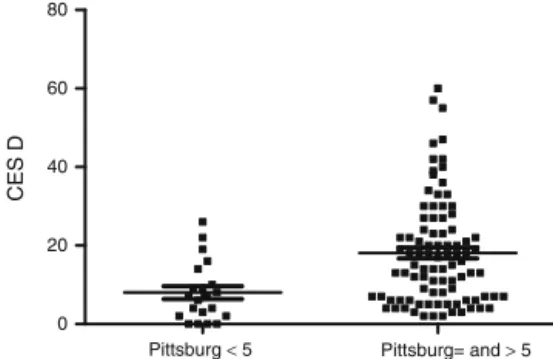
resultofassociationofPittsburgindexwithdepression(CES-D)
isinFig.2.
Inamultipleregressionstudythatincludeddailydosesof prednisone,VASfatigue,numberoftenderjoints,resultsof Berlinsleepapneascreeningquestionnaire,DepressionCES-D questionnaireandnumberofpainfuljoints(fromDAS28),we foundthatthePittsburgindexassociatedindependentlywith CES-Ddepressionquestionnaire(p=0.008)andBerlinapnea screeningquestionnaire(p=0.004).
Pittsburg Pittsburg < 5 ≥ 5 0
2 4 6 8
DAS 28
Fig.1–ComparisonofDAS-28(ESR)accordingtosleep qualitymeasuredbyPittsburgindex(p=0.01;Mann Whitney).ComparisonofESRwithp=0.12;globalVASwith p=0.43;numberofswollenjointswithp=0.31;numberof painfuljointswithp=0.005.
Discussion
Oneofthemoststrikingfindingsofthepresentstudyisthat lessthan20%ofRApatientshaveasleepofgoodquality.This mustbetakenintoaccountindailypracticeifoneintendsto improvepatients’qualityoflife.Thishighprevalenceofsleep disorderhasalreadybeennotedbyothers.1–4
Inthisstudy,univariateanalysisdisclosedassociationof poor sleep with DAS 28, dailydose ofprednisone, fatigue, depression and risk of sleep apnea. Sariyildiz et al.1 and
Son et al.11 have also found association of disease
activ-ity withpoorsleepquality.Somestudieshavedocumented qualitative alterations and rupture in sleep continuity in relationship with certain immunological factors.12 In RA,
Pittsburg < 5 Pittsburg= and > 5 0
20 40 60 80
CES D
Table2–Comparisonofdemographic,laboratorial,serologicalandtreatmentdatainrheumatoidarthritispatients accordingtosleepqualitymeasuredbyPittsburgindex(goodsleep≤5;sleepdisorder>5).
Pittsburgindex≤5 n=21
Pittsburgindex>5 n=91
p
Gender(male/female) 5/16 13/78 0.32a
Tabagism(smokers/notsmokers) 5.2% 14.2% 1.00a
Ethnicbackground
(Afrodescendants/Caucasians)
2/18 20/71 0.35a
Meanage(years) 58.4±2.2 54.7±10.6 0.15b
Meanageatdiagnosis(years) 45.0±15.6 42.5±11.56 0.42b
Medianbodymassindex(kg/m2) 26.7
(IQR=22.3–28.6)
27.6
(IQR=24.7–31.59)
0.25c
Positiverheumatoidfactor 47.6% 61.5% 0.24c
Positiveanti-CCP 30% 50.9% 0.30a
Positiveantinuclearantibody 40% 33.7% 0.59d
MedianCreactiveprotein(mg/L) 11.0
(IQR=6.0–20.8)
10.7
(IQR=5.0–20.7)
0.85c
Medianhemoglobin(g/dL) 13.5
(IQR=12.0–14.0)
13.4
(IQR=12.4–14.0)
0.80c
Medianprednisonedose(mg/day) 5.0
(IQR=0.0–5.0)
5.0
(IQR=5.0–10.0)
0.03c
Metotrexateusers 71.4% 73.9% 0.83d
Leflunomideusers 42.8% 43.9% 0.92d
Antimalarialusers 19.04% 21.9% 1.00a
Biologicmedicationusers 9.5% 9.8% 1.00a
Mediansedimentationrate 26.0
(IQR=13.5–47.5)
39.0
(IQR=21.0–60.0)
0.12c
IQR,interquartilerate.
a Fishertest. b Unpairedttest. c MannWhitneytest. d Chisquaredtest.
circulatingTNF-␣ isincreasedandtherehasbeena
sugges-tionthatthelevelofthiscytokinemaybeconnectedtosleep disorders.12BrainlevelsofIL-1andTNF␣ arelinkedwithsleep
deprivation.12 Onestudy13 conductedinten RApatients to
assesswhether antiTNFdrugshadany effectonthesleep patternsuggestedthatitsqualityimprovedwiththistypeof medication.
However,in the present study,when the elements that areincludedintheDAS28 wereexaminedapart,the num-beroftenderjoint was thecomponent responsible forthe association.Thus,painand notinflammationcouldbethe realassociation.Sleepdisturbanceinpatientswithjointpain hasbeen notednotonlyinRAbut inother chronicpainful conditions.14
Thedaily dose ofprednisone was alsorelated to lower performance in the Pittsburg score in univariate analysis. Endogenousglucocorticoidsarecriticalforthepathogenesis ofsustainedstress-relatedsleepdisorders.15Highserum
lev-elsofglucocorticoidsinducepoorsleep qualityandshorter sleepdurationthroughreceptorsthatarehighlyexpressedin thebrain.16Nevertheless,higherdosesofprednisoneareused
bypatientswithmoreinflammationand itispossiblethat, again,painresultingfromtheinflammatoryprocesscouldbe thetrueresponsiblefortherelationship.
The Berlin apnea screening questionnaire displayed an independentassociation withpoor sleep inRA. Drossaers-Bakeretal.17 showedthatsleepapneaintheirRApatients
was due to a mixed pattern: central and obstructive,
suggestingthatthisproblemismultifactorial.Contributorsto theobstructivecomponentcouldbeincreasedneck circum-ferencebyglucocorticoiduse,narrowingofupperairwayby changes intemporomandibularjoint, repositionof cervical axisincasesofcervicalsubluxationorevenbydiminished muscle tone in the airway.17 A high BMI is also common
inRApatientsandwasfoundin60% ofthissample. Verti-calluxationoftheodontoidprocessmaycausecompression of the brain stem and could result in central impairment of breathing.18 Patients with hypoventilation complain of
headacheuponawakening,nocturnalunrest,day-time sleepi-nessandimpairedconcentration.19Thesesymptomsareoften
mildandmaybeeasilyoverlooked.Curiously,antiTNFdrugs arealsodescribedasimprovingthesleepapneasyndrome.19
Inoursamplethenumberofpatientsusingthistypeofdrug wastoosmalltoallowanyconclusions.
Finally,depressionwasindependentlylinkedtopoorsleep quality.DepressionisahighlyprevalentprobleminRA1and
contributestodisability,badadherencetotreatment,andpoor socialfunctioning.Insomniaindepressedpatientswasfirst consideredtobeasymptomofdepression.20 Morerecently
there is evidence to sustain that there is a bidirectional connectionbetweenthesetwovariables.Accordingtosome studies,sleepdisorder isalsoamajorriskfactorforfuture onsetandforrecurrenceofdepressiveepisodes.21,22
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. SariyildizMA,BatmazI,BozkurtM,BezY,CetincakmakMG, YazmalarL,etal.Sleepqualityinrheumatoidarthritis: relationshipbetweenthediseaseseverity,depression, functionalstatusandthequalityoflife.JClinMedRes. 2014;6:44–52.
2. BourguignonC,LabyakSE,TaibiD.Investigatingsleep disturbancesinadultswithrheumatoidarthritis.HolistNurs Pract.2003;17:241–9.
3. LouieGH,TektonidouMG,Caban-MartinezAJ,WardMM. Sleepdisturbancesinadultswitharthritis:prevalence, mediators,andsubgroupsatgreatestrisk.Datafromthe2007 NationalHealthInterviewSurvey.ArthritisCareRes.
2011;63:247–60.
4. NicassioPM,OrmsethSR,KayM,CustodioM,IrwinMR, OlmsteadR,etal.Thecontributionofpainanddepressionto self-reportedsleepdisturbanceinpatientswithrheumatoid arthritis.Pain.2012;153:107–12.
5. LeeYC,LuB,EdwardsRR,WasanAD,NassikasNJ,ClauwDJ, etal.Theroleofsleepproblemsincentralpainprocessingin rheumatoidarthritis.ArthritisRheum.2013;65:59–68. 6. ArnettFC,EdworthySM,BlochDA,McShaneDJ,FriesJF,
CooperNS,etal.TheAmericanRheumatismAssociation 1987revisedcriteriafortheclassificationofrheumatoid arthritis.ArthritisRheum.1988;31:315–24.
7. BertolaziAN,FagondesSC,HoffLS,PedroVD,MennaBarreto SS,JohnsMW.Portuguese-languageversionoftheEpworth sleepinessscale:validationforuseinBrazil.JBrasPneumol. 2009;35:877–83.
8. BertolaziAN,FagondesSC,HoffLS,DartoraEG,MiozzoIC,de BarbaME,etal.ValidationoftheBrazilianPortugueseversion ofthePittsburghSleepQualityIndex.SleepMed.2011;12:70–5. 9. NetzerNC,StoohsRA,NetzerCM,ClarkK,StrohlKP.Using
theBerlinQuestionnairetoidentifypatientsatriskforthe sleepapneasyndrome.AnnInternMed.1999;131:485–91.
10.daSilveiraDX,JorgeMR.Reliabilityandfactorstructureofthe BrazilianversionoftheCenterforEpidemiologic
Studies-Depression.PsycholRep.2002;913Pt1:865–74. 11.SonCN,ChoiG,LeeSY,LeeJM,LeeTH,JeongHJ,etal.Sleep
qualityinrheumatoidarthritis,anditsassociationwith diseaseactivityinaKoreanpopulation.KoreanJInternMed. 2015;30:384–90.
12.KruegerJM,ObalFJ,FaigJ,KubotaT,TaishiP.Theroleof cytokinesinphysiologicalsleepregulation.AnnNYAcadSci. 2001;933:211–21.
13.Taylor-GjevreRM,GjevreJA,NairBV,SkomroRP,LimHJ. Improvedsleepefficiencyafteranti-tumornecrosisfactor␣ therapyinrheumatoidarthritispatients.TherAdv MusculoskeletDis.2011;3(5):227–33.
14.BrownGK.Acausalanalysisofchronicpainanddepression.J AbnormPsychol.1990;99:127–37.
15.WangZJ,ZhangXQ,CuiXY,CuiSY,YuB,ShengZF,etal. Glucocorticoidreceptorsinthelocuscoeruleusmediatesleep disorderscausedbyrepeatedcorticosteronetreatment.Sci Rep.2015;5:9442.
16.BradburyM,DementWC,EdgarDM.Effectsofadrenalectomy andsubsequentcorticosteronereplacementonratsleepstate andEEGpowerspectra.AmJPhysiol.1998;275:R555–65. 17.Drossaers-BakkerKW,HamburgerHL,BongartzEB,Dijkmans
BA,VanSoesbergenRM.Sleepapnoeacausedbyrheumatoid arthritis.BrJRheumatol.1998;37:889–94.
18.HamiltonJ,DaggK,SturrockR,AndersonJ,BanhamS.Sleep apnoeacausedbyrheumatoidarthritis.Rheumatology (Oxford).1999;38:679–80.
19.WalshJA,DuffinKC,CrimJ,CleggDO.Lowerfrequencyof obstructivesleepapneainspondyloarthritispatientstaking TNF-inhibitors.JClinSleepMed.2012;8:643–8.
20.MaglioneJE,Ancoli-IsraelS,PetersKW,PaudelML,YaffeK, EnsrudKE.Depressivesymptomsandsubjectiveand objectivesleepincommunity-dwellingolderwomen.JAm GeriatrSoc.2012;60:635–43.
21.FranzenPL,BuysseDJ.Sleepdisturbancesanddepression: riskrelationshipsforsubsequentdepressionandtherapeutic implications.DialoguesClinNeurosci.2008;10:473–81. 22.PerlisML,SmithLJ,LynessJM,MattesonSR,PigeonWR,