www.revportcardiol.org
Revista
Portuguesa
de
Cardiologia
Portuguese
Journal
of
Cardiology
ORIGINAL
ARTICLE
Triple-site
pacing
for
cardiac
resynchronization
in
permanent
atrial
fibrillation
---
Acute
phase
results
from
a
prospective
observational
study
Pedro
Marques
∗,
Miguel
Nobre
Menezes,
Gustavo
Lima
da
Silva,
Ana
Bernardes,
Andreia
Magalhães,
Nuno
Cortez-Dias,
Luís
Carpinteiro,
João
de
Sousa,
Fausto
J.
Pinto
CardiologyDepartment,UniversityHospitalSantaMaria,CentroHospitalardeLisboaNorte,CCUL,UniversityofLisbon,Portugal
Received28October2015;accepted20December2015
Availableonline30May2016
KEYWORDS Cardiac resynchronization therapy; Multi-sitepacing; Triple-sitepacing; Heartfailure; Atrialfibrillation; Cardiacoutput; QRSduration; Ejectionfraction Abstract
IntroductionandAim:Multi-sitepacingisemergingasanewmethodforimprovingresponseto cardiacresynchronizationtherapy(CRT),buthasbeenlittlestudied,especiallyinpatientswith atrialfibrillation.Weaimedtoassesstheeffectsoftriple-site(Tri-V)vs.biventricular(Bi-V) pacingonhemodynamicsandQRSduration.
Methods:Thiswasaprospectiveobservationalstudyofpatientswithpermanentatrial fibrilla-tionandejectionfraction<40%undergoingCRTimplantation(n=40).Onerightventricular(RV) leadwasimplantedintheapexandanotherintherightventricularoutflowtract(RVOT)septal wall.Aleftventricular(LV)leadwasimplantedinaconventionalvenousepicardialposition. Cardiacoutput(usingtheFloTracTM VigileoTM system),meanQRSandejectionfractionwere calculated.
Results:Meancardiacoutputwas4.81±0.97l/minwithTri-V,4.68±0.94l/minwithRVOTseptal andLVpacing,and4.68±0.94l/minwithRVapicalandLVpacing(p<0.001for Tri-Vvs.both BiV).Meanpre-implantationQRSwas170±25ms,123±18mswithTri-V,141±25mswithRVOT septalpacingandLVpacingand145±19withRVapicalandLVpacing(p<0.001forTri-Vvs.both BiVandpre-implantation).MeanejectionfractionwassignificantlyhigherwithTri-V(30±11%) vs.Bi-Vpacing(28±12%withRVOTseptalandLVpacingand28±11withRVapicalandLVpacing) andpre-implantation(25±8%).
Conclusion: Tri-VpacingproducedhighercardiacoutputandshorterQRSdurationthanBi-V pacing.ThismayhaveasignificantimpactonthefutureofCRT.
© 2016SociedadePortuguesade Cardiologia.Publishedby ElsevierEspa˜na,S.L.U.Allrights reserved.
∗Correspondingauthor.
E-mailaddress:[email protected](P.Marques).
http://dx.doi.org/10.1016/j.repc.2015.12.006
PALAVRAS-CHAVE Terapêuticade ressincronizac¸ão cardíaca; Pacingmulti-site; Pacingtriple-site; Insuficiência cardíaca;
Fibrilhac¸ãoauricular; Débitocardiaco; Durac¸ãoQRS; Frac¸ãodeejec¸ão
Pacingtriple-sitepararessincronizac¸ãocardíacanafibrilhac¸ãoauricularpermanente
--- resultadosdafaseagudadeumestudoprospetivoobservacional
Resumo
Introduc¸ãoeobjetivo: O pacing multi-site está a emergir como um novo método de ressincronizac¸ãocardíaca. Todavia,foi poucoestudado, sobretudo em fibrilhac¸ãoauricular. Esteestudovisaaferiroefeitohemodinâmicoenadurac¸ãodoQRSdepacingTri-VversusBi-V.
Métodos: Estudoprospetivoobservacionaldedoentescomfibrilhac¸ãoauricularpermanentee frac¸ãodeejec¸ão<40%submetidosaimplantac¸ãodeCRT(n=40).Implantou-seumeletrocateter direitonoápex,outronaparedeseptaldotratodesaídadireitoeoutroemposic¸ãovenosa epicárdicaesquerdaconvencional.Calcularam-seodébitocardíaco(usandoosistemaVigileo Flotrac®),oQRSmédioeafrac¸ãodeejec¸ão.
Resultados: Odébitocardíacomédiofoi4,81±0,97L/minemTri-V,4,68±0,94L/mincom
pacingseptaleesquerdoe4,68±0,94L/mincompacingapicaleesquerdo(p<0,001para Tri-VversusambosBiV).OQRSpré-implantac¸ãomédiofoi170±25ms,123±18msemTri-V, 141±25msempacingseptaleesquerdoe145±19empacingapicaleesquerdo(p<0,001 paraTri-VversusambosBiVepré-implantac¸ão).Afrac¸ãodeejec¸ãomédiafoiestatisticamente superioremTri-V(30±11%)versusBi-V(28±12%empacingseptaleesquerdoe28±11em
pacingapicaleesquerdo),eversuspré-implantac¸ão(25±8%).
Conclusão:OpacingemTri-VproduziuumdébitocardíacosuperioreQRSmaisestreitodoque emBi-V.Estesresultadospoderãomodificarofuturodaterapêuticaderessincronizac¸ão. ©2016SociedadePortuguesadeCardiologia.PublicadoporElsevierEspa˜na,S.L.U.Todosos direitosreservados.
Listofabbreviations AF atrialfibrillation AV atrioventricular Bi-V biventricularpacing
CRT cardiacresynchronizationtherapy ECG electrocardiographic
EF ejectionfraction LV leftventricular
NYHA NewYorkHeartAssociation RV rightventricular
RVOT rightventricularoutflowtract Tri-V triple-siteventricularpacing
Introduction
Cardiac resynchronization therapy (CRT) is an established therapyforpatientswithdrug-refractoryheartfailureand electrical evidenceof dyssynchrony. Several large clinical trials have demonstrated that biventricular (Bi-V) pacing significantlyreducesall-causemortalityandheart failure-relatedhospitalizationsandsymptoms,andimprovesquality oflife,exercisetoleranceandleftventricular(LV)systolic performance.1However,evenwhenappropriatelyselected,
20-30%ofpatientsdonotrespondtoCRT.Thismaybedueto incompleteresynchronization,asintraventricularand inter-ventriculardyssynchrony canpersist in 25-30%of patients despiteCRT.2Forsuchnon-responders,multi-siteand
multi-point pacing are emerging as new methods of CRT. The
fewpreviouslypublishedstudiesregardingthesenovel pac-ingmodalitieshaveshownimprovedLVhemodynamicsand synchrony.3---6However,doubtsremainconcerningtheir
indi-cations andshort-termand long-term efficacyand safety, andthustheoptimalmethodofresynchronizationremains unknown.
Inthesubgroup ofpatientswithatrial fibrillation(AF), nofewerthan23%ofallthosewithimplantedCRTdevices,7
studiesarestillscarce,andthesepatientsareparticularly challenging.However,currentlyavailableevidencesuggests CRT may be of benefit. A meta-analysis8 of prospective
cohortstudiescomparingresponsetoCRTinpatientswith sinus rhythmvs.AFshowednotonlythat CRTwas benefi-cialinboth groups, butalsothatthe AFgroupperformed betterintermsofreverseremodeling(assessedas improve-mentinejectionfraction[EF]),albeitwithworsefunctional outcomes.Becauseachievinghighlevelsofpacingisharder inpatientswithAF,thereis evidencethatatrioventricular (AV)junction ablation may further enhance CRT response and improve not only remodelingresponse but also func-tionaloutcomes.9Interestingly,thereisevidencethateven
AFpatients without severelydepressedEF,prolongedQRS or severe heart failure (i.e. in New York Heart Associa-tion[NYHA]class≤II)maybenefitfromCRT.Arandomized trial10 assessingpatientswhounderwentAVjunction
abla-tion due to severely symptomatic permanent AF showed thatCRTwasmorebeneficialthanconventionalright ven-tricular (RV) apical pacing both in patients who met the current recommendations for CRT implantation regarding EF,QRSdurationandfunctionalclassandinthosewhodid not. Finally, only one trial of multi-site pacing has been undertaken in the subgroup of AF patients,11 with good
Thus,todate,theoptimalmethodofcardiac resynchro-nization remains tobe established, especially in patients with AF. We are currently undertaking an observational prospectivetrialtoassessthisissue.Inthispaperwepresent our results from the acute post-implantation phase, with particularfocusonhemodynamicperformance.
In this study cardiac resynchronization with multi-site pacingwasachievedbymeansoftworightventricular(RV) leads.Moststudiesonmulti-sitepacingusedtwoLVleads andoneRVlead.12-14OnlytwotrialsusingtwoRVleadshave
beenpublishedthusfar.5,13Giventhattheformerapproach
has shown to have greater procedure duration, radiation exposure and LV pacing threshold12,15 and that multi-site
pacing using two RV leads has never been assessed in patientswithAF,wechosetousethelatterapproach.
Sincethebenefitofrightventricularoutflowtract(RVOT) septal pacing is still regarded as controversial,14 we also
assessedtheperformanceofRVOTseptalpacingvs.RV api-calpacingasasecondaryobjective,inordertoshedfurther lightonthisquestion.
Objective
Theprimaryaimof thisstudywastoassesstheeffectsof triple-siteventricular(Tri-V)pacingvs.Bi-Vpacingon hemo-dynamicperformanceandQRSduration.Thesecondaryaim wastoassesstheeffectsofRVOTseptalpacingvs.RVapical pacingonhemodynamicperformanceandQRSduration.
Methods
Patientselection
Patientsmeeting all thefollowing criteria wereincluded: (1)permanentAF;(2)EF<40%; (3)heartfailureNYHA≥II despite appropriate medical treatment and baseline QRS >120msorneedforanti-bradycardiapacingwithan antic-ipatedpercentageofventricularpacing>40%;(4)cognitive capacitytounderstandthestudyandhencegiveinformed consent.
Implantationandconnectionmethod
When a CRT defibrillatordevice wasimplanted, the defi-brillator leadwaspositioned inthe RV apex,andfor CRT pacemaker implantation, one conventional RV lead was implantedintheRVapex.Inbothcases,asecondRVlead wasimplantedintheRVOTseptalwallmeetingfluoroscopic criteria14 combinedwithelectrocardiographic(ECG)
crite-riaforcorrectplacement,16ensuringavoidanceoftheRVOT
anterioror freewall. Finally,a coronarysinus leadfor LV pacing was implanted as usual for CRT pacing (i.e. in a posterolateralmid-basal position).The RVapicalleadwas connected tothe RV channel. If the LV lead wasbipolar, withapacingthresholdbelow2.5Vandnodiaphragmatic stimulation,theLVleadwasconnectedtotheatrial chan-nelandtheRVOTleadconnectedtotheLVchannel.Ifthe LVlead wasquadripolar, if the pacing thresholdwasover 2.5V,if specificLVvector programmingwasnecessary,or if therewas any type of diaphragmatic stimulation, then
theLVleadwasconnectedtotheLVchannelandtheRVOT leadwasconnectedtotheatrialchannelonthegenerator. Anydeviceandleadbrandcouldbeused.Programmingwas settoDDDRwiththelowestpossibleAVinterval(25-40ms dependingondevicebrand)andaVVintervalof0ms.
Hemodynamicassessment
Uptoonemonthafterimplantation,allpatientsunderwent minimally invasive hemodynamic assessment with place-mentofaradialarteriallineusingtheFloTracIIITMVigileoTM monitoringsystem(EdwardsLifesciences,Irvine,CA,USA), whichcalculatescardiacoutputbasedonthearterial pres-sure waveform. This system is widely used in peri- and intraoperative settings as well as in intensive care units, andisusefulindetectingsuddenchangesincardiacoutput andvolumestatusprovidedthecardiacrhythmisregular.17
Cardiacoutputandsystolicvolumewereassessedat70 beatsper minute in the following configurations: RV api-cal,RVRVOT,LV,Bi-VpacingusingtheRVapical(RVA)and LVleads (Bi-VRVA-LV), Bi-V pacing usingtheRVOT andLV leads (Bi-V RVOT-LV), and Tri-V. The assessment was per-formedunder≥99%pacing.Inordertoachievetheselevels, AVnodesuppressionwasachievedpreviously bymeans of pharmacotherapyorbyAVnodeablationindrug-refractory cases.Eachconfigurationwasassessedfor15mintoachieve stablemeasurements.Duringtransitions,toavoida poten-tialcarry-overeffect,thefirst5minofmeasurementswere disregarded,andonlymeasurementsfromthefollowing15 minwereconsidered.Theoperatorperformingthe hemody-namicassessmentwasblindedtothepacingmodeused.
Electrocardiographicassessment
Simultaneously with the hemodynamic assessment, all patients underwent standard 12-lead ECG assessment in each of the following configurations: RV apical,RV RVOT, LV,Bi-V RVA-LV, Bi-V RVOT-LV and Tri-V. QRS duration was measured in each of these configurations by two blinded operators.
Echocardiographicassessment
TheechocardiographicstudywasperformedwithaVivid7 device(GeneralElectric®)ineachofthefollowing configu-rations:Tri-V,Bi-VRVA-LVandBi-VRVOT-LV.The studywas undertakensimultaneously with the hemodynamic assess-ment.
EFwasestimatedbytheSimpsonbiplanemethod deter-mined from the cine loops acquired in two-dimensional mode,end-diastolic and latesystolicvolumes being mea-suredinthreeconsecutive cardiac cycles.Post-processing analysiswas performed by two operatorsusing EchoPAC© software(GeneralElectric).
Statisticalanalysis
Meancardiacoutput,QRS andEFwerecalculatedin each group.Differenceswereassessedbyapairedsamplesttest.
Table1 Patientpopulationdetails.
n 40
Age,years(mean±SD) 73±11
Male,n(%) 37(97.5) Ischemiccardiomyopathy,n(%) 10(25) NYHAI,n(%) 3(7.5) NYHAII,n(%) 14(34) NYHAIII,n(%) 24(58.5) NYHAIV,n(%) 0(0) ACEinhibitor,n(%) 34(85)
Aldosteronereceptorblocker,n(%) 3(7.5) Mineralocorticoidreceptorantagonist,n(%) 23(57.5)
Beta-blocker,n(%) 34(85) Diuretic,n(%) 36(90) Digoxin,n(%) 11(27.5) Amiodarone,n(%) 7(17.5) Antithrombotics,n(%) 6(15) VitaminKantagonist,n(%) 24(60) Neworalanticoagulant,n(%) 11(27.5)
Pre-implantationQRS,ms 170±25
Pre-implantationEF,%(mean±SD) 27±6
CRT-D,n(%) 26(65)
CRT-P,n(%) 14(35)
AVnodeablation,n(%) 6(17.5)
ACE:angiotensin-convertingenzyme;CRT-D:cardiac resynchro-nizationtherapydefibrillator;CRT-P:cardiacresynchronization therapypacemaker;EF:ejectionfraction;NYHA:NewYorkHeart Association;SD:standarddeviation.
In order to assess differences in procedure duration, fluoroscopyduration and radiation dosage, the additional amountsoftheseparametersrequiredfor implantationof the second RV lead were quantified, and the differences betweenBi-VandTri-Vwereassessedbythettest.
Ethicalconsiderations
This paperconforms with the Helsinki Declaration onthe EthicalPrinciplesforMedicalResearchInvolvingHuman Sub-jects and was approved by our local ethics committee. Writteninformedconsentwasobtainedfromallpatients.
Results
Population
A total of 40 patients were included. Baseline pre-implantation characteristics are summarized in Table 1. Mostpatients were severely symptomatic, with markedly depressedEF and a significantly prolonged QRS. AV node ablationwasnecessaryinsixpatientspriortohemodynamic assessment.
Hemodynamicresults
The hemodynamic results are depicted in Table 2 and
Figures 1A and B. Cardiac output wassignificantly higher duringTri-VcomparedtoBi-Vpacing.Therewasno statis-tically significant differencebetweenthe twoBi-V pacing
Table2 Cardiacoutputindifferentpacingconfigurations. Pacingconfiguration Cardiacoutput,
l/min(mean±SD)
Tri-V 4.81±0.97
Bi-VwithRVOTseptalpacing 4.68±0.94 Bi-VwithRVapicalpacing 4.66±0.91
RVOTseptalpacing 4.56±0.93
RVapicalpacing 4.44±0.84
LVpacing 4.47±0.92
Bi-V: biventricularpacing; LV: leftventricular; RV: right ven-tricular;RVOT:rightventricularoutflowtract;Tri-V:triple-site pacing. 5
A
B
p<0.001 Pacing configuration Pacing configuration Tri-V Bi-V (RVOT) RVOT Bi-V (apical) Rv apical LV Tri-V Bi-V (RVOT) RVOT Bi-V (apical) Rv apical LV p<0.001 p=NS p=NS p=NS p=0.007 4.9 4.8 4.7 4.6 4.5 4.4 4.3 4.2 4.1Cardiac output (l/min)
Cardiac output (l/min)
4 5 4.9 4.8 4.7 4.6 4.5 4.4 4.3 4.2 4.1 4
Figure1 DifferencesincardiacoutputbetweenTri-Vand Bi-Vpacing(A),betweenBi-VpacingandRVOTseptalpacing,and between RVOT septalpacing and RV apical pacing (B). Bi-V: biventricularpacing;LV:leftventricular;RV:rightventricular; RVOT:rightventricularoutflowtract;Tri-V:triple-sitepacing.
configurations, nor between Bi-V pacing and RVOT septal pacing. The latter produced a significantly higher cardiac output than RV apical pacing. These differences remain acrossischemicandnon-ischemiccardiomyopathygroups.
Electrocardiographicresults
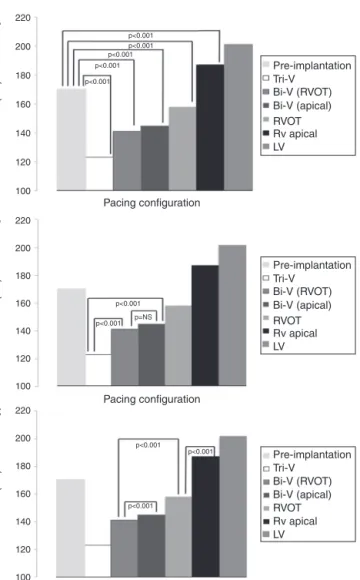
MeanQRSdurationineachpacingconfigurationisdepicted in Table 3 and Figures 2A, B and C. Tri-V pacing pro-duced a significantly shorter QRS than pre-implantation
Table3 QRSdurationineachpacingconfiguration. Pacingconfiguration MeanQRS,ms(mean±SD)
Tri-V 123±18
Bi-VwithRVOTseptalpacing 141±25 Bi-VwithRVapicalpacing 145±19 RVOTseptalpacing 158±20 RVapicalpacing 187±18
LVpacing 201±22
Bi-V: biventricularpacing; LV:left ventricular; RV:right ven-tricular;RVOT:rightventricularoutflowtract;Tri-V:triple-site pacing. p<0.001 p<0.001 p<0.001 p<0.001 p<0.001 p<0.001 p=NS p<0.001 p<0.001 p<0.001 p<0.001 Pacing configuration Pacing configuration Pacing configuration Tri-V Pre-implantation Bi-V (RVOT) RVOT Bi-V (apical) Rv apical LV QRS (ms) 100 120 140 160 180 200 220
A
B
C
QRS (ms) 100 120 140 160 180 200 220 QRS (ms) 100 120 140 160 180 200 220 Tri-V Pre-implantation Bi-V (RVOT) RVOT Bi-V (apical) Rv apical LV Tri-V Pre-implantation Bi-V (RVOT) RVOT Bi-V (apical) Rv apical LVFigure2 DifferencesinmeanQRSbetweenpre-implantation andpacing(A),betweenTri-VandBi-Vpacing(B),betweenBi-V andRVOTseptalpacing,andbetweenthelatterandRVapical pacing(C).Bi-V:biventricularpacing;LV:leftventricular;RV: rightventricular;RVOT: rightventricularoutflowtract;Tri-V: triple-sitepacing.
QRS and both Bi-V pacing configurations.Bi-V pacing also significantly shortened QRS duration compared with pre-implantation QRS. There was no statistically significant difference between the two Bi-V pacing configurations. RVOTseptalpacingproducedasignificantlyshorterQRSthan
Table4 Echocardiographicejectionfractionineach pac-ingconfiguration.
Pacingconfiguration Ejectionfraction, %(mean±SD)
Pre-implantation 25±8
Tri-V 30±11
Bi-VwithRVOTseptalpacing 28±12 Bi-VwithRVapicalpacing 28±11
Bi-V:biventricularpacing;RV:rightventricle;RVOT:right ven-tricularoutflowtract;Tri-V:triple-sitepacing.
Pacing configuration Pacing configuration Tri-V Pre-implantation Bi-V (RVOT) Bi-V (apical) Ejection fr action 20 22 24 26 28 30 32 34
A
B
Ejection fr action 20 22 24 26 28 30 32 34 Tri-V Pre-implantation Bi-V (RVOT) Bi-V (apical) p<0.001 p=0.07 p=0.018 p=0.005 p=NS p=0.0017Figure3 Differencesinmeanejectionfractionbetween pre-implantation and cardiac resynchronization therapy (A) and betweenTri-VandBi-Vpacing(B).Bi-V:biventricularpacing; RVOT:rightventricularoutflowtract;Tri-V:triple-sitepacing.
pre-implantationQRS andRVapicalpacingQRS,buta sig-nificantly longer QRS than Bi-V pacing. These differences remainacross ischemic and non-ischemic cardiomyopathy groups.
Echocardiographicresults
EFresultsaredepictedinTable4andFigures3AandB.All modesof CRTproduceda statisticallysignificant improve-mentinEF.Tri-Vproducedthegreatestimprovement,with asignificantdifferencecomparedtoBi-V.Thesedifferences remainacross ischemic and non-ischemic cardiomyopathy groups.
Table5 ProcedureandfluoroscopytimesandradiationdoseinTri-Vpacingvs.conventionalBi-Vpacing.
Tri-V Bi-V p
Proceduretime,min(mean±SD) 81±34 75±31 NS
Fluoroscopytime,min(mean±SD) 15±11 14±12 NS
Radiationdose,Gy/cm2(mean±SD) 0.61±0.38 0.58±0.32 NS
Bi-V:biventricularpacing;Tri-V:triple-sitepacing.
Meanfluoroscopyandproceduretime
AlthoughimplantationoftheTri-Vsystemresultedinlonger procedure and fluoroscopy times, the difference wasnot significant compared to conventional Bi-V implantation (Table5).
Discussion
In this study, Tri-V pacing produced a superior hemody-namicperformancecomparedtoconventionalBi-Vpacing, asdemonstratedbyincreasedcardiac outputand EF.This islikelyanimmediateconsequenceofimproved resynchro-nization,giventhatQRSdurationwassignificantlyshorterin Tri-Vpacingvs.conventionalBi-Vpacing,andthatthiswas anacutephasestudy,inwhichreverseremodelingcouldnot yethaveoccurred.ThereductioninQRSdurationobtained byTri-V pacingis especiallyremarkable,QRShaving been shortenedalmosttonormallength.Ourfluoroscopyand pro-ceduretimeswerescarcelyprolongedbythistechnique,and assuchwerenotasignificantlimitation.
There havebeen few studies onmulti-sitepacing,and themethodologyhasbeenveryheterogeneousregardingnot only pacingand implant techniques, but also themethod usedforassessinghemodynamicresponse.MostusedtwoLV leadsandoneRVlead.Inonenon-randomizedtrialoneof theLVleadswasconnectedtotheatrialchannel(allpatients hadpermanentAF),andtheothertwoleadswereconnected asusual. Triple-sitepacing yieldedhigherEF andreduced end-systolicvolume,withoutclinicalimprovement,atthree months.11 Ofcourse,byconnectingan LVleadtoan atrial
channel,theuseofvectorsislimited.Twootherrandomized trialsusedasimilarapproachbutconnectedbothLVleads withaY-connector.Theydemonstratedanadditionalclinical benefit,but greaterprocedure length, radiation exposure andLVpacingthreshold.12,15Regardingsafety,noneofthese
trialshave shown significant differences between Tri-V or Bi-Vpacing,andOganoetal.18recentlydemonstratedthat
dualLVpacingmightevenhaveaprotectiveeffectagainst ventriculararrhythmias.3
Only three trials using two RV leads and one LV lead alonehavebeenpublished.5,13,19However,intwoofthese,
theconnection technique wasdifferent,asboth RV leads were connected to the atrial channel by means of a Y-connector. Systolic function was assessed invasively by determiningpeakLVdP/dt(usingamicromanometer-tipped pigtailangiographiccatheter)andalsocardiacoutputwith aSwan-Ganzcatheter.Dyssynchronywasassessedwith tis-sueDoppler echocardiographicimaging. QRSduration was alsoassessedineachpacingconfiguration.Triple-site pac-ingwassuperiorregardingallfourparameterscomparedto
conventional BiV pacing.Therewere alsonosafetyissues regardingthismethod.Finally,onetrialusedbothtypesof triple-sitepacing(i.e.onegroupreceivedtwoRVleads,and anothertwoLVleads),withbetterclinicalandhemodynamic results in triple-site pacing compared toconventional Bi-Vpacing.20 AveryrecentrandomizedtrialcomparedTri-V
pacingwithconventionalBi-Vpacingintermsofclinicaland echocardiographicdataat12-monthfollow-up.Therewere nodifferencesinadverseeventsorclinicalbenefit,however Tri-VdidproducehigherEFat12months.5,13,19
Despite the heterogeneity of the studies, and the unique methodologyof ourstudy,all of these trialsusing triple-sitepacinghavedemonstratedsuperiorhemodynamic performanceandincreasedresynchronizationcomparedto conventional Bi-V pacing. The benefitwasalsopresent in AFpatients.11Thus,ourresultsareconsistentwithprevious
studies.
Itisworthnotingthatnoprevioustrialhaseverassessed theuse oftriple-sitepacingwithtwoRVleadsin patients withpermanentAF.Giventhatthesepatientsrepresentan understudiedandparticularlychallenginggroup,ourstudy adds pioneeringscientificdataonthismodalityofcardiac resynchronizationtherapyinthissubgroup.
Regardingtheresultsofsingle-sitepacing,ourstudy pro-duced interesting results. RVOT septal pacing wasclearly superior toRV apical pacing, with improved cardiac out-put and much shorter QRS duration. RVOT septal pacing aloneevendecreasedbaselineQRSlengthinourpatients. Studies comparing these two pacing modalities have pro-ducedconflictingresults.14 However,thediscrepanciesare
largelydue tothesignificant heterogeneity inlead place-ment technique:fewstudies havebeen carefulenoughto ensure proper lead placement in both the RVOT and the septalwall. This wasa criticalconcernin ourstudy. Sev-eraltrials in which theRV lead wasplaced undercareful fluoroscopic and/or electrocardiographicguidance yielded superior results for RVOT septalpacing.14 Our study adds
furtherweighttothisevidence.
Finally,theabsenceof astatisticaldifferencebetween cardiacoutputwithBi-VpacingandRVOTseptalpacingwas anunexpectedfinding,especiallyconsideringthattheQRS wassignificantlyshorterwithBi-Vpacing.Theclinical signif-icanceofthisfindingisunclear,giventhatwewerenot com-paringtheclinicalperformanceofthesetwopacing modali-ties.Studiescomparingsingle-siteRVpacingvs.Bi-Vpacing used echocardiographic and clinical endpoints obtained sometimeafterimplantation,andnotimmediate hemody-namicdata.21Inaddition,themajorityofthesestudies
com-pareRVapicalpacingratherthanRVOTseptalpacing.Thus, nostudycanbedirectlycomparedtoours,andwhilemost studiesfavorBi-Vpacing,theabove-mentionedlimitations regardingRVpacingsitemaybeofgreaterimportancethan
previouslythought.Therefore,whatevertheinterpretation ofourparticularresults,theyhighlighttheimportanceand potentialofRVOTseptalpacing.Indeed,inpatientsinwhom theCRTindicationisbasedonneed forpacingratherthan primarily onheart failure,could RVOTseptalpacing be a sustainable alternative to Bi-V pacing? Our trial was nei-ther designed nor statistically powered to answer such a question,butaddsfurtherevidencetotheissue.
Limitations
Ourstudy has several limitations. Use of the FloTracIIITM VigileoTMmonitoringsystemistime-consumingandwhileit hasbeen wellvalidatedinavarietyofclinicalscenarios,17
thisisthefirsttimethatithasbeentestedinthissetting. Also,ischemiccardiomyopathywasfoundinonly25%ofall patients.Despitethefactthatstatisticalresultswere sim-ilaracross thissubgroupof patients,theabsolute number of patients is small, and as such this heterogeneity may haveinfluencedourresults.Finally,althoughthe echocar-diographicresultswerestatisticallysignificant,theresulting differences are small and within the inter- and intraob-server variabilityof thetechnique. Thus,theseparticular results should be interpreted with caution. The observed differences in cardiacoutput were alsosmall,and there-fore we cannot yet be absolutely sure of their clinical significance.
Future
directions
The factthat multipletechniques, includingours, yielded benefit suggests that multi-site pacing should be further developed.Theoptimalmethod,whetherwithtwoRVleads, twoLVleads,asingleleadwithmulti-pointpacing capabil-itiesoracombinationof theseremains tobedetermined. Webelieve thatifthreeventricularleads aretobeused, two RV leads are much faster and probably more stable. The development of CRT generators designed specifically for multi-site pacing may also be important. So far only onemanufacturerhasproducedsuchadevice,whichwillbe testedinnon-respondersinarandomizedtrial.22Itisworth
pointing out,however, that in ourpopulation we deliber-ately did not select a subset of non-responders, and still achievedsuperiorresultswiththisnewpacingmodality.This raisesthepossibilityoforganizingalargetrialofmulti-site pacing as a first-line treatment in candidates for cardiac resynchronizationtherapy.
Conclusion
Triple-site pacing produced a superior hemodynamic per-formance with shorter QRS duration, which is likely the consequence of improved resynchronization. RVOT septal pacingwasclearlysuperiortoRVapicalpacing,withshorter QRSandgreatercardiacoutput.
Ethical
disclosures
Protection of human and animal subjects.The authors declare thatthe procedures followedwere in accordance
withtheregulationsoftherelevantclinicalresearchethics committeeandwiththoseoftheCodeofEthicsoftheWorld MedicalAssociation(DeclarationofHelsinki).
Confidentialityofdata.Theauthorsdeclarethattheyhave followedtheprotocolsoftheirworkcenteronthe publica-tionofpatientdata.
Righttoprivacyandinformedconsent.Theauthorshave obtainedthe written informed consentof the patients or subjectsmentionedinthearticle.Thecorrespondingauthor isinpossessionofthisdocument.
Funding
Nospecificfundinggrantswereusedregardingthisstudy.
Conflicts
of
interest
Theauthorshavenoconflictsofinteresttodeclare.
References
1.AbrahamWT,FisherWG,SmithAL,etal.Cardiac resynchroniza-tioninchronicheartfailure.NEnglJMed.2002;346:1845---53. 2.Bleeker GB, Bax JJ, Fung JW-H, et al. Clinical versus echocardiographic parameters to assess response to cardiac resynchronizationtherapy.AmJCardiol.2006;97:260---3. 3.Lenarczyk R, Kowalski O, Sredniawa B, et al.
Implanta-tion feasibility, procedure-related adverse events and lead performance during 1-year follow-up in patients undergo-ing triple-site cardiac resynchronization therapy:a substudy ofTRUST CRTrandomized trial.JCardiovasc Electrophysiol. 2012;23:1228---36.
4.Pappone C, Calovi´c Z, Vicedomini G, et al. Multipoint left ventricularpacinginasinglecoronarysinusbranchimproves mid-term echocardiographic and clinicalresponseto cardiac resynchronizationtherapy.JCardiovascElectrophysiol.2014. 5.YoshidaK,SeoY,YamasakiH,etal.Effectoftriangleventricular
pacingonhaemodynamics and dyssynchronyin patientswith advancedheartfailure:acomparisonstudywithconventional bi-ventricularpacingtherapy.EurHeartJ.2007;28:2610---9. 6.GinksMR,ShettyAK,LambiasePD,etal.Benefitsofendocardial
andmultisitepacingaredependentonthetypeofleft ventricu-larelectricactivationpatternandpresenceofischemicheart disease:insightsfromelectroanatomicmapping.CircArrhythm Electrophysiol.2012;5:889---97.
7.Dickstein K, Bogale N, Priori S, et al. The European car-diac resynchronizationtherapy survey.EurHeartJ. 2009;30: 2450---60.
8.Upadhyay GA, Choudhry NK, Auricchio A, et al. Cardiac resynchronizationin patientswithatrialfibrillation: a meta-analysis of prospective cohort studies. J Am Coll Cardiol. 2008;52:1239---46.
9.Wilton SB,Leung AA, Ghali WA,et al. Outcomesof cardiac resynchronizationtherapyinpatientswithversusthose with-outatrialfibrillation:a systematicreviewandmeta-analysis. HeartRhythm.2011;8:1088---94.
10.BrignoleM,BottoG,MontL,etal.Cardiacresynchronization therapyinpatientsundergoingatrioventricularjunction abla-tionforpermanent atrialfibrillation: arandomizedtrial.Eur HeartJ.2011;32:2420---9.
11.Leclercq C, Gadler F, Kranig W, et al. A randomized com-parison oftriple-site versus dual-siteventricular stimulation
in patientswithcongestiveheartfailure.JAm CollCardiol. 2008;51:1455---62.
12.LenarczykR,KowalskiO,SredniawaB,etal.Triple-siteversus standardcardiacresynchronizationtherapystudy(TRUSTCRT): clinical rationale,design, and implementation. J Cardiovasc Electrophysiol.2009;20:658---62.
13.Yamasaki H, Seo Y, Tada H, et al. Clinical and procedural characteristicsofacutehemodynamicresponders undergoing triple-siteventricularpacingforadvancedheartfailure.AmJ Cardiol.2011;108:1297---304.
14.Hillock RJ, Mond HG. Pacing the right ventricular outflow tractseptum:timetoembracethefuture.Europace.2011;14: 28---35.
15.LenarczykR, KowalskiO, KukulskiT, et al.Triple-site biven-tricularpacinginpatientsundergoingcardiacresynchronization therapy:afeasibilitystudy.Europace.2007;9:762---7.
16.McGaviganAD, Roberts-Thomson KC,Hillock RJ,et al. Right ventricular outflow tract pacing: radiographic and elec-trocardiographic correlates of lead position. Pacing Clin Electrophysiol.2006;29:1063---8.
17.Mayer J, Boldt J, PolandR, et al. Continuous arterial pres-surewaveform-basedcardiacoutputusingtheFloTrac/Vigileo:
a review and meta-analysis. J Cardiothorac Vasc Anesth. 2009;23:401---6.
18.OganoM,IwasakiY,TanabeJ,etal.Antiarrhythmiceffectof cardiacresynchronizationtherapywithtriple-sitebiventricular stimulation.Europace.2013;15:1491---8.
19.AnselmeF,Bordachar P,PasquiéJL,et al.Safety,feasibility, andoutcomeresultsofcardiacresynchronizationwith triple-siteventricularstimulationcomparedtoconventionalcardiac resynchronization.HeartRhythm.2015.
20.RogersDPS,LambiasePD,LoweMD,etal.Arandomized double-blindcrossovertrialoftriventricularversusbiventricularpacing inheartfailure.EurJHeartFail.2012;14:495---505.
21.BrignoleM, Auricchio A, Baron-Esquivias G, et al. 2013 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy:theTaskForceoncardiacpacingandresynchronization therapyoftheEuropeanSocietyofCardiology(ESC).Developed incollaborationwiththeEuropeanHeartRhythmAssociation. EurHeartJ.2013;34:2281---329.
22.Triple-site biventricular stimulation in the optimiza-tion of CRT. ClinicalTrials.gov [Internet]. Available from: https://clinicaltrials.gov/ct2/show/NCT02350842 [accessed 25.04.15].