Arq. Bras. Cardiol. vol.91 número1 en a07v91n1
Texto
Imagem

Documentos relacionados
With respect to the article “Catheter Ablation of Atrial Fibrillation – Techniques and Results”, published in the October 2005 edition (Arq Bras Cardiol. 2005;85:295- 301), the
Neste trabalho o objetivo central foi a ampliação e adequação do procedimento e programa computacional baseado no programa comercial MSC.PATRAN, para a geração automática de modelos
The probability of attending school four our group of interest in this region increased by 6.5 percentage points after the expansion of the Bolsa Família program in 2007 and
We found that it is true that mahogany is a mid-successional species; its leaves showed greater plasticity for leaf growth allometry than tonka bean.. For leaf nutrient content,
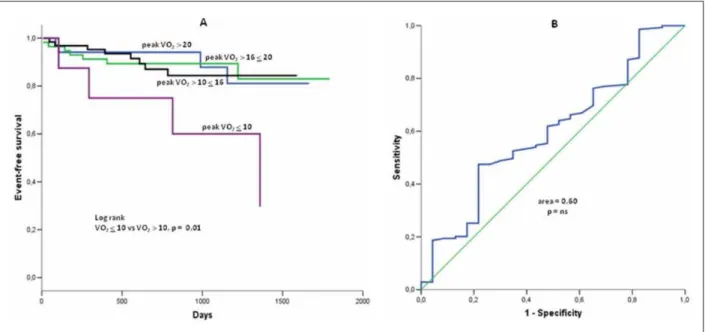
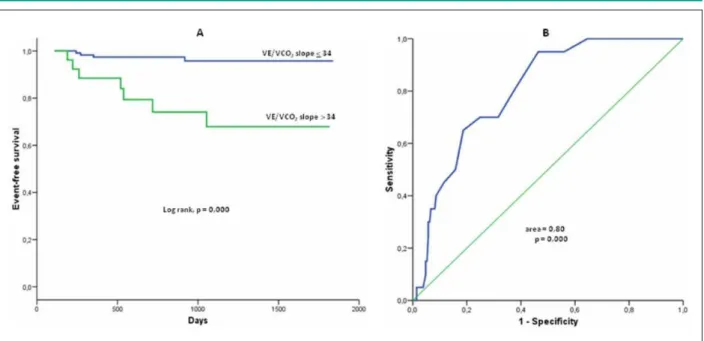
Conclusion: The present study showed that there was an incidence of patients with EOV and lower peak VO 2 and higher VE/VCO 2 slope values, but they showed no difference on other
In particular, the results of our study showed that most older women with acute LBP were at risk of sarcopenia and had worse performance in the mobility/balance test, confirming
Seja através da ação à escala de uma cidade, no caso do Grupo Pro-Évora, seja com propósitos e ações de alcance nacional, os dois exemplos evidenciam a importância que
O fato de que no cristianismo uma determinada forma de “ poimênica” toma o lugar da prática do cuidado de si da Antiguidade significa, sob essa perspectiva, nada mais
