SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Update
Article
Advantages
and
limitations
of
national
arthroplasty
registries.
The
need
for
multicenter
registries:
the
Rempro-SBQ
夽
Luiz
Sérgio
Marcelino
Gomes
∗,
Milton
Valdomiro
Roos,
Edmilson
Takehiro
Takata,
Ademir
Antônio
Schuroff,
Sérgio
Delmonte
Alves,
Antero
Camisa
Júnior,
Ricardo
Horta
Miranda
SociedadeBrasileiradeQuadril(SBQ),RegistroMulticêntricodeProcedimentosOperatórios(Rempro),Batatais,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received14December2016
Accepted26January2017
Availableonline13September2017
Keywords:
Arthroplasty,replacement,
hip/surgery
Arthroplasty,replacement,
hip/complications
Prosthesisfailure
Registries
a
b
s
t
r
a
c
t
Whilethevalueofnationalarthroplastyregistries(NAR)forqualityimprovementintotalhip
arthroplasty(THA)hasalreadybeenwidelyreported,somemethodologicallimitations
asso-ciatedwithobservationalepidemiologicalstudiesthatmayinterferewiththeassessment
ofsafetyandefficacyofprostheticimplantshaverecentlybeendescribedintheliterature.
AmongthemainlimitationsofNAR,theneedforatleast80%complianceofallhealth
institutionscoveredbytheregistryisemphasized;completenessequalorgreaterthan90%
ofallTHAperformed;restricteddatacollection;useofrevisionsurgeryasthesole
crite-rion foroutcome;andtheinabilityofestablishingadefinitecausallinkwithprosthetic
dysfunction.
ThepresentarticleevaluatestheadvantagesandlimitationsofNAR,inthelightof
cur-rentknowledge,whichpointtotheneedforabroaderdatacollectionandtheuseofmore
structuredcriteriafordefiningoutcomes.
Inthisscenario,theauthorsdescribeofidealization,conceptualandoperational
struc-ture,andtheprojectofimplantationandimplementationofamulticenterregistrymodel,
calledRempro-SBQ,whichincludeshealthcareinstitutionsalreadylinkedtotheBrazilian
HipSociety(SociedadeBrasileiradeQuadril[SBQ]).Thispartnershipenablesthecollection
ofmorereliableandcomprehensivedataatahigherhierarchicallevel,withasignificant
reductioninmaintenanceandfinancingcosts.Thequalityimprovementactionssupported
bySBQmayenhanceitseffectivenessandstimulategreateradherenceforcollecting,storing,
interpreting,anddisseminatinginformation(feedback).
©2017SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora
Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedbythemembersoftheDiretoriade RegistroMulticêntricodeProcedimentosOperatórios (Rempro),Sociedade
BrasileiradeQuadril(SBQ),Batatais,SP,Brazil.
∗ Correspondingauthor.
E-mails:[email protected],[email protected](L.S.Gomes).
http://dx.doi.org/10.1016/j.rboe.2017.08.008
2255-4971/©2017SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Thisisanopenaccessarticle
Vantagens
e
limitac¸ões
dos
registros
nacionais
de
artroplastias.
A
necessidade
de
registros
multicêntricos:
O
Rempro-SBQ
Palavras-chave:
Artroplastiadequadril/cirurgia
Artroplastiade
quadril/complicac¸ões
Falhadeprótese
Registros
r
e
s
u
m
o
Ainda queosregistros nacionais deartroplastias (RNAs) sejamum importante
instru-mentodecontroleemelhoriadaqualidadedaartroplastiatotaldequadril(ATQ),algumas
limitac¸ões metodológicas associadas aos estudos epidemiológicos observacionais, que
podeminterferirnaavaliac¸ãodaseguranc¸aeeficáciadosimplantesprotéticos,têmsido
recentementedescritasnaliteratura.
Dentreasprincipaislimitac¸õesdestacam-seanecessidadedecoberturamínimade80%
dasinstituic¸õeshospitalaresdaregiãoobjetodoregistro;integralidademínimade90%de
todasasATQsfeitas;coletadeinformac¸õesmaisrestritas;usodacirurgiaderevisãocomo
critérioúnicodedesfechoeadificuldadedeseestabelecerumnexocausalcomadisfunc¸ão
protética.
Nopresenteartigoavaliamosasvantagenselimitac¸õesdosRNAs,àluzdos
conheci-mentosatuais,queapontamparaanecessidadedacoletadeinformac¸õesmaisamplase
deusodecritériosmaisestruturadosnadefinic¸ãodedesfechos.
Nessecenário,descrevemososprocessosdeidealizac¸ão,aestruturaconceituale
opera-cionaleoprojetodeimplantac¸ãoeimplementac¸ãodeummodeloderegistromulticêntrico,
denominadoRempro-SBQ,queincluioscentroshospitalaresdetreinamentoemcirurgiade
quadriljáligadosinstitucionalmenteàSociedadeBrasileiradeQuadril(SBQ).Essa
parce-riapossibilita,simultaneamente,acoletadeinformac¸õesmaisabrangentesedeelevado
nívelhierárquico, deformaconfiável,comreduc¸ãobastantesignificativadoscustos de
manutenc¸ãoefinanciamento.Asac¸õesdemelhoriadaqualidade,amparadaspelaSBQ,
podemprotagonizarumacondic¸ãodemaiorefetividadeemaioradesãoaosprocedimentos
decoleta,armazenamento,interpretac¸ãoedivulgac¸ãodasinformac¸ões.
©2017SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier
EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Although total hip arthroplasty (THA)is a procedure with
excellent risk– and cost–benefit ratios that provides pain
reliefand functionrecoveryinpatientswithterminaljoint
disease, the rate ofcomplications and patient
dissatisfac-tion with the surgical procedure ranges between 7% and
15%.1,2 Whilethe occurrenceofsurgicalcomplicationsmay
involvecharacteristicsanddeterminantsthatareoften
dis-tinct from those related to patient satisfaction, it should
beconsidered that theultimate goal ofarthroplasty isthe
recovery of quality of life, by achieving a painless,
func-tional, stable,and lastingprosthetic reconstruction. Inthis
context,adverseeventsandcomplicationsassociatedtothis
procedureshouldbeassessedconsideringthepresenceof
per-manentprostheticimplants,aswellasthefunctionalityand
longevityoftheprostheticjointreplacement(PJR)associated
tothem.
Longitudinal evaluations that investigate signs of
pros-thetic dysfunction (symptomatic or asymptomatic) have
alwaysbeen highlyrecommendedtoidentifyearlyadverse
events,complications,andpoorlyperformingimplants,thus
allowingearlymanagementplanning,aimingtopreventthe
occurrence of progressive bone loss and irreversible
peri-articular and/or vascular and nervous damage that can
compromisethequalityoffutureprostheticjoint
reconstruc-tionatanytime.
Cycles
of
innovation
and
quality
control
of
arthroplastic
implants
Priortothe1960sanduntiltheearly1970s,wheninnovations
inthisareaofknowledgewereveryfrequent,theintroduction
anduseofprostheticimplantsinclinicalpracticewerebased
on evidence of low scientificquality, suchas expert
opin-ionsand/orretrospectiveseriesofclinicalcases,commonly
conductedby theimplant/procedure designers themselves.
During thiscycle, termedtheempiricalcycle ofinnovation
andqualitycontrol,oreventhetrial-and-errorcycle(Fig.1A),3
the only criterion for keeping an implant on the market
wastheinformationfromthesetypesofstudy;thus,
count-lessscientificreveriesandsomecreativebreakthroughshave
givenrisetoimplantsandprocedureswithtrulycatastrophic
outcomes.
The following decades were marked by the progressive
interferenceandenforcementmeasuresofeither
governmen-tal or private regulatory and surveillance organizations, in
additiontopost-marketsurveillance.Theseentitiesbeganto
A
Procedure or implant design
Regulation
Unnaceptable failure rate Satisfactory
results
Clinical trials
Experimental studies (concepts or materials)
Concepts or materials
Marketing approval
Post-marketing surveillance
Regulation Approval Private
Efficacy and safety assessment (Tests and assays)
Government Similarity
Approval
New concepts or materials
Clinical research
Experimental searches In vivo
production/ application
B
Fig.1–Empiricalcycleofinnovationandqualitycontrol,ortrial-and-errorcycle(A)andtheanalyticalcycleofinnovation andqualitycontrol(B)inprostheticjointimplants.
pre-clinicalstudiesandtrials.Thiscycleistermedanalytical
cycleofinnovationandqualitycontrol(Fig.1B).3
Althoughevidenceoflowscientificquality(retrospective
caseseries)waswidelyacceptedinpost-marketsurveillance,
andstill is,theuse ofrandomizedcontrolledclinicaltrials
(RCTs)ofhighscientificqualitywasalsoproposedfor
effec-tivenessandsafetyassessment,especiallyastestspriortothe
authorizationtomarketnewimplants.
Althoughwell-suitedaspre-clinicaltrials,theuseofRCTs
inthelongitudinalevaluationofpatientsundergoingPJRshas
somedisadvantages.Apracticalexampleistheuseofthehip
arthroplasticimplantsintroducedbyChristiansenin1969in
Norway.ThefirstreportsbySudmannetal.4indicateda
revi-sionrateof31%infivetoeightyearsoffollow-up,compared
witharateof4%fortheCharnleyprosthesis,consideredthe
goldstandard,inthesametimeinterval.However,overthis
13-yearperiod,over10,000Christiansenimplantshadalready
beenmadeinNorway.5
RCTs
vs.
observational
epidemiological
studies
(OESs)
on
post-market
quality
control
of
arthroplastic
implants
ThemaindisadvantagesintheuseofRCTsfortheassessment
ofpatientssubmittedtoPJRare:(a)prosthetic(andtherefore
permanent)articularimplantsrequireunlimitedfollow-upto
the ultimate outcome;(b) adverse PJR effectsare also
rep-resentedbylowfrequencycomplications,butwithahigher
prevalenceinthelong term,which alsoindicates theneed
for long-termfollow-up; (c) foradequate statistical
signifi-cance,RCTsrequiretheinclusionofahighnumberofpatients.
Infact,toobtainalevelofsignificanceof0.05andapower
of80%,it isnecessary toinclude3008patientstodetect a
3–5%differenceinfailureratebetweentwodifferentimplants,
whereasitisnecessarytoinclude13,474patientstodetecta
Table1–DisadvantagesofRCTsandadvantagesofOESs,determinedbythecharacteristicsoflongitudinalevaluationin patientswithprostheticjointreplacements(PJRs).
CharacteristicsoftheevaluationinPJR RCTs(disadvantages) OESs(advantages)
Permanentimplants(unlimited follow-up)
Expensivestudieswithrestrictive inclusioncriteriaanddifficultyto follow-upanunlimitednumberof patientsandprocedures
Lowercostforlong-termfollow-up andpossibilityofincludingofan unlimitednumberofpatientsand procedures
Low-frequencyifcomplicationsand significantprevalenceinlong-term follow-up
Highnumberofpatientsandprocedures Real-worldview,withdifferentcenters andsurgeonsinvolved(external validation)
Centersofexcellence Fewsurgeonsinvolved
Reporttherealityoftheinstitution (limitedgeneralization)
Participationofalargenumberof centersandsurgeons
(generalizationispossible)
Cross-sectionalevaluations(survival curves)
Unusualpractice(predeterminedperiods) Usualpractice
(longitudinal-to-endpoint) Numberofexposurefactorsand
outcomes(simultaneous)
Limited Multiple
RCTs,controlledandrandomizedcontrolledtrials;OESs,observationalepidemiologicalstudies.
(d)RCTsreflectthe realityofoneinstitution, andtoooften involvetheparticipationofwell-trainedsurgeonsincenters ofexcellence.Thus,from the real-worldstandpoint,which isexpectedto includedifferentcenters and surgeons with differentlevelsoftraining,analysisisimpaired, compromis-ingthepossibilityofgeneralizations(external validation),a veryrelevantaspectintheassessmentofthesafetyof per-manentimplants.Nonetheless,RCTsforPJR arevery often conductedbythedesignersoftheimplantstobeevaluated, whichisanadditionalbias7;(e)duetotheverydesignofRCTs,
patientinclusionislimited;(f)theevaluationofimplantsin
PJRrequiresunlimitedcross-sectionalandlongitudinal
stud-ies,inordertoconstructsurvivalcurves,apracticethatisnot
commonduringRCTs;and(g)RCTsarenotadequatewhen
simultaneousmulti-factorexposureandoutcomeevaluation
arerequired(Table1).
Therefore, RCTsare aratheronerous option, difficultto
perform,andwithspecificbiases,consideringthe
particular-itiesoflongitudinalevaluationstudiesofpatientssubmitted
toPJR.
In this scenario, observational epidemiological studies
(OESs)havebecome animportanttoolforthe early
detec-tionoffailuresinPJRosteoarticularimplants.Whencompared
withRCTs, which are considered tobethe highestquality
intheproductionofscientificevidence,OESshaveprovedto
bequiteattractive,sincetheyarelesscostlyandsupportthe
inclusionofalargenumberofpatients,whocanbe
followed-up forlonger periods,evidencing failures long before they
areidentifiedbyRCTs,whileassessingtheresultswithina
scenarioclosertoreallife,withtheinvolvementof
numer-oussurgeonsfromdifferentcenters.OESsarecreditedwith
notonlythegreaterpossibilityofgeneralizingtheirfindings,
whichstrengthensthe implantsafety assessment,but also
withtheopportunitytosimultaneouslystudymultiple
expo-surefactorsandoutcomes.
Itshouldbenotedthattheinitialimpactoftheincreased
useofOESsinnon-orthopedicareaswasverynegativeand
stronglycriticized.StudiesthatcomparedtheresultsofRCTs
and epidemiological studies in non-orthopedic specialties
between1970and1980suggestedthatOESscouldenhance
thepositiveeffectsoftreatment.8–10
Thus,atrendtosacrificeOESsarose,suggestingthatsuch
studieswouldnotbeappropriateforevidence-basedmedical
care;tothepointthatSackettstatedthat,“Ifthestudywasn’t
randomized,we’dsuggestthatyoustopreadingitandgoon
tothenextarticleinyoursearch.”11
Nonetheless, in the followingdecades, the
inconsisten-ciesbetweenthe resultsofRCTsandOESs wereattributed
tothedesignandinadequate implementationofthe latter,
especiallyregardingstudydesign,qualityoftheinformation
collected,and statisticalmethodologyadopted,which were
responsiblefornumeroussystematicbiases.
Infact,amorerecentstudycomparingtheresultsofRCTs
withOESsinarticlespublishedafter1985concludedthatthere
werenosignificantdifferencesbetweenthefindingsofboth
studies.12Theauthorscreditedthisevolutiontothereduction
ofsystematicbiasduetoamoreelaborate processofdata
collecting,storing,andprocessing,aswellastheincreased
sophistication in the scientific methodology adopted in
OESs.
National
Arthroplasty
Registries
(NARs)
Thegreatadvances,standardizations,andimprovementsin
the scientific qualityof the OESswere undoubtedly driven
bytheNARs,whosecreation,implantation,and
implemen-tationisintertwinedwiththeevolutionofthemethodological
qualityofOESs.
Theconceptofmedicalregistryisnotnew;itsbeginnings
dateto1905,withanattempttoregistercancerpatientsin
Denmark.Thus,evenconsideringthewidevarietyofregistry
types(ofpatients,diseases,procedures,treatments,and
prod-ucts,amongothers),theirimportanceintheassessmentof
newtypesoftreatmenthaslongbeenrecognized,primarily
inthecontrolandimprovementofthequalityofhealthcare.
abletoanswerquestionsthathavenotyetbeenclarifiedand
thatcannotberesolvedotherwise.
AccordingtoGliklich,apatientregistryisanorganized
sys-temthatusesobservationalstudymethodstocollectuniform
(clinicaland other) dataand to evaluatespecificoutcomes
inapopulationdefinedbyaparticulardisease,condition,or
exposure,fulfillingoneormorepredeterminedpurposes:
sci-entific,clinical,orhealthcarepolicy.14Regardingtheirscope,
registriesmay includea certainspecific geographical area,
a country, a region or state, or even a particular
hospi-tal.Moreover,twoormoreregistriescanbegroupedinto a
consortium.
Specificallyinorthopedics,registriesofarthroplastic
pro-cedureswereinitiatedinScandinaviain1975(SwedishKnee
Arthroplasty Registry) and 1979(Swedish Hip Arthroplasty
Registry);asproduct/procedureregistries,thesehadquality
improvementand controlas mainobjectives,through
lon-gitudinal monitoring of outcomes and results, in order to
stimulate best practices in the selection, use, and
assess-mentofarthroplasticimplants.Surprisingly,duringthefirst
four years ofoperation,favorable resultswere observed in
the improvement of care and in the performance parity
among different institutions. From an initial situation in
which 25% of the participating Swedish institutions
per-formedbelow the nationalaverage, this rate fell to13%.15
Therevisionratedecreasedbyapproximately50%overtime,
a decline from 6.5% to 4.2% at seven years of follow-up,
from 14.5% to 9% at ten years, and from 24% to 16% at
26years,which wasassociatedwitha drasticreductionin
thenumber ofdifferent implantsavailable forusein
Swe-den.Moreover,thefinancialimpactofa5%reductioninthe
revisionratewasassociatedwithsavingsofUS$14million
annually.
Nationalimplantregistriesarebasedonsomeprinciples,
whosepurpose istoensure the validity,quality, and
com-pletenessoftheinformationcollected.Themainprinciples
are:(a)collectinginformationfromeveryarthroplastyunder
thescopeoftheregistry,soastoberepresentativeofall
pro-cedures,not just asample ofthe population, which could
cause bias and hinder the interpretation of results; (b) as
aconsequenceofthisfact, andalsotoencouragethe
inte-gralityoftherequestedinformation,theformsforcollecting
and storing the information should be very succinct and
contain only essential and validated information; (c) as a
permanentimplant registry,theoutcome shouldbeclearly
defined as any surgical revision procedure in which part
orall ofthe components are removed or replaced;and (d)
the feedback obtained through the registries should reach
physicians, institutions, and the publichealthcare system,
inorderto stimulatequalityimprovementthrough actions
indicated and guided by continuous monitoring. This
pro-cessstimulatesaleadingroleofmedicalspecialtysocieties
indataselection,collection,storage,interpretation,and
dis-semination;italsostimulatestheparticipationofthepublic
healthsystem,anotheragentthatisveryinterestedinquality
improvementandthereforeexpectedtoprovidesupportfor
accesstosecondary informationand partialfunding ofthe
project.15
Theidea,principles,and conceptsofNRAssoon spread
throughout Scandinavia, reinforcing its importance in the
continuousmonitoringofimplants.Injust2.5yearsof
follow-up,theNorwegianregistrydetectedthelowperformanceof
a particularbone cement formulation introduced in
surgi-calpractice;therefore,thisformulationwaswithdrawnfrom
themarketthefollowingyear,16whichfurtherstimulatedthe
implementationofnewregistriesinEurope,NewZealand,and
Australia.
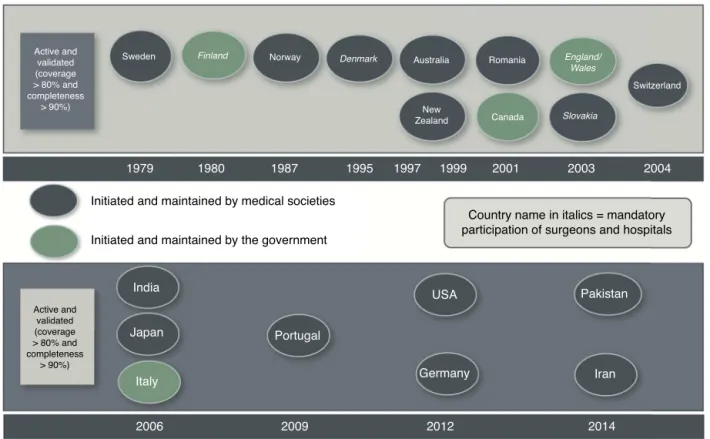
In 2004, the International Society of Arthroplasty
Reg-istries(ISAR)wascreated,andmanyregistrieswereinitiated,
withsomedifferencesininitiative,maintenance,andfunding
(Fig.2).
Subsequently, alerts issued by registries that detected
the inferior performance of some implant models for hip
resurfacing, and especially the increase in complications
relatedtothemetal-on-metalsurface,highlightedthe
impor-tance ofregistriesinthe detectionofinferiorperformance,
as well as in the comparison of performance between
implants.17–19
AlthoughtheimportanceoftheNARsasaninstrumentto
controlandimprovethequalityofcareinpatients
undergo-ingPJRsurgeryiswelldocumented,somecriticismsregarding
theinferencesarisingfromthemodelandthemethodology
usedindatacollection,analysis,andinterpretationhavebeen
recentlyreportedinthe literature.20,21 Inthe following
sec-tions,thesecriticismswillbeanalyzed,basedonnumerous
concepts,principles,andevidence.
Datacoverageandcompleteness,andtheirconsequences
InorderforNARstoberepresentativeofanentiregeographic
area,ratherthansimplyasampleofthepatientpopulation,
aminimum of80%ofthehospitalsinthe geographic area
surveyed (coverage)and a minimum of90% ofthe
arthro-plastiesconductedineachinstitution(completeness)mustbe
included.22,23
Inthisscenario,itisnecessarytorequestbriefinformation,
inordertofacilitatecollectionandencouragetheadherence
ofphysiciansandhospitalstotheregistry.
However,limitedinformationpotentiatesOESs’limitations
in establishinga causal linkwithimplant failure. In these
situations, NARsareinadequate fordeterminingfailure causes;
theyonlyindicatetrendsthatwilllaterbeevaluatedby
stud-ies ofbetter scientificquality.24 Asdetermining the causal
relationship isnotthe mainfocus ofthe registries, caution
in datainterpretationisrequired,onceNARsmerelyindicate trends.
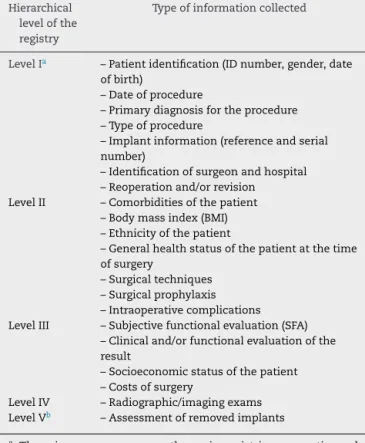
Indeed,manyregistriesarecurrentlyrequestingincreasing
information,whichhasledtoaclassificationofregistriesat
differenthierarchicallevels(Table2).25–27Evenifthebroader
datacollectionappliesonlytoasmallergroupofpatients,it
mayhinderparticipants’adherencetotheregistries,aswellas
generatebiasesbyrepresentingonlyasampleofallregistered
patients.
Theuseofrevisionsurgeryasanoutcomemarkerfor implantfailuresisnotadequate
Although revision surgery is a seemingly quite objective
outcome in its determination, its relation to implant
Active and validated (coverage > 80% and completeness
> 90%)
Active and validated (coverage > 80% and completeness
> 90%)
Initiated and maintained by medical societies
Country name in italics = mandatory participation of surgeons and hospitals Initiated and maintained by the government
India
Japan
Italy
Portugal
USA
Germany Iran
Pakistan
Sweden
1979
2006 2009 2012 2014
1980 1987 1995 1997 1999 2001 2003 2004
Norway Denmark Australia Romania
Switzerland
Canada Slovakia England/
Wales
New Zealand
Finland
Fig.2–Diagramshowingthebeginningandtypeofactivityofsomeregistries,accordingtoresponsibleorganizationsand voluntaryormandatoryparticipation.Noticethewideprevalenceofregistriescreated,managedandmaintainedbymedical societiesinitiative.Cooperationbetweenmedicalsocietiesandgovernmentagenciesisthemostfrequentstructure.
may be influenced by a number of factors, such as the
willingnessofthesurgeontoperformrevisionsurgery,due
to procedure complexity; clinical conditions and patient’s
willingness toundergo revision surgery; availability of the
revision procedure in the healthcare system; and implant
replacement(revision)biasinproceduresnotdirectlyrelated
to implant failure, but to the original surgical technique
itself.
Performancecomparisonbetweenimplantshasnotbeen
validated
Theperformanceofprostheticimplantsisafunctionnotonly
ofthe characteristics ofthe implant perse, but it can also
beinfluencedbythecriteriaforindicationoftheprocedure
andbythesurgicaltechnique;andtheseparametersarenot
assessedordetectedbytheregistries.Atypicalexampleofthis
limitationcanbeobservedwhencomparingdifferentmodels
ofkneearthroplasty.In2009,whentheSwedishregistry
indi-catedaparticularimplantashavingtheworstperformance,
thesamemodelhad hadthebest performanceintheNew
Zealanderregistry.
NARmaintenanceandfunding
Important factors of NARs success include: the definition
of the type of information, interpretation of results, and
production of annual reports (feedback) to physicians and
institutions.Forthisreason,mostoftheregistriescurrently
in operation (Fig. 2) are maintained by medical specialty
societies.15,28 Albeitcontroversial,anotheraspecttobe
con-sidered inincreasingadherence to NARsisthe mandatory
participationofphysiciansandinstitutions.Sinceitscreation,
theSwedishregistry(non-governmentaladministration),does
notincludecompulsoryparticipationofphysiciansand
insti-tutions. Thefirst NARtoadvocate andinstitutemandatory
participationwastheFinnishregistryin1980,whichwasalso
thefirstregistrywithgovernmentalinitiative,maintenance,
andfunding.
The low performance of this Finnish registry
culmi-natedintherecently-establishedpartnershipswithmedical
societies.15
In Brazil, the project for anarthroplasty registry is
fol-lowing an inverse path. Initiated in 2006 by the Brazilian
SocietyofOrthopedicandTraumaSurgery,thepilotproject
wasinterruptedin2010duetofinancialreasons;currently,a
partnershiphasbeenestablishedwiththeNationalAgencyof
SanitaryVigilance(AgênciaNacionaldeVigilânciaSanitária
[ANVISA]).
Although registries should be an integral part of the
nationalhealthsystem,theirgreatpotentialforcontroland
improvementofthequalityofcareiscloselylinkedtothe
med-icalpracticeindatachoice,collection,storage,interpretation,
Table2–Classificationofarthroplastyregistriesin hierarchicallevels,accordingtothetypeofinformation collected.
Hierarchical levelofthe registry
Typeofinformationcollected
LevelIa –Patientidentification(IDnumber,gender,date
ofbirth)
–Dateofprocedure
–Primarydiagnosisfortheprocedure –Typeofprocedure
–Implantinformation(referenceandserial number)
–Identificationofsurgeonandhospital –Reoperationand/orrevision
LevelII –Comorbiditiesofthepatient –Bodymassindex(BMI) –Ethnicityofthepatient
–Generalhealthstatusofthepatientatthetime ofsurgery
–Surgicaltechniques –Surgicalprophylaxis –Intraoperativecomplications LevelIII –Subjectivefunctionalevaluation(SFA)
–Clinicaland/orfunctionalevaluationofthe result
–Socioeconomicstatusofthepatient –Costsofsurgery
LevelIV –Radiographic/imagingexams
LevelVb –Assessmentofremovedimplants
a Thereisconsensusamongthemainregistries,consortia,and
international companies only regarding theinformation that characterizes level I, while much controversy still persists regardingtheotherlevels.25,26
b Morerecently,someauthorshaveproposedtheinclusionoflevel
V,whichrecommendstheevaluationofremovedimplants.27
andinstitutionaltrainingstrategies.Thesearesufficientand
absolutely essential arguments forstimulating the leading
roleofmedicalsocietiesintheinterpretationand
dissemina-tionofresults.15,28Partnershipswiththegovernment,which
isgreatlyinterestedinqualitycontrol,aremainlyrelatedto
funding;theyare alsojustifiedduetotheprovisionof
sec-ondaryinformation,requiredtoreducethelosstofollow-up
ofregisteredpatients.
On
the
need
for
Multicentric
Arthroplasty
Registries:
Rempro-SBQ
In2010,theBrazilianHipSurgerySociety(SociedadeBrasileira
deQuadril[SBQ])decidedtoincludeinitsstatutory
determina-tionsaprojectcalledtheMulticenterRegistryofSurgical
Pro-cedures(RegistroMulticêntricodeProcedimentosOperatórios
[Rempro-SBQ]).Inthefollowingyear,thefoundationsofthe
projectwerediscussed,basedonthepreviouslymentioned
mainlimitationsonthecollection,storage,andinterpretation
ofdata from national registries. Thus, an implementation
program29 wasdeveloped,basedon theproposition of
cre-atingamulti-centerregistry withinstitutionalmaintenance
and funding through the voluntary cooperation of SBQ
membersandtheirhospitalswherehipsurgeryservicesare
provided.
Thisinitiativeisjustifiedbytheneedforgreater
compre-hensiveness,validity,andconfidentialityoftheinformation
collected, aswell as theestablishment ofoutcome criteria
thataremorespecificallylinkedtothecausesoffailureofthe
prostheticimplantandofthesurgicalprocedureitself.Forthis
purpose,subjectivefunctionalandimagingevaluationcriteria
arealsoused.
Implantfailuresaredefinedthroughwell-established
crite-riathathavebeenpreviouslydescribedintheliterature;they
areevaluatedbyanadjudicationcommittee,alsocomposed
bymembersoftheSBQ.
Themulticenterregistry
Rempro-SBQaimstomonitorandimprovethequalityofcare
bycollectinginformationabouthipsurgeryprocedures
per-formed in 53 hospital institutions, called research centers
(centrosdepesquisa[CPs]),distributedthroughoutthe
coun-tryandrecognizedbytheSBQascentersoftrainingforhip
surgeons.Theseinstitutionshaveatleasttwosurgeons
asso-ciatedtotheSBQ,aswellasonehipsurgeoninchargeofthe
service.
AspartoftheRempro-SBQregistrationprocess,whichhas
been inprogress since April 2016, the institutions provide
detailed information on human, physical, and operational
resources, aswell asoninstalledcapacity, equipment,and
support services, so thatthe institution’s level of carecan
beclassified.Allsurgeons whopracticehip surgeryinCPs,
whetherornottheyareassociatedwiththeSBQ,areregistered
individually. Once the CP is registered, a term of
commit-mentwithRempro-SBQissignedbytheheadoftheservice,a
medicalcoordinator,andanadministrativecoordinator(and,
optionally,bythelegalrepresentativeoftheinstitution);the
term lists the rights and duties ofthis partnership. Thus,
Rempro-SBQaimstorecordall hipsurgicalprocedures
per-formedintheCPs,withaminimumvoluntaryparticipationof
80%ofCPs.
Thecriteriaforvalidationofcoverage andcompleteness
are met through monthly reports preparedby the
institu-tion,inwhichallthespecificproceduresperformedattheCP
arelisted;thesereportsalsoincludesecondaryinformation,
providedbythepublicagenciesresponsibleforthespecific
indicators. Therate oflosstofollow-up isalsodetermined
through primary information collected from the
Rempro-SBQ electronic database, as well as secondary indicators
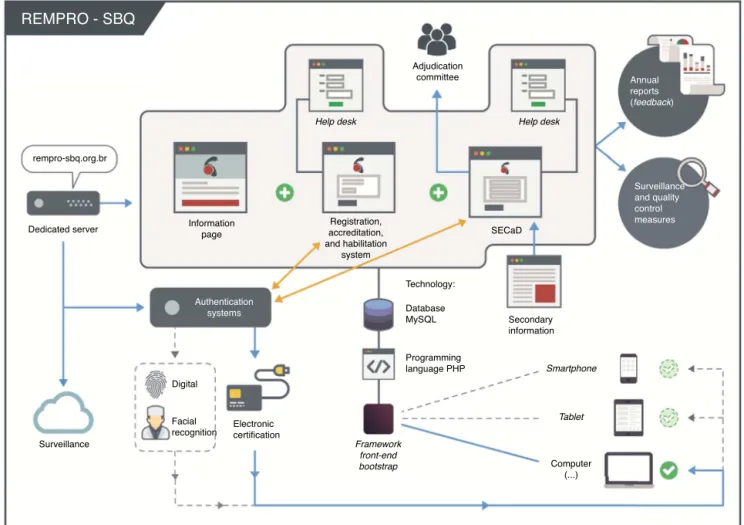
(Fig.3).
Inthislight,Rempro-SBQisaconsortiumofinstitutional
registries, in which information, standardized for all CPs,
is centralized in a single electronic database. The 53 CPs
are distributedinthe Southeast(35), South(nine),Midwest
(five)andNortheast(four)regions;theSouthandSoutheast
regions,whichrepresent83%ofCPs,accountedfor80%ofthe
primary totalhiparthroplastiesperformed bytheBrazilian
PublicHealthSystembetweenJanuary2015andJanuary2016,
REMPRO - SBQ
rempro-sbq.org.br
Dedicated server Informationpage
Adjudication committee
SECaD Registration,
accreditation, and habilitation
system
Authentication systems
Surveillance
Digital
Facial
recognition Electroniccertification
Technology:
Database MySQL
Programming language PHP
Secondary information
Surveillance and quality control measures Annual reports (feedback)
Computer (...)
Tablet Smartphone
Framework front-end bootstrap
Help desk Help desk
Fig.3–SchematicdrawingpresentingtheorganizationalandoperationalstructureofRempro-SBQ.Theauthentication systemisintransitiontoalsoacceptdigitalandfacialrecognition.Seetextfordetailedexplanations.
Comprehensiveness,qualityofinformation,and
hierarchicallevelofRempro-SBQ
KonanandHaddad21emphasizethattheobservational
infor-mation obtained from the NARs is only one facet of the
informationthatmustbeofferedtoorthopedicsurgeons,and
it certainly has lower scientific quality than well-planned
prospective multi-center studies. Thus, there is a
consen-susthatinformationfrom NARs onlyindicates trendsthat
shouldbefurtherinvestigatedthroughstudiesofbetter
sci-entificquality, sothat thecause-effect relationshipcriteria
canbeevaluated.21,24Thesefactswereagreatstimulustothe
progressiveinclusionofmoredetailedinformationonsome
NARs,whichresultedintheestablishmentofregistriesof
dif-ferenthierarchicallevels,aspreviouslymentioned(Table2).
However, dueto a possible reductionin the adherence by
physiciansandinstitutions,theregistrieshavechosento
col-lectmorespecificinformationonlyinasampleoftheirtotal
population, which in itself can be a source of systematic
bias.
In turn,given the partnership ofRempro-SBQ and CPs,
which are already institutionally linked to the SBQ, this
registryhasauniqueopportunitytopromotethecollection
ofmorecomprehensiveinformationwithoutcompromising
the adherence ofhospitalsdedicated tothetraining ofhip
surgeons.Thus,detailedpre-operativeinformationon
demo-graphics, comorbidities,medications inuse,riskfactorsfor
complications, subjectiveand objective functional capacity,
physical examination, and laboratory and imaging exams
arecollectedinastandardizedway.Likewise,informationon
thetechniquesandcircumstancesofthesurgicalprocedure,
detailsoftheimplantused,andcomplicationsarethoroughly
explored.Moreover,postoperativefollow-up, complications,
and outcomes are also monitored through detailed
infor-mation collected by the CPs. All information is collected
prospectively,guidedbyaresearcher’smanual.
ThisinformationranksRempro-SBQinthe highest
hier-archical level of registries, considering the most current
classifications.25,26Thelargevolumeofinformationobtained
may allow not only the detection of risk factors hitherto
unknown, but also to establish some cause-effect
rela-tionships to the outcome, using more refined statistical
methodologyandassessmentsbytheadjudication
Collectionandconfidentialityofinformation
TheElectronicDataCollectionSystem(SistemaEletrônicode
Capturade Dados [SECaD]) was developedby Rempro-SBQ
withthespecificobjectiveofbeinganagiletool,easytouse
by CPs, not only in responsive data collection but also in
storage,asanelectronicdatabaseinadedicatedserverthat
is dynamic and able to perform tasks automatically, from
basiccalculationstotheresultsofmorecomplexfunctional
scores.
Patientdata canonlybe includedinto the system after
theinformedconsentissignedbythepatientorhis/herlegal
representative.
The entire process of collection, storage, and access
to information follows the guidelines of the Brazilian
SocietyofHealthcareInformationTechnology/Federal
Coun-cil of Medicine (Sociedade Brasileira de Informática em
Saúde/ConselhoFederaldeMedicina[SBIS/CFM])31regulating
thesupplyofelectronicmedicalrecords.Theauthors
empha-sizethataccesstoSECaDisonlypossiblethroughelectronic
authentication of the medical and administrative
coordi-natorsofeachCP,whoonlyhaveaccesstotheinformationon
patientsfromthatsameCP.Broaderaccesstopatient
informa-tionislimitedtotheadjudicationcommittee,subordinateto
theExecutiveBoardofRempro-SBQ.Eventhiscommitteehas
torequestdataaccessforspecificactions,aspartofitsrole
ofmonitoringandpreparingtheannualreports.Withdigital
certification,Rempro-SBQisalsointheprocessofoffering
bio-metricrecognition,inordertoallowdatainputfromportable
electronicdevices in real time,directly from the operating
room.Alternatively, specificformscan beprintedfor
man-ualcompletionand subsequentuploadtotheSECaD;these
formsmayalsobeanintegralpartofthepatient’sphysical
record(Fig.3).
Outcomedefinitionsandtheirimplications
Thelimitation of NARs in the assessmentof performance
andcomparisonbetweenimplants,aswellasinthe
interpre-tationoftheinformationcollected,isadirectconsequence
ofthelimitationcausedbythechoiceofrevisionsurgeryas
anoutcomeandbytheevaluationofrestrictedinformation,
whicharethepillarsofNARsthemselves,asdiscussedinthis
article.
However, if revision surgery with implant replacement
is considered as the only outcome, technical failures or
adverse events ofthe procedure willbegrouped with
fail-ures directly related tothe product (implant) in the same
scenario.This isa major biasin the determination ofthe
safety and efficacy of a product, as well as in the
com-parison between different implants. Moreover, it hinders
thedeterminationofthe truecausal factorsofarthroplasty
failure.
Thus, Rempro-SBQ, considering that different outcome
evaluations are required for these various circumstances,
hasrecognizedtwocategories:procedurerevisions(or
reop-erations), which characterize the procedure endpoint; and
functional revisions of implants, which characterize the
functional endpoint of the implant. Any other partial or
completereplacementoftheprostheticimplantisconsidered
as a structuralrevision of the implant; the corresponding
endpoint situation is termed the structural implant
end-point. This differentiation also implies the acceptance of
the fact that these distinct conditions require different
actions. In the case of functional endpoints, the
imple-mentation of continuing education programs is strongly
recommended; in turn, in endpoints caused by implant
failures (structural implant revision), ifthey are frequently
observed in a specific model, more rigorous monitoring is
required.
Basedon theseconsiderations,Rempro-SBQhaschosen
tocreate mechanismsto diagnosefailure ofthe procedure
and/oroftheprostheticimplantitself,evenbeforetherevision
surgeryisperformed.Thesemechanismsusesubjective
func-tionalevaluations,degreeofpatientsatisfaction,andimaging
examsevaluatedbyanadjudicationcommittee,whichallows
differentiating the functional procedure endpoint from the
structuralimplantendpoint.
Maintenanceandfunding
Sincethemainpurposeofregistriesofproceduresand
prod-ucts is to control and improve the quality of care, their
success is based on data choice, collection, and
interpre-tation, performed at sequential and defined times. That
implies participation and the leading role of medical
soci-eties in the perpetuation of these actions. Furthermore,
the feedback ofinformation (presented asannual reports),
an important tool of the registries, requires the
analy-sis and interpretation of the findings, which can only be
done by specialists in the area. Moreover, actions to
con-trol and improve quality can also only be implemented
through medical societies.These are sufficient reasons for
the centralizationofregistrymaintenanceinmedical
insti-tutions.
Regarding funding,whichwas thereasonforthe failure
ofsome registries, Rempro-SBQwasstructured inorder to
exploit its partnershipwithCPs, using theinstalled
capac-ity of the centers that train hip surgeons. This measure
by itself results in adrastic reduction ofthe costs of
reg-istry maintenance, which can then be borne by the SBQ.
However,thegreatrelevanceoftheinformationandactions
promoted bythe registry hasarousedthe interest ofother
medicalsocietiesandseveralpublicentitiesfromthenational
healthcaresystem,aswellasprostheticimplantcompanies.
Thus, some information can be shared through
fund-ing partnerships, preservingthe confidentiality ofpatients,
physicians, and institutions, without violating any ethical
precepts.
Conclusions
NARsareimportanttoolsformonitoringpatientsundergoing
prostheticjointreplacements.Theirmainlimitationsmaybe
overcomeinacomplementarywaybybetterscientificquality
Rempro-SBQ, which incorporates into its organizational
andfunctionalstructurethetrainingcentersforhipsurgery
(institutionally linked with the SBQ), allows the
simulta-neousandreliablecollectionofmorespecificinformationof
highhierarchicallevel,withasignificantreductionin
main-tenance and funding costs. Quality improvement actions,
supported by the SBQ, have created a scenario of higher
effectiveness and adherence to data collection, storage,
interpretation, and dissemination procedures. The
begin-ningoftheactual activitiesofprocedure registries,already
underway through a pilot project, will be important for
theconsolidationofthepreceptsandfundamentals hereby
presented.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. JonesCA,BeaupreLA,JohnstonDW,Suarez-AlmazorME. Totaljointarthroplasties:currentconceptsofpatient outcomesaftersurgery.RheumDisClinNorthAm. 2007;33(1):71–86.
2. AnakweRE,JenkinsPJ,MoranM.Predictingdissatisfaction aftertotalhiparthroplasty:astudyof850patients.J Arthroplasty.2011;26(2):209–13.
3. GomesLSM,RigolJP.Mecanismosdefalhasassépticasdos implantesartroplásticosdequadril.In:GomesLSM,editor.O quadril.SãoPaulo:Atheneu;2010.
p.589–624.
4. SudmannE,HavelinLI,LundeOD,RaitM.TheCharnley versustheChristiansentotalhiparthroplasty.A comparativeclinicalstudy.ActaOrthopScand. 1983;54(4):545–52.
5. EspehaugB,HavelinLI,EngesæterLB,VollsetSE,Langeland N.Earlyrevisionamong12,179hipprostheses.Acomparison of10differentprosthesisbrandsreportedtotheNorwegian ArthroplastyRegister,1987–1993.ActaOrthopScand. 1995;66(6):487–93.
6. HavelinLI.HiparthroplastyinNorway1987–1994.The NorwegianArthroplastyRegister.Bergen:Universityof Bergen;1995.Thesis.
7. LabekG,NeumannD,AgreiterM,SchuhR,BöhlerN.Impact ofimplantdevelopersonpublishedoutcomeand
reproducibilityofcohort-basedclinicalstudiesin
arthroplasty.JBoneJointSurgAm.2011;93Suppl.3E:55–61.
8. ChalmersTC,CelanoP,SacksHS,SmithHJr.Biasin treatmentassignmentincontrolledclinicaltrials.NEnglJ Med.1983;309(22):1358–61.
9. SacksH,ChalmersTC,SmithHJr.Randomizedversus historicalcontrolsforclinicaltrials.AmJMed. 1982;72(2):233–40.
10.ColditzGA,MillerJN,MostellerF.Howstudydesignaffects outcomesincomparisonsoftherapy.I:Medical.StatMed. 1989;8(4):441–54.
11.SackettDL,RichardsonWS,RosenbergW,HaynesRB. Evidencebasedmedicine:howtopracticeandteachEBM. NewYork:ChurchillLivingstone;1997.
12.BensonK,HartzAJ.Acomparisonofobservationalstudies andrandomizedcontrolledtrials.NEnglJMed.
2000;342(25):1878–86.
13.WeddellJM.Registersandregistries:areview.IntJEpidemiol. 1973;2(3):221–8.
14.GliklichRE,DreyerNA,editors.RegistriesforEvaluating
PatientOutcomes:user’sguide.2nded.RockvilleMD:Agency
forHealthcareResearchandQuality;2010[accessedin
17/07/2015].Availablein:http://www.ncbi.
nlm.nih.gov/books/NBK49444/#ncbidlgcitbxNBK49444. 15.LabekG,JandaW,AgreiterM,SchuhR,BöhlerN.
Organisation,dataevaluation,interpretation,andeffect ofarthroplastyregisterdataontheoutcomeintermsof revisionrateintotalhiparthroplasty.IntOrthop. 2011;35(2):157–63.
16.HavelinLI,EspehaugB,VollsetSE,EngesaeterLB.The effectofthetypeofcementonearlyrevisionofCharnley totalhipprostheses:areviewofeightthousandfive hundredandseventy-nineprimaryarthroplastiesfrom theNorwegianarthroplastyregister.JBoneJointSurgAm. 1995;77(10):1543–50.
17.NationalJointRegistryEnglandandWalesAnnualReport
[BancodedadosInternet].2008[accessedin15/07/2015].
Availablein:http://www.njrcentre.org.uk/njrcentre/
Portals/0/Documents/England/Reports/5th%20Annual. pdf.
18.AustralianOrthopaedicAssociationNationalJoint
ReplacementRegistryAnnualReport[Bancodedados
internet]2008[accessedin12/07/2016].Availablein:
https://aoanjrr.sahmri.com/documents/10180/42662/ Annual%20Report%202008?version=1.1&t=1349406277970.
19.MHRA(2010)MedicalDeviceAlert:MDA/2010/069,DePuyASR
hipreplacementimplants.MedicinesandHealthcare
ProductsRegulatoryAgency,London[accessedin
12/01/2012].Availablein:
http://www.mhra.gov.uk/Publications/
Safetywarnings/MedicalDeviceAlerts/CON093789. 20.GoodfellowJW,O’ConnorJJ,MurrayDW.Acritiqueof
revisionrateasanoutcomemeasure.Re-Interpretationof KneeJointRegistryData.JBoneJointSurgBr.
2010;92(12):1628–31.
21.KonanS,HaddadFS.Jointregistries.Aptolemaicmodelof datainterpretation?BoneJointJ.2013;95-B:1585–6.
22.EuropeanArthroplastyRegister.Qualityofdatatsetsfor
outcomemeasurement[accessedin12/07/2015].Availablein:
http://www.ear.efort.org/downloads/EBOOKQualityof Datasetsfinal.pdf.
23.InternationalSocietyofArthroplastyRegistries.Bylaws.2013
[accessedin18/03/2015].Availablein:
http://www.isarhome.
org/Bylaws%20ISAR%202013-rev.pdf?attredirects=0. 24.GravesSE.Thevalueofarthroplastyregistrydata.Acta
Orthop.2010;81(1):8–9.
25.RobertssonO.Kneearthroplastyregisters.JBoneJointSurg Br.2007;89(1):1–4.
26.CallananMC,JarrettB,BragdonCR,ZurakowskiD,RubashHE, FreibergAA,etal.TheJohnCharnleyAward:riskfactorsfor cupmalpositioning:qualityimprovementthroughajoint registryatatertiaryhospital.ClinOrthopRelatRes. 2011;469(2):319–29.
27.HansenVJ,GreeneME,BragdonMA,NebergallAK,BarrCJ, HuddlestonJI,etal.Registriescollectinglevel-IthroughIV data:institutionalandmulticenteruseAAOSexhibit selection.JBoneJointSurgAm.2014;96:e160.
28.KollingC,SimmenBR,LabekG,GoldhahnJ.Keyfactorsfora successfulNationalArthroplastyRegister.JBoneJointSurg Br.2007;89(12):1567–73.
29.Rempro-SBQ.Estrutura,organizac¸ãoeimplantac¸ão.
(informac¸õesnainternet)[accessedin20/10/2016].Available
30.Brasil.MinistériodaSaúde.Datasus-Informac¸õesdesaúde.
(informac¸õesnainternet)[accessedin20/11/2016].Available
in:http://tabnet.datasus.gov.br/cgi/tabcgi.exe? sih/cnv/qiuf.def.
31.SociedadeBrasileiradeInformáticaemSaúde/Conselho
FederaldeMedicina.ManualdeCertificac¸ãoparaSistemasde
RegistrosEletrônicosemSaúde.(Informac¸õesnainternet)
[accessedin12/08/2016].Availablein: