SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Social
profile
and
cost
analysis
of
deep
infection
following
total
hip
replacement
surgery
Vera
Lucia
Frazão
a,
Helder
de
Souza
Miyahara
a,
Ricardo
Akihiro
Kirihara
a,
Ana
Lucia
Lei
Munhoz
Lima
b,
Alberto
Tesconi
Croci
b,
José
Ricardo
Negreiros
Vicente
a,∗ aInstitutodeOrtopediaeTraumatologia,FaculdadedeMedicina,UniversidadedeSãoPaulo,SãoPaulo,SP,BrazilbDepartamentodeOrtopediaeTraumatologia,FaculdadedeMedicina,UniversidadedeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received30August2016 Accepted4October2016 Availableonline23October2017
Keywords: Hiparthroplasty Infection Costanalysis
a
b
s
t
r
a
c
t
Objective:Tocharacterizethesocio-economicanddemographicprofileofpatients under-goingsurgeryforrevisiontotalhiparthroplastyregardingthediagnosisofdeepprosthetic infection.
Methods:Twentypatientswereretrospectivelystudied,admittedintheperiodbetween2009 and2010bytheHipSurgeryGroupwiththediagnosisofdeepprostheticinfection,whose proposedtreatmentwassurgical.Thisstudywascarriedoutinthepresenceofthepatient bycompletingtwoformsappliedbythesocialworkeroftheGroup.
Results:Ina20-patientsample,40%weremale,45%wereworkingage,50%ofpatients orig-inatedfromthecapital,85%dependedonbenefits,70%wereretired,60%ofpatientswere fromthishospital,and40%werefromotherservices.Theaveragecostofpatientstothe publicsystemwasR$55,821.62perpatientandthetotalspentontreatmentofpatientsin thestudyexceededonemillionBrazilianreals,totallingR$1,116,432.40.
Conclusion:Infectionfromtotalhiparthroplastygeneratesamajorexpensetothesocial securitysystemandtothepublichealthcaresystem.Physiciansmustalwaysbealerttothe possibleriskfactorsandperioperativecare,strivingtominimizethiscomplication.
©2017PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeOrtopedia eTraumatologia.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Perfil
social
e
análise
de
custo
da
infecc¸ão
pós-operatória
da
artroplastia
total
do
quadril
Palavras-chave: Artroplastiadequadril Infecc¸ão
Análisedecusto
r
e
s
u
m
o
Objetivo:Caracterizaroperfilsocioeconômicoe demográficodepacientessubmetidos à cirurgiade revisãodeartroplastiatotaldoquadrilpordiagnósticodeinfecc¸ãoprotética profunda.
∗ Correspondingauthor.
E-mail:[email protected](J.R.Vicente). http://dx.doi.org/10.1016/j.rboe.2017.10.003
Métodos: Análisede20pacientesinternadosentre2009e2010peloGrupodeQuadrilcom diagnósticodeinfecc¸ãoprotéticaprofundacujotratamentopropostofoicirúrgico.O tra-balhofoifeitocompreenchimentonapresenc¸adopacientededoisformuláriosaplicados pelaassistentesocialdogrupo.
Resultados:Naamostrade20pacientes,40%pertenciamaosexomasculino,45%estavamem idadeprodutiva,50%eramorigináriosdacapital,85%previdenciários,70%aposentados,60% provenientesdoprópriohospitale40%deoutrosservic¸os.Amédiadecustodospacientes aosistemapúblicofoideR$55.821,62porpaciente,ogastototalnotratamentodospacientes doestudototalizouR$1.116.432,40.
Conclusão: Conclui-sequeaartroplastiatotaldoquadrilinfectadageraumgrandegasto aosistemaprevidenciárioeaosistemadesaúdepúblico,deve-se,portanto,sempreatentar paraospossíveisfatoresderiscoecuidadosperioperatóriosparaqueesseproblemaseja evitado.
©2017PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileirade OrtopediaeTraumatologia.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Amongthepossiblecomplicationsoftotalhiparthroplasties, prostheticinfectionisoneofthemostdevastating,with seri-ousconsequencesforpatients,sincemostofthemwillrequire furthersurgicalinterventions;furthermore,theyare associ-atedwithhigh costs forthe paying sources.They are also associatedwithperiodsofworkleaves,alsooverburdeningthe socialsecuritysystem.
Anumber offactors are relatedtothe increasedriskof prostheticinfection,includingobesity,diabetes, immunosup-pression,previouslargehipsurgeries,smoking,malnutrition, prolonged corticoid therapy, and prolonged surgical time, amongothers.1,2
InBrazil,Law9.431/97hasmadehospitalinfection surveil-lance mandatory, in order to systematically reduce the prevalenceof this complication as a whole in the various medicalspecialties.3ThePanAmericanHealthOrganization coordinated the Study on the efficacy of nosocomial infection control, conducted in Atlanta (United States). That study concludedthat hospital stayincreases the duration ofthe infectionbyameanoffourdays,withanadditionalcostper patientof$1800onadmission.4
Thepresentstudyisaimedatestablishingthe socioeco-nomicanddemographicprofileofpatientswho underwent total hip arthroplasty revision at this medical service due to a diagnosis of deep prosthetic infection, and to identify the costs involved in the treatment of these patients.
Methods
Afterapproval by the Research Ethics Committee,a retro-spectivedescriptivestudywasconductedwithqualitativeand quantitativeanalysis.
Thestudyincludedpatientsadmittedbetween2009and 2010 by The Hip Group of a quaternary university hospi-tal,witha diagnosis ofdeep prosthetic infection inwhom the proposed treatment was surgical. Patients with infec-tionresultingfromtotalhiparthroplastyrevisionsurgeryand
thosewhorequiredintravenousantibiotictherapyas defini-tivetreatmentwithouttheneedforsurgicaltreatmentwere notincluded.Furthermore,patientswhodidnotagreetosign theinformedconsentformtoparticipateintheprojectwere alsoexcluded.
Thestudywascarriedoutbycompleting,inthepatient’s presence,twoformsappliedbythesocialworkerofthegroup, themainauthorofthisstudy.
Questionnaire1(Appendix)addressedthesocialandfamily dataofpatients,aswellasthoseinherenttotreatment.
Questionnaire2(Appendix)addressedthesocioeconomic issuesbasedontheBrazilEconomicClassification,acriterion adopted by the Brazilian Association of Research Compa-nies(Associac¸ãoBrasileiradeEmpresasdePesquisa[Abep]),5 whichassessesthepurchasingpowerofthepopulationand the degreeofeducation ofthehead ofthe family, stratify-ingthepopulationatthefollowinglevels:A1,A2,B1,B2,C1, C2, D, and E. Both forms were pre-tested infive patients, attempting to solve possible execution and reproducibility issues.
Thestudyincluded20patients,fromaninitialpopulation of24 patients, who met theinclusion criteria inthestudy period.Twopatientsdiedduetocausesunrelatedtothe ini-tialdiagnosis,onecontinuedtreatmentintheSupplementary HealthSystem,andonedidnotsigntheInformedConsent Form.
Results
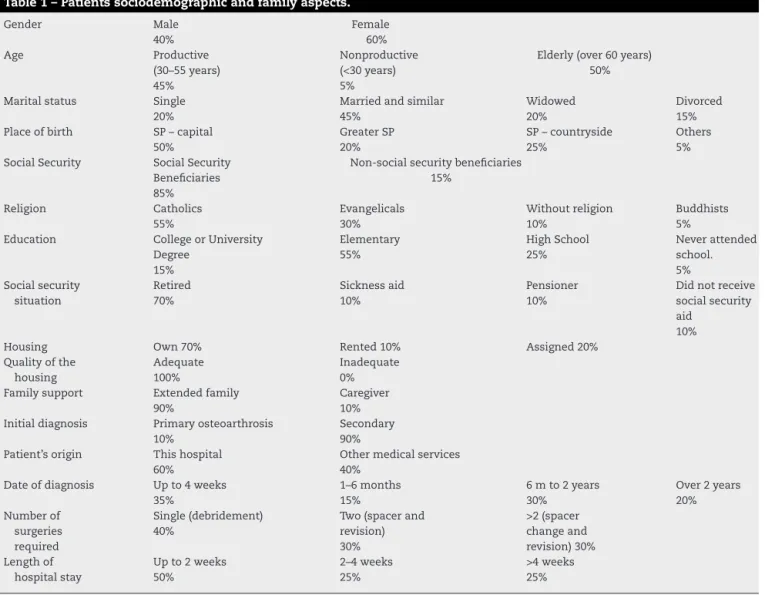
Patient’s sociodemographic and family data are shown in Table1.
Fig.1standsforpatientdistributionaccordingto socioeco-nomiclevel.
Themeannumberofdaysonantibiotictherapy,whether intravenousororal,was266days(30–376).
Table1–Patientssociodemographicandfamilyaspects. Gender Male 40% Female 60% Age Productive (30–55years) 45% Nonproductive (<30years) 5%
Elderly(over60years) 50%
Maritalstatus Single 20%
Marriedandsimilar 45%
Widowed 20%
Divorced 15% Placeofbirth SP–capital
50%
GreaterSP 20%
SP–countryside 25%
Others 5% SocialSecurity SocialSecurity
Beneficiaries 85%
Non-socialsecuritybeneficiaries 15% Religion Catholics 55% Evangelicals 30% Withoutreligion 10% Buddhists 5% Education CollegeorUniversity
Degree 15% Elementary 55% HighSchool 25% Neverattended school. 5% Socialsecurity situation Retired 70% Sicknessaid 10% Pensioner 10%
Didnotreceive socialsecurity aid
10%
Housing Own70% Rented10% Assigned20%
Qualityofthe housing
Adequate 100%
Inadequate 0% Familysupport Extendedfamily
90%
Caregiver 10% Initialdiagnosis Primaryosteoarthrosis
10%
Secondary 90% Patient’sorigin Thishospital
60%
Othermedicalservices 40%
Dateofdiagnosis Upto4weeks 35%
1–6months 15%
6mto2years 30%
Over2years 20% Numberof surgeries required Single(debridement) 40%
Two(spacerand revision) 30% >2(spacer changeand revision)30% Lengthof hospitalstay
Upto2weeks 50% 2–4weeks 25% >4weeks 25% 0 10 5 20 30 20 15 0 0 5 10 15 20 25 30 35 E D C2 C1 B2 B1 A2 A1
Socioeconomic level – relative distribution (%)
Fig.1–Patientdistributionaccordingtosocioeconomic level.
Discussion
Prostheticinfection isoneofthemostseriousof complica-tions,withsevereconsequencesforpatients,sinceitresults innewsurgicalinterventions,prolongedhospitalstays,and theneedforlong-termantibiotictherapy.6Moreover,revisions
ofinfectedarthroplastiesarecostlytohealthcareandsocial securitysystems.
The initial diagnosis of infected patients treated at the medical service, primary osteoarthrosis in 10% and osteoarthrosis secondary to another previous pathology in 90%,isprobablyduetotheprofileofpatientsreferredtothis referenceservice;itmightalsoduetotheagedistributionof theBrazilianpopulation,notablyyoungerthanthatofother countries, which justifiesahigher prevalenceofsecondary osteoarthrosis.
Ofthepatients,40%weremaleand60%female. Accord-ing to Bozig et al.,7 white women aged between 70 and 74yearswithcomorbiditiessuchasalcoholism,depression, cardiopulmonary disease, and peripheral vascular insuffi-ciency aremorepronetoperiprosthetic infection.However, accordingtoPoultsidesetal.,8comorbidity-associated infec-tion may also be observed male patients with the same probability.
Table2–Meancostofhospitalizationaccordingto region.
Presentstudy(BR) US$23,857
Europe US$40,485
UnitedStates US$11,494
UnitedKingdom US$36,728
cases,inwhichasimpledebridementsurgerymightsavethe originalimplantandcauselessharmtothepatient,in addi-tiontoalowersocialcost.Theauthorsthereforeemphasize theimportanceofinitialoutpatientfollow-upconsultations, whichshouldalwaysbeconductedunderthesupervisionofa physicianexperiencedinthematter.
InastudyoftheDepartmentofOrthopedicSurgery, Univer-sityofNorthCarolina(UnitedStates),Clementetal.9reported meancostsof$11,494inthetreatmentofpatientsreadmitted withadiagnosisofperiprostheticinfection.Vanheganetal.,10 inastudyperformedattheorthopedicdepartmentofthe Uni-versityofLondon,observedamean costof£21,937inthe treatmentofthiscomplication.Datafrom theUniversityof Rostock,Germany,inastudybyHaenleetal.,11showedamean costofD 29,331forthetreatmentofaninfectedarthroplasty vs.D 6265forprimaryarthroplasty.Otherstudiesalsoshow
thatthiscostisgreatlyincreasedwhentheetiologicalagent responsiblefortheinfectionisamultiresistant microorgan-ism;accordingtoFiliceetal.,thesecostscandoubleinthe caseofaninfectioncausedbyamultisensitivebacterium.12
Table2standsforthemean costofarthroplastiesinthe aforementionedplaces.
Despite the variations observed, due to tax differences (leading to different costs of medication and implants) as well as from the unequal healthcare systems, it is noted that eventhe lowest observedvalue wassignificant, espe-ciallywhen consideringthis data collectivelyin thewhole country.
In addition to expenses with hospital services and materials, it is important to emphasize the deficit in the social security system. In most cases, it is caused by disability retirement due to illness and the prolonged period of hospitalization. In the present study, 90% of the patients were insured by the social security system, of whom 45% were of working-age, which demonstrates the seriousconsequences ofarthroplasty infection forthis system.
Another serious socioeconomic problem found in this study was the origin of the patients: 40% were referred from other medical services, which may be associated with a lack of adequate distribution of hospitals capable of treating high complexity cases, that require adequate equipment for surgical procedures, experienced surgeons, hospital infrastructure, and drug availability. The problem ofthe centralizationofhighcomplexity servicesremains a challenge to be solved in Brazil, a country of continental dimensions.
Inthepresentstudy,thecausesorriskfactorsfor peripros-thetic infection were not studied, but a large part of the population was stratified into socioeconomic classes B2,
C1, and C2, according to the Abep Classification (2007).5 These social classes have lower purchasing power, which may berelatedtosomeofthe mainriskfactorsassociated with periprosthetic infections foundin other studies,such asmalnutrition,preoperativeanemia, andhydroelectrolytic disorders.13
Ofthepatientsincludedinthepresentstudy,15%hada collegeoruniversitydegree,55%elementaryschooldegree, 25%highschooldegree,and5%neverattendedschool,which identifiesthepatientsofthissampleashavinglowpurchasing powerandlowschooling,asindicatedbyOngetal.14intheir workonthecorrelationbetweenperiprostheticinfectionand thesocioeconomicstatusofpatients.
Conclusion
Infectedtotalhiparthroplastyisapostoperativecomplication thetreatmentofwhichgeneratesgreatexpensetothesocial securityandpublichealthcaresystems,becauseitfrequently involvesrelativelyyoungpatientsofworking-age.Therefore, inordertoavoidtheissue,thepossibleriskfactorsandthe quality of perioperative care should always be taken into account.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Appendix.
Questionnaire1–Patientssocialandfamilydata
•Identification:name,age,gender,religion,schooling,
maritalstatus,andplaceoforigin.
•Socialsecuritysituation:associationandsocial
securitybenefit.
•Housing:area,property,typeofhousing,numberof
rooms,numberofinhabitants,sanitation,selective garbagecollection,drinkingwater,andhealthcare serviceneartheresidence.Asatisfactoryhousing wasdefinedasonewithatleasttworooms,with sanitation,andgarbageandsewagecollection,as wellasaprivatebathroom,allofthesefactors concomitantwiththepresenceofanaccessible healthcareserviceneartheresidence.
•Familysupport:familydynamicsduringtreatment
andhomecare.Theconceptofanextendedfamily denotesaunitbeyondparentsandchildrenformed bycloserelativeswithaffectivetiesandabletogive supporttothepatient.
•Hospitalization:initialdiagnosis,date,numberof
Questionnaire2–Socioeconomiclevel (questionnaireto obtaintheBrazilianEconomicClassificationdata–newAbep –2008).
Ownershipofcertainitems
Items Does
not own
1 2 3 4
ColorTVs 0 1 2 3 4
VCR/DVD player
0 2 2 2 2
Radios 0 1 2 3 4
Bathrooms 0 4 5 6 7
Vehicles 0 4 7 9 9
Monthly-paid housemaids
0 3 4 4 4
Washing machine
0 2 2 2 2
Refrigerator 0 4 4 4 4
Freezera 0 2 2 2 2
a Independentapplianceora2nddoorontherefrigerator.
Levelofschoolingofheadofthehousehold
Oldnomenclature Points Current
nomenclature
Illiterate/incomplete elementaryschool
0 Illiterate/upto3rd yearofelementary school
Complete
elementaryschool
01 4thgradeelementary school
Completehigh school
02 Complete
elementaryschool Completehigh
school
04 Completehigh
school CollegeorUniversity
Degree
08 CollegeorUniversity Degree
Classes Score
A1 42to46points
A2 35to41points
B1 29to34points
B2 23to28points
C1 18to22points
C2 14to17points
D 8to13points
E 0to7points
Minimumscore:0 Maximumscore:46
r
e
f
e
r
e
n
c
e
s
1.DermanPB,GrahamDS,SpeckRM,FlynnDN,LevinLS, FleisherLA.Riskfactors,causes,andtheeconomic implicationsofunplannedreadmissionsfollowingtotalhip arthroplast.JArthroplasty.2013;288Suppl.:7–10.
2.BozicKJ,LauE,KurtzS,OngK,RubashH,VailTP,etal.Patient relatedriskfactorsforperiprostheticjointinfectionand postoperativemortalityfollowingtotalhiparthroplastyin Medicarepatients.JBoneJtSurgAm.2012;94(9):794–800. 3.Brasil.Lein◦9.431,de6dejaneirode1997.Dispõesobrea
obrigatoriedadedamanutenc¸ãodeprogramadecontrolede infecc¸õeshospitalarespeloshospitaisdoPaís.Brasília [Internet].
DiárioOficial[da]RepúblicaFederativadoBrasil.Availabefrom: ahref=http://www.lexml.gov.br/urn/urn:lex:br:federal:lei:1997-01-06;9431[accessed
20.08.16].
4.HaleyRW,QuadeD,FreemanHE,BennetJV.Studyonthe efficacyofnosocomialinfectioncontrol.AmJEpidemiol. 1980;111(5):472–85.
5.Associac¸ãoBrasileiradeEmpresasdePesquisa.Critériode classificac¸ãoeconômicaBrasil2008.SãoPaulo:Associac¸ão BrasileiradeEmpresasdePesquisa;2008.Availabefrom: www.abep.org.DadoscombasenoLevantamento Socioeconômico,2005.
6.KloucheS,SarialiE,MamoudyP.Totalhiparthroplasty revisionduetoinfection:acostanalysisapproach.Orthop TraumatolSurgRes.2010;96(2):124–32.
7.BozicKJ,OngK,LauE,BerryDJ,VailTP,KurtzSM,etal. EstimatingriskinMedicarepatientswithTHA:anelectronic riskcalculatorforperiprostheticjointinfectionandmortality. ClinOrthopRelatRes.2013;471(2):574–83.
8.PoultsidesLA,MaY,DellaValleAG,ChiuYL,SculcoTP.In hospitalsurgicalsiteinfectionsafterprimaryhipandknee arthroplasty–incidenceandriskfactors.JArthroplasty. 2013;28(3):385–9.
9.ClementRC,DermanPB,GrahamDS,SpeckRM,FlynnDN, LevinLS,etal.Riskfactors,causes,andtheeconomic implicationsofunplannedreadmissionsfollowingtotalhip arthroplasty.JArthroplasty.2013;288Suppl.:7–10.
10.VanheganIS,MalikAK,JayakumarP,UIIslamS,HaddadFS.A financialanalysisofrevisionhiparthroplasty:theeconomic burdeninrelationtothenationaltariff.JBoneJtSurgBr. 2012;94(5):619–23.
11.HaenleM,SkripitzC,MittelmeierW,SkriptzR.Economic impactofinfectedtotalhiparthroplastintheGerman diagnosis–relatedgroupsystem.Orthopade. 2012;41(6):467–76.
12.FiliceGA,NymanJA,LexauC,LeesCH,BockstedtLA, Como-SabettiK,etal.Excesscostsandutilizationassociated withmethicillinresistanceforpatientswithStaphylococcus aureusinfection.InfectControlHospEpidemiol.
2010;31(4):365–73.
13.PulidoL,GhanemE,JoshiA,PurtillJJ,ParviziJ.Perisprothetic jointinfection:theincidence,timing,andpredisposing factors.ClinOrthopRelatRes.2008;466(7):1710–5.