rev bras ortop.2015;50(4):482–485
w w w . r b o . o r g . b r
Case
Report
Atypical
femoral
fracture
due
to
chronic
use
of
bisphosphonates:
case
report
夽
Eduardo
Frois
Temponi
∗,
Lúcio
Honório
de
Carvalho
Junior,
Lincoln
Paiva
Costa
HospitalMadreTeresa,BeloHorizonte,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received13July2014 Accepted26August2014 Availableonline10July2015
Keywords: Osteoporosis Femoralfractures Bisphosphonates
a
b
s
t
r
a
c
t
Thecausalrelationshipbetweenchronicuseofbisphosphonatesandoccurrencesofatypical femoralfractureshasnotyetbeenestablished.Nonetheless,itisknownthattheirchronic useismorerelatedtofractureswithapatterndifferingfromthatofclassicalosteoporotic fractures.Atypicalfracturesarestillrareeventsandthebenefitfromusingbisphosphonates remainsgreaterforpreventionandtreatmentofosteoporosis.Therearefewstudiesguiding thediagnosisandmanagementofthesefractures,thusmakingitdifficulttoachievebetter results.Inthisreport,wepresentthecaseofanelderlypatientwithanatypicalfemoral fracturethatwasmanagedinaccordancewithguidancefromtheAmericanSocietyfor BoneandMineralResearch.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Fratura
femoral
atípica
devida
a
uso
crônico
de
bifosfonato.
Relato
de
caso
Palavras-chave: Osteoporose Fraturasdofêmur Bifosfonato
r
e
s
u
m
o
Arelac¸ãocausalentreousocrônicodosbifosfonatoseaocorrênciadefraturasfemorais atípicasnãotemsidoaindaestabelecida.Todavia,sabe-sequeousocrônicodosbifosfonatos temtidomaiorrelac¸ãocomfraturascompadrãodiferentedasclássicasfraturas osteoporóti-cas.Fraturasatípicassãoaindaeventosraroseobenefíciodousodosbifosfonatosaindaé maiornaprevenc¸ãoenotratamentodaosteoporose.Poucosãoosestudosqueorientamo diagnósticoeaconduc¸ãodessasfraturas,oquedificultamelhoresresultados.Nesterelato apresentamoscasodepacientedaterceiraidadecomfraturafemoralatípicaconduzida segundoorientac¸ãodaSociedadeAmericanaparaPesquisaÓsseaeMineral.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevierEditora Ltda.Todososdireitosreservados.
夽
WorkperformedintheOrthopedicsandTraumatologyService,HospitalMadreTeresa,BeloHorizonte,MG,Brazil.
∗ Correspondingauthor.
E-mails:[email protected](E.F.Temponi),[email protected](L.H.deCarvalhoJunior). http://dx.doi.org/10.1016/j.rboe.2015.06.016
rev bras ortop.2015;50(4):482–485
483
Introduction
Bisphosphonatesaretodayamongthemaintypesof medica-tionsprescribedworldwidefortreatingosteoporosis.Several studies have proven that they have an important role in reducing theincidenceofvertebral and non-vertebral frac-tures when used for treating senile and postmenopausal osteoporosis.1,2 Theindicationsforusingthesemedications alsoextendtoothermetabolicdiseasessuchasbone metas-tasis, Paget’s disease and hypercalcemia.3,4 The action of bisphosphonatesoccursthroughinhibitionofthefunctionof osteoclasts.Thisinducesapoptosisofosteoclastsand gives risetosignificantsuppressionofremodelingandconsequent lossofbonebalance.5However,theuseofthesemedications isnotfreefromcomplications.
Severalcaseserieshavealreadyindicatedthatthereisan associationbetweenatypicalfemoralfracturesandprolonged use ofbisphosphonates. These fractures differfrom classi-calosteoporoticfractures inseveralrespects,including the mechanismofaction,locationandfractureconfiguration.6–8 AlthoughtheAmericanSocietyforBoneandMineralResearch (ASBMR)haspublishedguidelinesforevaluatingandfollowing upfracturesthatareconsideredatypical,littleisknownabout thisparticulargroupofinjuries.9Theaimsofthepresent arti-cleweretopresentacaseofatypical fracturinginducedby chronicuseofbisphosphonatesandtoreviewthe characteris-tics,epidemiology,pathogenesisandtreatmentofsuchcases, soastoaidorthopedicsurgeonsinconductingsimilarcases.
Case
report
Thepatientwasa90-year-olddark-skinnedwomanofweight 75kgandheight1.50m,whopresentedapainfulconditionof mechanicalpatterninherrightthighthatstartedin Novem-ber2013.Previously, shehad been abletowalk withinher community.Shesufferedinvolutionofhergaitpatternasthe painfulconditionintensifiedandbecamecapableofwalking onlyathome,withthehelpofawalkingframe.Shedidnot haveanyhistoryoffallsoranylocaltraumaticfactor.Shewas knowntopresentsystemicarterialhypertension, non-insulin-dependentdiabetesmellitus,cardiopathyandosteoporosis, whichwereallbeingtreatedwithdrugs.
Shesoughttheorthopedicsandtraumatologyoutpatient clinicofourserviceinFebruary2014,inordertohaveher com-plaintinvestigated.Shehadahistoryofaleft-sideproximal femoralfracture6yearspreviously,whichhadbeentreated atourinstitution,withoutanycomplaint.Shealsoreported thatsincethen,shehadbeenusingcalciumreplacementand hadkeptonusingbisphosphonatesoverthesameperiod.She didnotpresentanyabnormalityintheclinicalexamination, exceptfordiscomfortinherrightlower limb,atthighlevel when walking. Serial radiographs demonstrated normality andgoodevolutionoftheleft-sidefracturethathadpreviously beentreated,butwitharchingofthefemoralcorticalboneand sclerosisofthelateralwallinitsmiddlethird.Inthelightof thesefindings,magneticresonanceimagingofthethighwas requested.Thisshowedthepresenceofincomplete fractur-ingoftheposterolateral/lateralcorticalbonewiththickening
oftheadjacentcorticalboneandboneedema,inassociation withslightunilamellarperiostealthickening.Investigationof laboratoryparametersdidnotshowanyassociatedmetabolic abnormality(Fig.1).
Giventhesefactorsandthesymptomaticcondition,a sur-gicalapproachwasindicated.Therewasdiscussionregarding the best fixation method: intramedullary fixation using a cephalomedullarynailorfixationusingaplate.Inthisspecific case,aninitialattemptwasmadetouseanintramedullary nail,butbecauseofdiaphysealarchingandtheriskof wors-eningtheexistingfracture,itwasdecidedtoplacealocked plateasabridge.
Today,thepatientpresents4monthsofpostoperative evo-lution, with involution of the symptomatic condition and improvementofthegaitpattern,andwithoutanycomplaints. Shealreadypresentsradiologicalindicationsoffracture con-solidation(Fig.2).Becauseofthehistoryofapreviousproximal femoral fracture and the atypical fracture induced by bis-phosphonates (high risk of new fractures), it was decided tomaintainthesupplementationofcalciumandvitaminD, withdrawtheuseofbisphosphonatesandstartthepatienton denosumab.
Discussion
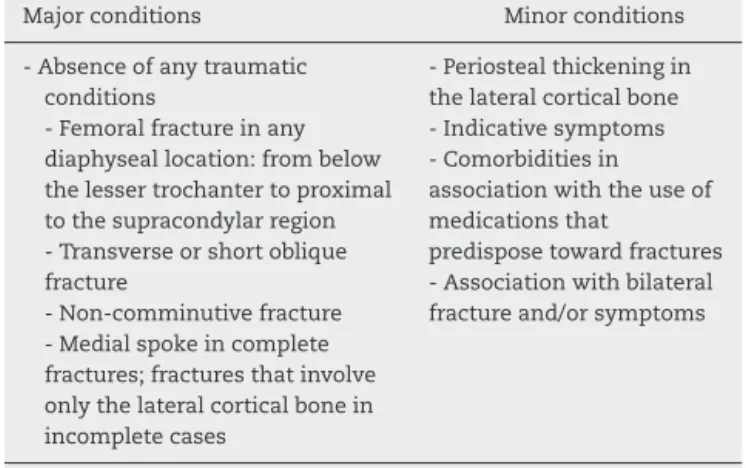
Becauseofthelackofcriteriafordefiningatypicalfemoral
fractures, the ASBMR has established major and minor
conditions for diagnosing these fractures.The presenceof the major conditions is fundamental for designating the fracture asatypical anddistinguishing itfrom osteoporotic fractures, while the minor conditions may be associated with atypical fractures but are notfundamental (Table1).9 Atypicalfemoralfractureshavebeencorrelatedwithseveral factors,includingAsianancestry,bilateralfractures, indica-tivesignsandsymptoms,chronicuseofcorticosteroidsand proton pumpinhibitors, vitaminDdeficiencyandpresence ofdiabetesmellitusandrheumatoidarthritis.7,8TheASBMR has estimated that the accumulated incidence of atypical fracturesis0.9to78casesper100,000individualsperyear. Theincreaseeachyearistwocasesper100,000after2years
Table1–Majorandminorconditionsfordiagnosing
atypicalfemoralfractures.
Majorconditions Minorconditions
-Absenceofanytraumatic conditions
-Femoralfractureinany diaphyseallocation:frombelow thelessertrochantertoproximal tothesupracondylarregion -Transverseorshortoblique fracture
-Non-comminutivefracture -Medialspokeincomplete fractures;fracturesthatinvolve onlythelateralcorticalbonein incompletecases
-Periostealthickeningin thelateralcorticalbone -Indicativesymptoms -Comorbiditiesin associationwiththeuseof medicationsthat
484
rev bras ortop.2015;50(4):482–485Fig.1–Preoperativeradiologicalevaluation.(a,b)Radiographicimagesshowingareaofsclerosisinthemiddlethirdand synthesismaterialfrompreviousfemoralfractureand(c,d)magneticresonanceimagingslicesshowingareaofincomplete fractureintheposterolateralcorticalbone,withpermeatingedema.
ofuseofbisphosphonatesandthisrisesto78per1,000,000 everyyearafter8yearsofuseofthismedication.9
Severalpathogenicmechanismsthatexplainthe relation-ship betweenchronicuse ofbisphosphonates and atypical femoralfractureshavebeenstudied.Chronicuseis respon-sibleforthedeleteriouseffectonbonequality,becausethis inhibits bone remodeling atcell level. Although increased remodeling predisposes toward bone fragility, this effect
also contributes toward an accumulation of architectural damage, reductionof the heterogeneity ofthe cell matrix, increasedglycationofthefinalproductsandlossesthrough remodeling.1,2,7–9 Afteraconditionofatypicalfemoral frac-turehasbeendiagnosed,useofbisphosphonatesshouldbe halted.TheideaofvitaminDandcalciumsupplementation should beevaluated; introduction of bone anabolic agents shouldbeconsidered(denosumaborteriparatide);laboratory
rev bras ortop.2015;50(4):482–485
485
testsshouldbeusedtoidentifyanyexistenceofpredisposing metabolicconditions;thecontralateralsideshouldbe eval-uated, given that the risk of bilaterality is 28–44.2%; and lastly,the best fixationmethod should beevaluated.8,9 No controlledstudiescomparingfixationwithplatesandscrews inrelationtointramedullaryfixationhavebeenconducted, althoughthelatterhasthetheoreticalbenefitofpresenting consolidationthroughendochondralrepair.Therefore,there is a certain degree of preferencefor using nails for treat-ingatypicalfemoralfractures.8–10Despiteallthecarethatis takentoday,andthebetterknowledgeavailable,the progno-sisforthesefractures isstillpoor,withdescriptionsofthe needtorepeat the procedure inup to44% ofthecases in somestudies.Thetimetakenforconsolidationtobeachieved thathasbeendescribed intheliteraturerangesfrom12 to 60months.
The screening for evaluating bone abnormalities in all patients receiving bisphosphonates is inadequate because of the low incidence rate of these fractures and because radiological abnormalities are often unidentifiable. Never-theless, in view of the presence of pain of mechanical patterninpatientswhomakechronicuseofbisphosphonates, carefulassessmentneedstobemadeusingserial radiolog-icalimaging,scintigraphyandmagneticresonanceimaging, in order to institute early diagnosis and treatment.5,8–10 Because many questions relating to atypical femoral frac-turesstilldonothaveanswers,furtherstudiesaimingtoward better histomorphometric and bone biomechanical evalu-ations and the relationship of these fractures to certain medications are fundamental.Moreover,discussiontoward creating a national register of atypical femoral fractures will ensure better understanding and discussion of these cases.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgment
TheauthorsacknowledgetheFroisTemponifamilyformaking thedataandimagesofthecaseavailable.
r
e
f
e
r
e
n
c
e
s
1.NgAC,PngMA,ChuaDT,KohJS,HoweTS.Review: epidemiologyandpathophysiologyofatypicalfemur fractures.CurrOsteoporosRep.2014;12(1):65–73. 2.AspenbergP,SchilcherJ.Atypicalfemoralfractures,
bisphosphonates,andmechanicalstress.CurrOsteoporos Rep.2014;12(2):189–93.
3.TylerW,BukataS,O’KeefeR.Atypicalfemurfractures.Clin GeriatrMed.2014;30(2):349–59.
4.PolascikTJ.Bisphosphonatesinoncology:evidenceforthe preventionofskeletaleventsinpatientswithbone metastases.DrugDesDevTher.2009;3:27–40.
5.FloresSantosF,PinheirodaSilvaJ,FelicíssimoP.Atypical femoralfracturesassociatedwithlong-termtreatmentwith bisphosphonates.ActaMedPort.2013;26(6):746–50. 6.KwekEB,GohSK,KohJS,PngMA,HoweTS.Anemerging
patternofsubtrochantericstressfractures:along-term complicationofalendronatetherapy?Injury.
2008;39(2):224–31.
7.SchilcherJ.Epidemiology,radiologyandhistologyofatypical femoralfractures.ActaOrthopSuppl.2013;84(352):1–26. 8.UnnanuntanaA,SalehA,MensahKA,KleimeyerJP,LaneJM.
Atypicalfemoralfractures:whatdoweknowaboutthem? AAOSExhibitSelection.JBoneJointSurgAm.2013;95(2):e8, 1–13.
9.ShaneE,BurrD,EbelingPR,AbrahamsenB,AdlerRA,Brown TD,etal.Atypicalsubtrochantericanddiaphysealfemoral fractures:reportofataskforceoftheAmericanSocietyfor BoneandMineralResearch.JBoneMinerRes.
2010;25(11):2267–94.
10.HaYC,ChoMR,ParkKH,KimSY,KooKH.Issurgery necessaryforfemoralinsufficiencyfracturesafterlong-term bisphosphonatetherapy?ClinOrthopRelatRes.