rev bras ortop.2015;50(6):743–746
w w w . r b o . o r g . b r
Case
report
Avulsion
fracture
of
the
posterior
cruciate
ligament
in
an
uncommon
location
associated
with
distal
injury
to
the
patellar
ligament
夽
Rodrigo
Pires
e
Albuquerque
∗,
Idemar
Monteiro
da
Palma,
Hugo
Cobra,
Alan
de
Paula
Mozella,
Victor
Vaques
CentrodeCirurgiadoJoelho,InstitutoNacionaldeTraumatologiaeOrtopedia(Into),RiodeJaneiro,RJ,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received4October2014 Accepted26November2014 Availableonline18October2015
Keywords: Knee
Posteriorcruciateligament Bonefractures
a
b
s
t
r
a
c
t
Avulsionfracturesoftheposteriorcruciateligamentinunusuallocationsarerareinjuries. Wereportthefirstcaseintheliteratureofanavulsionfractureoftheposteriorcruciate ligamentassociatedwithdistalinjurytothepatellarligament.Theaimofthisstudywasto presentanovelcase,thetherapyusedandtheclinicalfollow-up.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Fratura
avulsão
do
ligamento
cruzado
posterior
em
uma
localizac¸ão
incomum
associada
a
lesão
distal
do
ligamento
patelar
Palavras-chave: Joelho
Ligamentocruzadoposterior Fraturasósseas
r
e
s
u
m
o
Afraturaavulsãodoligamentocruzadoposterioremlocalizac¸ãonãousualéumalesão rara.Relatamosoprimeirocasodaliteraturadeumafraturaavulsãodoligamentocruzado posteriorassociadaalesãodistaldoligamentopatelar.Oobjetivodesteestudofoiapresentar umcasoinédito,aterapêuticaadotadaeoseguimentoclínico.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevierEditora Ltda.Todososdireitosreservados.
夽
StudycarriedoutatCentrodeCirurgiadoJoelho,InstitutoNacionaldeTraumatologiaeOrtopedia(Into),RiodeJaneiro,RJ,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](R.P.eAlbuquerque).
http://dx.doi.org/10.1016/j.rboe.2015.10.004
744
rev bras ortop.2015;50(6):743–746Fig.1–Preoperativeradiographyoftherightknee(A)AP viewand(B)profileview.
Introduction
Theavulsionfractureoftheposteriorcruciateligament(PCL) isconsideredarareinjury.1Theunusuallocationofthislesion,
aswellasthefactthatitoccurred simultaneouslywiththe distalavulsionoftheipsilateralpatellarligament,makesthis caseevenmoreunusual.
Theobjectiveofthisresearchwastopresentthefirstcaseof theavulsionfractureofPCLinanunusuallocation,associated withdistalruptureoftheipsilateralpatellarligament.
Case
report
A17-year-oldmale,healthyindividual,whosufferedtrauma duetoamotorcycleaccident, immediatelydevelopedpain, hemarthrosisand inability to walk. Thepatient wastaken totheemergencyroomandwastransferredtoourinstitute oneweekaftersufferingtheinjury.Physicalexamination dis-closed++/++++edemainhisrightkneeandrangeofmotionof 30–70◦.
Therightkneeradiographyshowedatibialbonefragment located in the intercondyle with preserved patellar height (Fig.1).Magneticresonanceimaging(MRI)oftherightknee wasperformedtobetterclarifythelesionandplanthesurgical approach,consideringthatclinicalexaminationwashindered bythepresenceofhemarthrosisandjointlimitation.Theright knee MRI showed distalpatellar ligament rupture, and an avulsionfractureofthePCLwithabonefragmentlocatedin theintercondyle(Fig.2).
Thesurgicalproceduretookplacetwodaysafter admis-sion,withthepatientinthesupineposition.Atourniquetwas usedandananteriorstraightincisionwasmadeintheknee toreachthepatellarligament,whereasanotherposteromedial incisionwasmadewiththekneebenttoreachtheavulsion fractureofthePCL.Thesurgicaltechniqueemployedwasthe openreductionandosteosynthesis,witha3.5mmcannulated screwwithafullscrewthreadboltfortheavulsionfractureof PLC(Fig.3).Osteosynthesiswastestedbycarefulbendingthe kneejoint.Regardingthepatellarligament,adistalrupture
Fig.2–PreoperativeMRIoftherightknee.
wasobserved,whichwassuturedwithtransosseousholesand 2.0ethibondwire.
A long kneeimmobilizer was usedforsix weeksofthe postoperativeperiod,whichwasremovedtoperformactive rehabilitation exercisestoprevent quadricepsatrophy.The rangeofmotionwentfrom0to120◦andtotalkneefunction
wasattainedwithinsixmonths.
Thepatientwasreevaluatedafteroneweek,15days,one month,45days,twomonthsandafterthat,monthlyuntilthe sixth monthofevolution, whenthe consultationsoccurred quarterly. Patient follow-up was carried out for one year byclinical andradiographiccontroland hereturnedtohis usualactivities. Theseregularactivitieswerewalking with-outpaincomplaintsandrecreationalsoccertwiceaweek.In thefunctionalkneeevaluation,weusedthemodifiedLysholm
rev bras ortop.2015;50(6):743–746
745
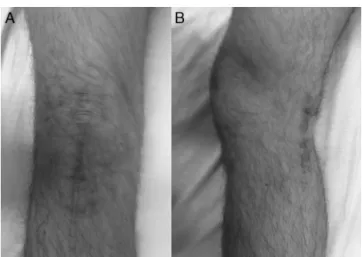
Fig.4–Surgicalaccessroutesinthelatepostoperative periodoftherightknee(A)anteriorand(B)posteromedial.
system,2 whichhadshownpoorresultsinthe preoperative
analysis.Incontrast,inpostoperativeanalysis,anaverageof 95pointswasobtained,whichisconsideredanexcellent aver-ageaccordingtothesameevaluationsystem(Figs.4and5A,B).
Discussion
Amongthe isolated lesions of the PLC,the one caused by tibialboneavulsionistheonewiththegreatestconsensus intheliteratureregardingthesurgicalindicationandearly intervention,3aconceptweagreewithandsupport.
Theisolatedlesion byavulsionofthetibial insertionof thePCLismorefrequentinyoungindividualsanditsnature isessentiallytraumatic.4Motorcycleaccidentsarethemajor
cause ofsuch lesions.4 Our casereport corroboratesthese
claims.According toTrickey,5 the usualmechanism ofthe
avulsionfractureofthePCLisananteriortibialtraumawith thekneeflexed.Webelievethiswasthemechanismofinjury sufferedbyourpatient.Theliteratureshowedonlyonearticle thatmentionedtheunusuallocationoftheavulsedPCL frag-mentintheintercondyle.6Asaresult,weobservedtherarity
ofthiscaseandtherelevanceofitspublication.
Fig.5–Postoperativeclinicalevaluation.(A)Knee extensionand(B)kneeflexion.
Thecontroversyregardingthe treatmentoftheavulsion fractureofthePCLliesinthechosenaccessroute.Asaresult, wechosetheposteromedialsurgicalapproachoftheknee.7
Wechosetheapproachwithtwoincisionsduetothe simul-taneouspresenceofthedistalinsertionlesionofthepatellar ligamentandavulsionfractureofthePCL.Furthermore,the posteromedial access avoidspositioning the patient in the proneposition,andthereisnoneedforgeneralanesthesia.
Clinicalevaluationisessential,butimagingassessmentis complementaryand ofutmostimportanceinassessingthe sizeandlocationofthefragment.Kneeradiographiesarethe firstcomplementaryteststobeordered.Radiographic exami-nationshowedthepatellainitsnormalheight.Itisnoteworthy thatanisolatedPCLlesionisrareandtheMRIcandisclosethe presenceofassociatedlesions.Inourcasereport,thekneeMRI confirmed theavulsed fragmentofPCLintheintercondyle andthedistalpatellarligamentinjury.MRIwasessentialto preventthepatellarligamentlesionfrombeingneglected.
Anothercontroversyisthetypeoffixationintheavulsed fragmentofPLC.7Asaresult,wealwayschosetouseimaging
testswithimproveddetailingofthebonefragmentwhen com-paredtoconventionalradiographies.WethinkthattheMRIor CThelpinsurgicalplanning.Itisnotunusualtousetwotypes ofdevicesintheintraoperativeperiodandduringsurgery,we choosebetweenscrewsoranchors.
Postoperatively,thereisacontroversybetweenkeepingthe kneeimmobilizedornot,duetotheassociatedlesions.One must rememberthatthislesion occurredinanadolescent. Inpatientsinthisagegroup,medicalrecommendationsare morelikelytobedisregarded.8 Theimmatureskeletonhas
alowerriskofjointstiffnesswhencomparedtothatofthe adultpopulation.8Asaresult,wesupporttheuseofabrace
forsixweeks,withdailyremovaltoperformrangeofmotion exercisesandmusclestrengthening.
Themainobjectives ofagoodtreatmentare thecorrect diagnosisand earlyrepairofthelesionstoachieveabetter functionaloutcome.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.BaliK,PrabhakarS,SainiU,DhillonMS.Openreductionand internalfixationofisolatedPCLfossaavulsionfractures.Knee SurgSportsTraumatolArthrosc.2012;20(2):315–21.
2.TegnerY,LysholmJ.Ratingsystemsintheevaluationofknee ligamentinjuries.ClinOrthopRelatRes.1985;198:
43–9.
3.ChiuFY,WuJJ,HsuHC,LinL,LoWH.Managementofavulsion injuryofthePCLwithreattachment.Injury.1994;25(5): 293–5.
4.HughstonJC,BowdenJA,AndrewsJR,NorwoodLA.Acutetears oftheposteriorcruciateligament.Resultsofoperative treatment.JBoneJointSurgAm.1980;62(3):438–50.
5.TrickeyEL.Injuriestotheposteriorcruciateligament:
746
rev bras ortop.2015;50(6):743–7466.NizlanMN,SuhailA,SamsudinOC,MasbahO.Anunusual radiographicpresentationofposteriorcruciateligament avulsionfracture.MedJMalays.2004;59Suppl.F: 65–8.
7.ZhangX,CaiG,XuJ,WangK.Aminimallyinvasive postero-medialapproachwithsutureanchorsforisolated
tibialavulsionfractureoftheposteriorcruciateligament. Knee.2013;20(2):96–9.