REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
MISCELLANEOUS
Can
supreme
TM
laryngeal
mask
airway
be
an
alternative
to
endotracheal
intubation
in
laparoscopic
surgery?
Meltem
Turkay
Aydogmus
∗,
Hacer
Sebnem
Yeltepe
Turk,
Sibel
Oba,
Oya
Unsal,
Sıtkı
Nadir
Sınıkoglu
DepartmentofAnesthesiologyandReanimation,SisliEtfalTrainingandResearchHospital,Istanbul,Turkey
Received16October2012;accepted5December2012
KEYWORDS
Intubation; Intratracheal;
LaryngealMasks;
Laparoscopy
Abstract
Backgroundandobjectives: Inlaparoscopicsurgicalprocedures,expertsrecommendtracheal intubationforairwaymanagement.Laryngealmaskairway(LMA)canbeagoodalternativeto intubation.Inthiscaseseries,weaimedtoexaminetheuseoftheSupremeTM LMA(SLMA)in
laparoscopicsurgicalpractice.
Methods:Weplannedthestudyforsixtypatientsbetweentheagesof18and60,whowould undergolaparoscopicsurgery.Werecordedone,15,30,45,and60-minuteperipheralO2
satu-ration(SpO2)andend-tidalcarbondioxide(EtCO2)values,heartrateandmeanarterialblood
pressure(MAP).WeobservedthedurationofSLMAinsertion,therateofgastrictube applicabil-ity,whethernausea,vomiting,andcoughingdeveloped,andwhethertherewaspostoperative 1-hoursorethroat.
Results:TheinitialEtCO2meanwaslowerthantheEtCO2meansof15,30,45,and60minutes
(p<0.0001)andthe15-minuteEtCO2meanwaslowerthanothermeasuredEtCO2means.We
observedtheinitialheartratemeantobehigherthantheonesfollowingtheSLMAinsertion, priortotheSLMAremoval,andaftertheSLMAremoval.TheheartratemeanaftertheSLMA insertionwasremarkablylowerthantheheartratemeanpriortotheSLMAremoval(p=0.013). TheMAPafter theSLMAinsertionwaslowerthantheinitialMAPmeans,aswellastheMAP averagespriortoaftertheremovalofSLMA(p=0.0001).
Conclusion:SLMAcanbeasuitablealternativetointubationinlaparoscopicsurgicalprocedures inagroupofselectedpatients.
©2013SociedadeBrasileiradeAnestesiologia.PublishedbyElsevier EditoraLtda.Allrights reserved.
∗Correspondingauthor.
E-mail:[email protected](M.T.Aydogmus).
Introduction
Forpatientsatriskofaspiration,endotrachealintubationis stillacceptedasthegoldstandard.Inrecentyears,however, alternativeairwaydeviceslikelaryngealmaskairway(LMA) havebeenusedinthispatientgroup,bothinroutine
proce-0104-0014/$–seefrontmatter©2013SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
Cansupreme laryngealmaskairwaybeanalternativetoendotrachealintubationinlaparoscopicsurgery? 67
duresandinthepresenceofairwayproblems.1Endotracheal
intubationisalsosuggestedtoopenuptheairwayin laparos-copicsurgicalprocedures.Inaddition,insomeprospective and retrospective studies, it is recommended that classic LMAcanbeusedasanalternative.2
LMAhasbeenusedsuccessfullyinanticipatedand unanti-cipateddifficultairwaymanagementsince1981.3,4
Follow-ingthefirstclassicLMAmodel,researchershavedeveloped sub-models.5 The ProSeal laryngeal mask (PLMA), unlike
theclassicLMAmodel,hasadrainagetubewhichprovides a gastric tube passage. SupremeTM LMA (SLMA) has been
desig- ned to combine the desired features of fast-track (ILMA)and PLMA.The fact thatSLMA iselliptical and has ananatomi-callyshapedsemi-hardairwaytubeenablesit tobeinsertedquickly.Moreover,ithasgotagastricchannel forthegastrictubepassage.Whenplacedaccurately,it pro-videsprotectionagainstregurgitationandpreventsgastric distension.2,6,7Inthisstudy,weaimedtoshareour
experi-encesrelatedtotheuseofSLMAinlaparoscopicsurgery.
Methods
Afterapproval from thelocal ethics committee and writ-ten informed consentof the patients, we completed this study in a 6-month period.We selected sixty patients of the ASA I group who were 18 to 40 years old and were scheduledtoundergolaparoscopicsurgery.Patientswhohad abnormalairway,ahistoryofreactiveairway,severeheart andres-piratorytractdiseases,gastro-esophagealreflux,a historyof hiatalhernia,andwhohadrecovered from res-piratorytractinfectionsinthelast6weekswereexcluded fromthe study. Patientshad to fastfor an 8-hour period priortothestudy.Forpremedication,standardintravenous 0.05mg.kg-1 of midazolam was applied. In the operation
room,non-invasivesystemicarterialpressure,cardioscope onDIIderivation,andpulseoximetermonitorization(SpO2)
wereperformed.Wegavepatientsastandardinductionwith 2mg.kg-1ofpropofol,1
g.kg-1offentanyl,and0.5mg.kg-1
ofrocuronium.AlubricatedSLMA(LaryngealMaskCompany Limited,LeRocher,Victoria,Mahe,Seychelles) withasize of either 3 or 4 was inserted by an anesthesiologist with morethanfiveyearsofexperience.Nodigitalmanipulation orother apparatuswasusedwhile theSLMAwasbeing in-serted. The SLMA cuff was inflated to the maximum vol-umeandit wasconfirmed thattherewasnogasleakage. WedeterminedthesizeoftheSLMAtobeinserted depend-ing on the gender and weight of the patient. After the SLMAwasinserted,weassessedventilationbyobservingthe patient’schestexpansionandlisteningtobothlungs bilater-allywithastethoscope.WerecordedtheSpO2valueone,15,
30,45and60-minutesafterSLMAinsertion.Wemonitored theendtidalcarbondioxide(EtCO2)valuethroughout the operation periodrecordedat one, 15, 30,45, 60-minutes after SLMAapplication. A gastric tube was inserted in all patients.Wecarriedontheanesthesiawiththemixtureof 2%sevofluraneand40%air/O2.Wegaveadditionalboluses
ofrocuronium(0.1mg.kg-1)whenrequired.Wedidnotuse
nitrousoxide.Weperformed controlledventilationonthe patientstoob-tain8mL.kg-1tidalvolume,12.min-1
respira-tionrate,and1:2inspiratory:expiratoryrate.WekeptSLMA cuffpressurebelow60cmH2Ousingadigitalmanometer.We
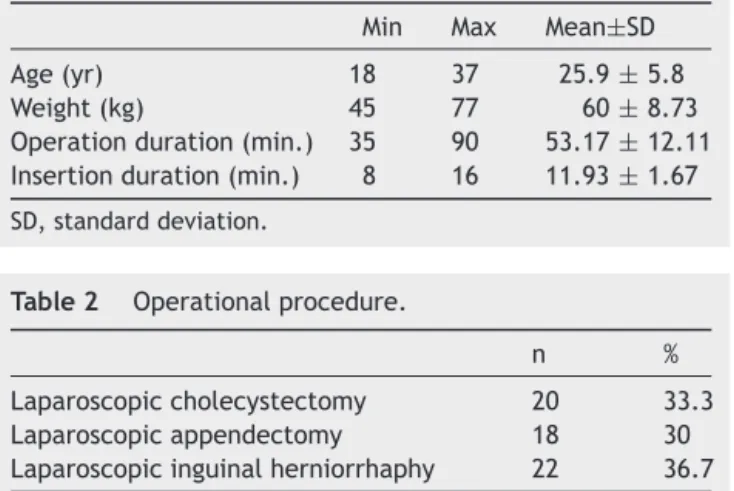
Table 1 Patients age, weight, operation duration and LaryngealMaskAirwayinsertionduration.
Min Max Mean±SD Age(yr) 18 37 25.9±5.8 Weight(kg) 45 77 60±8.73 Operationduration(min.) 35 90 53.17±12.11 Insertionduration(min.) 8 16 11.93±1.67
SD,standarddeviation.
Table2 Operationalprocedure.
n % Laparoscopiccholecystectomy 20 33.3 Laparoscopicappendectomy 18 30 Laparoscopicinguinalherniorrhaphy 22 36.7
recordedtheheart rateand meanarterial bloodpressure
(MAP)ofthepatientsuponentry,followingtheSLMA
inser-tion,priortotheSLMAremoval,andaftertheSLMAremoval.
Foranalgesia,wegavethepatientspreoperative30mg.kg-1
intravenousparacetamol. Afterthe patients’ spontaneous
breathing re- sumed, they have reversal of
neuromuscu-lar block with 0.01mg.kg-1 of atropine and 0.03mg.kg-1
of neostigmine.When breathing normalized, we removed
SLMA. We recorded the duration of SLMA insertion. We
recordedtherateofgastrictubeapplicability,whether
nau-sea,vomiting,aspiration,coughingdeveloped,andwhether
patientshadasorethroat1-hourpostoperatively.
Statistical
evaluation
Weusedthedescriptivestatisticalmethods(mean,standard
deviation,frequencydistribution)inthe evaluationofthe
data.Intherepetitivemeasurementsofmultiplegroupswe
usedone-wayvariantanalysisandinthecomparisonof
sub-groupsweusedtheNewman-Keulsmultiplecomparisontest.
Weconsideredp<0.05valueasstatisticallysignificant.
Results
Theaverageage ofthepatientsenrolledinthestudy was
25.9±5.8years,theaverageweightwas60±8kg,the
aver-ageoperationperiodwas53.17±12minutes,theduration
ofSLMAinsertionwas11.93±1.67seconds(Table1).Welist
operationalproceduresinTable2.Table3displaysthe
dis-Table3 Therangeofpatientsaccordingtothegenderand thesizeofLaryngealMaskAirwaysize.
n %
Sex
Male 29 48.3 Female 31 51.7
LaryngealMaskAirwaysize
3 28 46.7
Table4 Rateofnausea,vomiting,gastrictube insertabil-ity,sorethroatandcoughing.
N %
No 53 88.3 Nausea Yes 7 11.7 No 53 88.3 Vomiting Yes 7 11.7 No 4 6.7 Gastrictube Yes 56 93.3 No 55 91.7 Sorethroat Yes 5 8.3 No 55 91.7 Coughing Yes 5 8.3
Table5 TheSpO2andEtCO2values.
Time SpO2 EtCO2
1minute 98.47±1.35 33.4±4.05 15minutes 98.82±0.98 35.02±4.55 30minutes 98.83±1.06 36.58±5.03 45minutes 98.62±0.97 36.48±4.59 60minutes 98.7±0.87 36.62±4.41 p 0.396 0.0001a
SpO2,peripheralO2saturation;EtCO2,end-tidalcarbondioxide. ap<0.05(mean±SD).
tributionofthepatientsaccordingtogenderandSLMAsize. Weobservednauseaandvomitingin11.7%ofthepatients. Wecouldnotplacethegastrictubein6.7%ofpatients.We observedcoughingandsorethroatsin8.3%ofthepatients (Table4).
Statistically, no remarkable variation was observed in one,15,30,45,and60-minuteSpO2valueaveragesofthe
patients(Table5).
Statistically, we observed a considerable variation in EtCO2 meansatminutesone,15,30,45,and60(p<0.05,
Newman-Keuls).The 1-minute EtCO2 means were
remark-ably lower than the means of 15, 30, 45, and 60-minute EtCO2 (p<0.0001, Newman-Keuls). While the 15-minute
EtCO2 means were statistically much lower than the 30,
45,and60-minuteEtCO2means(p<0.0001,Newman-Keuls),
Table 6 Statistical differences between EtCO2 values
accordingtomeasurementtimes.
Newman-Keulsmultiplecomparisontest pvalue Initial/15minutes 0.001a
Initial/30minutes 0.0001a
Initial/45minutes 0.0001a
Initial/60minutes 0.0001a
15minutes/30minutes 0.003a
15minutes/45minutes 0.001a
15minutes/60minutes 0.0001a
30minutes/45minutes 0.751 30minutes/60minutes 0.919 45minutes/60minutes 0.481
ap<0.05.
Table 7 Patients average heart rate and Mean Arterial BloodPressure.
Heartrate MAP
Initial 98.38±17 84.43±14.31 Aftertheinsertionof
LMA
91.4±15.36 68.35±13.03 PriortoLMAremoval 95.53±12.55 85.13±12.35 Aftertheremovalof
LMA
93.02±14.91 83.9±13.09 p 0.001a 0.0001a
MAP,meanarterialbloodpressure;LMA,laryngealmaskairway.
a p<0.05(mean±standarddeviation).
therewasnostatisticallyconsiderabledifferencebetween theothertimes(Tables5and6).
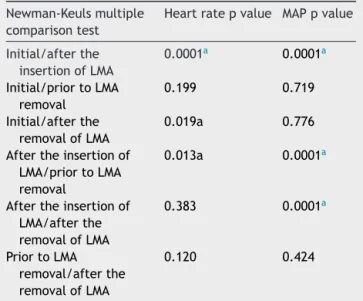
Therewas a significant variationin the initial average heartrateafterweinsertedtheSLMA,beforeweremoved theSLMA,andafterweremovedtheSLMA.Theinitialheart rate meanwashigherthanthe pulseratemean following the SLMA insertion,prior tothe SLMA removal,and after theSLMAremoval.Whiletheaverageheartrate following theinsertionoftheSLMAwasstatisticallymuchlowerthan the average heart rateprior tothe removalof theSLMA, therewasnostatisticallysignificantstatisticallydifference betweentheothertimes(pvaluesinTables7and8).
Aremarkablevariationwasobservedintheinitial aver-ageMAP,afterwe insertedtheSLMA,beforeandafterwe remo-vedtheSLMA(p=0.0001,Newman-Keuls).The aver-age MAP after the SLMA insertion was statistically much lower than the initial average MAP prior to the SLMA removaland aftertheremoval(p=0.0001). Therewasno statisticallysignificantdifferencebetweentheothertimes (Tables7and8).
We could not provide efficient ventilation in only one patient;therefore,weappliedendotrachealintubation.
Table 8 Statistical differences between heart rate and MAPvaluesaccordingtomeasurementtimes.
Newman-Keulsmultiple comparisontest
Heartratepvalue MAPpvalue
Initial/afterthe insertionofLMA
0.0001a 0.0001a
Initial/priortoLMA removal
0.199 0.719
Initial/afterthe removalofLMA
0.019a 0.776
Aftertheinsertionof LMA/priortoLMA removal
0.013a 0.0001a
Aftertheinsertionof LMA/afterthe removalofLMA
0.383 0.0001a
PriortoLMA removal/afterthe removalofLMA
0.120 0.424
MAP,meanarterialbloodpressure;LMA,LaryngealMaskAirway.
Cansupreme laryngealmaskairwaybeanalternativetoendotrachealintubationinlaparoscopicsurgery? 69
Discussion
Hypoventilation, gastric distension, and aspiration asso-ciated with the use of LMA were not more frequent in laparoscopic surgery than with the use of endotracheal tubes.8 In their literature review, Viira et al.9 found the
reported aspiration incidence and serious morbidity fre-quencytogetherwithLMA tobevery low.Inlaparoscopic surgery, the risk of aspiration may increase depending ontheTrendelenburgposition,peritonealstimulationthat occurredduringthesurgery,andincreasedintra-abdominal pressure as a result of the pressure on abdominal wall.8
Someauthorsreportedthat,alongwiththeincreasein intra-abdominalpressure,thepossibilityofgastro-esophagealrefl ux was also increasing in laparoscopic surgery.8 However,
ingynecologicallaparoscopies,thestudiesinvestigatingthe riskofgastro-esophagealrefluxwhenapplyingpositive pres-sure ventilation with a tracheal tube and LMA found no evidencethatshowedthattheriskofgastro-esophagealrefl uxincreasedwithLMA.10,11
The useofLMAin casesin whichanemergency appen-dectomyisperformediscontroversial. Becauseitincludes agastricchannel,PLMAmaybesuperiortoother supraglot-tic airway devices. The gastric distension in laparoscopic surgeryproceduresinwhichPLMAisusedisnotgreaterthan trachealtube.Themostimportantpointtoconsiderwhen usingPLMAinappendectomiesistheexperienceoftheuser andthecarefulselection ofthecases. Theaspirationrisk in appendectomieswithnoadditional riskfactors isquite low.RelyingonthefactthatPLMAislessinvasivethan intu-bationandprovidesbetterprotectionthanclassicLMA,we usedPLMAinappendectomiesandsafelycarriedoutairway management.7Ourstudywasplannedconsideringthefact
thatSLMAismoresuitabletotheanatomicstructure than PLMAanditcauseslessoropharynagealleakagepressure.7
Wemeticulouslyselectedpatients;we particularlydidnot involvepatientswithdoubtfuldiagnosesinthestudy.After weinsertedtheSLMA,weconfirmedthatpatientsreceived efficientventilation
In laparoscopic cholecystectomies, studies have sug-gestedendotrachealintubation-oneofthemostcommonly appliedgeneralsurgeryprocedures-asairwaymanagement. However,one retrospective andthree prospectivestudies claimthatclassicLMAisasuitablealternative.AsforPLMA, it is more effective than classic LMA since it includes a gastric channel.12 One studyfound that nogastric
disten-tion was caused by a laparoscopic cholecystectomy with properlyplaced PLMA, which ventilatesin equal affectiv-ity to the endotracheal tube.13 Carron et al.14 described
one patient with severe pulmonary fi brosis who had an electivelaparoscopiccholecystectomy;theyensuredairway control with SLMA and stated that there wasless airway resistance.
In several studies with patients undergoing gyneco-logical laparoscopic surgery, studies found PLMA to be superiortoclassicLMAandendotrachealintubation.15,16 In
addition,Lee et al.17 compared SLMAwithPLMA in
gyne-cological laparoscopic surgery and showed that, although their complication rates are similar, in SLMA there was less oropharyngealleak pressurethanin PLMA.In astudy comparingSLMAwithendotrachealintubation,researchers foundthatairwaycontrolwasprovidedinequalaffectivity
in gynecological laparoscopic surgeries and SLMA devel-opedless laryngopharyngealmorbidity.18 In anotherstudy,
Yao et al.19 reported that in gynecological laparoscopy,
SLMA ensures ventilation that is equally safe and effec-tiveasendotrachealintubation.TheyalsostatedthatSLMA causesfewerstressresponsesandsideeffects.Furthermore, besidespreventingthesofttissuedamageassociatedwith laryngoscopies,avoidingendotrachealintubationhas advan-tagessuchasreducingairwayresistanceaswellastherisks ofbronchialandesophagealintubation.7Inourstudy,MAP
andheartratesaftertheSLMAinsertionwereconsiderably lowerthantheinitialvalue.Wedidnotdetectanincrease inMAPandpulseratesfollowingtheextubation.
We related this to the lack of hemodynamic stress responsesassociatedwithSLMA
In laparoscopic surgery, as a result of the increase in intraabdominalpressure,earlyclosureinsmallairwaysand an increase in peakairway can beseen. In this case, an increasein EtCO2 can develop withnovariationinSpO2.8
Ourfindings confirmed this.Although therewasno con-siderablevariationintheSpO2valuesofourpatients,the 15, 30, 45, and 60minute EtCO2values were remarkably higherthantheinitialEtCO2values.Inaddition,30,45,and
60-minuteEtCO2valuesweremeaningfullyhigherthan
15-minuteEtCO2values.Forthisreason,wesuggestthatEtCO2
valuesofpatientsshouldbefollowedcarefully
Intheirfirststudy,Eschertzhuberetal.20foundagastric
tubeinsertionsuccessrateof92%inSLMA.Natalinietal.16
showedthatgastric tubeinsertiondoes notguaranteethe fulldrainageofstomachcontents,andin10%ofthepatients in PLMA, the gastric tube is folded with no symptoms of oropharyngeal leakage. We aimed to insert a nasogastric tubeintoallofthepatients.However,wewereunableto dosoinfour(6.7%)patients.
Laparoscopic surgery is a high risk factor related to postoperativenausea and vomiting.21 Patients undergoing
generalanesthesiafor laparoscopic cholecystectomy have ahighriskofpostoperativenauseaandvomitingwith inci-dencesupto75%.22Inourstudy,theratesofpostoperative
nauseaandvomitingareconsiderablyless.Forthisreason, LMASupremeTMmaybepreferableforthisgroupofpatients.
Sore throat after tracheal intubation is common, with an incidence of 30-70%.23 In our study, the rates of sore
throataresignificantly less. Westress that thissituation isimportantforpatientcomfort.
Inconclusion,althoughourstudywaslimitedtoasmall samplesizeofheterogeneouspatients,wesuggestthatSLMA canbeagoodalternativetointubationinselectedgroups of patientsin laparoscopic surgical proceduresby experi-enceduserswhenitisplacedproperlyandtheirpositionis stabilized.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
2.LuPP,BrimacombeJ,YangC,ShyrM.ProSealversustheClassic laryngealmaskairwayforpositivepressureventilationduring laparoscopiccholecystectomy.BrJAnaesth.2002;88:824---7.
3.Singh M,BhartiR, KapoorD.Repairofdamaged supraglottic airwaydevices:anovelmethod.ScandJTraumaResuscEmerg Med.2010;17(18):33.
4.SharmaV,VergheseC,McKennaPJ.Prospectiveauditontheuse oftheLMA-Supremeforairwaymanagementofadultpatients undergoingelectiveorthopaedicsurgeryinproneposition.BrJ Anaesth.2010;105:228---32.
5.AliA,CanturkS,TurkmenA,TurgutN,AltanA.Comparisonof thelaryngealmaskairwaySupremeandlaryngealmaskairway Classicinadults.EurJAnaesthesiol.2009;26:1010---4.
6.VergheseC,RamaswamyB.LMA-Supreme-anewsingle-useLMA withgastricaccess:areportonitsclinicalefficacy.BrJAnaesth. 2008;101:405---10.
7.SeetE,RajeevS,FirozT,etal.Safetyandefficacyoflaryngeal maskairwaySupremeversuslaryngealmaskairwayProSeal:a randomizedcontrolledtrial.EurJAnaesthesiol.2010;27:602---7.
8.OzdamarD,Güvenc¸BH,TokerK,SolakM,EkingenG. Compari-sonoftheeffectofLMAandETTonventilationandintragastric pressureinpediatriclaparoscopicprocedures.Minerva Aneste-siol.2010;76:592---9.
9.ViiraD,MylesPS.Theuseofthelaryngealmaskin gynaecolog-icallaparoscopy.AnaesthIntensiveCare.2004;32:560---3.
10.HoBY,SkinnerHJ,MahajanRP.Gastro-oesophagealreflux dur-ingdaycasegynaecologicallaparoscopyunderpositivepressure ventilation:laryngealmaskvs.trachealintubation. Anaesthe-sia.1998;53:921---4.
11.SkinnerHJ,HoBY,MahajanRP.Gastro-oesophagealrefluxwith thelaryngealmaskduringday-casegynaecologicallaparoscopy. BrJAnaesth.1998;80:675---6.
12.LuPP,BrimacombeJ,Yang1C,ShyrM.ProSealversustheClassic laryngealmaskairwayforpositivepressureventilationduring laparoscopiccholecystectomy.BrJAnaesth.2002;88:824---7.
13.MaltbyJR,BeriaultMT,WatsonNC,LiepertD,FickGH.The LMA-ProSeal isan effectivealternative totracheal intubation for laparoscopiccholecystectomy.CanadianJournalofAnesthesia. 2002;49:857---62.
14.CarronM,MarchetA,OriC.Supremelaryngealmaskairwayfor laparoscopiccholecystectomyinpatientwithseverepulmonary fibrosis.BrJAnaesth.2009;103:778---9.
15.Piper SN, Triem JG, Röhm KD, Maleck WH, Schöllhorn TA, BoldtJ.ProSeal-laryngealmaskversusendotrachealintubation inpatients undergoing gynaecologiclaparoscopy. Anasthesiol IntensivmedNotfallmedSchmerzther.2004;39:132---7.
16.Natalini G, Lanza G, Rosano A, Dell’Agnolo P, Bernardini A. StandardlaryngealmaskairwayandLMA-ProSealduring laparo-scopicsurgery.JClinAnesth.2003;15:428---32.
17.LeeAK, Tey JB,Lim Y, Sia AT. Comparison ofthe single-use LMAsupremewiththereusableProSeal LMAfor anaesthesia ingynaecologicallaparoscopicsurgery.AnaesthIntensiveCare. 2009;37:815---9.
18.Abdi W, Amathieu R, Adhoum A, et al. Sparing the larynx duringgynecologicallaparoscopy:arandomizedtrial compar-ingtheLMASupremeand theETT.Acta AnaesthesiolScand. 2010;54:141---6.
19.Yao T, Yang XL, Zhang F, et al. The feasibility of Supreme laryngeal mask airway in gynecological laparoscopy surgery. ZhonghuaYiXueZaZhi.2010;90:2048---51.
20.EschertzhuberS,Brimacombe J, HohlriederM, KellerC.The laryngealmaskairwaySupreme-asingleuselaryngealmask air-waywithanoesophagealvent.Arandomised,cross-overstudy withthelaryngeal mask airwayProSeal in paralysed, anaes-thetisedpatients.Anaesthesia.2009;64:79---83.
21.WangB,He KH,JiangMB,LiuC,MinS. Effectof prophylac-ticdexamethasoneonnauseaandvomitingafterlaparoscopic gynecologicaloperation:meta-analysis.MiddleEastJ Anesthe-siol.2011;21:397---402.
22.Ryu JH, Jeon YT, Hwang JW, et al. Intravenous, oral, and thecombination of intravenous and oralramosetron for the preventionofnausea and vomiting afterlaparoscopic chole-cystectomy:arandomized,double-blind,controlledtrial.Clin Ther.2011;33:1162---72.