w ww.e l s e v i e r . c o m / l o c a t e / b j p
Original
Article
Evaluation
of
the
effects
of
passion
fruit
peel
flour
(
Passiflora
edulis
fo.
flavicarpa
)
on
metabolic
changes
in
HIV
patients
with
lipodystrophy
syndrome
secondary
to
antiretroviral
therapy
Simone
do
Socorro
Fernandes
Marques
a,
Rosana
Maria
Feio
Libonati
b,
Armando
Ubirajara
Oliveira
Sabaa-Srur
c,
Rensheng
Luo
d,
Pushkar
Shejwalkar
e,
Kenji
Hara
e,
Thomas
Dobbs
f,
Robert
E.
Smith
f,g,∗aCentroUniversitáriodoPará,Belém,PA,Brazil
bNúcleodeMedicinaTropical,UniversidadeFederaldoPará,Belém,PA,Brazil
cInstitutodeNutric¸ão,CentrodeCiênciasdaSaúde,UniversidadeFederaldoRiodeJaneiro,RiodeJaneiro,RJ,Brazil dDepartmentofChemistryandBiochemistry,UniversityofMissouri,St.Louis,USA
eSchoolofEngineering,TokyoUniversityofTechnology,Hachioji,Tokyo,Japan fU.S.FoodandDrugAdministration,Lenexa,KS,USA
gParkUniversity,Parkville,MO,USA
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received11May2015 Accepted21March2016 Availableonline2April2016
Keywords:
Passionfruitpeelflour HIVpatients
Lipodystrophysyndrome Dyslipidemia
a
b
s
t
r
a
c
t
Thisstudyevaluatedtheeffectsofusingpassionfruitpeelflourtogetherwithdiettherapyandcounseling in36patientswithHIVlipodystrophywhowereinanambulatoryclinicinauniversityhospital.The patientsweredividedintotwogroups.Onereceived30gofpassionfruitpeelflourdailyfor90daysand diettherapycounseling.Theothergroupreceivedonlydiettherapycounseling.Themetabolicchanges wereanalyzedbeforeandaftertheintervention,withasignificancelevelpredeterminedatp≤0.05. Theuseofpassionfruitpeelflourwaseffectiveinreducingtotalcholesterolandtriacylglyceridesafter 30days.TheconcentrationsofLDL-Cdecreased,whileHDL-Cincreasedinthebloodoflipodystrophy patientsafter90dayspassionfruitpeelflourtreatment.Nosignificantdifferencesinfoodconsumption wereseenbetweengroups.Theuseof30gofpassionfruitpeelflourfor90daystogetherwithdiet therapycounselingwaseffectiveinimprovingplasmaconcentrationsoftotalcholesterol,LDL-C,HDL-C andtriacylglycerides.
PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeFarmacognosia.Thisisanopen accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Thetreatmentofacquiredimmunodeficiencysyndrome(AIDS) withreversetranscriptaseandproteaseinhibitorsrepresenteda positive impactonthesurvival rate ofindividuals carrying the humanimmunodeficiencyvirus,orHIV(Smith,2014).However, whenHAARTorhighlyactiveantiretroviraltherapy(Smith,2015) became a routine treatment, changes in body fat distribution anddyslipidemiawereobserved(Guimarãesetal.,2007).These changesarecalledHIVLipodystrophysyndrome(Tienetal.,2006;
Guimarãesetal.,2007;Araújoetal.,2007),whichcanincreasethe
riskofcardiovasculardiseases(Friis-Mølleretal.,2003).
∗ Correspondingauthor.
E-mail:[email protected](R.E.Smith).
Soluble fiber may increase short-chain fatty acid synthesis (Wongetal.,2006),therebyreducingendogenouscholesterol pro-ductionandassociatedwithadietlowincholesterolandsaturated fatcanreducebloodlevelsofLDL-Candtriacylglycerides(Liuetal.,
2000;Schneeman,2002; Solàetal.,2007).TheAmericanHeart
Association(2006)recommendedtheuseof5–10g/dayof
solu-blefiberforthereductionofdyslipidemia.Afiber-richdietmay bebeneficialinpreventingthedevelopmentoffatdepositionin peoplewithHIV(Hendricksetal.,2003).
Passionfruitisthecommonnameforvariousspeciesofplants inthegenusPassiflora(Zeriaketal.,2010).Thetwospecieswith themostcommercialvalueareP.edulisfo.edulis(redpassionfruit) andP.edulisfo.flavicarpaO.Deg.(yellow),withtheyellowspecies beingthemostwidelycultivated(Zeriaketal.,2010).Ithasseveral healtheffects,includingloweringtheconcentrationsofLDL-Cand cholesterolintheblood(Ramosetal.,2007).Thepeelscanbedried
http://dx.doi.org/10.1016/j.bjp.2016.03.002
andmadeintoafoodproductcalledpassionfruitpeelflour(PFPF) thathasseveralhealtheffectsandissoldinBrazilasanadjuvant treatmentfordiabetesduetoitshypoglycemiceffect(Smithetal., 2012).Flourpreparedfromyellowpassionfruitpeelshasalsobeen showntoreducebloodglucoseindiabeticpeople.InaphaseI clin-icalstudy,passionfruitpeelflourwaswelltoleratedin36people betweenages20and60,ofbothsexes.Theyreceived10gofflour threetimesadayandweretoldtoputitintheirchoiceofjuice, soup,oranyotherfoodorbeverage.Therewasanaverage reduc-tionofbloodglucose,triacylglycerides,totalcholesterolandLDLof 5.2,15.0,18.2and19.0%,respectively.
InphaseIIstudies,flourpreparedfromyellowpassionfruitpeels reducedbloodglucose,cholesterol,LDL,bloodpressureandbody weightindiabeticpatients.
Thepeels,orrinds,ofHawaiianyellowpassionfruithavebeen fedtocattleandfoundanincreaseinmilkproduction(Otagakiand
Matsumoto,1958).Therearemanyanecdotalaccountsofit
increas-ingmilkproductionandpreventingbacterialinfection,butthese effectshavenotbeenquantified.
PFPFcontainsabout10%moisture,7.5%ash,4%protein,19% solublefiber,38%insolublefiberand21%solublecarbohydrates
(Córdovaetal.,2005;Pinheiroetal.,2008).Themajorcompound
inPFPFispectin,adietaryfiberthatisrichinpolygalacturonicacid anditsmethylester(Smithetal.,2012).However,tothebestof ourknowledge,thesolublecarbohydratesandothersoluble com-poundshaveneverbeenidentifiedoranalyzedbyeitherHPLCor NMR.
Thus,consideringthatPFPFis agoodsourceofsolublefiber, this studyevaluatedtheeffectivenessof PFPFin improvingthe bloodlipidprofileofindividualscarryingHIVandreceivingHAART who developed lipodystrophy. In addition,the hot, pressurized methanolicextract(100◦Cand10MPapressure)wasanalyzedby HPLCandNMR.
Materialsandmethods
Chemicals
Chloroform(CHCl3),deuteratedchloroform(CDCl3),methanol (CH3OH) and deuteratedmethanol (CD3OD) were fromSigma– Aldrich,St.Louis,MO.
PreparationandcharacterizationofthePFPF
ThePFPFwasproducedfromsanitizedripeyellowpassionfruits (Passifloraedulisfo.flavicarpaO.Deg),thatwereidentifiedby AUOS-SandstoredattheFederalUniversityofRiodeJaneiroforfurther reference.Thepeelwasseparatedfromthepulp,dehydrated,and transformedintoflourusing aknifemill.Inorder to character-ize thePFPF,10gofit wasmixedwithenoughHydroMatrixTM (Sigma–Aldrich,St.Louis,MO)tofillthe100mlstainlesssteel sam-plecellusedinanAcceleratedSolventExtractor(ASE,ThermoFisher Scientific,Sunnyvale,CA).Then,CH3OHwasaddedwhilethe tem-perature and pressure were increased to 100◦C and 10.3MPa (1500psi,100atm)overa3mintime(statictime).Next,the sol-ventwaspurgedintoacollectionvessel.Atotaloffourcycleswere runtostaticallyextractthesample,resultinginatotalvolumeof about160ml.Thesolventwasevaporatedoffandtheoilyresidues remainingwereweighed.Aportionoftheresidueremainingafter evaporatingtheCH3OHfromthemethanolicextractofeachsample wasredissolvedinCD3ODforNMRanalysis.Anotherportionwas dissolvedinmethanolforHPLCanalysis.
NMRanalysesweredoneusinganAgilentDD2600MHzNMR (SantaClara,CA).A30◦pulsewidthand1spulsedelaywereused forthe1HNMR,whilea30◦pulsewidthand2spulsedelaywere
usedforthe1H-coupled13C-NMRspectra,alsoknownas13C{1H} -NMR.ChemicalshiftswerereferencedtotheCD3ODsignalsat3.35 and4.78ppm(for1H)and49.30ppm(for13C)forthespectraofthe methanolicextractsandtotheCDCl3signalsat7.27and77.23ppm, for1Hand13C{1H}-NMR,respectively.
TheFTIRspectrumoftheresidueremainingfromthemethanolic extract,afterevaporatingoffthemethanolwasacquiredusingATR attachmentonShimadzuIRAffinity-1S.TheUV–Visspectrumofa 5g/mlsolutionoftheextractinmethanolwasobtainedusing ShimadzuUV-2600.Plainmethanolwasusedasblank.Thesource oflightwasshiftedtodeuteriumbulbat300nmandthespectrum windowwasopenedbetween900nmand185nm.
Experimentaldesign
A clinical therapeutic randomized trial was performed with individuals carrying HIV, presenting Lipodystrophy Syn-drome,receivingHAART,andshowingdyslipidemia (hypercholes-terolemia,hypertriglyceridemia,orboth)asdefinedbytheNational
Cholesterol Education Program (2002). These individuals were
monitoredat theLipodystrophyAmbulatory Centerin theJoão deBarrosBarretoUniversityHospital(HUJBB),duringtheperiod of JanuarytoDecember 2009,and fulfilled thecriteria for par-ticipationin the study.Thesample wascalculated through the calculationofProportion:twosamples.Forthefirstsample(from thegroupusingPFPF),theestimatedproportionofplasma choles-terolimprovementwas50%;forthesecondsample,thisestimate wasof10%.Theratiobetweenthesesampleswasstipulatedas1:1. Thepowerofthetestwasfixedas0.8,andtheunilateralalphalevel in0.05.Thesamplewascalculatedfromsixteenindividualsineach group.
The36individualsparticipatinginthestudywere systemati-callydividedintotwogroups.Group1(n=18)receiveddiettherapy counselingand30g/dayofPFPF,consumedasadilutesolutionin water,juices,and/orfruitsmoothies.Group2(n=18)receiveddiet therapycounselingonly.Therewere12menand6womenineach group.
Informationaboutpathology,weight,height,andfoodintake wasassessedintheinitialevaluationbythe24hrecordingmethod (R24)atthetimeoftheinitial(beginningoftheintervention)and lastassessments(endofthestudy).
Individualsfromthetwogroupswereinstructedtohave bio-chemicaltestsperformedmonthly(totalcholesterol–TC,LDL-C, HDL-C,andtriacylglycerides)attheHUJBB’slaboratory.Thesetests wereperformedinthemorning,after12hfastingandat4time pointsinthestudy:beforetheintervention(T0),at30(T30),60 (T60),and90days(T90)aftertheintervention.
Thefollowingparameterswerefollowedasinclusioncriteria inthestudy:beanadultpatient(anygender)receivingHAART, attending treatmentattheLipodystrophy ambulatory centerat theHUJBB,presentingchangesintheTCand/orLDL-Cand/or tri-acylglycerides,presentingundetectableHIVviralloadandLTCD4+ above300cells/mm3 andagreeingtoparticipateinthestudyby voluntarilysigninganinformedconsentform.
Thefollowingcriteriawerefollowedforstudyexclusion: indi-viduals presenting triacylglycerides above 700mg/dl, or using lipid-loweringdrugs,whocouldnotcompletethe90daysof mon-itoring, didnot tolerate theuseof PFPF,missed appointments, displayedmentalillness,wereunderage18(children,and ado-lescents),anddidnotaccepttoparticipateinthestudy.
Thepairedt-test wasusedtoassessthevariation intheresults fromlaboratorytests.
Thestudywasconductedaccordingtotheguidelineslaiddown intheDeclarationofHelsinkiandNurembergCoderespectingthe standardsofresearchinvolvinghumansubjects(resolution196/96) oftheNationalHealthCouncil.Thisstudywasauthorizedbythe EthicsCommitteeforResearchwithHumanBeingsoftheHUJBB fromtheFederalUniversityofParáunderProtocolNo.1945/08. Writteninformedconsentwasobtainedfromallpatients.
Thisresearchreceivednospecificgrantfromanyfundingagency inthepublic,commercialornot-for-profitsectors.
Results
Drymethanol at 100◦C and 10MPa (100atm) pressure in a sealedcontainersolubilized31%ofthePFPF.TheFTIRspectrumof theresidueremainingafterevaporatingoffthemethanolisshown in Fig.1. Thepeaks in theregion from1400to 1800cm−1 are listedinTable1.TheUV–Visspectrumofa5g/mlsolutionofthe extractinmethanolisshowninFig.2.The1Hand13C{1H}-NMR spectraoftheextractareshowninFigs.3and4.The13Cchemical shiftsaretabulatedintheSupplementaryMaterial.Signalsdueto theCHOandCH2Oofcarbohydratesaccountedfor75.9%ofthe totalpeakarea(Fig.1).TherewerealsosignalsduetoCH3(CH2)n
groupsinfattyacylsthatarecovalentlyboundtocarbohydrates asfattyacidglycosidesinboththe1Hand13C{1H}-NMRspectra
(Figs. 1 and 2).On the other hand,several of thesignals that
areproducedbyd-fructosewerenotseen,includingtheonesat 105.93,99.30,84.24,83.31,77.60,76.84,71.93,66.00,65.19and 64.28ppm. So, even though d-fructose is soluble in methanol,
100
98
96
94
92
90
88
86
3700 3200 2700 2200 Wavenumber (cm–1)
% tr
ansmission (a.u.)
1700 1200 700
100
98
96
94
92
90
88
86
1800 1750 1700 1650 1600 1550 1500 1450 1400 Wavenumber (cm–1)
% tr
ansmission (a.u.)
Fig.1.FTIRspectrumofthehot,pressurizedmethanolicextract(100◦Cand10MPa
pressure)ofpassionfruitpeelflour,afterevaporatingoffthemethanol.Thepeaks canbeusedasatypeoffingerprintthatcanbeusedtoidentifyit.
185 1
0.8
0.6
0.4
0.2
0
285 385 485 585
Wavelength (nm) 270 nm
Nor
maliz
ed absorbance units
685 785 885
Fig.2.UV–Visspectrumofthehot,pressurizedmethanolicextract(100◦
Cand 10MPapressure)ofpassionfruitpeelflour,inmethanol.Themaximumat270nm canbeusedtohelpidentifythepassionfruitpeelflour.
8 7
HC = of aromatic compounds
(CH2)n
CD3OD CD3OD
CHO and CH2O of
carbohydrates
CH3
6 5 4 3 2 1 ppm
Fig.3.1HNMRofthehot,pressurizedmethanolicextract(100◦
Cand10MPa pres-sure)ofpassionfruitpeelflour.Thesignalscanbeusedasatypeoffingerprintthat canbeusedtoidentifyit.
ppm 20 40 60 80 100 120 140 160 180
C=O
HC = and C=C of aromatic compounds
(CH2)n CH3 CD3OD
CHO and CH2O of carbohydrates
Fig.4.13C{1H}-NMRofthehot,pressurizedmethanolicextract(100◦Cand10MPa
Table1
PeaksintheFTIRspectrumofthehot, pres-surizedmethanolicextract(100◦Cand10MPa
pressure)ofpassionfruitpeelflour.
cm−1 cm−1
1796 1610
1792 1609
1785 1603
1781 1595
1723 1591
1767 1577
1762 1570
1757 1565
1751 1559
1749 1555
1744 1549
1740 1540
1734 1533
1730 1528
1723 1521
1719 1517
1716 1507
1707 1499
1700 1497
1696 1490
1684 1481
1681 1477
1676 1473
1669 1465
1663 1458
1654 1448
1647 1437
1636 1430
1628 1424
1624 1420
1617 1412
itis notpresent ata sufficientconcentrationtobedetectedby 13C{1H}-NMR.Glucoseandsucrosearenotsolubleinmethanol,
butarenotknowntobeinPFPF,whichdoesnothaveasweettaste. Still,there isa significantconcentrationof fattyacidglycosides inthemethanolicextractofPFPF.Theyproducednotonlysignals duetoCH3(CH2)n,butalsothecarbonylcarbonduetoestersat
170.397and172.635ppm.Thereisalsoatleastonefreefattyacid, asindicatedbythecarbonylcarbonat181.573ppm.Finally,there arealsosignalsduetoHC CRcarbonsandprotonsduetoaromatic compoundsinthe1Hand13C{1H}-NMRspectra.
AsshownintheSupplementaryMaterial,analysisbyHPLC sup-portsthehypothesisthattherearearomaticcompounds.
Outofthe41individualsselectedtoparticipateinthestudy, three wereeliminated fromGroup 1 (tworeported unpleasant tastewhenusingPFPF,andoneinitiatedtheuseoflipid-lowering drugsduringthestudy).InGroup2,twopatientswereeliminated (one initiated the useof lipid-lowering drugs, and one missed subsequent appointments).Thirty-six patientsremained in the studyandwereevaluated.Table2describesthecharacteristicsof thepatients.Thestatisticalanalysisdemonstratednodifference betweenthegroupsaccordingtotheevaluatedvariables.The aver-agevaluesforTC,LDL-C,HDL-C,andtriacylglyceridesarepresented
inTables3and4forpatientsinGroup1and2,respectively.
TheincreaseinHDL-C,inthegroupusingPFPFduring90days averaged5.9±10.7mg/dl,whichcorrespondedto13.4%ofthe ini-tialvalue.On theotherhandinGroup2,theincreaseaveraged 1±10.4mg/dlandcorrespondedto2.3%oftheinitialvalue.
Theaveragevalue(Table3)forbasaltotalcholesteroldetected inGroup1(227.3±42.9mg/dl)isconsideredaborderlinevalue accordingtotheNCEPIII(2003),however,after90daysof inter-vention with PFPF, this value decreased to 192.1±45.2mg/dl, whichisclassifiedasoptimal.Thisreductionwashighlysignificant (p=0.001)andalready noticedasasignificantdecrease30days
Table2
EffectsofPFPFontheplasmaconcentrationsofcholesterol,LDL-C,HDL-CandTGin HIVpatientswithlipodystrophysyndromesecondary.
Variable Group1 Group2 pvalue
Average SD Average SD
Age(years) 46.0 8.4 46.6 7.0 0.83
Timesincediagnosis(years) 9.1 4.9 11.0 5.4 0.28 DurationofHAART(years) 8.2 4.5 10.0 5.0 0.25
Weight(kg) 59.7 10.1 57.5 10.4 0.52
BMI(kg/m2) 23.3 2.8 22.1 3.5 0.28
Therewere12menand6womenineachgroup.Thedataobtainedwere tabu-latedandanalyzedusingtheBiostat5.0program(2007)withasignificancelevelof
p≤0.05.Thedietproprogram(EstevesandMonteiro,2002)wasusedforthe eval-uationofR24h.Thebilateralt-testwasusedfortheverificationofhomogeneityin theobservedvaluesbetweenthegroups.Thepairedt-testwasusedtoassessthe variationintheresultsfromlaboratorytests.
aftertheintervention(p=0.007).TheLDLconcentrationsin indi-vidualswhousedPFPFduring30and60daysshoweddiscreteand non-significantreduction.AsignificantLDL-Creductionwasonly observedafter90daysofintervention(p=0.0082).
AdiscreteandnotsignificantelevationintheHDL-C concentra-tionswereobservedinindividualswhousedPFPFduring30days; however,asignificantincreasewasobservedafter90daysofits use(p=0.0294).TherewerenosignificantchangesintheHDL-C concentrationsinGroup2throughouttheinterventionperiod.
Theplasmatriacylglyceridesconcentrationsdecreased signifi-cantly(p=0.034)after30daysofPFPFconsumptiontogetherwith diettherapycounseling.However,therewasnofurthersignificant reductionafterwards,showingthatPFPFassistedinreducingthe levelsoftriacylglyceridesinjustthefirst30daysandmaintaining thislowerlevelthroughoutthestudy.
Table3
Averagesandstandarddeviationsanddifferencesbetweentheaveragevaluesof theevaluatedparametersduringtheinterventioninGroup1(whichreceiveddiet therapycounselingand30g/dayofPFPF).Comparisonbetweenthebasalvaluesand valuesobservedinotherperiodsthroughoutthestudy.
Evaluation Differencebetweenaverages(SD)
Average SD T0/T30 T0/T60 T0/T90
TC
T0 227.3 42.9 26.8(40.8) 34.5(27.4) 35.2(39.5) T30 200.6 51.2 p=0.007a p<0.0001a p=0.001a
T60 192.8 45.5 T90 192.1 45.2
LDL-C
T0 125.8 33.1 13.2(36.4) 14.5(32.6) 32.3(34.72) T30 112.6 47.7 p=0.14 p=0.1 p=0.0082a
T60 111.3 42.6 T90 93.5 45.8
HDL-C
T0 43.9 12.2 −1.1(9.2) 0.6(9.7) −5.9(10.7) T30 44.8 16.9 p=0.33 p=0.4 p=0.0294a
T60 43.1 13.9 T90 49.7 19.1
TG
T0 323.9 114.4 68.6(140.3) 97.7(149.1) 96.47(164.6) T30 255.2 115.2 p=0.034a p=0.0078a p=0.0140a
T60 226.1 118.4 T90 227.4 139.3
TC,totalcholesterol;TG,triacylglycerides.
ap-value<0.05.Thedataobtainedweretabulatedandanalyzedusingthe
Bio-stat5.0program(2007)withasignificancelevelofp≤0.05.Thedietproprogram (EstevesandMonteiro,2002)wasusedfortheevaluationofR24h.Thebilateral
Table4
Averagesandstandarddeviationanddifferencesbetweentheaveragevaluesof theevaluatedparametersduringtheinterventioninGroup2(whichreceiveddiet therapycounselingonly).Comparisonbetweenthebasalvaluesandvaluesobserved inotherperiodsthroughoutthestudy.
Evaluation Differencebetweenaverages(SD)
Avg SD T0/T30 T0/T60 T0/T90
TC
T0 234 59.7 8.8(36.2) 7.0(26.3) 4.83(35.4) T30 226 56.7 p=0.16 p=0.14 p=0.28 T60 228 55.3
T90 230 50.1
LDL-C
T0 143 52.6 16.9(49.5) 18.5(51.8) 12.7(34.0) T30 126 51.6 p=0.11 p=0.10 p=0.09 T60 125 45.8
T90 131 42.5
HDL-C
T0 43.6 16.5 −0.6(10.6) 2.77(7.8) −1(10.4) T30 44.2 17.3 p=0.40 p=0.09 p=0.35 T60 40.9 14.9
T90 44.6 17.7
TG
T0 294 120.4 −16.2(131.4) 5.33(72.3) −7.94(118.9) T30 310 137.4 p=0.30 p=0.38 p=0.39 T60 288 115.9
T90 302 153.6
TC,totalcholesterol;TG,triacylglycerides.
ThedataobtainedweretabulatedandanalyzedusingtheBiostat5.0program(2007) withasignificancelevelofp≤0.05.Thedietproprogram(EstevesandMonteiro, 2002)wasusedfortheevaluationofR24h.Thebilateralt-testwasusedforthe verificationofhomogeneityintheobservedvaluesbetweenthegroups.Thepaired
t-testwasusedtoassessthevariationintheresultsfromlaboratorytests.
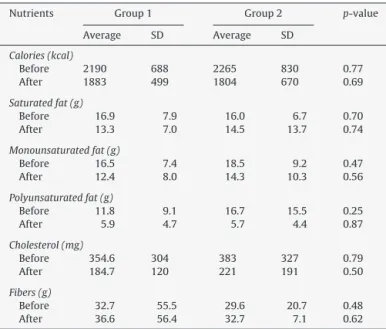
Table5showstheevaluationofeffectsfromtheconsumption
ofmacronutrientsanddietaryfibers,constituentsofthedietused inthestudy,beforeandafterintervention.Therewasnodifference intheconstituentsofthedietbetweenthegroups,thisconfirming theeffectsofthePFPFintheobtainedresults.
Table5
Averageandstandarddeviationoftheconsumptionlevelsofthemainfood compo-nents,beforeandafterintervention,inGroups1and2.
Nutrients Group1 Group2 p-value
Average SD Average SD
Calories(kcal)
Before 2190 688 2265 830 0.77
After 1883 499 1804 670 0.69
Saturatedfat(g)
Before 16.9 7.9 16.0 6.7 0.70
After 13.3 7.0 14.5 13.7 0.74
Monounsaturatedfat(g)
Before 16.5 7.4 18.5 9.2 0.47
After 12.4 8.0 14.3 10.3 0.56
Polyunsaturatedfat(g)
Before 11.8 9.1 16.7 15.5 0.25
After 5.9 4.7 5.7 4.4 0.87
Cholesterol(mg)
Before 354.6 304 383 327 0.79
After 184.7 120 221 191 0.50
Fibers(g)
Before 32.7 55.5 29.6 20.7 0.48
After 36.6 56.4 32.7 7.1 0.62
ThedataobtainedweretabulatedandanalyzedusingtheBiostat5.0program(2007) withasignificancelevelofp≤0.05.Thedietproprogram(EstevesandMonteiro, 2002)wasusedfortheevaluationofR24h.Thebilateralt-testwasusedforthe verificationofhomogeneityintheobservedvaluesbetweenthegroups.Thepaired
t-testwasusedtoassessthevariationintheresultsfromlaboratorytests.
Discussion
To the best of our knowledge, this is the first report that describestheFTIR,UV–VisandNMRanalysisofPFPF.Hot, pres-surized,dry methanolwaschosenasthesolventtoextractthe PFPF,becausepreviousstudieshaveshownthatitisbetterthan ultrasound,Soxhletextractionor othermethods forsolubilizing solids in fruits(Richter et al., 1996; Richards et al.,2014).Dry methanolat100◦Cand10MPa(100atm)pressureinan acceler-atedsolventextractorwasabletosolubilized-fructose,fattyacid glycosidesandothercompoundsfromavarietyoffruits(Richards etal.,2014).d-fructoseproducedmorethansixsignals,becauseit existsasamixtureofthreeisomersinmethanol:-fructopyranose, ␣-fructofuranoseand-fructofuranose(Richardsetal.,2014).Fatty acidglycosideshavebeenshowntohaveimportant neuromodula-toryeffects(Akihisaetal.,2007;Lietal.,2008;Smith,2015).
TheFTIRspectrumhadalarge,broadpeakfromabout3000to 3500cm−1.Thisindicatesthepresenceofhydroxylgroups(Smith,
2014).Therewere alsopeaks from1650to 1780,and 1600to 1650cm−1duetoC OandC Obonds,respectively(Smith,2014). TheUV spectrum hadmaximum absorbance(max)at 205and 270nm.Themaxat270nmindicatesthepresenceofoneormore aromaticcompounds.The1Hand13C{1H}-NMRspectracontained signalsfromabout3.0to5.4ppmand64to110ppm,respectively, duetoCHOandCH2Ogroupsincarbohydrates.Fructoseistheonly simplesugarthatdissolvesinmethanol.However,PFPFdoesnot tastesweetandtherewereseveralsignalsthatfructoseisknown toproducein13C-NMRspectra(Richardsetal.,2014)thatwere not seen inthe spectrum. Also, there weresignals from 0.6to 1.0ppmand14.5to34ppminthe1Hand13C{1H}-NMRspectra duetotheCH3and(CH2)noffattyacylgroups.Thissupportsthe
hypothesisthatPFPFcontainsfattyacidglycosides.Therewere sig-nalsfromabout6.8to8.2ppmand128to136ppminthe1Hand 13C{1H}-NMRspectraduetoC CandHC Cbonds.Thisis
consis-tentwiththeUVspectrumthatshowedthepresenceofaromatic compounds.Finally,thereweresignalsinthe13C{1H}-NMR spec-trumfromabout171to182ppmduetoC Obondsinestersand carboxylicacids.TheFTIRspectrumisagoodfingerprintofthePFPF, whiletheUVandNMRspectrawerealsoquiteinformative.
Aclinicaltrialwasconductedinwomenpresenting
dyslipide-mia(Ramosetal.,2007)usingthesame30g/daydoseofPFPFthat
wasusedinthepresentstudy.Similarreductionsinthe concen-trationsofcholesterolinthebloodwereseen(Ramosetal.,2007). Areductionof31.7±28.0mg/dlinthisvaluewasobservedafter 30daysofinterventionand47.0±29.5mg/dlafter60days(Ramos etal.,2007).Bothwerestatisticallysignificant,withp=0.0001and p=0.0000,respectively(Ramosetal.,2007).
Inanotheropenclinicaltrialwasconductedon36healthyadults ofbothgenders,whowereinstructedtoeat10gofPFPFthreetimes aday,dailyforduringeightweeks(Medeirosetal.,2009).A sig-nificantreductionintotalcholesterolconcentrationsintheblood (17.0%forwomenand19.5%formen)wasobserved(Medeirosetal.,
2009).
Elevatedtotalcholesterolisariskfactorfordeveloping cardio-vascular disease(Smith, 2015).Thishasbecomemore frequent amongHIV+ individualswho receiveHAART drugtherapy. Car-diovasculardiseasesaretheleadingcauseofdeathintheUS,but theirincidencecanbeloweredbytakingdrugslikestatinsthat reducebloodcholesterollevels(Smith,2015),andbyconsuming moredietaryfiber(Brownetal.,1999).TheNationalCholesterol EducationProgramintheUSA(2002)estimatedthatforevery1% reductionincholesterolconcentrationintheblood,adecreaseof 2%intheriskofcardiovasculardiseasescouldbeobserved.
compositionofhealthybacteriainthegut,withconcomitanthealth effects.Finally,thefattyacidglycosidesmaybeabletoboostthe immunesystem,reducesmolderinginflammation,whichcanhelp preventcardiovascularandneurodegenerativediseasesaswellas cancer(Smith,2015).
ThereductionofLDL-Cobservedinthisstudyissimilartothe resultsobservedbyothers(Ramosetal.,2007)whosawadecrease of33.6±33.3mg/dlintheLDL-C(p=0.0003)whenintroducing6g ofsolublefiberintheusualdietof52women. Onestudy eval-uatedtheintroductionof14goffiberper dayin womenliving inacommunityinFortCollinsandtherewasan8%reductionin theamountsofLDL-Cafter90daysoffollow-up,lowerthanthe presentstudythatthedecreasewasonaverage32.3±34.7mg/dl ingroup1whichequals25.6%(Davyetal.,2002).Ameta-analysis wasperformedontheeffectsoffiberintakeoncholesterollevels andconcluded,thattheincreaseinsolublefiberinthediet,produce significantresultsontheLDL-Cvalues(Brownetal.,1999).
LDL-Cistheprimarylipoproteinintheplasma,actsasa choles-terol transporter and seems to be the most atherogenic of all
(GoldsteinandBrown,1977).Thedepositionofcholesterolisa
con-sequenceofoxidationofcirculatingcholesterol-richlipoproteins, inparticular LDL-C(Steinber,1997;Cobbold etal.,2002).Thus, theNCEPhasidentifiedthislipoproteinasthemaintargetinthe treatmentofdyslipidemia(NCEP,2002).TheincreaseinLDL-C lev-elspromotesatherogenesishowever,therestorationoftheideal serumlevelsreducestheriskofatheroscleroticcardiovascular dis-easesignificantlyeveninpatientswhoalreadypresentadvanced pathology(Grundyetal.,2004;Tabasetal.,2007).Thereduction of39mg/dlinthislipoproteinlevelreducesin30%therelativerisk fordevelopingcoronaryarterydisease(Grundyetal.,2004).
It wasfoundthatadults of bothsexes who received30gof PFPFdailyforeightweekshadsignificantlyloweraverageHDL-C concentrationsattheendofthestudycomparedtothebeginning
(Janebroetal.,2008).Thispatternwasalsoobservedinthepresent
study,inbothfourthandeighthweek.Thevaluesreachedthe nor-malrangeforbothwomenandmeninthislatestevaluation,andthe respectiveaverageswere53.50±10.8mg/dland43.2±8.13mg/dl
(Janebroetal.,2008).
TheresultsfromtheVeteransAffairsHigh-Density Lipoprotein Intervention Trial reinforced the idea that elevated HDL-C can reducetherisk ofcoronarydisease(Rubinsetal.,2000).In this study,the22%reductionindeathsfromcoronaryeventsor non-fatal myocardial infarctions was correlated to thereduction in cholesterolandtriacylglycerideslevels,by4%and31%,respectively, andintheincreaseofHDL-Cby6%,withoutsignificantchanges in LDL-C(Rubinset al., 2000).It shouldbe emphasizedthat in thepresent study,theHDL-CinthegroupusingPFPFincreased from 43.9±12.2mg/dl at dayzero to 49.7±19.1 after 90 days
(Table3).OntheotherhandHDL-Cchangedfrom43.6±16.5to
44.6±17.7mg/dlafter30days.
DespitethefibersnotinterferingdirectlyintheHDL-Clevels, thislipoproteinvariesinareversedwaywiththetriacylglycerides (Vegaetal.,2014).Thereductioninlipolysisofthelipoproteins richintriacylglycerideslowersthelevelsofavailablesubstratefor thematurationofHDL-C(deManetal.,2003).Inaddition,the enrichmentofHDL-Cwithtriacylglyceridesincreasesthecatabolic rateandtherefore,reducesitsplasmaconcentration.Also,thelipid exchangebetweenHDL-Candthelipoproteinsrichin triacylglyc-eridesarereducedleadingtoafasterdisappearanceoftheplasma HDL-C(Genestetal.,2006).Foreach1%increaseinHDL-Cthere wasa1%reductionincoronaryeventsregardlessofthevariation ofLDL-C,becauseHDL-Cpromotestheesterficationofcholesterol andprotectsthearteriesduetothereversetransportof choles-terol.Thispromotesthewithdrawalofcholesterolfromthetissues peripheraltotheliverwhereitisexcretedinthebile(Abbottetal.,
1988;Barter,2004;Daminellietal.,2008).
In agreement with the present study, 43 volunteers who received30g/dayPFPFexperiencedasignificantreductionin tria-cylglyceridesafter8weeksusingthisflour.Theaveragevaluesfell from212.0±119.3to161.2±91.1mg/dl(Janebroetal.,2008).
Hypertriglyceridemiaisanindependentriskfactorfor athero-genesis,stroke,andacutemyocardialinfarction.Itwasobservedin ameta-analysiswithseventeenprospectiveepidemiological stud-iesthateveryincreaseof89mg/dlinthetriglyceridemialedtoan increasein therisk ofcardiovasculardiseaseof 32%and76%in menandwomen,respectively(Abbottetal.,1988).Thehigherthe triglyceridemia,thegreatertheformationofLDL-CtypeB,which aresmalleranddenser.Thisisimportantbecausesmallanddense LDL-Cparticlesmaybemoresusceptibletooxidativemodification. Also,anincreasednumberofatherogenicparticlesmayadversely influencecardiovascularrisk(Passarelietal.,2007;Milleretal.,
2011).
Conclusion
Itwasconcludedthattheuseof30gofpassionfruitpeelflour during30daystogetherwithdiettherapycounselingwaseffective inreducingcholesterolandtriacylglycerideslevels.PFPFtreatment showedgoodeffectsagainstlipodystrophyinHIVpatientstreated for90days.Theuseofthisproductfor90dayswaseffectivein reducingtheLDL-C,andincreasingtheHDL-Cvaluesinindividuals presentingHIV Lipodystrophysyndromeanddyslipidemia.PFPF wasfoundtocontainmethanol-solublefattyacidglycosidesand aromaticcompounds whenanalyzed byNMR. FTIRandUV–Vis spectraarealsousefulinestablishinga“fingerprint”ofPFPF.
Ethicaldisclosures
Protectionofhumanandanimalsubjects. Theauthorsdeclare thattheproceduresfollowedwereinaccordancewiththe regula-tionsoftherelevantclinicalresearchethicscommitteeandwith thoseoftheCodeofEthicsoftheWorldMedicalAssociation (Dec-larationofHelsinki).
Confidentialityofdata. Theauthorsdeclarethattheyhave fol-lowed theprotocolsof theirwork centeronthe publicationof patientdata
Righttoprivacyandinformedconsent.Theauthorsdeclarethat nopatientdataappearinthisarticle.
Authors’contributions
SSFM,RMFLandAUOSSdesignedtheexperimentsandcarried themout.SSFMwrotethefirstdraft.RMFLisheradvisor.She con-ceivedtheproject,anddidthestatisticalanalyses.RESaddedmore backgroundinformation,rewrotethepaperandsubmitteditand revisedit basedon reviewers’comments. TDdidthemethanol extractions.PSandSHacquiredtheFTIRandUV–Visspectraand analyzedthem.RLdidtheNMRanalyses.
Conflictsofinterest
Theauthorsdeclarenoconflictsofinterest.
AppendixA. Supplementarydata
References
Abbott,R.D.,Wilson,P.W.F.,Kannel,W.B.,Castelli,W.P.,1988.Highdensity lipopro-teincholesterol,totalcholesterolscreening, andmyocardialinfarction.The FraminghamStudy.Arterioscler.Thromb.Vasc.Biol.8,207–221.
Akihisa,T.,Matsumoto,K.,Tokuda,H.,Yasukawa,K.,Seine,K.,Nakamoto,K., Kun-ninaga,H.,Suzuki,T.,Kimura,Y.,2007.Anti-inflammatoryandpotentialcancer chemopreventiveconstituentsofthefruitsofMorindacitrifolia(Noni).J.Nat. Prod.70,754–757.
AmericanHeartAssociation,2006.Dietandlifestylerecommendationsrevision:a scientificstatementfromtheAmericanHeartAssociationNutritionCommittee. Circulation114,82–96.
Araújo,P.S.R.,Ximenes,R.A.A.,Lopes,C.F.C.,Duarte,J.Y.,Silva,M.M.,Carneiro,E.M., 2007.AntiretroviraltreatmentforHIVinfection/AIDSandtheriskofdeveloping hyperglycemiaandhyperlipidemia.Rev.Inst.Med.Trop.S.Paulo49,73–78.
Barter,P.,2004.Ishigh-densitylipoproteintheprotectorofthecardiovascular sys-tem?Eur.HeartJ.6,A19–A22.
Brown,L.,Rosner,B.,Willett,W.W.,Brown,F.M.S.,Sacks,F.M.,1999. Cholesterol-loweringeffectsofdietaryfiber:ameta-analysis.Am.J.Clin.Nutr.69,30–42.
Cobbold,C.A.,Sherratt,J.A.,Maxwell,S.R.J.,2002.Lipoproteinoxidationandits sig-nificanceforatherosclerosis:amathematicalapproach.Bull.Math.Biol.64, 65–95.
Córdova,K.R.V.,Gama,T.M.M.T.B.,Winter,C.M.G.,Neto,G.K.,Freitas,R.J.S.,2005.
Característicasfísico-químicasdacascademaracujáamarelo(Passifloraedulis flavicarpaDeg)obtidaporsecagem.Bol.CEPPA23,221–230.
Daminelli,E.N.,Spada,C.,Arício,T.,Oliveira,T.V.,Latrilha,M.C.,Maranhão,R.C.,2008.
Alterationsinlipidtransfertohigh-densitylipoprotein(HDL)andactivityof Paraoxonase-1inHIV+patients.Rev.Inst.Med.Trop.S.Paulo50,223–227.
Davy,B.M.,Davy,K.P.,Ho,R.C.,Beske,S.D.,Davrath,L.R.,Melby,C.L.,2002. High-fiberoatcerealcomparedwithwheatcerealconsumptionfavorablyalters LDL-cholesterolsubclassandparticlenumbersinmiddle-agedandoldermen.Am. J.Clin.Nutr.76,351–358.
deMan,F.H.A.F.,Cabezas,M.C.,vanBarlingen,H.H.J.J.,Erkelens,D.W.,deBruin, T.W.A.,2003.Triglyceride-richlipoproteinsinnon-insulin-dependentdiabetes mellitus:post-prandialmetabolismandrelationtoprematureatherosclerosis. Eur.J.Clin.Invest.26,89–108.
Esteves,E.A.,Monteiro,J.B.R.,2002.Sistemadesuporteaavaliac¸ãonutricionale prescric¸ãodedietas.Dietpro[programacomputacional].Versão4.0.Agromídia Software,Vic¸osa,MG.
Friis-Møller,N.,Weber,R.,Reiss,P.,Thiebaut,R.,Kirk,O.,Monforte,A.A.,Pradier,C., Morfeldt,L.,Mateu,S.,Law,M.,El-Sadr,W.,DeWit,S.,Sabin,C.A.,Phillips,A.N., Lundgren,J.D.,DADstudygroup,2003.CardiovasculardiseaseriskfactorsinHIV patients–associationwithantiretroviraltherapy.ResultsfromtheDADstudy. AIDS17,1179–1193.
Genest,J.,Liby,P.,Gotto-Junior,A.,2006.Distúrbiosdaslipoproteínasedoenc¸a car-diovascular.In:Braunwald,E.,etal.(Eds.),Tratadodedoenc¸ascardiovasculares. ,7ed.Elsevier,RiodeJaneiro.
Goldstein,J.L.,Brown,M.S.,1977.Thelow-densitylipoproteinpathwayandits rela-tiontoatherosclerosis.Ann.Rev.Biochem.46,897–930.
Grundy,S.M.,Brewer,H.B.,Cleeman,J.I.,Smith,J.R.,Lenfant,C.,2004.Definitionof metabolicsyndromereportofnationalheart,lungandbloodinstitute/American heartassociationconferenceonscientificissuesrelatedtodefinition.Circulation 109,433–438.
Guimarães,M.M.M.,Greco,D.B.,Júnior,A.R.O.,Penido,M.G.,Machado,L.J.C.,2007.
Corporal fatdistribution and lipidicand glicemic profilesof HIV-infected patients.Arq.Bras.Endocrin.Metab.51,41–51.
Hendricks,K.M.,Dong,K.R.,Tang,A.M.,Ding,B.,Spiegelman,D.,Woods,M.N.,Wanke, C.A.,2003.High-fiberdietinHIV-positivemenisassociatedwithlowerriskof developingfatdeposition.Am.J.Clin.Nutr.78,790–795.
Janebro,D.I.,Queiroz,M.S.R.,Ramos,A.T.,Sabaa-Srur,A.U.O.,Cunha,M.A.L.,Diniz, M.F.F.M.,2008.Efeitodafarinhadacascadomaracujá-amarelo(Passifloraedulis f.flavicarpaDeg.)nosníveisglicêmicoselipídicosdepacientesdiabéticostipo 2.Rev.Bras.Farmacogn.18,724–732.
Liu,S.,Manson,J.A.E.,Stampfer,M.J.,Rexrode,K.M.,Hu,F.B.,Rimm,E.B.,Willett, W.C.,2000.Wholegrainconsumptionandriskofischemicstrokeinwomen:a prospectivestudy.J.Am.Med.Assoc.284,1534–1540.
Medeiros,J.S., Diniiz, M.F.M.,Sabaa-Srur,A.U.O., Pessoa,M.B., 2009.Avaliac¸ão dasatividadeshipoglicemiantes e hipolipemiantesdacasca do maracujá-amarelo(Passifloraedulis,f.flavicarpa).Rev.Bras.Adolesc.Conflitualidade41, 99–101.
Miller,M.,Stone,N.J.,Ballantyne,C.,Bittner,V.,Criqui,M.H.,Ginsberg,H.N., Gold-berg,A.C.,Howard,W.J.,Jacobson,M.S.,Kris-Etherton,P.M.,Lennie,T.A.,Levi, M.,Mazzone,T.,Pennathur,S.,AmericanHeartAssociationClinicalLipidology, Thrombosis,andPreventionCommitteeoftheCouncilonNutrition,Physical Activity,andMetabolism,CouncilonArteriosclerosis,ThrombosisandVascular Biology,CouncilonCardiovascularNursing,CouncilontheKidneyin Cardio-vascularDisease.,2011.TriglyceridesandcardiovasculardiseaseAscientific statementfromtheAmericanHeartAssociation.Circulation123,2292–2333.
NationalCholesterolEducationProgram(NCEP)ExpertPanelonDetection, Evalua-tion,andTreatmentofHighBloodCholesterolinAdults(AdultTreatmentPanel III),2002.ThirdReportoftheNationalCholesterolEducationProgram(NCEP) ExpertPanelonDetection,Evaluation,andTreatmentofHighBloodCholesterol inAdults(AdultTreatmentPanelIII)finalreport.Circulation106,3143–3421.
Otagaki,K.K.,Matsumoto,H.,1958.Nutritivevaluesandutilityofpassionfruit by-products.Agric.FoodChem.6,54–57.
Passareli,M.,Nakandakare,E.R.,Quintão,E.C.R.,2007.Dislipidemia.In:Saad,M.J.A., Maciel,R.M.B.,Mendonc¸a,B.B.(Eds.),Endocrinologia.Atheneu,SãoPaulo.
Pinheiro,E.R.,Silva,I.M.D.A.,Gonzaga,L.V.,Amante,E.R.,Teofilo,R.F.,Ferreira, M.M.C.,Amboni,R.D.M.C.,2008.Optimizationofextractionofhigh-esterpectin frompassionfruitpeel(Passifloraedulisflavicarpa)withcitricacidbyusing responsesurfacemethodology.Biores.Technol.99,5561–5566.
Ramos,A.T.,Cunha,M.A.L.,Sabaa-Srur,A.U.O.,Pires,V.C.F.,Cardoso,A.A.,Diniz,M.F., 2007.UseofPassifloraedulisf.flavicarpaoncholesterolreduction.Braz.J. Phar-macogn.17,592–597.
Richards,K.M.,Levine,R.A.,Luo,R.,Maia,G.M.,Sabaa-Srur,A.U.O.,Maciel,M.I.S., Melo,E.A.,deMoraes,M.R.,Godoy,H.T.,Chaves,M.A.,doSacramento,C.K., Thomas,A.L.,Smith,R.E.,2014.Improvedextractionofsolublesolidsfromfruits. Nat.Prod.J.4,201–210.
Richter,B.E.,Jones,B.E.,Ezzell,J.L.,Porter,N.L.,Avdalovic,N.,Pohl,C.,1996. Accel-eratedsolventextraction:atechniqueforsamplepreparation.Anal.Chem.68, 1033–1039.
Rubins,H.B.,Collins,D.,Robins,S.J.,2000.TheVAHDLinterventiontrial:clinical implications.Eur.HeartJ.21,1113–1115.
Schneeman,B.O.,2002.Gastrointestinalphysiologyandfunctions.Br.J.Nutr.88, S159–S163.
Smith,R.E.,Menezes,E.M.S.,Sabaa-Srur,A.U.O.,Wycoff,W.,2012.Potentialhealth benefitsofpassionfruitpeelflour.Nat.Prod.J.2,104–107.
Smith, R.E., 2014. Medicinal Chemistry – Fusion of Traditional and Western Medicine,2nded.BenthamScience,Sharjah,pp.375–376.
Smith, R.E., 2015. Medicinal Chemistry – Fusion of Traditional and Western Medicine,3rded.BenthamScience,Sharjah.
Solà, R.,Godàs,G.,Ribalta, J.,Vallvé,J.C.,Girona, J.,Anguera,A., etal.,2007.
Effectsofsolublefiber(Plantagoovatahusk)onplasmalipids,lipoproteins andapolipoproteinsinmenwithischemicheartdisease.Am.J.Clin.Nutr.85, 1157–1163.
Steinber,D.,1997.Lowdensitylipoproteinoxidationanditspathobiological signif-icance.J.Biol.Chem.34,20963–20966.
Tabas,I.,Williams,K.J.,Borén,J.,2007.Subendotheliallipoproteinretentionasthe initiatingprocessinatherosclerosis:updateandtherapeuticimplications. Cir-culation116,1832–1844.
Tien,P.C.,Benson,C.,Zolopa,A.R.,Sidney,S.,Osmond,D.,Grunfeld,C.,2006.Thestudy offatredistributionandmetabolicchangeinHIVinfection(FRAM):methods, design,andsamplecharacteristics.Am.J.Epidemiol.163,860–869.
Vega,G.L.,Barlow,C.E.,Grundy,S.M.,Leonard,D.,deFina,L.F.,2014. Triglyceride-to-highdensitylipoprotein-cholesterolratioisanindexofheartdiseasemortality andofincidenceoftype2diabetesmellitusinmen.J.Invest.Med.62,345–349.
Wong,J.M.W.,deSouza,R.,Kendall,C.W.C.,Emam,A.,Jenkins,D.J.A.,2006.Colonic health:fermentationandshortchainfattyacids.J.Clin.Gastroenterol.40, 235–243.