r e v b r a s r e u m a t o l . 2015;55(1):22–30
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
www . r e u m a t o l o g i a . c o m . b r
Original
article
Assessing
the
magnitude
of
osteoarthritis
disadvantage
on
people’s
lives:
the
MOVES
study
Luís
Cunha-Miranda
a,∗,
Augusto
Faustino
a,
Catarina
Alves
b,
Vera
Vicente
b,
Sandra
Barbosa
caInstitutoPortuguêsdeReumatologia,Lisboa,Portugal bEurotrials,ScientificConsultants,Lisboa,Portugal
cAstraZeneca,ProdutosFarmacêuticosLda.,Barcarena,Portugal
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received27March2014 Accepted28July2014
Availableonline8January2015
Keywords:
Osteoarthritis Qualityoflife Self-report
a
b
s
t
r
a
c
t
Introduction:Osteoarthritis (OA) is one ofthe ten mostdisablingdiseases in developed countriesandoneoftheleadingcausesofpainanddisabilityovertheworld.Earlydiagnosis increasesthelikelihoodofpreventingdiseaseprogression.
Objectives:Toestimatetheprevalenceofself-reportedosteoarthritisandqualityoflifein Portugueseadultswith45ormoreyearsold.
Methods:Observational,cross-sectionalstudy,implementedinhouseholdsbyface-to-face interview.
Results:1039subjectswithmeanageof62yearsand54.2%femalewereincluded.The preva-lenceofself-reportedosteoarthritiswas9.9%.Kneesandhandswerethemostfrequentsite ofdisease.TheprevalenceofOAwashigherinwomenandinparticipantswithout profes-sionalactivity.PresenceofOAwashigherinparticipantswithcomorbidities.Mostsubjects havedonesometreatmentatsomepointintimeforthisdisease:94.5%haddrug ther-apy,49.5%physiotherapy,and19.8%physicalactivity.Painwasassociatedwithheight,with somediseaselocationsspecificallyneck,lowerspineandshoulders,SF12scoresofquality oflife,andmeasurementsofimpactindailyliving,severityofdiseaseanddisability.The impactofOAindailylivingwasgreaterinsubjectsthathadbeenonsickleaveorstopped workingduetoOA,hadworsephysicalandmentalhealth,andwithmoresevereofdisease.
Conclusion:Thisstudyconfirmedthatosteoarthritisisaveryrelevantdiseasewithahigh potentialimpactonqualityoflife,functionandworkabilityandbecauseofitsprevalence withaveryhighgrowingsocialimpact.
©2014ElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthor.
E-mail:[email protected](L.Cunha-Miranda).
http://dx.doi.org/10.1016/j.rbre.2014.07.009
Avaliac¸ão
da
magnitude
da
desvantagem
da
osteoartrite
na
vida
das
pessoas:
estudo
MOVES
Palavras-chave:
Osteoartrite Qualidadedevida Auto-relato
r
e
s
u
m
o
Introduc¸ão:Aosteoartrite(OA)éumadasdezdoenc¸asmaisincapacitantesnospaíses desen-volvidoseumadas principaiscausasdedor eincapacitac¸ãono mundo.Odiagnóstico precoceaumentaaprobabilidadedeprevenc¸ãodaprogressãodadoenc¸a.
Objetivos: Estimara prevalênciadeosteoartriteauto-referidaeaqualidadedevidaem adultosportuguesescom45oumaisanosdeidade.
Métodos: Estudoobservacional,transversal,implementadoemdomicíliosporentrevista interpessoal.
Resultados: Foramincluídosnoestudo1039indivíduoscomidademédiade62anos,sendo 54,2%dogênerofeminino.Aprevalênciadeosteoartriteauto-referidafoide9,9%.Os joe-lhoseasmãosforamolocalmaisfreqüentedadoenc¸a.AprevalênciadeOAfoimaiorem mulhereseemparticipantessematividadeprofissional.Apresenc¸adeOAfoimaiorem participantescomcomorbidades.Amaioriadosindivíduosjátinhampassadoporalgum tratamentoemalgumaocasiãodesuasvidasparaestadoenc¸a:94,5%tiveramtratamento farmacológico,49,5%fisioterapia,e19,8%atividadefísica.Adorestavaassociadacoma estatura,comalgunslocaisdadoenc¸a,especificamentepescoc¸o,colunalombareombros, pontuac¸ãodoSF12paraqualidadedevida,emedidasdeimpactonocotidianodos partic-ipantes,gravidadedadoenc¸aeincapacitac¸ão.OimpactodaOAnodia-a-diafoimaiorem indivíduosquetinhamgozadolicenc¸apordoenc¸aouquepararamdetrabalharporcausada OA,apresentavam-secompiorsaúdefísicaemental,eexibiammaiorgravidadedadoenc¸a.
Conclusão: Esteestudoconfirmouqueaosteoartriteéumadoenc¸amuitorelevante,com impactopotencialelevadonaqualidadedevida,nofuncionamentoenacapacidadepara otrabalhoe,porcausadesuaprevalência,exerceumimpactosocialmuitoelevadoe cres-cente.
©2014ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Osteoarthritis(OA)isthemostimportantrheumaticdisease, whichaffectsallthecomponentsofjoints,mainlythe articu-larcartilage.1OAisoneofthetenmostdisablingdiseasesin
developedcountries,1andisthoughttobethemostprevalent
chronicjointdisease.2Itis,byfar,themostcommonformof
arthritisandoneoftheleadingcausesofpainanddisability worldwide.1,3
PainisthemainsymptomofpatientswithOA,4with
sig-nificantimpactonfunctionalability,causingseveredisability inactivitiesofdailyliving, andbeing associatedwith con-siderablelossinproductivityanddecreasedqualityoflife.4–7
Consideredanage-relateddisease,itismostlikelytoaffect joints that have been continually stressed throughout the years,including knees,hips, small hand joints,and lower spineregion.1,4,8
Worldwide,it hasbeen estimatedthat 9.6%ofmenand 18.0% of women aged over 60 years have symptomatic osteoarthritis.1 Themainrisk factors associatedto OA are
age,gender(morefrequentinwomen),obesity,metabolicor endocrinediseases,traumaorjointoverload,andalsogenetic factors.8–10However,theimportanceofindividualriskfactors
varies,andevendiffers,betweenjointsites.8 Manylifestyle
riskfactors,however, arereversibleor avoidablewhich has important implications for its prevention. Early diagnosis
increasesthelikelihoodofpreventingdiseaseprogressionto situationsofgreaterdisability.
Becausepatientsfrequentlydisregardpainandsymptoms, OA tendstoprogressalmostsilently. Patientsshould know their diseaseand havea preventionplan,avoiding mecha-nismsthat may intensifyprogressionofdisease and using pharmacologicaltreatmentsthatmaypreventthestructural degradationofthejoint.
TheMOVESstudyaimedtoestimatetheprevalenceof self-reportedosteoarthritisanditsimpactonthequalityoflife,in Portugueseadultswith45ormoreyearsold.Inthisstudy,we attemptedtocomparesubjectswithandwithoutself-reported OAinsomeoftheparametersthatmaycontributetoaworse qualityoflifeandlossoffunctionality.
Methods
24
r e v b r a s r e u m a t o l . 2015;55(1):22–30interviewers. Subjects from the households selected were invitedtoparticipateiftheywereaged>45yearsandagreed toparticipateinthestudy.
Asamplesizeof1039participantswasestimatedtoallow thecalculationof95%confidenceintervals(95%CI)for self-reportedprevalenceofosteoarthritiswithaprecisionerrorof 1.8%.
Collected data included, for all responders, sociode-mographic variables, professional activity and working conditions, comorbidities, and self-reported aspects ofthe disease.ForsubjectsreportingOA,specificdatawasfurther collected,including OA characterization(date of diagnosis, symptoms,siteofdisease),workingabilitiesand sickleave, treatment and therapeutic characterization,and quality of lifeandfunctionality(SF-12v2.0).Additionally,subjectswere askedtoanswertofivevisualanalogscales(VAS)tomeasure painintensity,impactofOAindailyliving,severityofdisease, disabilitylevelandpatient’sperceptionoftheimportancethat thedoctorgivestothedisease.
Statisticalanalysis
Self-reportedosteoarthritisprevalenceestimateswere calcu-latedforthePortuguesepopulation,stratifiedbyregion,age andgender.Resultsweresubdividedintwogroups,subjects withself-reportedOAandsubjectswithoutself-reportedOA. ThescoresofSF-12v2.0wereobtainedwithHealthOutcomes ScoringSoftware4.5andrangebetween0and100(highervalues indicatebetterqualityoflife/healthstatus).
Chi-square (CS) and Fisher exact tests (FS), for small cell counts, were used to identify associations between osteoarthritisandqualitativevariables.Thenon-parametric test of Mann–Whitney U was used to compare partic-ipants with and without osteoarthritis and quantitative variables, since the assumption of normality was not accepted(Kolmogorov–Smirnov).Associationbetween quan-titativevariables wasconfirmedwithSpearmancorrelation coefficient. Multiple logistic regression analysis results for thepresenceofself-reportedOAarepresentedbyoddsratio (OR)and95%confidenceintervals.Alltestsweretwo-sided consideringasignificancelevelof5%.Statisticalanalyseswere carriedoutusingIBM®SPSS®Statistics18.
This observational study was registered in ClinicalTri-als.gov,underthenumberNCT01423097.
Results
Thisstudyincluded1039participantswithaverageageof62 years(45–99yearsold)and54.2%female.Table1summarizes thesociodemographicandanthropometriccharacteristicsof thetotalsampleandbygroup(withorwithoutOA).
Overall,approximately72%ofthesamplelivedwithspouse and/orchildren.Overweightwasobservedinalmosthalfof thesubjects(47.0%),andobesitywaspresentin18.0%.65%of participantsdidnothaveprofessionalactivity,mostofthem (76.2%)byretirement,notduetoOA.Themeanageofonset oflaborwas15.2years(SD=5.7).
Hypertensionwasthemostfrequentcomorbidity(32.2%), followed by diabetes (15.4%) and cardiovascular disorders (14.2%).Approximately30%ofparticipantsreportednoillness. Theprevalenceofself-reportedosteoarthritis,inthisstudy, was9.9%(95%CI:8.1–11.7%).
The prevalenceofOA was higher inwomen (13.3% ver-sus5.9%;p<0.001),insubjectsfromNorteandinparticipants withoutprofessionalactivity,asshowninTable1.The partici-pantswithOAwereolder(medianage=64)andhadlessyears ofeducation.
Fortheoverallsample,theself-reportedprevalenceofOA was6.3%intheknees,and5.5%and3.1%inhandsandfeet, respectively.Spinehadaprevalenceof2.7%,andanklesand hips,2.2%.Fists,shoulders,elbows,neckandthoracicspine allhadprevalence’sunder2%.
PresenceofOAwashigherinparticipantswith comorbidi-ties (13.5%versus1.6%without;p<0.001).Subjects withOA presentedhighermediannumberofcomorbidities(2versus1 insubjectswithoutOA;p<0.001).
The prevalence of OA was associated with some of the comorbidities: rheumatoid arthritis, depression, kidney problems, intestinal disorders, osteoporosis, cardiovascular disorders,diabetesandhypertension(Fig.1).
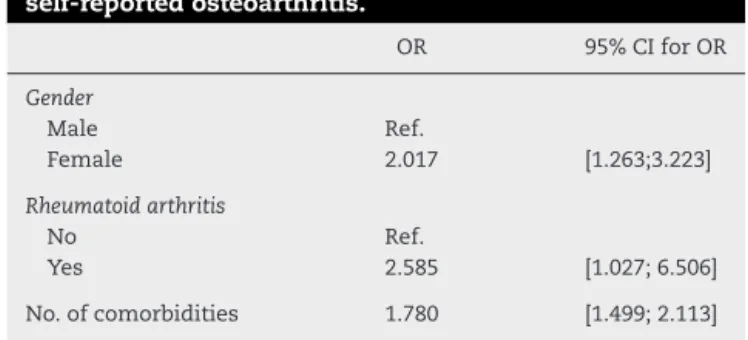
Theresultsofmultiplelogisticregressionsforthepresence ofself-reportedosteoarthritis(Table2)showedthattheriskof OAis2timeshigherforwomen,2.6timeshigherforsubjects withrheumatoidarthritis,and1.8timeshigherforthosewith morecomorbidities.
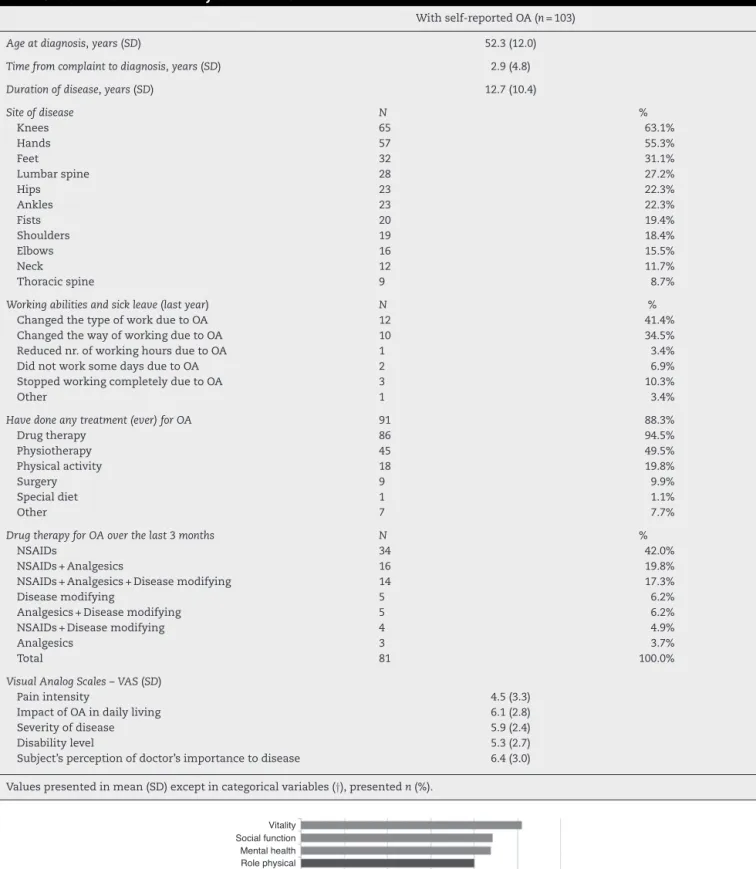
For the subgroupofsubjects withself-reportedOA, fur-therdatawascollectedinordertounderstandwhichvariables couldhavehadsomeimpactonthedisease.Table3 summa-rizestheevaluationvariablesofsubjectswithOA.
Inthisgroupofsubjects,theaverageageatdiagnosiswas 52yearsold(20–85years),andthemeantimebetween com-plaintanddiagnosis was3years,rangingfrom 1monthto 35 years.Themean duration ofdiseasewas13 years(1–56 years).Inmostcases,thegeneralpractitionerdiagnosedthe disease(63.0%)andistheonewhofollowsthepatient(58.4%). Approximately92%ofself-reportedprevalentsubjectshad X-rayconfirmeddiagnosis.
AmongsubjectswithOA,kneesandhandswerethemost frequentsiteofdisease(63.1%and55.3%respectively),andthe thoracicspinethelessfrequentsiteregistered(8.7%).
Approximately30%ofOAsubjectshavebeenonsickleave atsomemomentintimeorstoppedworkingduetothis con-dition.Absenteeismrangedbetween3daysand3years.From these, 41.4%changedtheir typeofwork,34.5%change the wayofworkingforreasonsrelatedtoOA,and10.3%stopped workingcompletelybecauseofthedisease.
Most of OA prevalent subjects (88.3%) have done some treatmentforthisdiseaseatsomemomentintime:94.5%had drugtherapy,49.5%physiotherapy,and19.8%physical activ-ity;surgeryandspecialdietwerealsoreferred.Approximately 84% of patients tookNSAIDs totreat OA (42.0% usedonly NSAIDs),46.9%tookanalgesics(3.7% usedonlyanalgesics), and34.6%wereondiseasemodifyingdrugs(6.2%usedonly diseasemodifyingdrugs)(Table3).
r
e
v
b
r
a
s
r
e
u
m
a
t
o
l
.
2
0
1
5;
5
5(1)
:22–30
25
Total(n=1039) Withoutself-reportedOA(n=936) Withself-reportedOA(n=103) p-value
Age(years) 62.0(45–99) 61.0(45–99) 64.0(45–87) MW:0.002
Gender†
Female 563 54.2% 488 86.7% 75 13.3% CS:<0.001
Male 476 45.8% 448 94.1% 28 5.9%
Region†
Norte 355 34.2% 309 87.0% 46 13.0% CS:0.036
Centro 262 25.2% 243 92.7% 19 7.3%
Lisboa 284 27.3% 253 89.1% 31 10.9%
Alentejo 94 9.0% 88 93.6% 6 6.4%
Algarve 44 4.2% 43 97.7% 1 2.3%
Scholarship(years) 5.0(0–26) 6.0(0–26) 4.0(0–19) MW:0.020
Livingwith†
Alone 183 17.6% 166 90.7% 17 9.3% NA
Withfamily/friends 105 10.1% 101 96.2% 4 3.8%
Spouse/children 749 72.2% 667 89.1% 82 10.9%
Retirementhome 1 0.1% 1 100.0% 0 0.0%
BMI(kg/m2)† 22.2(15.2–42.2) 26.2(15.2–42.2) 26.7(16.9–40.1) MW:0.068
Underweight 6 0.6% 5 83.3% 1 16.7% CS:0.213
Normalweight 356 34.4% 329 92.4% 27 7.6%
Overweight 486 47.0% 435 89.5% 51 10.5%
Obesity 186 18.0% 162 87.1% 24 12.9%
Professionalactivity† 369 35.5% 342 92.7% 27 7.3% CS:0.038
Comorbidities†
Hypertension 334 32.2% 289 30.9% 45 43.7% CS:0.008
Cardiovasculardisorders 147 14.2% 121 12.9% 26 25.2% CS:0.001
Diabetes 160 15.4% 137 14.7% 23 22.3% CS:0.041
Osteoporosis 100 9.6% 80 8.6% 20 19.4% CS:<0.001
Depression 87 8.4% 67 7.2% 20 19.4% CS:<0.001
Kidneyproblems 51 4.9% 40 4.3% 11 10.7% CS:0.004
Intestinaldisorders 43 4.1% 34 3.6% 9 8.7% FS:0.031
Rheumatoidarthritis 25 2.4% 16 1.7% 9 8.7% FS:<0.001
Lungproblems 29 2.8% 23 2.5% 6 5.8% FS:0.059
Cancer 52 5.0% 47 5.0% 5 4.9% CS:0.939
Liverproblems 16 1.5% 12 1.3% 4 3.9% FS:0.065
Gastriculcer 19 1.8% 17 1.8% 2 1.9% FS:>0.999
Fibromyalgia 5 0.5% 4 0.4% 1 1.0% FS:0.408
Other 197 19.0% 163 17.4% 34 33.0% –
No.ofcomorbidities 1.0(0–8) 1.1(0–6) 2.1(0–8) MW:<0.001
MW,Mann–Whitney;CS,Chi-square;FS,Fisherexacttest;NA,Notapplicable.
26
r e v b r a s r e u m a t o l . 2015;55(1):22–30Rheumatoid arthritis** Liver problems Depression* Kidney problems* Intestinal disorders** Lung problems Osteoporosis* Fibromyalgia Cardiovascular disorders* Diabetes* Hypertension* Gastric ulcer Cancer
5%
0% 10% 15% 20% 25% 30% 35% 40%
No Yes
% participants with self-reported osteoarthritis * p < 0.050, Chi-square test.
** p < 0.050, Fisher exact test.
Fig.1–Associationbetweencomorbiditiesandosteoarthritis.
Table2–Logisticregressionforthepresenceof
self-reportedosteoarthritis.
OR 95%CIforOR
Gender
Male Ref.
Female 2.017 [1.263;3.223]
Rheumatoidarthritis
No Ref.
Yes 2.585 [1.027;6.506]
No.ofcomorbidities 1.780 [1.499;2.113]
Ref.:Categoryversustheoneismakingcomparisons.
occurred4days/week(1–7daysperweek)during6weeks.The intakeofanti-inflammatorydrugsoccurredonaveragefor5 days/weekduring7weeks.
ResultsfromVASevaluationareshowninTable3.On aver-age, pain intensity adds up to4.5 points whileseverity of diseaseaddsupto5.9points,consideringameandisability levelof5.3.Impactondailylivingscores6.1pointsonVAS, beingthemostimportantparameterassociatedtothisdisease fromthepatient’sperspective.Subject’sperceptionofdoctor’s importancetodiseaseisscoredwith6.4points.
AnalysisofSF-12v2.0demonstratedthatoverallscorefor mentalhealthregisteredahighervaluethanoverallscorefor physicalhealth,suggestingthatpatientshaveabetterquality ofmentallifethanphysical(45.9points[SD=12.7]and38.5 points[SD=9.3],respectively)(Fig.2).
Association tests have been done to understand which variablesrelatetopaininOA.Inthepresentstudy,painwas associatedwithstature(rs=−0.221;p=0.025)andsomesites
ofdisease [neck (7.9 versus4.2points inOA ofother sites;
p=0.008);hands (5.0 versus 3.1points inOA ofother sites;
p=0.029); spine (7.3 versus 4.1 points inOA in other sites;
p=0.020);andshoulders(7.2versus4.1pointsinOAinother sites; p=0.025)].Pain was alsoassociatedwith SF12 scores ofquality oflife (physical health: rs=−0.479; p<0.001 and
mentalhealth:rs=−0.414;p<0.001),andVASmeasurements
ofimpactofOAindailyliving(rs=0.524; p<0.001),severity
ofdisease(rs=0.557;p<0.001)anddisabilitylevel(rs=0.587;
p<0001).
Furthermore,weevaluatedtheparameters towhichthe impact ofOAin dailyliving(VAS)was related.Statistically higherscoresfortheimpactofOAindailylivingwereshown bysubjectsthathadbeenonsickleaveorstoppedworking duetoOA(8.1pointsversus6.0points;p=0.001).Inaddition, a higher impactofOA on dailylivingwas associatedwith worse physical health(rs=−0.582; p<0.001),mental health
(rs=−0.460; p<0.001), and with higher severity of disease
(rs=0.506;p<0.001).
Discussion
Thisepidemiologicalstudyaimedtoevaluateosteoarthritisin adultindividualsover45yearsofageinPortugal.Theresults suggest that theprevalenceofself-reportedOA inthe Por-tuguesepopulationwith45ormoreyearsofageisbetween 8.1%and11.7%.Thisresultissimilartotheprevalenceresults reportedincountrieslikeCanada,UnitedStates,UK,Australia, NewZealand,Belgium,andtheNetherlands.11,12Theoverall
prevalenceofOA amongNorwegianinhabitantswas12.8%, being significantly higheramong womenthan men.13,14 In
DutchpopulationwithOA,theprevalenceofknee osteoarthri-tiswashigherthanhipone,whichisalsoreportedinother countries,12,14aswellasinourstudyinPortugal.15InPoland,
OA wasdiagnosedin14.7%ofparticipants. Theoccurrence ofOA increasedwith age,being highestinthe groupaged morethan 50years,andmorefrequentinwomen.14 Spain
hasshownanestimatedprevalenceofsymptomatickneeOA of10.2%ingeneraladultpopulationover20 yearsold,and 6.2%forsymptomatichand OA.Theseresultswere mainly relatedtoahighrateofkneepaininwomenagedmorethan 55years.14,16–18
However,mostofthepublishedstudies11,13–15report
preva-lence data from knees, hands and hip symptomatic OA. Informationaboutothersitesofdiseaseisveryscarce.
Table3–CharacterizationofsubjectswithOA.
Withself-reportedOA(n=103)
Ageatdiagnosis,years(SD) 52.3(12.0)
Timefromcomplainttodiagnosis,years(SD) 2.9(4.8)
Durationofdisease,years(SD) 12.7(10.4)
Siteofdisease N %
Knees 65 63.1%
Hands 57 55.3%
Feet 32 31.1%
Lumbarspine 28 27.2%
Hips 23 22.3%
Ankles 23 22.3%
Fists 20 19.4%
Shoulders 19 18.4%
Elbows 16 15.5%
Neck 12 11.7%
Thoracicspine 9 8.7%
Workingabilitiesandsickleave(lastyear) N %
ChangedthetypeofworkduetoOA 12 41.4%
ChangedthewayofworkingduetoOA 10 34.5%
Reducednr.ofworkinghoursduetoOA 1 3.4%
DidnotworksomedaysduetoOA 2 6.9%
StoppedworkingcompletelyduetoOA 3 10.3%
Other 1 3.4%
Havedoneanytreatment(ever)forOA 91 88.3%
Drugtherapy 86 94.5%
Physiotherapy 45 49.5%
Physicalactivity 18 19.8%
Surgery 9 9.9%
Specialdiet 1 1.1%
Other 7 7.7%
DrugtherapyforOAoverthelast3months N %
NSAIDs 34 42.0%
NSAIDs+Analgesics 16 19.8%
NSAIDs+Analgesics+Diseasemodifying 14 17.3%
Diseasemodifying 5 6.2%
Analgesics+Diseasemodifying 5 6.2%
NSAIDs+Diseasemodifying 4 4.9%
Analgesics 3 3.7%
Total 81 100.0%
VisualAnalogScales–VAS(SD)
Painintensity 4.5(3.3)
ImpactofOAindailyliving 6.1(2.8)
Severityofdisease 5.9(2.4)
Disabilitylevel 5.3(2.7)
Subject’sperceptionofdoctor’simportancetodisease 6.4(3.0)
Valuespresentedinmean(SD)exceptincategoricalvariables(†),presentedn(%).
0 10 20 30 40 50 60
Vitality Social function Mental health Role physical Pain Role emotional Physical function
Mental health summary Physical health summary
Worst state Mean Best state
General health
28
r e v b r a s r e u m a t o l . 2015;55(1):22–30mightthinktheyhavebeendiagnosedwithanothercondition butwerediagnosedwithOA,implyingariskoffalse-positiveor false-negativediagnosis.Insummary,assessmentofdisease throughself-report information canlead tosome misdiag-noses,nevertheless self-reportedinformationisconsidered animportantindicatorofaperson’scondition,eventhough itisdependentonhowoneperceivesandacknowledgeshis orherdisease.
Notsurprisingly,inourstudythemostcommonsitesforOA werealsokneesandhands.However,despitehighevidence ofhipOAreportedinothercountries,13,19–21thishasnotbeen
demonstratedinthispopulation.
Age, gender, obesity, injuries, occupation and physical activity are some of the risk factors associated with OA thathavebeenextensivelydiscussedpreviouslyonpublished literature.14,22–24
The oxidative damage that occurs with age is one of the main responsible for the development of OA. Women are morelikely tohave OA than men and alsoto develop moresevere forms ofdisease.The resultsfrom this study confirmthese findingswith prevalenceofOA beinghigher in women than in men, in line with results reported from other countries.11,13,16,18,25,26 Also in line with other
studies,2,11,13,16,18,25,27 age was associated with OA, with a
highermedianageinsubjectswithOA.
SomestudieshaveshownthatriskfactorsforOAof dif-ferentlocalizationmayvary.InItaly,hipOAresultsshowed correlations with weight, genetic factors, gender, previous traumas,occupationalfactors,andage, whileknee OAhad greatcorrelationwithweight,lifestyle,andphysicalactivity.14
Obesityandoverweighthavelongbeenrecognizedapotent riskfactorforOA,especiallyOAoftheknee.2,7,22,27Also,BMI
appearstoplayimportantrolesindeterminingdisabilityof individuals.28Inthepresentstudy,however,OAwasnot
asso-ciatedwithBMI,asopposedtodatafromapopulationsurvey inNorway,13whereBMIwassignificantlyassociatedwithhip
andkneeOA.
Ithas been shown that, in OA patients, comorbid con-ditions may affect not only disease progression, but also theirpsychologicalwell-being,independentlyoftheextentof disease.29,30Inourstudy,theprevalenceofOAwashigherin
subjectswithhypertension,cardiovasculardisordersand dia-betes.Thesecomorbiditieshavealsobeenreportedbyother authors,along withdepression,dyslipidemiaorother mus-culoskeletalconditions.31–33OurfindingsshowedariskofOA
higherforsubjectswithmorecomorbiditieswhichresultin anincreasedneedforattention,investigateandtreatthose comorbiditiesinordertotrytodiminishtheassociated dis-abilityanddecreaseinQoLinpatientswiththoseconditions. OurresultsshowedthatOAwasassociatedwithlessyears ofeducationandabsenteeism,whichwasalsooneofthe find-ingsfromtheNorwegian13andSpanish16,18studies,inwhich
anincreasedoccurrenceofOAwasobservedinpeoplewith lessthan12yearsofeducationandinthoseoutofwork.
Concerningabsenteeismorworkingconditionsassociated to OA, the results of the present study were in line with those reportedin the US,4 with similarpercentage of
sub-jects, changing type or way of working due to OA in our studycomparedtooverallworkandactivityimpairment reg-isteredinUS.EmploymentreductionduetoOAmightalsobe
dependentonthesiteaffectedbyOA.34IntheUSstudy,4
work-ers with OA pain reportedsignificantly lower SF-12 health statuswhencomparedtoworkerswithoutOApain.Likewise, wealsofoundlowerscoresonphysicalcomponentswhich, notsurprisingly,havebeenprovedtobeassociatedtopain, sinceOAandpainaffectphysicalfunctioning.4,13,30
Inourstudy,painmeasuredbyVAS wasalsoassociated withimpactondailyliving,severityofdiseaseanddisability level.Accordingtoliterature,painreliefisthemain motiva-torinpatientswithOAseekingmedicalattention.14Giventhe
relationshipbetweenpainandqualityoflife,itisimportant toseekproperwaystoprovidepatient’swithbetterqualityof life.ItisimportanttounderstandtherelationshipbetweenOA, self-reportedpainanddisabilitymeasures,todevelopabetter knowledgeoftheeffectthatOAhasonapatient’slife, progres-sionofdisease,andeffectivepathwaysforintervention.29,30
Forsomeauthors,22,30 painandfunctionareassumedas
symptomaticoutcomes ofOA that may frequently be con-sidered by patients as part of the pharmacologic efficacy evaluation,associatedwithone’sperceptionsofseverityand improvement.Inourstudy,theresultspointouttoa relation-shipbetweenimpactondailyliving,severityanddisability, whichweretheoutcomesmostconsideredasbeingassociated to thisdisease,from the patients’perspective. Statistically, neckhasbeenthemostpainfulsiteofdiseaseforthe sub-jectsinthisstudy,whichisquiteuncommoninothersimilar studiesalreadypublished.Alongwithneck,alsolumbarspine andshoulderswerestatisticallysignificantforpainand over-allthesepainlevelsmightberesponsiblefortheresults,from thepatients’perspectiveforimpactondailylivingand disabil-ity.Somestudies5,14,28,29reportedthatthepresenceofpainin
osteoarthritisofthehipandkneeswerestronglyassociated withperceptionsofdisabilityinbasicactivitiesofdailyliving. Associationsbetweenself-reportedOA,severityandother patient-reported outcomes indicate the clinical relevance of asking patients to self-evaluate their condition.14 This
approachmay representanadditionalwaytoassess OAin clinicalpractice,althoughfurtherdataisneededtoconfirm theutilityofthismethod.
Conclusion
There are a fewstudies assessingself-reported OA and its impactondailylife.Withthisstudyweattemptedto under-standhowpatientsareaffectedbythisdisease.
Ourstudy confirmsthat theprevalenceofosteoarthritis washigherinwomenandisassociatedwithage.Among sub-jectswithOA,kneesandhandswerethemostfrequentsite ofself-reporteddisease.OAwasassociatedwithfeweryears of education and absenteeism. Impact on dailyliving was patients’mostimportantparameterassociatedtothisdisease, whichwasalsoassociatedwithworsephysicalandmental health,andwithhigherseverityofdisease.
Ina growing-old population, that hastowork for more years,OAhastobeconsidered intermsofpreventionand treatmentinordertocontroltheglobalimpactofthedisease notonlyonpatients,butalsoonsociety.
Financial
support
ThisstudywassponsoredbyAstrazenecaProdutos Farmacêu-ticos,Lda.,Portugal.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. WorldHealthOrganization(WHO)[internet].Availablefrom:
http://www.who.int/chp/topics/rheumatic/en/[accessed 15.01.13].
2. BijlsmaJW,BerenbaumF,LafeberFP.Osteoarthritis:anupdate withrelevanceforclinicalpractice.Lancet.2011;377:2115–26.
3. GuermaziA,NiuJ,HayashiD,RoemerFW,EnglundM,Neogi T,etal.PrevalenceofabnormalitiesinkneesdetectedbyMRI inadultswithoutkneeosteoarthritis:populationbased observationalstudy(FraminghamOsteoarthritisStudy).BMJ. 2012;345:e5339.
4. DiBonaventuraMC,GuptaS,McDonaldM,SadoskyA. Evaluatingthehealthandeconomicimpactofosteoarthritis painintheworkforce:resultsfromtheNationalHealthand WellnessSurvey.MusculoskeletDisord.2011;12:83.
5. MannoniA,BrigantiMP,DiBariM,FerruciL,CostanzoS,Serni U,etal.Epidemiologicalprofileofsymptomaticosteoarthritis inolderadults:apopulationbasedstudyinDicomano,Italy. AnnRheum.2003;62:576–8.
6. NguyenUD,ZhangY,ZhuY,NiuJ,ZhangB,AliabadiP,etal. Increasingprevalenceofkneepainandsymptomaticknee osteoarthritis.AnnInternMed.2011;155:725–32.
7. SowersMF,Karvonen-GutierrezCA.Theevolvingroleof obesityinkneeosteoarthritis.CurrOpinRheumatol. 2010;22:533–7.
8. TheNationalCollaboratingCentreforChronicConditions. Osteoarthritis:Nationalclinicalguidelineforcareand managementinadults.London:RoyalCollegeofPhysicians; 2008.
9. PortaldaSaúde[internet].Availablefrom:http://www. portaldasaude.pt/portal/conteudos/enciclopedia+da+saude/ doencas/doencas+reumaticas/osteoartrose.htm[accessed August2011].
10.SaúdePública®2011;N(46.[internet].Availablefrom:
http://www.jasfarma.pt/artigo.php?publicacao=sp&numero= 46&artigo=34[accessedinAugust,2011].
11.WongR,DavisAM,BadleyE,GrewalR,MohammedM. Prevalenceofarthritisandrheumaticdiseasesaroundthe world.ModelsCareArthritisBoneJtDis(MOCA).2010.
12.RouxCH,SarauxA,MazieresB,PouchotJ,MorvanJ,FautrelB, etal.Screeningforhipandkneeosteoarthritisinthegeneral population:predictivevalueofaquestionnaireand
prevalenceestimates.AnnRheumDis.2008;67:1406–11.
13.GrotleM,HagenKB,NatvigB,DahlFA,KvienTK.Prevalence andburdenofosteoarthritis:resultsfromapopulationsurvey inNorway.JRheumatol.2008;35:677–84.
14.Sakalauskien ˙eG,Jauniskien ˙eD.Osteoarthritis:etiology, epidemiology,impactontheindividualandsocietyandthe mainprinciplesofmanagement.Medicina(Kaunas). 2010;46:790–7.
15.PicavetHS,HazesJM.Prevalenceofselfreported musculoskeletaldiseasesishigh.AnnRheumDis. 2003;62:644–50.
16.CarmonaL,BallinaJ,GabrielR,LaonA,EPISERStudyGroup. Theburdenofmusculoskeletaldiseasesinthegeneral populationofSpain:resultsfromanationalsurvey.Ann RheumDis.2001;60:1040–5.
17.PueyoMJ,SurísX,LarrosaM,AuledaJ,MompartA,BrugulatP, etal.Importanciadelosproblemasreumáticosenla poblacióndeCatalu ˜na:prevalenciayrepercusiónenlasalud percibida,restriccióndeactividadesyutilizaciónderecursos sanitarios.GacSanit.2012;26:30–6.
18.Fernandez-LopezJC,LaffonA,BlancoFJ,CarmonaL,EPISER StudyGroup.Prevalence,riskfactors,andimpactofknee painsuggestingosteoarthritisinSpain.ClinExpRheumatol. 2008;26:324–32.
19.DrivingmusculoskeletalhealthforEurope(eumusc.net). [internet].MusculoskeletalhealthinEurope:Summary report.Availablefrom:http://eumusc.net/[accessed 22.02.13].
20.QuintanaJM,ArosteguiI,EscobarA,AzkarateJ,GoenagaJI, LafuenteI.Prevalenceofkneeandhiposteoarthritisandthe appropriatenessofjointreplacementinanolderpopulation. ArchInternMed.2008;168:1576–84.
21.ThiemU,SchumacherJ,ZacherJ,BurmesterGR,PientkaL. Prevalenceofmusculoskeletalcomplaintsandself-reported jointosteoarthritisinthepopulationofHerne:atelephone survey.ZRheumatol.2008;67:432–9.
22.ZhangY,JordanJM.Epidemiologyofosteoarthritis.Clin GeriatrMed.2010;26:355–69.
23.PalmerKT.Occupationalactivitiesandosteoarthritisofthe knee.BrMedBull.2012;102:147–70.
24.MurphyL,HelmickCG.Theimpactofosteoarthritisinthe UnitedStates:apopulation-healthperspective.AmJNurs. 2012;112:S13–9.
25.SymmonsD,MathersC,PflegerB.Globalburdenof
osteoarthritisintheyear2000.Draft15-08-06.Availablefrom:
http://www.who.int/healthinfo/en/[accessedJune, 2013].
26.SrikanthVK,FryerJL,ZhaiG,WinzenbergTM,HosmerD, JonesG.Ameta-analysisofsexdifferencesprevalence, incidenceandseverityofosteoarthritis.OsteoarthrCartil. 2005;13:769–81.
27.IssaR,GriffinTM.Pathobiologyofobesityandosteoarthritis: integratingbiomechanicsandinflammation.PathobiolAging Age-relatDis.2012;2:17470.
28.WilliamsDA,FarrellMJ,CunninghamJ,GracelyRH,Ambrose K,CuppsT,etal.Kneepainandradiographicosteoarthritis interactinthepredictionoflevelsofself-reporteddisability. ArthritisRheum(ArthritisCareRes).2004;51:558–61.
29.NebelMB,SimsEL,KeefeFJ,KrausVB,GuilakF,CaldwellDS, etal.Therelationshipofself-reportedpainandfunctional impairmenttogaitmechanicsinoverweightandobese personswithkneeosteoarthritis.ArchPhysMedRehabil. 2009;90:1874–9.
30.SadoskyAB,BushmakinAG,CappelleriJC,LionbergerDR. Relationshipbetweenpatient-reporteddiseaseseverityin osteoarthritisandself-reportedpain,functionandwork productivity.ArthritisResTher.2010;12:R162,
http://dx.doi.org/10.1186/ar3121.
31.LeiteAA,CostaAJ,MatheosdeLimaBA,PadilhaAV,
30
r e v b r a s r e u m a t o l . 2015;55(1):22–3032.RosemannT,LauxG,SzecsenyiJ.Osteoarthritis:qualityof life,comorbidities,medicationandhealthserviceutilization assessedinalargesampleofprimarycarepatients.JOrthop SurgRes.2007;2:12,http://dx.doi.org/10.1186/1749-799X-2-12. 33.KadamUT,JordanK,CroftPR.Clinicalcomorbidityinpatients
withosteoarthritis:acase-controlstudyofgeneralpractice
consultersinEnglandandWales.AnnRheumDis. 2004;63:408–14.