r e v b r a s r e u m a t o l . 2015;55(5):464–467
w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Brief
communication
Diagnosing
vertebral
fractures:
missed
opportunities
João
Lindolfo
Cunha
Borges
a,b,∗,
Julianne
Lira
Maia
a,
Renata
Faria
Silva
a,
Edward
Michael
Lewiecki
caCentrodePesquisaClínicadoBrasil,Brasília,DF,Brazil
bUniversidadeCatólicadeBrasília,Brasília,DF,Brazil
cNewMexicoClinicalResearch&OsteoporosisCenter,Albuquerque,UnitedStates
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received29May2014 Accepted7December2014 Availableonline16March2015
Keywords:
Vertebralfractures Osteoporoticfractures Osteoporosis
a
b
s
t
r
a
c
t
Vertebral fractures are the single most common type of osteoporotic fracture. Post-menopausalwomenareatincreasedriskforosteoporoticvertebralfracturescomparedwith womenofchildbearingage.Vertebralfracturesareassociatedwithanincreaseinmorbidity, mortality,andhighriskofasubsequentvertebralfracture,regardlessofbonemineral den-sity.Despitethecommonoccurrenceandseriousconsequencesofvertebralfractures,they areoftenunrecognizedormisdiagnosedbyradiologists.Moreover,vertebralfracturesmay bedescribedbyvariableterminologythatcanconfuseratherthanenlightenreferring physi-cians.WeconductedasurveyofspineX-rayreportsfromagroupofpostmenopausalwomen
screenedforparticipationinastudyofosteoporosisatCentrodePesquisaClínicadoBrasil. Adescriptiveanalysisevaluatedthevariabilityofreportsin7patients.Fourindependent generalradiologistsissuedreportsassessingvertebralfracturesthroughablindedanalysis. Theobjectiveofthisstudywastoevaluateforconsistencyinthesereports.Theanalysis foundmarkedvariabilityinthediagnosisofvertebralfracturesandtheterminologyusedto describethem.Incommunitymedicalpractices,suchvariabilitycouldleadtodifferences inthemanagementofpatientswithosteoporosis,withthepotentialforundertreatmentor overtreatmentdependingonclinicalcircumstances.Accurateandunambiguousreporting ofvertebralfracturesislikelytobeassociatedwithimprovedclinicaloutcomes.
©2015ElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthor.
E-mail:[email protected](J.L.C.Borges).
http://dx.doi.org/10.1016/j.rbre.2014.12.008
rev bras reumatol.2015;55(5):464–467
465
Diagnóstico
de
fraturas
vertebrais:
oportunidades
perdidas
Palavras-chave:
Fraturasvertebrais Fraturasosteoporóticas Osteoporose
r
e
s
u
m
o
Asfraturasvertebraissãootipomaiscomumdefraturaosteoporótica.Asmulheresna pós-menopausatêmumriscoaumentadodefraturasvertebraisosteoporóticasemcomparac¸ão comasmulheresemidadefértil.Asfraturasvertebraisestãoassociadasaumaumento namorbidadeemortalidadeeàelevac¸ãodoriscodefraturavertebralsubsequente, inde-pendentementedadensidademineralóssea.Apesardaocorrênciacomumedasgraves consequências dasfraturasvertebrais,elasmuitas vezespassam despercebidasousão erroneamentediagnosticadaspelosradiologistas.Alémdisso,asfraturasvertebraispodem serdescritascomumaterminologiavariável,quepodeconfundiremvezdeesclarecero médicosolicitante.Foifeitoumlevantamentodoslaudosdasradiografiasdecoluna verte-braldeumgrupodemulheresnapós-menopausaselecionadasparaparticipardeumestudo deosteoporosenoCentrodePesquisaClínicadoBrasil.Aanálisedescritivaavalioua vari-abilidadedoslaudosemsetepacientes.Quatroradiologistasgeraisindependentesemitiram laudosdeavaliac¸ãodasfraturasvertebraispormeiodeumaanálisecega.Oobjetivodeste estudofoiavaliaraconsistênciadesseslaudos.Aanálisedescobriuumaacentuada variabil-idadenodiagnósticodasfraturasvertebraisenaterminologiausadaparadescrevê-las.Na práticaclínicadacomunidade,essavariabilidadepoderialevaradiferenc¸asnotratamento depacientescomosteoporose,comopotencialdesubtratamentooutratamentoexagerado, adependerdascircunstânciasclínicas.Laudosprecisoseinequívocosdefraturasvertebrais sãosusceptíveisdeestarassociadosamelhoresdesfechosclínicos.
©2015ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
AccordingtotheNationalOsteoporosisFoundation,44million peopleintheUnitedStateshaveosteoporosisorosteopenia.1
It isestimated that osteoporosis affects about 200 million womenworldwide,withoccurrenceofanosteoporotic frac-ture every 3s and a vertebral fracture every 22s.1,2 The
annual incidence of osteoporotic fractures in the United States is higher than the combined incidence of heart attack, stroke and breast cancer. The prevalence of verte-bral fractures in Caucasians over 50 years old is 20–25%, and in Latin American is 12%.1,3 Still, people at 50 years,
present a major risk of osteoporotic fracture: 46–53% in womenand 21–22%in men;vertebral fracture in radiogra-phy: 27% in women and men 11%; and clinical vertebral fracture.4 Peri- and postmenopausal women witha
preva-lent vertebral fracture have a two to five-fold increased riskofasubsequentvertebralfracturecomparedtowomen without a prevalent vertebral fracture, regardless of bone mineraldensity.5Inaddition,thepresenceofavertebral
frac-ture increases the mortality rate and the chances of new fractures.6,7 However,failure to identify vertebral fractures
on radiographic studies is a common problem worldwide, withsomereportsofanoverallrateof34%formissed diag-noses,leadingtounder-treatmentandpoorclinicaloutcomes, includingbackpain,lossofindependence,andreduced qual-ity of life.6,8 We therefore undertook an investigation to
evaluateconsistencyanddivergenceofreportsofspine radio-graphsinagroupofpostmenopausalwomendiagnosedwith osteoporosis.
Materials
and
methods
Spineradiographswereperformedin7womenparticipating inastudy ofosteoporosisatCentrode PesquisaClínicado Brasil.ThepurposeoftheseX-rayswastoevaluatefor preva-lentspinefracture.Digitizedspineimages(posterior-anterior andlateralviews)weresentto4generalradiologists,eachof whom wasaware ofthe purposeofthe X-rays,forblinded independentinterpretations.Thereportswerethencompared forconsistencyofterminologyanddiagnosisofvertebral frac-tures.
Results
The interpretation of each radiologist for diagnosis and descriptionofvertebralfracturesisprovidedintheTable1.
Discussion
Osteoporosisisanosteometabolicdiseasethatleadstolow bonemineraldensity,bonemicroarchitecturaldeterioration ofbone,andskeletal fragility,predisposinganindividualto fractures withminimaltrauma.9,10 Postmenopausalwomen
466
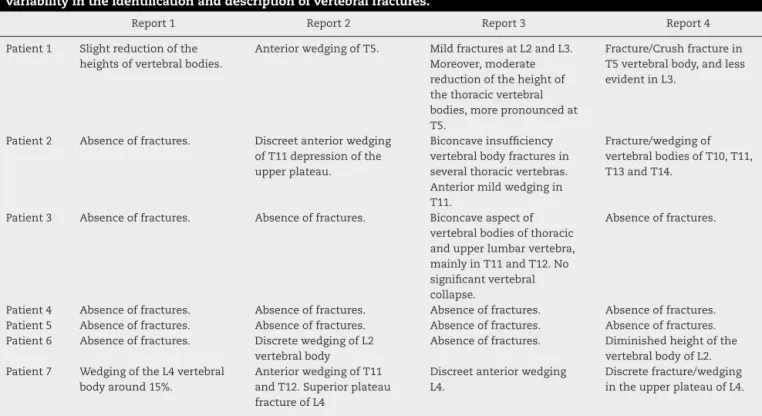
rev bras reumatol.2015;55(5):464–467Table1–RadiologyreportsofspineX-raysby4radiologistsin7womenwithosteoporosis.Thisshowsmarked variabilityintheidentificationanddescriptionofvertebralfractures.
Report1 Report2 Report3 Report4
Patient1 Slightreductionofthe heightsofvertebralbodies.
AnteriorwedgingofT5. MildfracturesatL2andL3. Moreover,moderate reductionoftheheightof thethoracicvertebral bodies,morepronouncedat T5.
Fracture/Crushfracturein T5vertebralbody,andless evidentinL3.
Patient2 Absenceoffractures. Discreetanteriorwedging ofT11depressionofthe upperplateau.
Biconcaveinsufficiency vertebralbodyfracturesin severalthoracicvertebras. Anteriormildwedgingin T11.
Fracture/wedgingof vertebralbodiesofT10,T11, T13andT14.
Patient3 Absenceoffractures. Absenceoffractures. Biconcaveaspectof vertebralbodiesofthoracic andupperlumbarvertebra, mainlyinT11andT12.No significantvertebral collapse.
Absenceoffractures.
Patient4 Absenceoffractures. Absenceoffractures. Absenceoffractures. Absenceoffractures. Patient5 Absenceoffractures. Absenceoffractures. Absenceoffractures. Absenceoffractures. Patient6 Absenceoffractures. DiscretewedgingofL2
vertebralbody
Absenceoffractures. Diminishedheightofthe vertebralbodyofL2. Patient7 WedgingoftheL4vertebral
bodyaround15%.
AnteriorwedgingofT11 andT12.Superiorplateau fractureofL4
Discreetanteriorwedging L4.
Discretefracture/wedging intheupperplateauofL4.
ofvertebralfractureisthroughspineX-rays,ideallyfollowed byevaluationandappropriatetherapytoreducetheriskof futurefractures.Effectivetherapiesarewidelyavailableand canreducetheoccurrenceoffuturevertebralfracturesby30% to70%.However,inspiteofvertebral fractures beingquite commonand associatedwithdecreased qualityoflifeand increasedmortality, they are often unreportedor misdiag-nosedbyradiologists.1,12
Inarecentretrospectivestudyof934womenage60years and older,therewas radiographicevidence ofmoderateor severevertebral fracturesin132(14%), butonly50%ofthe radiological reportsmentioned thesefractures.6 Inanother
study of 2000 postmenopausal women with osteoporosis, theaccuracyofspineX-rayinterpretationswasassessedby comparing the results oflocal radiographic reports with a radiographic central laboratory.8 This study showed
false-negative rates between 27 and 45 percent for diagnosing vertebralfractures.8Inaddition,whenavertebraldeformity
wasidentified,ambiguousterminologywasoftenusedinthe reports,leadingtopotentialconfusionindiagnosingvertebral fractures.6,8Despitethesmallnumberofpatients,ourresults
aresimilartotheinternationalliterature.13 Thisisthefirst
studyaddressingmissedopportunitiesfordiagnosing verte-bralfracturesinBrazil.
Conclusion
Thisstudy showsgreatvariability intheidentification and descriptionofvertebralfracturesinpostmenopausalwomen withosteoporosis.Clinicianswhorelyonaccuratereporting byradiologistsmayinturnmanagetheirpatientsdifferently dependingonwhichreportisreceived.Whenavertebral frac-tureisnotrecognizedorwhen adescriptionofavertebral
deformityisnotclear,thendecisionsforevaluatingand treat-ingpatientsmaybeincorrect.Improvementintheaccuracy and consistency ofreportingvertebral fractures islikelyto improvepatientcare.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgment
Wewouldliketothanktheradiologistswhowerewillingto assess theradiographsperformed,Bruno L.B.Cherulli,Elisa CristinaDias,PriscillaPiuzanaNogueira,SérgioVianaandthe doctorLudmillaPavlikHaddadforcollaboration.
r
e
f
e
r
e
n
c
e
s
1.KanisJA,JohanssonH,OdenA,JohnellO,DeLaetC,Eisman JA,etal.Afamilyhistoryoffractureandfracturerisk:a meta-analysis.Bone.2004;35:1029–37.
2.BandeiraFA,CarvalhoEF.Prevalênciadeosteoporosee fraturasvertebraisemmulheresnapós-menopausa atendidasemservic¸osdereferência.RevBrasEpidemiol. 2007;10:86–98.
3.VanStaaTP,DennisonEM,LeufkensHE,CooperC. EpidemiologyoffracturesinEnglandandWales.Bone. 2001;29:517–22.
4.SamelsonEJ,HannanMT,ZhangY,GenantHK,FelsonDT,Kiel DP.Incidenceandriskfactorsforvertebralfractureinwomen andmen:25-yearfollow-upresultsfromthe
rev bras reumatol.2015;55(5):464–467
467
5. NeerRM,ArnaudCD,ZanchettaJR,PrinceR,GaichGA, ReginsterJY,etal.Effectofparathyroidhormone(1–34)on fracturesandbonemineraldensityinpostmenopausal womenwithosteoporosis.NEnglJMed.2001;344:1434–41.
6. GenantHK,LenchikL,RogersLF,DelmasPD.Diagnosisof osteoporoticvertebralfractures:importanceofrecognition anddescriptionbyradiologists.AmJRoentgenol.
2004;183:949–58.
7. LindsayR,SilvermanSL,CooperC,HanleyDA,BartonI,Broy SB,etal.Riskofnewvertebralfractureintheyearfollowinga fracture.JAMA.2001;285:320–3.
8. DelmasPD,VandeLangerijtL,WattsNB,EastellR,GenantH, GrauerA,etal.Underdiagnosisofvertebralfracturesisa worldwideproblem:theImpactStudy.JBoneMinerRes. 2005;20:557–63.
9. SamelsonEJ,CupplesLA,BroeKE,HannanMT,O’DonnellCJ, KielDP.Vascularcalcificationinmiddleageandlong-term
riskofhipfracture:theFraminghamStudy.JBoneMinerRes. 2007;22:1449–54.
10.MajumdarSR,KimN,ColmanI,ChahalAM,RaymondG,Jen H,etal.Incidentalvertebralfracturesdiscoveredwithchest radiographyintheemergencydepartment:prevalence, recognition,andosteoporosismanagementinacohortof elderlypatients.ArchInternMed.2005;165:905–9.
11.KanisJA.WHOTechnicalReport.Sheffield:Universityof Sheffield;2007.p.66.
12.ClarkP,Cons-MolinaF,RagiS,DelezeM,HaddockL, ZanchettaJ,etal.Theprevalenceofvertebralfracturesin LatinAmericancountries:theLatinAmericanVertebral OsteoporosisStudy(Lavos).OsteoporosInt.2009;20:275–82.
13.BurgeR,Dawson-HughesB,SolomonDH,WongJB,KingA, TostesonA.Incidenceandeconomicburdenof