SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Primary
and
secondary
osteoporotic
fractures
prophylaxis:
evaluation
of
a
prospective
cohort
夽
Bruno
Gonc¸alves
Schröder
e
Souza
a,b,∗,
Luiz
Guilherme
Vidal
Assad
de
Carvalho
b,
Luiz
Felippe
Mokdeci
Martins
de
Oliveira
a,
Anmy
Gil
Ferreira
a,
Rita
de
Cássia
Santana
do
Amaral
a,
Valdeci
Manoel
de
Oliveira
a,baFaculdadedeCiênciasMédicasedaSaúdedeJuizdeFora(Suprema),JuizdeFora,MG,Brazil
bHospitaleMaternidadeTerezinhadeJesus,Servic¸odeOrtopediaeTraumatologia,JuizdeFora,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received17August2016 Accepted1September2016 Availableonline25August2017
Keywords:
Osteoporosis/epidemiology Osteoporosis/therapy Fractures,bone/epidemiology Fractures,bone/prevention& control
Primaryprevention Secondaryprevention Riskfactors
a
b
s
t
r
a
c
t
Objective:Tomeasuretheprevalenceofprimarydrugpreventionoffracturesdueto osteo-porosisinpatientsadmittedtoatertiaryteachinghospital,inamedium-sizedcity,admitted withosteoporoticfractures.Moreover,toidentifytheincidenceofprescribingsecondary pro-phylaxisafterthefirstfractureevent.Atthesametime,theprevalenceofriskfactorsfor suchfracturesasdescribedintheliteraturewasmeasured.
Methods:Thislongitudinalprospectivestudywasbasedonacohortofpatientsadmittedin atertiaryteachinghospitalfromOctober2015toJanuary2016.Patientswithlowenergyor fragilityfractureswereincludedinthestudyregardlessofgenderorrace,overtheageof 50years.Allpatientswhodidnothavethesecharacteristicswereexcluded.Thefollow-up lastedfourmonths.Serialquestionnaireswereappliedatadmissionandinthefollow-up consultationsatfourtoeightweeksandat16weeks.
Results:Onlyonepatientreportedreceivingtreatmentwithspecificdrugsforthedisease beforehospitaladmission,resultinginaprevalenceofprimarychemoprophylaxisofonly 2.27%.Nopatientwasprescribedmedicationforthetreatmentofosteoporosisafterthe fracture.Theprevalenceofriskfactorswassimilartothosefoundintheliteraturereview. Conclusion:In thepresent study,the frequency ofprimary and secondary osteoporosis chemoprophylaxisinpatientswhowereadmittedwithfragilityfractureswaslow,aswell astheearlyindicationofdrugtreatmentafterthefirstfracture.Theprevalenceoffragility fractureriskfactorsissimilartothosereportedintheliterature.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
PaperdevelopedatHospitaleMaternidadeTerezinhadeJesus,NúcleodePesquisaemOrtopediaeTraumatologia,JuizdeFora,MG, Brazil.
∗ Correspondingauthor.
E-mail:[email protected](B.G.Souza). http://dx.doi.org/10.1016/j.rboe.2016.09.010
Profilaxia
primária
e
secundária
de
fraturas
osteoporóticas:
avaliac¸ão
de
uma
coorte
prospectiva
Palavras-chave:
Osteoporose/epidemiologia Osteoporose/terapia
Fraturasósseas/epidemiologia Fraturasósseas/prevenc¸ão& controle
Prevenc¸ãoprimária Prevenc¸ãosecundária Fatoresderisco
r
e
s
u
m
o
Objetivo: Mediraprevalênciadaprofilaxiamedicamentosaprimáriadefraturaspor osteo-poroseempacientesinternadosemumhospitalterciáriodeensino,emumacidadede médioporte,admitidoscomfraturasosteoporóticas.Alémdisso,identificaraincidênciade prescric¸ãodeprofilaxiamedicamentosasecundáriaapósoeventodaprimeirafratura. Par-alelamente,medimosaprevalênciadefatoresderiscoparafraturaporosteoporosedescritos naliteratura.
Método:Estudolongitudinaldeumacoorteprospectivadepacientesadmitidosemhospital terciáriodeensinodeoutubrode2015ajaneiro2016.Foramincluídospacientescom frat-urasdebaixaenergiaouporfragilidade,independentementedogêneroouetnia,acimade 50anos.Todosospacientesquenãoapresentavamessascaracterísticasforamexcluídos.O seguimentofoidequatromeses.Foramaplicadosquestionáriosseriadosnaadmissão,no retornocomquatroaoitosemanasecom16semanas.
Resultado:Somenteumpacientereferiuterrecebidotratamentocomdrogasespecíficaspara adoenc¸aantesdainternac¸ãohospitalar,oquerevelaumaprevalênciadequimioprofilaxia primáriadeapenas2,27%.Nenhumpacienterecebeuprescric¸ãoparatratamentoda osteo-poroseapósafratura.Aprevalênciadosfatoresderiscodefraturaseassemelhaàquela encontradanaliteratura.
Conclusão: A frequênciade quimioprofilaxiaprimáriae secundáriada osteoporoseem pacientesadmitidoscomfraturasporfragilidadeébaixaemnossomeio,assimcomoa indicac¸ãoprecoce detratamentomedicamentosoapósaprimeirafratura.Aprevalência dosfatoresderiscodefraturaporfragilidadeésemelhanteàquelacitadanaliteratura.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Osteoporosis (OP) is a chronic, progressive, osteometabolic diseasecharacterizedbyadecreaseinbonemineraldensity (BMD),and duetothe deteriorationofbone microarchitec-ture, leading to mechanical fragility and predisposition to spontaneousandtraumaticfractures.1,2Theestimatedworld predominanceis7%inmalesand17%infemales.3InBrazil,it accountsforabout10millioncasesperannum.3–5 Therisk offractures due to osteoporosis is higher in females, and increaseswithage;theyareassociatedwithhighratesof mor-bidityandmortality.6
Themostcommonsitesofinvolvementarethedistalend oftheradius,vertebrae,proximalfemur,proximalhumerus, proximaltibia,ankle,andpelvis.7Diagnosisandtherapeutic planningareperformedandbasedonBMD,whichisthebest predictoroffractures.8
Mostpatientspresentingwithosteoporoticfractureshave neverpreviouslyundergoneBMDmeasuring,asurprisingfact ifwetaketheepidemiologicaldataofOPintoaccount,and becauseitisaneasilypreventablecomplication.9 Theearly diagnosisandconsequenttreatmentofthediseasereducethe rateofmorbidityandmortality.10
Althoughthereisnoconsensusastowhoisresponsible forinitiatingsecondary prophylaxis afterthe first fracture, anyphysicianwhoevaluatesthispatientshouldconsiderthe
multipletreatmentoptions.10,11Thetimingforhospitalization duetoafractureisagreatopportunityforpatientsandtheir familiestobeawareofthediseaseandoftheimportanceof thetherapeuticintervention,sincethepresenceofafracture inafragileboneisasufficientfactorforthediagnosisofOP, regardlessofothertests.10 Secondary pharmacological pro-phylaxis(preventionofnewfractures)canbeperformedwith theuseofdifferentdrugs,withsomebeingavailableinthe BrazilianPublicHealthSystem(SUS).11
Theobjectivesofthisstudy were tomeasurethe preva-lenceofprimarydrugprophylaxisofosteoporosisinpatients admittedtoatertiary teachinghospitalinamedium-sized city,admittedwithosteoporoticfractures.Inaddition,to iden-tifytheincidenceofprescriptionforsecondaryprophylaxisof fracturesaftertheeventofthefirstfracture.Atthesametime, wemeasuredinoursampletheprevalenceofknownfracture riskfactorsintheliterature.
Methodology
Table1–Demographiccharacteristicsofpatients attendedwithosteoporoticfracture.
Characteristic Type Prevalence
Gender Female 31patients
Male 13patients
Age 69.09±10.93years
Ethnicity White 30patients
Black 5patients Brown 9patients
BMI 25.12±4.83
Historyofsmoking 18patients(40.9%)
Historyofalcoholism 11patients(25%)
Boneaffected Femur 12patients(27.2%)
Radius 10patients(22.7%) Humerus 9patients(20.4%) Tibia 5patients(11.3%) Ankle 4patients(36.4%)
Ulna 2patients(4.5%)
Fibula 1patient(2.3%) Scaphoid 1patient(2.3%)
fractures. Patients who did not fit this description were excluded. Thefollow-up wasoffour months.However,the patientsareindefinitelyfollowedatthemedicalfacility.
Atadmission,aquestionnairewas usedtoevaluatethe sociodemographicdata,thefactorsdescribedintheliterature asriskforOP,andprioruseofdrugstotreatOP(Table1).In addition,theBrazilianversionoftheQualityofLife Question-naire-SF36,theTegnerActivityLevelScale,theOsteoporosis AssessmentQuestionnaire–PhysicalFunction,andtheFall RiskScorewereapplied.
Thepatientswere reassessedintwomoments:between four and eightweeks, and in the 16thweekafter hospital discharge.Ontheseoccasions,questionnairesdevelopedby theresearcherswereappliedwiththeobjectiveofevaluating thefrequencyofmedicalrecommendationforsecondary pro-phylaxisoffractures.Additionally,ontheultimatevisit,we repeatedtheapplicationoftheSF-36questionnaire.
Theresultsarepresentedasdescriptivestatisticsafterthey weretabulatedandtreatedonMicrosoftExcel2013and com-paredonGraphInstat3.0.
Results
Table1showsthemaincharacteristicsofthesampleofthe44 patientsstudied,31femalesand13males.Themeanagewas 69.09years(sd=±10.93),thebodymassindexwas25.12kg/m2
(sd=±4.83kg/m2)and,accordingtothe self-declaredethnic
group,30 were white,fiveblackand nine brown;18 had a history of smoking (40.9%), and 11 had a history of alco-holism(25%).Amongthewomenevaluated(n=31),30(96.8%) hadalreadyreachedmenopause,eight(25.8%)reporteduse ofhormonalcontraceptiveduringmenacme,andthree(10%) underwenthormonereplacementtherapy.
Whenquestionedaboutphysicalactivitypractice, accord-ingtotheTegnerActivityLevelScale(0–10),fourwereranked atlevel0,sixat1,15at2,11at3,1at4and5at5(mean=2.3, sd=±1.4,n=42)(Fig.1).
On admission, the patients were classified according to thelevelofdifficultytoperformactivitiessevendaysbefore
Frequency of drug use
Others
Insulin
Anticoagulant agent
Antiplatelet agent
Anticonvulsants
Hypoglycemic agents
Statins
Anxiolytic agents
Antidepressants
Diuretic agents
0 5 10 15 20 25 30
Anti-hypertensive agents
Fig.1–Druguseprevalenceinpatients.
Table2–Averagescoreoftheosteoporosisassessment.
OAQ-SF Dimensions Mean(standard
deviation)
Levelofdifficultyto developactivities
Mobility 8.79(6.82)
Physicalposition 11.47±8.15
Transfer 6.84±5.16
having an osteoporotic fracture, according to the scale of OsteoporosisAssessmentQuestionnaire–PhysicalFunction (OAQ-PF),inascaleof15to90,wherelowervaluesindicate greaterfunction.Threeitemsareconsidered:mobility(scale from5to30),physicalposition(from6to36)andtransfer(from 4to24).TheOAQ-PFwasonaverage24.7(sd=±16.9)andthe scoresonthesesubitemsarepresentedinTable2.
Regardingambulation,37weresocial(community) ambu-lators, four were household ambulators, one was a non-functional ambulator, and two were bedridden. Regarding household,35lived withtheirfamily,ninealone,andnone wereinstitutionalized.
Regarding theFallRiskScore(0to10,increasing accord-ingtoseverity),aquestionnaireassessingtheriskforfallsto whichthepatientisexposed,themean was2.45(sd=1.83); 18participantsreportedfrequentfallsand16reportedhaving sufferedpreviousfractures.
Comorbidities were reported by 38 patients (92.6%), the most prevalent being systemic arterialhypertension (59%), dyslipidemiaanddepression(20.4%each).Thedrugsinuse bythepatientsarelistedinFig.2.
RegardingthediagnosisandpreviousinvestigationofOP, only four patients had performed bone densitometry, the diagnosis ofwhichwasosteopenia intwo cases(2.5%) and osteoporosisintheothertwo(2.5%)(Fig.3).
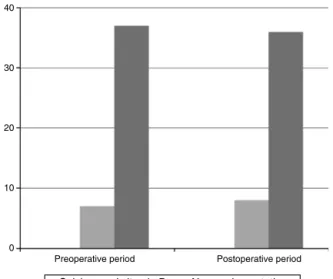
Before the fracture, seven subjects were supplemented withcalciumand/orvitaminD,andofthese,onlythreekept supplementationduringthefollow-upperiod.Followingthe fracture, five people started using calcium and vitamin D supplementation(Fig.4).
16
Level 0 Level 1 Level 2 Level 3 Level 4 Level 5 12
8
4
0
Fig.2–Frequencydistributionofphysicalactivitylevels accordingtoTegnerActivityScale.
BMD investigation before fracture
OSTEOPENIA 2
2
40
OSTEOPOROSIS
Without previous BMD
Fig.3–Frequencyofpreviousinvestigationanddiagnosis ofosteoporosiswithBMD.
patientsreportedbeingadvisedaboutthediseaseandthree ontheneedforBMDinvestigation.
Ofthe44patients,onedidnotcompletethelastfollow-up, duetoclinicalcomplications,withprolongedhospitalization in aIntensive CareUnit (ICU), which prevented him from answeringthequestionnaires.There werealsosevencases ofdeath,allover60yearsofage,sixhospitalizedforfemur
40
Preoperative period Postoperative period 30
20
10
0
Calcium and vitamin D No supplementation
Fig.4–PrevalenceoftheuseofcalciumandvitaminD beforeandafterthefracture.
60
48
36
24
12
0
Preoperative period Postoperative period
Physical component Mental component
Fig.5–GraphiccomparingqualityoflifebytheSF36before thefractureandafter16weeks.
fractureandonefordistalradiusfracture.Thus,themortality rateafterfragilityfracturesinthepresentstudywas15.9%.
The scores of Quality of Life Questionnaire – SF 36 on admissiontothehospitalwere47.11(sd=7.55)forthephysical component, and 46.56 (sd=6.76) for the mental compo-nent. At the ultimate visit, the physical component was 39.69(sd=18.33)and37.37(sd=18.68)forthemental compo-nent.Therefore,fracturetreatmentprovidedimprovementin patients’qualityoflife(p=0.019)inashortperiodoftime(four months)(Fig.5).
Discussion
Bone fragility fractures can be considered a public health problem,withanestimatedannualincidenceof3%inwomen aged at least 85 years, in the proportion of 3:1 compared tomen,11,12 withadirectcosttoBrazil’sPublicHealth Sys-tem of approximately 30 million dollars annually.3,13 This diseasepreventionisofparamountimportance,sinceitcan improveapatient’squalityoflife,aswellasreducemorbidity andmortality.14Inaddition,theepidemiologicaltransitionto theBrazilianpopulation,withtheincreaseinthenumberof elderlypeople,impliestheneedtocreatestrategiesto con-troltheriskofprimaryandsecondaryfractures.15Ourstudy evaluatedaspecificpopulationandfoundanepidemiological profilesimilartoothersintheliterature.Baronetal.16founda predominanceofthistypeoffractureamongthosebetween50 and70years,especiallyinfemalesaftermenacme.The inci-denceofnon-vertebralfracturesinseveralstudiesishigherin thefemur,radiusandhumerus,17similartoourstudy.
havealsoreportedthisobservation,attributingtheriskfactor forfragilityfracturestothisaspect.11
Other recognized risk factors for fragility fractures are: smoking,sedentarylifestyle,lowweight,previousfractures, alcohol,frequentfalls,amongothers.5 Infact, ourfindings show a higher prevalence ofsmoking amongour patients comparedtotheBrazilianaverage.15Likewise,frequent alco-holusewasreportedby25%ofthepatients,differentlyfrom thenationalaverage,whichaccordingtoBrazilianInstituteof GeographyandStatistics(IBGE)was14.2%in2013.15
Toassessthelevelofphysicalactivityofthepatientsbefore the fracture, a validated scale of level of physical activity –Tegner Activity LevelScale– wasused, and according to theresult,sedentarylifestylewasdemonstratedinthe admit-tedpatients.Pinheiroetal.4showthatsedentarylifestyleis amongthemainriskfactorsforlowimpactfracturesinboth genders,whichmayberelatedtopoorbonequality,aswell aslower neuromuscularcontrol(withahigherincidenceof falls).17
Theuse ofmultiplemedications inelderlypatientswas relatedtoahigherincidenceoffractures.18Theincidenceof falls, whichmay be influencedby the useof certain med-ications and associated diseases, was 40.9% in our study. AccordingtoPluijmet al.,19 evenafterdrugadaptationsto reducedizziness,vertigoandposturalhypotension,suchas antivertigos,anticonvulsants,antidepressants and benzodi-azepines, the number of fallscontinues to bea predictive factorfortheoccurrenceoffractures.
Arecentmeta-analysistodeterminetheriskoffractures inpsychotropicdrugusershasshownthatbenzodiazepines, antidepressants, non-barbiturate anticonvulsants, barbitu-rateanticonvulsants, antipsychotics,hypnoticsand opioids areassociatedwithincreasedriskoffractures.18Accordingto thesedata,werecorded18%ofanxiolyticdruguse,27.27%of antidepressantsuse,and6.81%ofanticonvulsants,or86.36% ofpatientswithassociateddiseasesorinchronicuseofsome medication.Wealsoobservedahighprevalenceofpatients takingantihypertensivedrugs(61.36%)anddiuretics(38.63%). Oatesetal.20statethatsomeantihypertensivedrugshavea negativeinotropichearteffect,whichisusuallycompensated byanincreaseinadrenergiccardiacstimulationto compen-satehypotension.Inelderlyindividuals,thisreflexisusually reduced,andmayleadtoanincreasedriskofhypotension, and increase the risk of falls.20 The relation between the useofdiuretics andthe increasedincidenceoffractures is still controversial.20 While LaCroix et al.21 defenda possi-bleprotectiveeffectofthiazidediureticsduetoareduction in urinary calcium excretion, with consequent increase in bonedensity,Cummings22attributesthehighestriskoffalls tohypokalemia, arrhythmiasand posturalhypotension.In general,ourfindings corroboratethose ofDaniachietal.,14 thatfoundafrequencyof85.84%forassociateddiseases,and 80.53%forchronicuseofmedication.
Theprevention of fractures due to osteoporosis should beginatpubertythrough theencouragementofsportsand balanced nutrition, aiming to reach an adequate peak of bonemass.23,24 However,the screeningforbonemass loss throughbonedensitometryisindicatedinpremenopausefor women,andinelderlymen,sincethetreatmentofosteopenia andosteoporosiscanreducetheincidenceoffractures due
to fragility, that is, it functions as primary drug fracture prophylaxis.25,26
Inourstudy,inaconveniencesample,probably represen-tativeofthecasesoffractureinourcity,weobservedthatthe prevalenceofprimaryprophylaxisoffracturesisminimal(one patient).
Weobservedalowfrequencyofindicationofsecondary fracture prophylaxis (beginning of treatmentafter the first fracture) in our cohort. Stolnicki and Oliveira13 say that a second episode offracture may occurwithina short inter-val,especiallyduringthefirstyear.Theearlierthesecondary drugprophylaxisisestablished,thebetter,becausetherisk ofrecurrencedecreases30%to60%.13Initially,theaimofthe studywastoidentifypossiblefactorsrelatedtotheeventual failureofthisindication.Forthis,wecalculatedasampleof 100patientsandafollow-upofoneyear.However,because theintermediateanalysisofthedatademonstratedthatthe patientsdidnotreceivethenecessarycare,therewasaneedto interruptthestudyforethicalreasons,andweimplemented measurestocorrectthisdistortion.Inourhospital,the meas-uresincludedaseriesofeducationallecturesfororthopedists andresidentsinvolved,aswellasthecreationofareference clinicforthepreventionofsecondaryfractures,inspiredby programssuchasPrevfrat.13Theimpactsofthesemeasures will be evaluated in future studies. Nevertheless, we have decidedtopublishourfindings,becausewebelievethatthis scenarioisprobablypresentinseveralhospitalsinthecountry. Itispossiblethatstudieslikeours,repeatedinothercenters, willfindsimilarresultsandencouragethemtoadopt meas-uresthat,accordingtotheliterature,canhelpavoid60%ofnew fractures,significantlyreducemortality,andreducethecost forSUSofthetreatmentoffracturesduetobonefragility.13
Experiments in other centers around the world seem promising.TheHealthyBonesProgram,consideredthelargest bonefragilityfracturepreventionprogramintheworld,and aims to reduce the incidence of cases by 20% within five years,isoneofthemostimportantprojectsinthe fieldof primaryprophylaxis.13Inthescopeofsecondaryprophylaxis, the RefractivePreventionProgram(Prevrefrat)standsout,a projectdevelopedinBrazilfouryearsago,aworldreference pointforthepreventionofnewfractures.Sinceits implan-tation, afall ofmore than 97% ofnew fractures has been observedinthegroupthatwasbeingfollowed.13
Regarding the limitations of the study, the number of patients,thathadtobereducedduringfollow-up,andtime, arehighlighted.
Conclusions
ThefrequencyofprimaryandsecondaryOP chemoprophy-laxisinpatientsadmittedwithfragilityfracturesislowinour country,revealingtheneedtodevelopspecificstrategiesto addressthisdisease.Theprevalenceoffragilityfracturerisk factorsissimilartothatreportedintheliterature.
Conflicts
of
interest
r
e
f
e
r
e
n
c
e
s
1. BandeiraF,CarvalhoEF.Prevalênciadeosteoporoseefraturas vertebraisemmulheresnapós-menopausa.RevBras Epidemiol.2007;10(1):86–98.
2. KhajuriaDK,RazdamR,MahapatraDR.Medicamentospara prevenc¸ãodaosteoporose:revisão.RevBrasReumatol. 2011;51(4):365–82.
3. MoraesLFS,SilvaEN,SilvaDAS,PaulaAP.Gastoscomo tratamentodaosteoporoseemidososdoBrasil(2008-2010): análisedosfatoresassociados.RevBrasEpidemiol. 2014;17(3):719–34.
4. PinheiroMM,CastroCH,FrisoliAJr,SzejnfeldVL. Discriminatoryabilityofquantitativeultrasound
measurementsissimilartodual-energyX-rayabsorptiometry inaBrazilianwomenpopulationwithosteoporoticfracture. CalcifTissueInt.2003;73(6):555–64.
5. PinheiroMM,CiconelliRM,JacquesNO,GenaroPS,Martini LA,FerrazMB.OimpactodasosteoporosenoBrasil:dados regionaisdasfraturasemhomensemulheresadultos–The BrazilianOsteoporosisStudy(Brazos).RevBrasReumatol. 2010;50(2):113–27.
6. BaccaroLFC,PaivaLC,PintoNetoAM.Osteoporose.RevBras Med.2014;71(3):48–54.
7. GaliJC.Osteoporose.ActaOrtopBras.2001;9(2):3–12. 8. BlackDM,CummingsSR,GenantHK,NevittMC,PalermoL,
BrownerW.Axialandappendicularbonedensitypredict fractureinolderwomen.JBoneMinerRes.1992;7(6): 633–8.
9. PremaorMO,PilbrowL,TonkinC,ParkerRA,CompstonJ. Obesityandfracturesinpostmenopausalwomen.JBone MinerRes.2010;25(2):292–7.
10.KiebzakGM,BeinartGA,PerserK,AmbroseCG,SiffSJ, HeggenessMH.Undertreatmentofosteoporosisinmenwith hipfracture.ArchInternMed.2002;162(19):2217–22.
11.PintoNetoAM,SoaresA,UrbanetzAA,SouzaACA,Ferrari AM,AmaralB,etal.Consensobrasileirodeosteoporose2002. RevBrasReumatol.2002;42(6):343–54.
12.KanisJA,JohnellO,OdenA,JohanssonH,McCloskeyE.FRAX andtheassessmentoffractureprobabilityinmenand womenfromtheUK.OsteoporosInt.2008;19(4):385–97.
13.StolnickiB,OliveiraLG.Forthefirstfracturetobethelast.Rev BrasOrtop.2016;51(2):121–6.
14.DaniachiD,NettoAS,OnoNK,GuimarãesRP,PoleselloGC, HondaEK.Epidemiologiadasfraturasdoterc¸oproximaldo fêmurempacientesidosos.RevBrasOrtop.2015;50(4):371–7. 15.InstitutoBrasileirodeGeografia,Estatística.Pesquisa
NacionaldaSaúde2013–Percepc¸ãodoestadodesaúde, estilosdevidaedoenc¸ascrônicas.RiodeJaneiro:IBGE;2014. 16.BaronJA,BarrettJA,KaragasMR.Theepidemiologyof
peripheralfractures.Bone.1996;183Suppl:209S–13S. 17.SouzaMPG.Diagnósticoetratamentodaosteoporose.Rev
BrasOrtop.2010;45(3):220–9.
18.TakkoucheB,Montes-MartinezA,GillSS,EtminanM. Psychotropicmedicationsandtheriskoffracture:a meta-analysis.DrugSaf.2007;30(2):171–84.
19.PluijmSM,SmitJH,TrompEA,StelVS,DeegDJ,BouterLM, etal.Ariskprofileforidentifyingcommunity-dwelling elderlywithahighriskofrecurrentfalling:resultsofa3-year prospectivestudy.OsteoporosInt.2006;17(3):417–25.
20.OatesJA,BrownNJ.Antihypertensiveagentsandthedrug therapyofhypertension.In:HardmanJG,LimbLE,editors. Goodman&Gilman’sthepharmacologicalbasisof therapeutics.10thed.NewYork:McGraw-Hill;2001.p. 871–900.
21.LacroixAZ,WienpahlJ,WriteLR,WallaceRB,ScherrPA, GeorgeLK,etal.Thiazidediureticagentsandtheincidenceof hipfracture.NEnglJMed.1990;322(5):286–90.
22.CummingsSR.Epidemiologicstudiesofosteoporotic fractures:methodologicissues.CalcifTissueInt.1991;49 Suppl:S15–20.
23.JongMR,ElstMV,Hartholt.Drug-relatedfallsinolder patients:implicateddrugs,consequencesandpossible preventionstrategies.TherAdvDrugSaf.2013;4(4):147–54. 24.RossiniM,AdamiS,BertoldoF,DiacintiD,GattiD,GianniniS,
etal.Guidelinesfordiagnosis,preventionandmanagement ofosteoporosis.Reumatismo.2016;68(1):1–39.
25.SampaioPRL,BezerraAJC,GomesL.Aosteoporoseea mulherenvelhecida:fatoresderisco.RevBrasGeriatr Gerontol.2011;14(3):295–302.