www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Auditory
and
language
skills
of
children
using
hearing
aids
夽
Leticia
Macedo
Penna
∗,
Stela
Maris
Aguiar
Lemos,
Cláudia
Regina
Lindgren
Alves
UniversidadeFederaldeMinasGerais(UFMG),BeloHorizonte,MG,Brazil
Received10November2013;accepted12May2014 Availableonline18October2014
KEYWORDS
Hearingloss; Childlanguage; Hearingaids; Auditoryperception; Correctionofhearing impairment
Abstract
Introduction:Hearinglossmayimpairthedevelopmentofachild.Therehabilitationprocess forindividualswithhearinglossdependsoneffectiveinterventions.
Objective:Todescribethelinguisticprofileandthehearingskillsofchildrenusinghearingaids, tocharacterize therehabilitationprocess andtoanalyze itsassociationwiththe children’s degreeofhearingloss.
Methods:Cross-sectionalstudywithanon-probabilisticsampleof110childrenusinghearing aids(6---10yearsofage)formildtoprofoundhearingloss.Testsoflanguage,speech percep-tion,phonemicdiscrimination,andschoolperformancewereperformed.Theassociationswere verifiedbythefollowingtests:chi-squaredforlineartrendandKruskal---Wallis.
Results:About65%ofthechildrenhadalteredvocabulary,whereas89%and94%hadaltered phonologyandinferiorschoolperformance,respectively.Thedegreeofhearinglosswas asso-ciatedwithdifferencesinthemedianageofdiagnosis;theageatwhichthehearingaidswere adaptedandatwhichspeechtherapywasstarted;andtheperformanceonauditorytestsand thetypeofcommunicationused.
Conclusion:Thediagnosisofhearinglossandtheclinicalinterventionsoccurredlate, contribut-ingtoimpairmentsinauditoryandlanguagedevelopment.
© 2014Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
夽
Pleasecitethisarticleas:PennaLM,LemosSM,AlvesCR.Auditoryandlanguageskillsofchildrenusinghearingaids.BrazJ Otorhino-laryngol.2015;81:148---57.
∗Correspondingauthor.
E-mail:[email protected](L.M.Penna).
http://dx.doi.org/10.1016/j.bjorl.2014.05.034
1808-8694/©2014Associac¸ãoBrasileiradeOtorrinolaringologia eCirurgiaCérvico-Facial. PublishedbyElsevierEditoraLtda.All rights
PALAVRAS-CHAVE
Perdaauditiva; Linguageminfantil; Auxiliaresdeaudic¸ão; Percepc¸ãoauditiva; Correc¸ãode deficiênciaauditiva
Habilidadeslinguísticaseauditivasdecrianc¸asusuáriasdeaparelhoauditivo
Resumo
Introduc¸ão: Adeficiênciaauditivapodecomprometerodesenvolvimentoinfantil.Oprocesso dereabilitac¸ãodosindivíduoscomperdaauditivadependedeintervenc¸õeseficientes.
Objetivo: DescreveroperfillinguísticoeashabilidadesauditivasdeusuáriosdeAparelhode Amplificac¸ãoSonoraIndividual(AASI),caracterizaroprocessodeintervenc¸ãofonoaudiológica eanalisarsuarelac¸ãocomograudaperdaauditivadascrianc¸as.
Método: Estudotransversalcomamostranão-probabilísticacompostapor110crianc¸asde6a10 anosdeidade,comperdaauditivadegrauleveaprofundo,usuáriasdeAASI.Foramrealizados testes de linguagem,percepc¸ão de fala, discriminac¸ão fonêmica e desempenho escolar.As associac¸õesforamverificadaspelostestes2detendêncialineareKruskal-Wallis.
Resultados: Cercade65%dascrianc¸asapresentavamalterac¸ãodovocabulário,89%defonologia e94%tiveramdesempenhoescolarconsideradoinferior.Ograudaperdaauditivamostrou-se associadoadiferenc¸asnasmedianasdasidadesdediagnóstico,deadaptac¸ãodoAASIedeinício dafonoterapia;dotempoentrediagnósticoeadaptac¸ãodoaparelhoauditivo;aoresultadodos testesauditivoseaotipodecomunicac¸ãoutilizada.
Conclusão:Independentemente dograu de perdaauditiva, odiagnóstico e as intervenc¸ões necessáriasocorreramtardiamente,comprejuízodashabilidadeslinguísticaseauditivasdestas crianc¸as.
©2014Associac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicado por ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Hearinglossisahigh-prevalencedisease,rangingfromone tothreeper1000individuals;thisnumberincreasesinthe presenceofriskfactorsforhearingimpairment.1,2Itsmain consequence, especiallyin children, is theimpactcaused bysensorydeprivationinthedevelopmentofauditoryand languageskillsandlearning.Anydegreeofhearinglosscan resultinsignificantdamage,asitinterfereswithperception andunderstandingofspeechsounds.3
Inthenationalscenario,duetothesocialmagnitudeof hearingimpairmentprevalenceanditsconsequencesinthe Brazilianpopulation,theMinistryofHealth4,5institutedthe HearingHealthCareServices(Servic¸osdeAtenc¸ãoàSaúde Auditiva ---SASA)which,togetherwiththeNeonatal Hear-ingScreeningProgram, haveasagoaltheearlydiagnosis, intervention,andrehabilitationofindividualswithhearing impairment.
The first years of life areconsidered critical for child development,as the peakof the central auditory system maturation process occurs during childhood and neuronal plasticityisat itsmaximum.6This makestheearly detec-tionofhearingimpairmentcrucialtominimizethedamaging impactonthedevelopmentoflanguageandlisteningskills, aswellasonthelearningprocesscausedbyhearingloss.6---11 In addition to an early diagnosis, the literature also points out the importance of interventional speech ther-apyinthesuccessfulrehabilitationofchildrenwithhearing impairment.6,7Theearlierthediagnosis isestablishedand auditory speech therapy is initiated, the closer develop-mentofaffectedchildrenwillbetothatofnormalhearing children.9,11
Thus,thisstudyaimedtodescribetheoral andwritten linguistic profile and auditory skills of children using an
individualsound amplification device (ISAD), fitted in the period2008---2010inaSASA,andtocharacterizetheprocess ofspeechtherapy interventionandanalyzeitsassociation withthedegreeofhearinglossofthechildren.
Methods
This wasa cross-sectional,observational study conducted inahigh-complexitySASAinBeloHorizonte,stateofMinas Gerais,Brazil,fromSeptemberof2011toMayof2012.
After data collectionfrom the service’s database, 206 childrentreatedintheyears2008---2010,whohadan audi-tory diagnosis confirmed through pure tone and speech audiometryassessment,wereidentified.
Exclusion criteria included normal hearing, history of otorhinolaryngological surgery, treatment abandonment, transfertoanotherSASA,presenceofsyndromesand asso-ciated neurological alterations, and death; the eligible populationconsistedof131children.Ofthese,sevencould notbelocatedand14didnotattendtheevaluation.Thus, thepopulationconsistedof110individuals.
All110childrenwereassessedindividuallyfor language and auditory skills, and during the evaluation they used theISAD.Theevaluationwasperformedinasinglesession lastingan averageof1h.Parentsorguardiansanswereda structuredquestionnaireaimedtocharacterizethesample, withthefollowing thematicaxes:riskindicators for hear-ingloss at birth, dataon auditory diagnosis, intervention andspeechtherapy/audiologicalfollow-up,schoollife,and socioeconomicindicators.
vocabulary,fluency,andpragmatics.Thisresearchusedthe phonologyandvocabularytasks.Onlyorallycommunicative children(n=80)wereabletoperformthesetests.
Forthevocabularytest, therecordingofthechildren’s responses immediately followed thenaming, inindividual sheets,andthecriteriaestablishedbythetestauthorwere followedfortheanalysis.13,14
Forthephonologyassessment,thisstudyusedthe sponta-neousnamingtask.Therecordingofresponseswascarried outwitha Cassio® Exilimdigital camera, in movie mode. Afterlistening tothe file, the phonetic transcription and analysisofresponseswereperformed.Therecordingofone childwithmoderatelyseveretoseverehearinglossdegree couldnotberecovered.Thecriteriaestablishedbythetest authorwerefollowedfortheanalysis.15
TheSchoolPerformanceTest(SPT)wasusedtoevaluate thewritten language16;itwasdevelopedforevaluationof schoolchildrenfromthefirsttothesixthgradeofelementary school.Itconsistsofthreesubtests:writing,arithmetic,and reading.ThefinalclassificationoftheSPTandofeach sub-testwasperformedasdescribedbytheauthorofthetool.17 Toanalyzetheresults ofSPTtest inthe firstgraders,the middle-lowerandmiddle-upperclassificationsweregrouped inthe‘‘medium’’category.
Twoprotocolswereusedtoevaluatehearingskills:the GlendonaldAuditoryScreeningProcedure(GASP)18 andthe phonemediscriminationtestwithfigures.19Thespeech per-ceptiontest --- GASP --- consists of fivetests thatevaluate thecapacityofdetectingLingsounds,voweldiscrimination, extension discrimination, word recognition, and compre-hensionofsentencesusingtheISAD.The testanalysiswas performed assuggested by the literature.18 This research also evaluated the overall test result by calculating the meansofalltestsinordertoanalyzetheoverallresultand compareindividuals.
Thephonemediscriminationtestwithfiguresassessesthe phonemic discrimination capacity through minimal pairs. The final score was classified as adequate or altered according to age, following the criteria proposed by the literature.19Azeroscorewasconsideredforthosechildren whowereunabletoperformthetest.
The analysis of the child’stype of communication was dividedintothreecategories:orallycommunicative,orally communicativeassociatedwiththeBrazilianSignLanguage (LínguaBrasileiradeSinais[LIBRAS];thechildcanexpress herselforally,butusesLIBRASwhenhe/shecannot commu-nicateeffectively), andnon-orallycommunicative(LIBRAS user exclusivelyand/or functional gestures), according to theanswergivenbytheparent/guardianonthe question-naire.
Theauditorydiagnosiswasmadeaccordingtothe crite-riaestablishedintheliteratureregardingdegreeandtype.20 Toanalyzethevariabledegreeofhearingloss,the diagno-sisinthebetterearwasconsideredandthechildrenwere divided into threegroups: mild tomoderate; moderately severetosevere,andprofoundbilateralhearingloss.This studyobservedchildrenwithsensorineural,conductive,and mixedhearinglossinallthreegroups.
Datawere storedin electronicfiles, withdoubleentry andcheckingoftheconsistencyofthedatabase.The statis-ticalpackageEpiInfo7.1.0.6wasusedfordataprocessing andanalysis.
Descriptive analysis of the frequency distribution of categorical variables and analysis of measures of central tendency anddispersionfor continuousvariableswas per-formed. The Kruskal---Wallis test was used to verify the association between the degree of hearing loss and the aspects of speech therapy intervention and auditory per-formanceintests.Thelevelofsignificancewassetat5%.
The chi-squared test for linear trend wasusedto ver-ifytheassociationbetweenthedegreeofhearinglossand thetypeof communicationused,comparingchildrenwith mild/moderatehearinglosstotheotherswithmore signifi-canthearingloss.
ThisstudywasapprovedbytheResearchEthics Commit-teeofUniversidadeFederaldeMinasGerais,underOpinion No.ETIC0316.0.203.000-10.Allparentsorguardiansofthe childrenparticipatinginthestudysignedtheinformed con-sent(IC).
Results
The main characteristics of the 110 childrenevaluated in thisstudyaredescribedinTable1.
Thedegreeofhearinglosswasmostfrequently moder-atelysevere/severe(43.7%).Themostfrequentaudiometric curve was downward sloping (56.3% in the RE and 53.6% in the LE). The median timeof hearing aid fitting of the childrenwas2.68years(range0.9---4.5years).
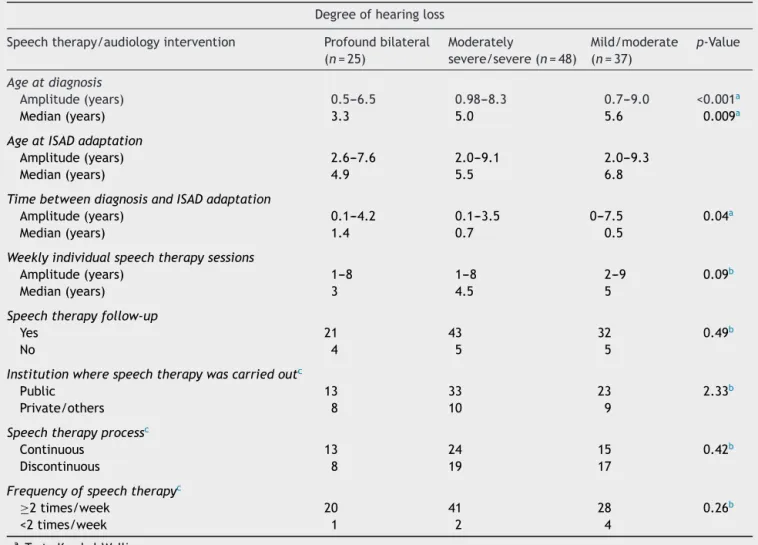
Table 2 describes aspects of the audiological/speech therapyintervention.
Therewasastatisticallysignificantdifferencebetween themedianagesatdiagnosis,ageathearingaidfitting,time betweendiagnosisandhearingaidfitting,andtheinitiation ofspeechtherapyaccordingtothedegreeofhearingloss.
Therewasno association between follow-upin speech therapy,thenumberofspeechtherapyconsultations, con-tinuity of the speech therapy process, and the type of institutionthechildrenattendedforspeechtherapy accord-ingtothedegreeofhearingloss.
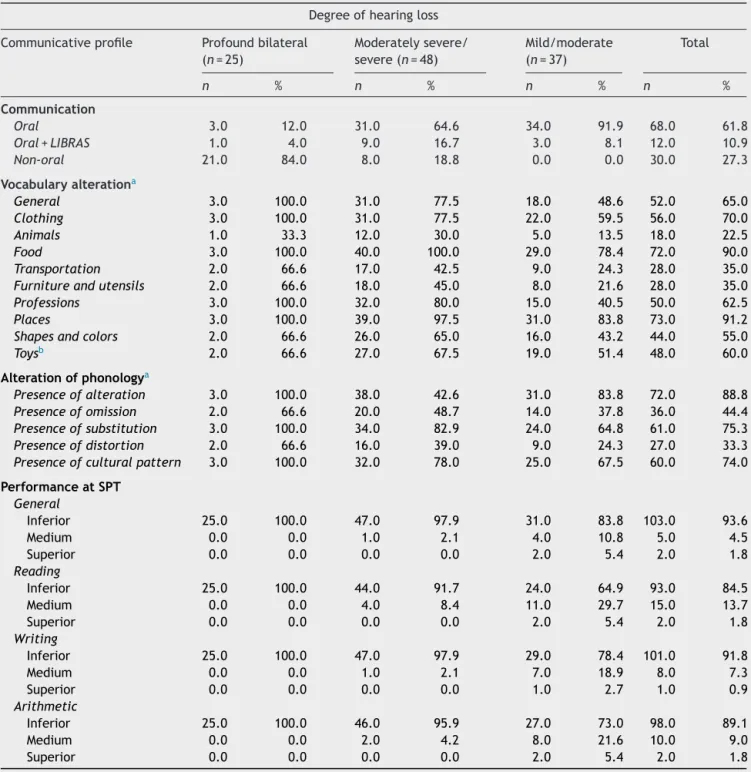
Thedistributionofthechildrenaccordingtothedegree ofhearinglossandthetypeofcommunicationused,andthe resultsoftheorallanguageandwritingtestsareshown in
Table3.
Regardinglanguage,65%ofthechildrenhadbelow nor-mal vocabulary and 88.8% had some abnormalities in the areaofphonology.
Table4showstheresultoftheassociationbetweenthe degreeofhearinglossandthetypeofcommunicationused bythechildrenwithhearingimpairment.
Therewasan association between thedegree of hear-inglossandthetypeofcommunicationusedbythechild. Theriskthatachildwithmoderatelysevere/severedegree of hearing loss would not use oral language to communi-catewas6.2timeshigherthanachildwithmild/moderate degreeofhearingloss;andtheriskofachildwithprofound bilateralhearinglossofnotusingorallanguageto communi-catewas83.1timeshigherthanachildwithmild/moderate degreeofhearingloss.
Table1 Generalcharacteristicsoftheassessedchildren andtheirfamilies.
Characteristic n %
Child’sgender
Female 42 38.2
Male 68 61.8
Child’sage
Mean±SD:8.5±1.5years 24 21.8 Median:8.5years 19 17.2 6years---7years 22 20.0 7years---8years 18 16.3 8years---9years 27 24.5 9years---10years
10years---11years
Typeofschool
Regularschool 92 83.6
Special-needsschool 18 16.4
Ageatschoolenrollment
Upto6years 100 90.9
After6years 6 5.4
Nodata 4 3.7
Appropriateagefortheschoolyear
Yes 41 37.3
No 69 62.7
TDEresult
Inferior 103 93.6
Medium 5 4.5
Superior 2 1.9
Maternalyearsofschooling
Mean±SD:7.8±3.4years/median8years 1 0.9
Illiterate 28 25.4
1---4yearsofschooling 30 27.2 5---8yearsofschooling 45 41.1 9---11yearsofschooling 3 2.7 Morethan11yearsofschooling
Noinformation
Percapitaincome
Upto1minimumwage 95 86.3 >1minimumwage 12 10.9
Noinformation 3 2.8
Presenceofriskindicatorforhearingloss
Yes 44 40
No 66 60
Degreeofhearingloss
Profoundbilateral 25 22.7 Moderatelysevere/severe 48 43.7
Mild/moderate 37 33.6
Typeofhearinglossintherightear
Sensorineural 104 94.5
Mixed 2 1.8
Conductive 3 2.8
Normalhearing 1 0.9
Table1(Continued)
Characteristic n %
Typeofhearinglossintheleftear
Sensorineural 104 94.5
Mixed 2 1.8
Conductive 3 2.8
Normalhearing 1 0.9
TimeofuseofISAD/day
Upto4h/day 14 12.7
From5to8h/day 37 33.7 Morethan8h/day 59 53.6
Discussion
Themean ageof thechildrenevaluatedin thisstudy was eightyearsandsixmonths;mostofthemattendedregular schoolandhadstartedschoolbeforeage6.Atthisage,the childisexpectedtobewell-adaptedatschoolandtohave acquiredanextensivevocabulary,toknowtherulesof syn-tax,andtohaveacquiredallspeechsounds.7,13,21However, most of the study children did not achieve the expected resultsinthephonologyandvocabularytest,regardlessof thedegreeofhearingloss.
The assessed children showed a prevalence of moder-atelysevere/severehearingloss,withadownwardsloping audiometriccurve.Thistypeofconfigurationcanresultin greatdeficitsin receptive andexpressive language, espe-ciallyin discrimination and recognition of speechsounds, particularlyfricativesounds.17,22
Regardingthetypeofhearingloss,thesensorineuraltype wasthemostoftenobservedinthisstudy.However,insome children,differenttypesofhearinglosswerefoundineach ear.In the sensorineural type, hearing loss is most often irreversibleandthegreaterinvolvementoccursatthelevel ofauditorycomprehension.23 Intheconductiveandmixed types, hearing fluctuation may hinder speech intelligibil-ity,and consequently, the child can develop phonological and auditory processing alterations, as well as learning difficulties.22
Inthegroupofchildrenwithprofoundbilateralhearing loss,theageattheauditorydiagnosis andtheageatISAD fitting were lower than in the other studied groups. This canbeexplainedbythefactthatprofound hearinglossis moreeasilyperceivedbythefamilyandhealthprofessionals involvedwiththechild.24Earlyreferralfavorstheprocessof diagnosisandthefittingoftheISADinatimelyandefficient manner.However,incasesofless severehearingloss,the child’sdifficultiescangoundetectedbyhealthprofessionals andthefamily,andareoftenobserved byteachersduring theemergenceoflearningdisabilities.6,23
Table2 Aspectsofspeechtherapyinterventionaccordingtothedegreeofhearingloss. Degreeofhearingloss
Speechtherapy/audiologyintervention Profoundbilateral (n=25)
Moderately
severe/severe(n=48)
Mild/moderate (n=37)
p-Value
Ageatdiagnosis
Amplitude(years) 0.5---6.5 0.98---8.3 0.7---9.0 <0.001a
Median(years) 3.3 5.0 5.6 0.009a
AgeatISADadaptation
Amplitude(years) 2.6---7.6 2.0---9.1 2.0---9.3
Median(years) 4.9 5.5 6.8
TimebetweendiagnosisandISADadaptation
Amplitude(years) 0.1---4.2 0.1---3.5 0---7.5 0.04a
Median(years) 1.4 0.7 0.5
Weeklyindividualspeechtherapysessions
Amplitude(years) 1---8 1---8 2---9 0.09b
Median(years) 3 4.5 5
Speechtherapyfollow-up
Yes 21 43 32 0.49b
No 4 5 5
Institutionwherespeechtherapywascarriedoutc
Public 13 33 23 2.33b
Private/others 8 10 9
Speechtherapyprocessc
Continuous 13 24 15 0.42b
Discontinuous 8 19 17
Frequencyofspeechtherapyc
≥2times/week 20 41 28 0.26b
<2times/week 1 2 4
aTesteKruskal-Wallis.
b TesteQuiQuadrado.
c Apenasascrianc¸asquerealizamfonoterapia.
numberofaudiologicaltestsrequiredforcompletionof diag-nosisinthesechildren.24
Inthisstudy,regardlessofthedegreeofhearingloss,age atdiagnosisandISADfittingoccurredlate,whichis in dis-agreementwithwhatisproposedintheliterature,i.e.,that theauditorydiagnosisshouldbeestablishedbeforethethird monthoflifeandspeechtherapyinterventionbestartedby 6monthsofage.1,22,25
Some studies carried out in Brazil also showed that it wasdifficulttoachieve therecommendedstandards. Ina studythatassessedthestatusofthediagnosisandcareof patients withhearing loss aged 0---14 years in the city of Campinas,themeanageatdiagnosiswas4.3yearsandthe meanageatISAD fittingwas7.5years.24Inthestudythat aimedtocharacterizetheageatdiagnosisandintervention ofchildrentreatedattheHospitaldasClínicasdeSãoPaulo, themeanageat thesestepswas5.4yearsand6.8 years, respectively.6
Theseaspectsoflanguageinterventionbecomerelevant becausetheageatdiagnosisandadaptationaredetermining factorsfortheprognosisofauditoryandlanguageskill devel-opmentinchildrenwithhearingimpairment.6TheNewborn HearingScreeningProgram(NHSP)wasimplementedinthe
state of Minas Gerais through SES Resolution No. 1.32126 and became mandatory nationwide through Federal Law No.12.30327 forearlydetectionofhearingloss,duetothe impact that hearing loss can have on child development. It is worth mentioning thatthe children evaluatedin this studywerenotsubmittedtotheNHSP,whichmayexplain theresultsrelatedtospeechtherapyintervention.
Regardless of the degree of hearing loss, the effec-tive use of the electronic device alone most often is not enough to minimize the damageto the auditory and lan-guageskills,andspeechtherapyisofutmostimportancein thisprocess.21,28Accordingtotheliterature,thetherapeutic processshouldbestartedasearlyaspossible,becontinuous, andinvolvethechild’sfamily.3
Table3 Distributionofchildrenaccordingtothedegreeofhearinglossandthetypeofcommunicationused,andresultsof oralandwrittenlanguagetests.
Degreeofhearingloss
Communicativeprofile Profoundbilateral (n=25)
Moderatelysevere/ severe(n=48)
Mild/moderate (n=37)
Total
n % n % n % n %
Communication
Oral 3.0 12.0 31.0 64.6 34.0 91.9 68.0 61.8
Oral+LIBRAS 1.0 4.0 9.0 16.7 3.0 8.1 12.0 10.9
Non-oral 21.0 84.0 8.0 18.8 0.0 0.0 30.0 27.3
Vocabularyalterationa
General 3.0 100.0 31.0 77.5 18.0 48.6 52.0 65.0
Clothing 3.0 100.0 31.0 77.5 22.0 59.5 56.0 70.0
Animals 1.0 33.3 12.0 30.0 5.0 13.5 18.0 22.5
Food 3.0 100.0 40.0 100.0 29.0 78.4 72.0 90.0
Transportation 2.0 66.6 17.0 42.5 9.0 24.3 28.0 35.0
Furnitureandutensils 2.0 66.6 18.0 45.0 8.0 21.6 28.0 35.0
Professions 3.0 100.0 32.0 80.0 15.0 40.5 50.0 62.5
Places 3.0 100.0 39.0 97.5 31.0 83.8 73.0 91.2
Shapesandcolors 2.0 66.6 26.0 65.0 16.0 43.2 44.0 55.0
Toysb 2.0 66.6 27.0 67.5 19.0 51.4 48.0 60.0
Alterationofphonologya
Presenceofalteration 3.0 100.0 38.0 42.6 31.0 83.8 72.0 88.8
Presenceofomission 2.0 66.6 20.0 48.7 14.0 37.8 36.0 44.4
Presenceofsubstitution 3.0 100.0 34.0 82.9 24.0 64.8 61.0 75.3
Presenceofdistortion 2.0 66.6 16.0 39.0 9.0 24.3 27.0 33.3
Presenceofculturalpattern 3.0 100.0 32.0 78.0 25.0 67.5 60.0 74.0
PerformanceatSPT
General
Inferior 25.0 100.0 47.0 97.9 31.0 83.8 103.0 93.6
Medium 0.0 0.0 1.0 2.1 4.0 10.8 5.0 4.5
Superior 0.0 0.0 0.0 0.0 2.0 5.4 2.0 1.8
Reading
Inferior 25.0 100.0 44.0 91.7 24.0 64.9 93.0 84.5
Medium 0.0 0.0 4.0 8.4 11.0 29.7 15.0 13.7
Superior 0.0 0.0 0.0 0.0 2.0 5.4 2.0 1.8
Writing
Inferior 25.0 100.0 47.0 97.9 29.0 78.4 101.0 91.8
Medium 0.0 0.0 1.0 2.1 7.0 18.9 8.0 7.3
Superior 0.0 0.0 0.0 0.0 1.0 2.7 1.0 0.9
Arithmetic
Inferior 25.0 100.0 46.0 95.9 27.0 73.0 98.0 89.1
Medium 0.0 0.0 2.0 4.2 8.0 21.6 10.0 9.0
Superior 0.0 0.0 0.0 0.0 2.0 5.4 2.0 1.8
LIBRAS,BrazilianSignLanguage;SPT,schoolperformancetest.
a Onlyorallycommunicativechildren.
b Toysandmusicalinstruments.
therapy was by the Brazilian Unified Health System (Sis-temaÚnicodeSaúde[SUS])30andanotherthatinvestigated the characteristics of diagnosis andspeech therapy inter-ventioninchildren withhearingimpairmentin thecityof Blumenau.31
The largenumberofchildrenwithbelownormal devel-opment of oral and written language and listening skills, regardless of the degree of hearing loss, reflects the
consequencesofspeechtherapyinterventionforthese indi-viduals.
Table4 Association between the degree of hearing loss and the type of communication used by children with hearing impairment.
Communicationuseda
Degreeofhearingloss Oral Others OR 95%CI
Mild/moderate 34 3 1
Moderatelysevere/severe 31 17 6.2 1.50---29.70
Profoundbilateral 3 22 83.1 12.67---731.15
aTesteQuiQuadradodeTendência.
an ISAD and undergoingspeechtherapy intervention,will have development close to that of children with normal hearing.17
Moderatelysevere/severehearinglosscanhaveagreater impactonthedevelopmentofauditoryandlanguageskillsin childrenwithhearingimpairmentwhencomparedtothose withmild/moderatehearingloss.However,theuseof hear-ing aids and the stimulation of the auditory skills would allowthesechildrenasatisfactoryhearingandorallanguage development.
Inthisstudy,alargenumberofchildrenhadsignificant difficultyinlisteningcomprehensionskills.Asaresult,many arenot orally communicative, and amongthose who use speechtocommunicate,mostofthemshowedgreatdelay inlexicalandphonologicaldevelopment.
Forthegroupofchildrenwithprofoundbilateralhearing loss,noresponsewasobserved tothedetection, discrim-ination,perceptionofextension,recognitionandlistening comprehensionskills.Fewchildreninthisgroupusedspeech tocommunicate, and those whowere orally communica-tiveshowedasignificant delayinlexicalandphonological development.Theresidualhearingobservedinchildrenwith profound bilateral hearing loss is small, which limits the dynamicrangeof hearingand, consequently,theauditory gainwiththeISAD,explainingthegreatdifficultythese chil-drenexperienceintheperceptionofenvironmentalsounds andspeech.32,33
In these cases, the use of the cochlear implant is indicated;ithasprovidedgreatbenefitsinlanguage devel-opmentinchildrenwithprofoundhearingloss,asitprovides accesstospeechinformation,particularlyathigh frequen-cies,whichisgenerallynotpossiblewiththeuseofanISAD. Moreover,implanted children have better speech percep-tion,increasednumberofproducedvowelsandconsonants, and better speech intelligibility than those using hearing aids.28,32,33
However,forthistypeof interventiontobeperformed withsatisfactoryoutcomesinthedevelopmentofauditory andlanguageskills,thehearingdiagnosisandspeech ther-apyinterventionmustbeearly.28,34
Regardingtheperformanceofwrittenlanguageskillsin allevaluatedgroups,themajorityofthechildrenhadalow performanceintheacademicachievementtest.Thisresult maybeassociatedwithlowperformanceintheauditoryand orallanguagetests.Itiscommontoobservelearning diffi-cultiesinchildrenwithhearingimpairment,asthedeficitsof orallanguageandauditoryskillscanhave,asaconsequence, changesinthedevelopmentprocessofreading,writing,and logicalandmathematicalreasoning.
Moreover, the domains of capacity of symbolization, generalization, manipulation of sounds, and phonological awarenessarealsocrucialinlearningandarepoorly devel-opedinthesechildren.35
Thehearingandlanguageimpairmentsobservedinthese twogroupscouldhavebeenminimizedifthesechildrenhad beenassessedbytheNHSPandspeechtherapyintervention hadbeeninitiatedearly.Thecriticalperiodofcentral audi-torysystemmaturationmainlyoccursinthefirstfiveyearsof life.34However,theageatdiagnosis,ISADfitting,andstart ofspeechtherapyfoundforthesegroupswereaftertheage of5years.Additionally,socioeconomicfactorscanalso influ-encechildren’sdevelopment.3,36 Inthisstudy,mostofthe childrencamefromfamilieswithpercapitaincomebelow theminimumwageandthelevelofparentaleducationwas low.
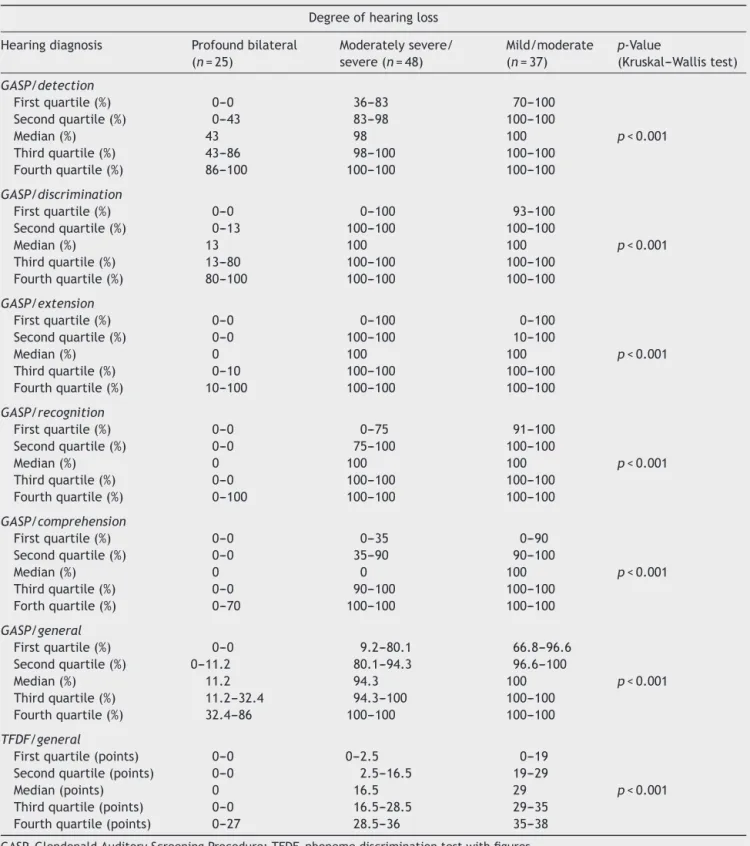
Thedifficultyintheauditoryskills oftheassessed chil-dren,regardlessofthedegreeofhearingloss,canalsobe seeninthediscrepancybetweentheresultsofthetwo hear-ingtests.Inallgroups,thebetterresultswereobservedin theGASPtestthaninthephonemediscriminationtestwith figures.Thisfactcanbeexplainedbythedifferentauditory skillsrequiredineachtest.Theskillsofdetection,vowel dis-crimination,perception ofextension,auditory recognition inaclosed set,andcomprehensionofeverydaysentences areinvolvedtheGASPtestperformance.
Asforthephonemediscriminationtestwithfigures,the auditory skill involved is phonemic discriminationof min-imal pairs. For the child to have a good performance in this test, other auditory skills should also be mastered, suchastemporalprocessing.19 Furthermore,the semantic andphonologicalcomponents,phonologicalawareness,and memoryinvolvedincreasethedegreeofthetestdifficulty forchildrenwithhearingimpairment.19
Difficultiesinauditorydevelopment,aswellasoraland writtenlanguageobservedinthesubjectsofthisstudy rein-force the importance of attention and care for children diagnosed with hearing impairment. After the implemen-tation of the National Hearing CarePolicy in 2004 by the Ministryof Health,4,5 theseindividualsnowhave accessto fullcare,fromtheauditorydiagnosis,provisionofelectronic sound amplification devices (hearing aids and cochlear implants),aswellasspeechtherapy.
Table5 Performanceoftheeligiblepopulationinthehearing,GASP,andTFDFtests,accordingtothedegreeofhearingloss. Degreeofhearingloss
Hearingdiagnosis Profoundbilateral (n=25)
Moderatelysevere/ severe(n=48)
Mild/moderate (n=37)
p-Value
(Kruskal---Wallistest)
GASP/detection
Firstquartile(%) 0---0 36---83 70---100
p<0.001 Secondquartile(%) 0---43 83---98 100---100
Median(%) 43 98 100
Thirdquartile(%) 43---86 98---100 100---100 Fourthquartile(%) 86---100 100---100 100---100
GASP/discrimination
Firstquartile(%) 0---0 0---100 93---100
p<0.001 Secondquartile(%) 0---13 100---100 100---100
Median(%) 13 100 100
Thirdquartile(%) 13---80 100---100 100---100 Fourthquartile(%) 80---100 100---100 100---100
GASP/extension
Firstquartile(%) 0---0 0---100 0---100
p<0.001 Secondquartile(%) 0---0 100---100 10---100
Median(%) 0 100 100
Thirdquartile(%) 0---10 100---100 100---100 Fourthquartile(%) 10---100 100---100 100---100
GASP/recognition
Firstquartile(%) 0---0 0---75 91---100
p<0.001 Secondquartile(%) 0---0 75---100 100---100
Median(%) 0 100 100
Thirdquartile(%) 0---0 100---100 100---100 Fourthquartile(%) 0---100 100---100 100---100
GASP/comprehension
Firstquartile(%) 0---0 0---35 0---90
p<0.001 Secondquartile(%) 0---0 35---90 90---100
Median(%) 0 0 100
Thirdquartile(%) 0---0 90---100 100---100 Forthquartile(%) 0---70 100---100 100---100
GASP/general
Firstquartile(%) 0---0 9.2---80.1 66.8---96.6
p<0.001 Secondquartile(%) 0---11.2 80.1---94.3 96.6---100
Median(%) 11.2 94.3 100
Thirdquartile(%) 11.2---32.4 94.3---100 100---100 Fourthquartile(%) 32.4---86 100---100 100---100
TFDF/general
Firstquartile(points) 0---0 0---2.5 0---19
p<0.001 Secondquartile(points) 0---0 2.5---16.5 19---29
Median(points) 0 16.5 29
Thirdquartile(points) 0---0 16.5---28.5 29---35 Fourthquartile(points) 0---27 28.5---36 35---38
GASP,GlendonaldAuditoryScreeningProcedure;TFDF,phonemediscriminationtestwithfigures.
asthetrainingofhealthprofessionalsregardingthe suspi-cionanddiagnosisofhearinglossinchildren,structuringof the newborn hearingscreening program, and investments toqualify the SASAs andrehabilitation centers.Agile and efficientaccessofchildrentoahearinghealthprogramand the availabilityof experiencedand qualified professionals toperformsuchfunctionsshouldbeguaranteed.
Currently,theassessmentofthehearinghealth service qualityisdirectedtowardinfrastructure(physicalfacilities, number of professionals, equipment) and monthly proce-dureproductivity,whichdoesnotguaranteetheassessment of the quality of services provided. The periodic and standardized assessment of the auditory skills and lan-guage development in children followed in SASAs must be systematically conducted, aiding treatment planning as a resource to assess the quality of the interven-tion.
Thus, longitudinal studies are needed to monitor the qualityof servicesandtheadvancesof thenational hear-inghealthprogramproposals.Theinfluenceofsomefactors suchasage,rehabilitationfacilities,family,socio-economic environment,andthechild’ssocialbehaviorshouldalsobe investigatedinordertoimplementmoreappropriateactions inthedifferentloco-regionalrealities.
Duringthestudyperformance,therewassomedifficulty intheselection ofstandardizedandvalidatedtools devel-opedin Brazilfor children withhearing impairmentolder than6 yearsofage, especiallyfor theassessment of oral language(vocabularyandphonology)andlearning.Inmost cases, in the available assessments, normal values were basedontheperformanceofchildrenwithnormalhearing and,astheprocessesofhearingandlanguagedevelopment ofchildrenwithhearinglossdonotfollowthesame stan-dards,therewassomedifficultywhencomparingwiththe resultsofotherstudies.
Regardingthedevelopmentofphonologyinchildrenwith hearingloss,veryoften thealterationobservedwas asso-ciatedwiththedifficulty inperception anddiscrimination ofspeechsoundscaused bytheauditoryacuityreduction. However,itwasdecidedtoevaluatethisaspectoflanguage developmentwiththe aim of investigatingthe exchanges andphonologicalprocessesobservedinthedevelopmentof theassessedchildren.
ItisnoteworthythattheeffectiveuseofISADs,timeof hearingaidfitting,andthetimeofspeechandaudiological therapymayalsoinfluenceauditorydevelopment,aswellas oralandwrittenlanguage.Inthisstudy,mostoftheassessed childreneffectivelyusedhearingaids.However,therewas alargevariabilityintimeofISADfittingandspeechtherapy amongtheindividuals.
Thesevariablesmayhaveinfluencedthedevelopmentof theassessedchildren,aswellastheirperformanceinthe tests.
Conclusion
Manyofthechildrenwithhearingimpairmenthadabnormal developmentofauditory skills,orallanguage,andwritten language.Thisoutcomeisrelatedtothecharacteristicsof speechtherapy,astheauditorydiagnosis,thefittingofthe ISAD,andspeechtherapy follow-upoccurredlate, regard-lessofthedegreeofhearingloss.
Evaluation of oral and written language and auditory skills of children with hearing impairment shouldbe per-formedperiodically,sothattheprocessofspeechtherapy interventionmaybereassessedandsothetherapeutic strat-egy is planned in accordance with the evolution of each individual.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.FernandesJC,NozawaMR.Estudodaefetividadedeum pro-grama de triagem auditiva neonatal universal. Ciênc Saúde Coletiva.2010;15:353---61.
2.Nazar MG, Goycoolea VM, Godoy SJM, Ried GE, Sierra GM. Evaluación auditiva neonatal universal: revisión de 10.000 pacientesestudiados.RevOtorrinolaringolCirCabezaCuello. 2009;69:93---102.
3.TanamatiLF,BevilacquaMC, Costa OA. Implante coclearem crianc¸as pós linguais: resultados funcionais após 10 anos da cirurgia.BrazJOtorhinolaryngol.2012;78:103---10.
4.Brasil.MinistériodaSaúdePortarian◦587,de7deoutubrode
2004[accessed10.11.13].Availablefrom:http://portal.saude.
gov.br/portal/sas/mac/area.cfm?idarea=824
5.Brasil.MinistériodaSaúdePortarian◦589,de08deoutubrode
2004[accessed10.11.13].Availablefrom:http://portal.saude.
gov.br/portal/sas/mac/area.cfm?idarea=824
6.Bellis TJ. Assessment and management of central auditory processingdisordersin the educationalsetting. 2nd ed.San Diego:Singular;2002.
7.StuchiRF,Nascimento LT,BevilacquaMC,Brito NetoRV. Lin-guagemoralde crianc¸as comcincoanos deusodoimplante coclear.Pró-Fono.2007;19:167---76.
8.Kiese-HimmelC,ReehM.Assessmentofexpressivevocabulary outcomesin hearing-impairedchildrenwithhearing aids:do bilaterallyhearing-impairedchildrencatchup?JLaryngolOtol. 2006;120:619---26.
9.CostaMCM,ChiariBM.Verificac¸ãododesempenhodecrianc¸as deficientesauditivasoralizadasemtestedevocabulário. Pró-Fono.2006;18:189---96.
10.FortunatoCAU, BevilacquaMC,CostaMPR. Análise compara-tivadalinguagemoraldecrianc¸asouvintesesurdasusuáriasde implantecoclear.RevCEFAC.2009;11:662---72.
11.Andrade CRF, Befi-Lopes DM, Fernandes FDM, Wertzner HF. ABFW: teste de linguagem infantil nas áreas de Fonologia, Vocabulário,FluênciaePragmática.SãoPaulo:Pró-Fono;2000. p.5---40.
12.Befi-lopesD.Provadevocabulário(parteB).In:AndradeCRF, Befi-LopesDM, Fernandes FDM, WertznerHF, editors.ABFW: testedelinguageminfantilnasáreasdeFonologia,Vocabulário, FluênciaePragmática.SãoPaulo:Pró-Fono;2000.p.5---40.
13.Befi-LopesDM.Prova deverificac¸ãodovocabulário: aspectos daefetividadecomoinstrumentodiagnóstico[LivreDocência]. SãoPaulo:UniversidadedeSãoPaulo;2002.
14.WertznerHF.Fonologia.In:AndradeCRF,Befi-LopesDM, Fer-nandesFDM,WertznerHF,editors.ABFW:testedelinguagem infantilnasáreasde fonologia,vocabulário,fluência e prag-mática.SãoPaulo:Pró-Fono;2000.p.5---40.
15.SteinLM.TDE---- testede desempenhoescolar:manualpara aplicac¸ãoeinterpretac¸ão.SãoPaulo:CasadoPsicólogo;1994.
16.BevilacquaMC,TechEA.In:MarchesanIQ,ZorziJL,GomesICD, editors.TópicosemFonoaudiologia.SãoPaulo:Lovise;1996.p. 411---33.
17.VieiraABC,MacedoLR,Gonc¸alvesDU.Odiagnósticodaperda auditivanainfância.JPediatr.2007;29:43---9.
18.CarvalhoBS.Testedefiguraparadiscriminac¸ãofonêmica [dis-sertation].SantaMaria:UniversidadeFederaldeSantaMaria; 2007.
20.GândaraJP,Befi-LopesDM.Tendênciasdaaquisic¸ãolexicalem crianc¸asemdesenvolvimentonormalecrianc¸ascomAlterac¸ões específicas no desenvolvimento da linguagem. Rev Soc Bras Fonoaudiol.2010;15:297---304.
21.Almeida K, Iorio MCM. Próteses auditivas: fundamentos teóricos e aplicac¸ões clínicas. 2nd ed. São Paulo: Lovise; 2003.
22.LewisDR,Marone SAM,MendesBCA, CruzOLM, Nóbrega M. Comitêmultiprofissionalem saúdeauditiva:COMUSA.Braz J Otorhinolaryngol.2010;76:121---8.
23.JointCommitteeonInfantHearing.Year2007position state-ment:principlesandguidelinesforearlyhearingdetectionand interventionprograms.Pediatrics.2007;120:898---921.
24.SígoloC,LacerdaCBF. Dasuspeitaàintervenc¸ãoemsurdez: caracterizac¸ãodesteprocessonaregiãodeCampinas/SP.JSoc BrasFonoaudiol.2011;23:32---7.
25.Pinto MM, Raimundo JC, Samelli AG, Carvalho ACM, Matas CG,Ferrari GMS, et al. Idade no diagnóstico eno início da intervenc¸ão decrianc¸as deficientesauditivas em um servic¸o públicodesaúdeauditivabrasileiro.Arq IntOtorrinolaringol. 2012;16:44---9.
26.MinasGerais.Secretariade EstadodeSaúde.Resoluc¸ão1321
de18deoutubrode2007[accessed10.11.13].Availablefrom:
http://www.saude.mg.gov.br/atos normativos/legislacao-sanitaria/estabelecimentos-de-saude/saude-auditiva/ Resolucao%20SES-MG%20no%201321,%20de%2018-10-2007.pdf
27.Brasil. Ministério da Saúde. Lei 12.303 de 02 de agosto
de 2010 [accessed 10.11.13]. Available from: http://www.
planalto.gov.br/ccivil03/Ato2007-2010/2010/Lei/L12303.htm
28.AngeloTCS,BevilacquaMC,MoretALM.Percepc¸ãodafalaem deficientesauditivospré-linguaisusuáriosdeimplantecoclear. Pró-Fono.2010;22:275---80.
29.CarvalhoLRL,LichtigI,CoutoMIV.Avaliac¸ãodobenefíciodouso deaparelhosdeamplificac¸ãosonoraindividualemcrianc¸as.Arq IntOtorrinolaringol.2012;16:170---8.
30.MinasGerais.SecretariadeEstadodeSaúde.Resoluc¸ão1669
de 19 de novembro de 2008 [accessed 10.11.13]. Available
from:
http://www.saude.mg.gov.br/servico/servicos-para-o-profissional-desaude/RESOLUCaO%20SES%20No1669%20DE %2019%20DE%20NOVEMBRO%20DE%202008.pdf
31.BazzoLMF,NoronhaCV.Aóticadosusuáriossobreaofertado atendimentofonoaudiológiconoSistemaÚnicodeSaúde(SUS) emSalvador.CiêncSaúdeColetiva.2009;14:1553---64.
32.TschoekeSN,JacobLCB,MarquesJM.Estudododiagnóstico, etiologiae(re)habilitac¸ãododeficienteauditivoemumcentro daRegiãoSul.CiêncCultura.2008;39:63---84.
33.Delgado-PinheiroEMC,AntonioFL,BertiLC.Perfilaudiológico ehabilidadesauditivasemcrianc¸aseadolescentescomperda auditiva.EstudosLinguísticos.2010;39:10---20.
34.QueirozCAUF,BevilacquaMC,CostaMPR.Estudolongitudinalda compreensãoverbaldecrianc¸asusuáriasdeimplantecoclear. RevCEFAC.2010;12:210---5.
35.MoretALM,BevilacquaMC,CostaOA.Implantecoclear:audic¸ão elinguagememcrianc¸asdeficientesauditivaspré-linguais. Pró-Fono.2007;19:295---304.