ww w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Mean
platelet
volume
is
decreased
in
adults
with
active
lupus
disease
Guillermo
Delgado-García
a,∗,
Dionicio
Ángel
Galarza-Delgado
a,b,
Iris
Colunga-Pedraza
b,
Omar
David
Borjas-Almaguer
a,
Ilse
Mandujano-Cruz
a,
Daniel
Benavides-Salgado
a,
Rolando
Jacob
Martínez-Granados
a,
Alexandro
Atilano-Díaz
aaUniversidadAutónomadeNuevoLeón,HospitalUniversitario,DepartamentodeMedicinaInterna,Monterrey,Mexico
bUniversidadAutónomadeNuevoLeón,HospitalUniversitario,ServiciodeReumatología,SanNicolásdelosGarza,Mexico
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received10June2015
Accepted13December2015
Availableonline21March2016
Keywords:
Systemiclupuserythematosus
Meanplateletvolume
Diseaseactivity
Inflammation
Biologicalmarkers
Serumalbumin
a
b
s
t
r
a
c
t
Background:Onlyafewbiomarkersareavailableforassessingdiseaseactivityinsystemic
lupuserythematosus(SLE).Meanplateletvolume(MPV)hasbeenrecentlystudiedasan
inflammatorybiomarker.Itiscurrentlyunclearwhether MPVmayalsoplayaroleasa
biomarkerofdiseaseactivityinadultpatientswithSLE.
Objective:We investigated the association between MPV and disease activity in adult
patientswithSLE.
Methods:In thisretrospectivestudy,wecomparedtwogroupsofadultpatientsdivided
accordingtodiseaseactivity(36pergroup).Subjectswereage-andgender-matched.
Results:MPV was significantly decreased with respect to those of inactive patients
(7.16±1.39vs.8.16±1.50,p=0.005).Atacutofflevel of8.32fL, MPVhasasensitivityof
86%andaspecificityof41%forthedetectionofdiseaseactivity.Amodestpositive
cor-relationwasfoundbetweenMPVandalbumin(r=0.407,p=0.001),whichinturnisinversely
associatedwithdiseaseactivity.
Conclusions:Insummary,MPVisdecreasedinadultpatientswithactivelupusdisease,and
positivelycorrelatedwithalbumin,anotherbiomarkerofdiseaseactivity.Prospective
stud-iesareneededtoevaluatetheprognosticvalueofthisbiomarker.
©2016ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND
license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](G.Delgado-García).
http://dx.doi.org/10.1016/j.rbre.2016.03.003
2255-5021/©2016ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/
O
volume
plaquetário
médio
está
reduzido
em
adultos
com
lúpus
ativo
Palavras-chave:
LúpusEritematosoSistêmico
Volumeplaquetáriomédio
Atividadedadoenc¸a
Inflamac¸ão
Marcadoresbiológicos
Albuminasérica
r
e
s
u
m
o
Antecedentes:Existempoucosbiomarcadoresdisponíveisparaavaliaraatividadedadoenc¸a
nolúpuseritematososistêmico(LES).Ovolumeplaquetáriomédio(VPM)foirecentemente
estudadocomoumbiomarcadorinflamatório.AtualmentenãoestáclaroseoVPMtambém
podedesempenharumpapelcomoumbiomarcadordaatividadedadoenc¸aempacientes
adultoscomLES.
Objetivo: Investigou-sea associac¸ãoentreoVPMeaatividadedadoenc¸aempacientes
adultoscomLES.
Métodos: Nesteestudoretrospectivo,compararam-sedoisgruposdepacientesadultos
divi-didosdeacordocomaatividadedadoenc¸a(36porgrupo).Osindivíduosforampareados
poridadeegênero.
Resultados: OVPMestevesignificativamentediminuídonospacientescomdoenc¸aativaem
comparac¸ãocomosníveisempacientescomdoenc¸ainativa(7,16±1,39versus8,16±1,50,
p=0,005). Emumníveldecortede8,32fL,oVPMtemumasensibilidadede86%euma
especificidadede41%paraadetecc¸ãodaatividadedadoenc¸a.Encontrou-seumacorrelac¸ão
positivamodestaentreoVPMeaalbumina(r=0,407,p=0,001),queporsuavezestá
inver-samenteassociadaàatividadedadoenc¸a.
Conclusões: Emresumo,oVPMestádiminuídoempacientesadultoscomlúpusativo,e
positivamentecorrelacionadocomaalbumina,outrobiomarcadordaatividadedadoenc¸a.
Sãonecessáriosestudosprospectivosparaavaliarovalorprognósticodessebiomarcador.
©2016ElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCC
BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Platelet size correlates with platelet activity. Autoimmune
reactionsarethoughttocontributetoplateletactivation in
systemiclupuserythematosus(SLE).Infact,thereisa
corre-lationbetweenmeanplateletvolume(MPV)valuesandactive
inflammatorydiseases.1,2 Ithasbeenrecentlyreportedthat
MPVisincreasedinpatientswithjuvenileSLE.Moreover,this
parameterincreasedinparallelwiththeactivityindex,and
appearstobemoreaccuratethanerythrocytesedimentation
rate(ESR)and C3indetectingdisease activity.3 However,it
iscurrentlyunclearwhetherMPVmayalsoplayaroleasa
biomarkerofdiseaseactivityinadultpatientswithSLE.
There-fore,weconductedthepresentstudytotestthishypothesis.
Material
and
methods
Subjectsandstudydesign
Aretrospective,cross-sectional,comparativedesignwasused
forthisstudy.Demographicandlaboratorydatawereobtained
byreviewingmedicalrecords ofall patientswho had been
diagnosed withSLE inour hospital. Systemic Lupus
Inter-national Collaborating Clinics (SLICC)classification criteria
wereusedforthe diagnosis,exceptforthose patientswho
werediagnosedbeforethesecriteriawerepublished,inwhich
caseitwasmadeusingtheAmericanCollegeof
Rheumato-logy(ACR)criteria.Lupusnephritiswasclassifiedaccording
tothe International Society ofNephrology/Renal Pathology
Society (ISN/RPS) 2003 classification. The inclusion
crite-ria were as follows: age older than 16 years; diagnosis of
SLE;andaMexicanSystemicLupusErythematosusDisease
Activity Index (Mex-SLEDAI) scored in the polyclinic
(inac-tivepatients)or atadmission(active patients),as recorded
byarheumatologyfellow.Exclusioncriteriawerethe
follow-ing:infection,thrombocytopenia,rheumatoid arthritis(RA),
ankylosingspondylitis(AS),inflammatoryboweldisease(IBD),
psoriasis, and incomplete medical record. Overall disease
activity wasassessedwithMex-SLEDAI.Patientsscoring<2
wereclassifiedasinactive,whilethosescoring>5were
clas-sified as active.4,5 This study was approved by the ethics
committeeoftheAutonomousUniversityofNuevoLeón
Fac-ultyofMedicine.Writteninformedconsentwasnotrequired.
Assays
BloodsamplesweretakenbyfrombothplainandEDTAtubes.
Thelatterwereusedforcompletebloodcount(CBC).Most
rou-tineCBC weredone withaCell-DynRubyanalyzer (Abbott
Diagnostics,USA),whilemostclinicalchemistryparameters
(creatinine, blood urea nitrogenand serum albumin) were
measuredusingaDxC800Synchronanalyzer(Beckman
Coul-ter,USA).ESRdeterminationswereperformedbytheWintrobe
method,whoseuppernormallimitwas20mm/h.
Statistics
BasedonapreviousreportonMPVinjuvenileSLE,3sample
size was calculated using comparisonsof means.
Calcula-tion was performed using ˛=0.05, ˇ=0.20, and two tails.
A total sample size of 60 (30 in each group) would be
required to demonstrate a statistically significant
usingShapiro–Wilktest.Comparisonsbetweengroupswere
performed by using chi-square test, Student’s t-test or
Mann–WhitneyUtest,asappropriate.Associationsbetween
the variables were explored using the Pearson
product-momentcorrelationcoefficientorSpearman’srho.Areceiver
operatingcharacteristic(ROC)curvewasgeneratedto
deter-minethe cutoffvalueinthe MPV(andother inflammatory
biomarkers)withthehighestlevelofaccuracyinidentifying
patientswithdiseaseactivity.Sensitivity,specificity,positive
predictive value (PPV), and negativepredictive value (NPV)
were calculated.Unless indicatedotherwise, all resultsare
expressedasmean±SDormedian(25–75%).Statistical
analy-seswereconductedusingSigmaStat(v.3.5,Erkrath,Germany)
orMedCalc(v.14.12.0,Ostend,Belgium),andap-valuebelow
0.05(p<0.05)wasconsideredsignificant.
Results
Atotalof72patientswereincludedinthisstudy,36patients
wereclassifiedashavingactivedisease(34females,aged18–64
years),and36patientsashavinginactivedisease(35females,
aged20–53years).Theageandgenderdistributionswere
sim-ilarinthetwogroups(p=0.83 andp=0.55,respectively).10
activepatients(27%)werediagnosedduringtheirfirst
hospi-talization,soyearssincediagnosisweresignificantlydifferent
betweengroups(1[0–15]vs.5[1–23],p≤0.001).The
percent-ageofapreviousdiabetesdiagnosisdidnotdifferbydisease
activity([1,n=70]=2.57,p=0.108,Yates’p-value).Patientswith
activediseaseweremorelikelytohaveaprevious
hyperten-siondiagnosisthanthosewithinactivedisease(38.2%vs.2.7%,
[1,n=70]=13.74,p≤0.001).Ten(27.7%)oftheactivepatients
had biopsy-provenlupus nephritis (LN).Ofthese, 40% had
ISN/RPSclassIIILN,30%hadclassIVLN,20%hadclassVLN,
and10%hadclassIILN.
Hemoglobin,absolutelymphocytecount(LYM),MPV,and
albuminofactivepatientsweresignificantlydecreasedwith
respecttothoseofinactivepatients,whereasESRwas
com-parativelyincreasedintheformergroup.Plateletcountand
100
80
60
40
20
0
0 20 40
Sensitivity
100-Specificity
60 80 100
ESR MPV Alb
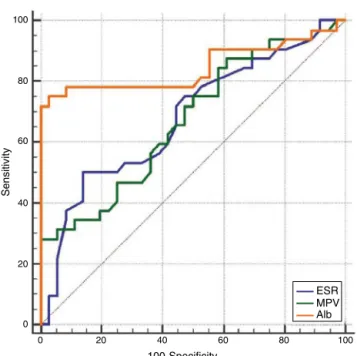
Fig.1–Receiver-operatingcharacteristics(ROC)curve analysisforthediagnosticperformanceofESR(blueline), MPV(greenline)andalbumin(Alb,orangeline).
creatinine were not significantly different between groups
(Table1).Amodestpositivecorrelationwas foundforMPV
andalbumininactivepatients(r=0.407,p=0.001).Therewere
nosignificantrelationshipsbetweenMPVandESR(p=0.26).
TheROCcurve analysisforMPVshowedanareaunderthe
curve(AUC)of0.685(95%CI0.565–0.790,p=0.003)withan
opti-malcutoffvalueof8.32fL(Fig.1).Sensitivity,specificity,PPV,
andNPVwere86%,41%,59%,and75%,respectively.TheAUC
forpredictingdiseaseactivitywas0.658(95%CI0.537–0.766,
p=0.015)forESR(Fig.1).Atacutofflevel of37mm/h,
sen-sitivity, specificity, PPV, and NPV were 44%, 86%,76%, and
60%,respectively.TheAUCforalbumin,withacutoffpoint
of3.2g/dL,was0.845(95% CI0.737–0.922,p≤0.001)(Fig.1).
Table1–Paraclinicalcomparisonbetweengroups.
Parameter Active(n=36) Inactive(n=36) p Test
Hb(g/dL) 10.9±1.97 12.69±1.2 <0.001 ST
WBC(109/L) 6.46±2.73 6.28±2.76 0.781 ST
NEU(109/L) 4.81±2.36a 4.12±2.49 0.237 ST
LYM(109/L) 1.12±0.74a 1.58±0.67 0.008 ST
PLT(109/L) 269.88±870.02 271.72±698.07 0.922 ST
MPV(fL) 7.16±1.39 8.16±1.50 0.005 ST
ESR(mm/h) 31(21.5–45) 22.5(14.5–34.5) 0.021 MWU
Crea(mg/dL) 0.61(0.57–0.89)a 0.64(0.53–0.72) 0.60 MWU
BUN(mg/dL) 13.4(10–22.75)a 12(10–14) 0.12 MWU
Alb(g/dL) 2.73±0.81b 3.7±0.27 <0.001 ST
Hb,hemoglobin;WBC,whitebloodcellcount;NEU,absoluteneutrophilcount;LYM,absolutelymphocytecount;PLT,plateletcount;MPV,mean plateletvolume;ESR,erythrocytesedimentationrate;Crea,creatinine;BUN,bloodureanitrogen;Alb,albumin;ST,Student’st-test;MWU, Mann–WhitneyUtest.
Allresultsareexpressedasmean±SDormedian(25–75%). a n=35.
Sensitivity,specificity,PPV,andNPVwere75%,97.2%,96%,and
81%,respectively.ThepairwisecomparisonamongtheROC
curvesshowednostatisticaldifference(p=0.054andp=0.947,
respectively).
Discussion
ContrarytopreviouslyreportedfindingsinjuvenileSLE,3 in
thisstudytheMPVwasfoundtobesignificantlylowerinadult
patientswithactivediseasecomparedtothoseclassifiedas
havinginactivedisease.Althoughseveralreportshave
indi-catedthepotentiallinkbetweenhigherMPVvaluesandactive
inflammatorydisease,theoppositehasbeenfoundinother
studies.1,2Inthelargestsampletodate,MPVwasdecreasedin
adultpatientswithactiveRA,andincreasedaftertreatment.6
Arecentreviewdidnotincludethisreport.7Inasmall
retro-spectivestudyof30adultpatientswithactiveAS,MPVwas
decreasedwheninitialtestswereperformed,andincreased
aftertreatment.8Notwithstanding,thisfindingwasnot
repro-ducedinalargerstudy.9AdultpatientswithIBD(bothinactive
andremissionstages)alsohavealowerMPVwhencompared
tocontrolgroup.10Likewise,inchildrenwithacuterheumatic
fever,MPVhasbeenreportedasdecreased,andincreasedafter
treatment.11
PlateletactivationisobservedinpatientswithSLE,andits
pathophysiologycould includeinflammatorycytokinesand
complement.12,13 One plausible mechanism to explain the
associationbetweendecreasedMPVanddiseaseactivitycould
betheconsumptionoflargeactivatedplateletsin
extravascu-larsitesofinflammation.1However,whileplateletactivation
isenhancedinpatientswithSLE,thesepatientshavenormal
valuesforplateletmeanlife-span,14suggestingthatplatelet
consumptionisminimal.Morestudiesareneededinorderto
furtherelucidatethecauseofthisreductioninplateletsize.
Serumalbumin was comparatively lower in those with
active disease. A modest positive correlation was found
betweenMPVandalbumin,whichinturnisinversely
asso-ciatedwithdiseaseactivity.15 ESRwassignificantlyelevated
in patients with active disease.This is in line with
exist-ingliterature,sinceESRelevationshavebeenassociatedwith
overall disease activity.16 Interestingly,we found no
corre-lationbetweenESRandMPV.Eventhoughbothparameters
mightevaluatediseaseactivity,thislackofcorrelationcould
be,inpart,becausethesebiomarkersmayreflecttwoseparate
biologicalprocesses.
Onlyafewbiomarkersareavailableforassessingdisease
activityinSLE.Anidealbiomarkermustbeeasilymeasured,
reproducibleand sensitiveto changes indisease activity.17
In this study, there was no significant difference in
over-allaccuracybetweenMPVand ESRfordetectionofdisease
activity.Besidesbeingawidelyavailabletest,MPVisalso
cost-effective.Atacutofflevelof8.32fL,MPVhasahighsensitivity
(86%)forthedetectionofdiseaseactivity.Ahighlysensitive
testischieflyimportantwhenitisusedtoidentifyaserious
buttreatablecondition(asalupusflare).
Thisis the first study, toour knowledge, tospecifically
examinetherelationshipbetweenMPVanddiseaseactivity
inadultpatientswithSLE.Variousauthorshaveidentifieda
previousstudy thatfounddecreasedMPVinadultpatients
withSLE.1,3 Nonetheless,theaforementionedstudywasnot
intendedtodemonstratethatMPVisassociatedwithdisease
activity,sinceitstrulyaimwastocomparetheperformance
oftwoautomatedcellcounters.18
Thetimedelaybetweensamplingandprocessingwasnot
controlledinourstudy.However,wefoundadecreasedMPV
inadultpatientswithactivedisease,andMPVincreases(not
decreases)overtimeinEDTAtubes.2Phlebotomistsand
lab-oratory technicians were blindtothe clinical status ofthe
patient,thusrationallyexcludingbias.Also,thediagnosisof
hypertensionwasmorefrequentinpatientswithactive
dis-ease,yetthiswouldmostlikelynotaffectourresults,because
hypertensionisassociatedwithanincreasedMPV, andnot
withitsdecrease.19,20
Insummary,MPVisdecreasedinadultpatientswithactive
lupusdisease,andpositivelycorrelatedwithserumalbumin,
anotherbiomarkerofdiseaseactivity.Prospectivestudiesare
neededtoevaluatetheprognosticvalueofthisbiomarker.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.GasparyanAY,AyvazyanL,MikhailidisDP,KitasGD.Mean plateletvolume:alinkbetweenthrombosisand
inflammation?CurrPharmDes.2011;17:47–58.
2.LeaderA,PeregD,LishnerM.Areplateletvolumeindicesof clinicaluse?Amultidisciplinaryreview.AnnMed.
2012;44:805–16.
3.YavuzS,EceA.Meanplateletvolumeasanindicatorof diseaseactivityinjuvenileSLE.ClinRheumatol. 2014;33:637–41.
4.GuzmánJ,CardielMH,Arce-SalinasA,Sánchez-GuerreroJ, Alarcón-SegoviaD.Measurementofdiseaseactivityin systemiclupuserythematosus.Prospectivevalidationof3 clinicalindices.JRheumatol.1992;19:1551–8.
5.Arce-SalinasA,CardielMH,GuzmánJ,Alcocer-VarelaJ. Validityofretrospectivediseaseactivityassessmentin systemiclupuserythematosus.JRheumatol.1996;23:846–9.
6.KimDA,KimTY.Controversiesovertheinterpretationof changesofmeanplateletvolumeinrheumatoidarthritis. Platelets.2011;22:79–80.
7.BeinsbergerJ,HeemskerkJW,CosemansJM.Chronicarthritis andcardiovasculardisease:alteredbloodparametersgive risetoaprothromboticpropensity.SeminArthritisRheum. 2014;44:345–52.
8.KisacikB,TufanA,KalyoncuU,KaradagO,AkdoganA,Ozturk MA,etal.Meanplateletvolume(MPV)asaninflammatory markerinankylosingspondylitisandrheumatoidarthritis.Jt BoneSpine.2008;75:291–4.
9.YaziciS,YaziciM,ErerB,ErerB,CalikY,BulurS,etal.The plateletfunctionsinpatientswithankylosingspondylitis: anti-TNF-alphatherapydecreasesthemeanplateletvolume andplateletmass.Platelets.2010;21:126–31.
10.ÖztürkZA,DagMS,KuyumcuME,CamH,YesilY,YilmazN, etal.Couldplateletindicesbenewbiomarkersfor
inflammatoryboweldiseases?EurRevMedPharmacolSci. 2013;17:334–41.
12.BoilardE,BlancoP,NigrovicPA.Platelets:activeplayersinthe pathogenesisofarthritisandSLE.NatRevRheumatol. 2012;8:534–42.
13.HabetsKL,HuizingaTW,ToesRE.Plateletsand autoimmunity.EurJClinInvest.2013;43:746–57.
14.KuttiJ,BergströmAL.Plateletkineticsinsystemiclupus erythematosus(SLE),withspecialreferencetocorticosteroid andazathioprinetherapy.ScandJRheumatol.1981;10:266–8.
15.YipJ,AghdassiE,SuJ,LouW,ReichH,BargmanJ,etal.Serum albuminasamarkerfordiseaseactivityinpatientswith systemiclupuserythematosus.JRheumatol.2010;37:1667–72.
16.StojanG,FangH,MagderL,PetriM.Erythrocyte
sedimentationrateisapredictorofrenalandoverallSLE diseaseactivity.Lupus.2013;22:827–34.
17.JungJY,BaeCB,SuhCH.Promisingbiomarkersforsystemic lupuserythematosus.ExpertOpinMedDiagn.2013;7:601–13.
18.Turner-StokesL,JonesD,PattersonKG,Todd-PokropekA, IsenbergDA,GoldstoneAH.Measurementofhaematological indicesofchronicrheumaticdiseasewithtwonewer generationautomatedsystems,theH1andH6000 (Technicon).AnnRheumDis.1991;50:583–7.
19.VarolE,AkcayS,IcliA,YucelH,OzkanE,ErdoganD,etal. Meanplateletvolumeinpatientswithprehypertensionand hypertension.ClinHemorheolMicrocirc.2010;45:67–72.