SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
Prediction
of
flexor
tendon
graft
diameter
in
reconstruction
of
the
anterior
cruciate
ligament
by
means
of
magnetic
resonance
imaging
夽
Fabiano
Kupczik
a,
Luiz
Otávio
Bombonatto
Tauscheck
a,∗,
Marlus
Eduardo
Gunia
Schiavon
a,
Bruno
Sbrissia
a,
Lucio
Sergio
Rocha
Ernlund
b,
Ricardo
Augusto
Lass
Alves
aaPontifíciaUniversidadeCatólicadoParaná(PUC-PR),HospitalUniversitárioCajuru,Curitiba,PR,Brazil bInstitutodeJoelhoeOmbro,Curitiba,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received15July2015 Accepted8September2015 Availableonline6June2016
Keywords:
Anteriorcruciateligament Anteriorcruciateligament reconstruction
Magneticresonancespectroscopy Orthopedicprocedures
a
b
s
t
r
a
c
t
Objective:Toevaluatethediameteroftheflexortendonsinpreoperativemagnetic reso-nanceimaging(MRI)examinationsandcomparethiswiththediameterofthegraftobtained intraoperatively.
Methods:Thiswasaretrospectivelongitudinalepidemiologicalstudy.Forty-fourpatients wereeligibleforthestudyandtheirMRIexaminationsandsurgicaldatawereevaluated. ThetendonsweremeasuredonMRIacrosstheirlargestdiameterintheaxialplane,usingthe medialepicondyleofthefemurastheslicelevel.Inthesurgery,routinegraftpreparation wasperformed,consistingoffoldingthegracilisandsemitendinosustendonstoforma four-strandgraft.Itsmeasurementwasrecorded.
Results:Toevaluatetheassociationbetweenthevariables,Pearson’scorrelationcoefficient wasestimated.Asignificantcorrelationwasfoundbetweenthemeasurementsofthe gra-cilisandsemitendinosustendonsandthefinaldiameterofthegraft(p<0.001).AROCcurve wasfittedtothesumofthetendondiametersinordertodetermineacutoffpointassociated withthegraftdiameter(≤8mmor>8mm).Ifthesumwasgreaterthan5.28mm,thechance ofobtainingagraftlargerthan8mmwouldbe75%.
Conclusion: Measurement ofthe diameters ofthe gracilis and semitendinosus tendons throughapreoperativeMRIexaminationisasimpleandeffectivewaytopredictthefinal sizeofthegrafttobeusedinACLreconstructionsurgery.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedatHospitalUniversitárioCajuru,PontifíciaUniversidadeCatólicadoParaná(PUC-PR),Curitiba,PR,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](L.O.B.Tauscheck). http://dx.doi.org/10.1016/j.rboe.2016.06.002
Predic¸ão
do
diâmetro
do
enxerto
dos
tendões
flexores
na
reconstruc¸ão
do
ligamento
cruzado
anterior
por
meio
da
ressonância
nuclear
magnética
Palavras-chave:
Ligamentocruzadoanterior Reconstruc¸ãodoligamento cruzadoanterior
Espectroscopiaderessonância magnética
Procedimentosortopédicos
r
e
s
u
m
o
Objetivo: Avaliarodiâmetrodostendõesflexoresemexamesderessonânciamagnética (RNM)pré-operatóriaecompararcomodiâmetrodoenxertoobtidonoatointraoperatório.
Métodos: Emum estudo epidemiológicolongitudinal retrospectivo,44 pacientesforam elegíveisaoestudoetiveramosexamesdeRNMedadosdecirurgiasavaliados.Ostendões forammedidosnaRNMnoseumaiordiâmetronoplanoaxialcomousodoepicôndilo medialdofêmurcomoníveldecorte.Nacirurgiafoifeitopreparoderotinadoenxerto, dobraram-seostendõesgrácilesemitendinoso,formou-seumenxertoquádruploqueteve suamedidaregistrada.
Resultados: Paraaavaliac¸ãodaassociac¸ãoentreasvariáveisfoiestimadoocoeficientede correlac¸ãodePearson.Foiencontradacorrelac¸ãosignificativaentreasmedidasdostendões grácilesemitendinosoeodiâmetrofinaldoenxerto(p<0,001).Ajustou-seumacurvaROC paraasomadodiâmetrodostendões,paraadeterminac¸ãodeumpontodecorteassociado aodiâmetrodoenxerto(≤8mmou>8mm).Casoasomasejamaiordoque5,28mm,a chancedeobterumenxertomaiordoque8mméde75%.
Conclusão: AmedidadodiâmetrodostendõesgrácilesemitendinosonoexamedaRNM pré-operatóriaéumamaneirasimpleseeficaznapredic¸ãodotamanhofinaldoenxertoa serusadonacirurgiadereconstruc¸ãodoLCA.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Ruptureofthe anteriorcruciateligament(ACL)isthemost commonkneeligamentousinjury,affectingover100,000 peo-ple annually in the United States. Its incidence has been increasingduetoagreaterstimulustoandpracticeofsports bythepopulation.1,2
TheACLoriginatesintheposteriorportionofthelateral femoralcondyle and inserts laterallyand anteriorly tothe medialtibialspine.Itfeaturesanintra-articularand extrasyn-ovial course, with a mean length of 38mm and a mean diameterof11mm.3–5
Currently,itisknownthattheACLiscomposedoftwosets offibersorbands:oneanteromedial(AM)andanother pos-terolateral(PL).Atthefemoralorigin,theAMbandemerges moreproximallyandposteriorly,whilethePLbandemerges moredistallyandanteriorly.Thebandsaretwistedalongtheir pathintheintercondylezone,andthetibialinsertionfollows theorderwhichgivesthemtheirname:anteromedialforthe AMandposterolateralforthePL.5–8
Surgicaltreatmentbasedonligamentreconstructionis rec-ommendedformostACLinjuries.Currently,thereareseveral optionsforgraftstoreplaceit;theflexortendons (semitendi-nosusandgracilis),patellartendon,andquadricepstendon aremostused.2,9Choiceshouldconsiderprofileandpatients’ age,typeofsport,associatedlesions,andsurgeons’ experi-ence.Theidealgrafthasnotbeendefinedyet;somestudies showthatgraftswithdiameterslessthan7mmareassociated withahigherchanceoffailureandrelapse.10–13
Along with the advancement of imaging, preoperative measurementofthe diameter ofthe tendonson magnetic
resonance imaging (MRI) is possible, which is the gold standardimagingstudyforthediagnosisofthisinjury, allow-inganobjectiveparameterforthegrafttobechoseninACL reconstructionpriortosurgery.1,2,14–20
Thisstudyaimedtoevaluatethediameteroftheflexor ten-donsonpreoperativeMRIandcomparewiththediameterof thegraftobtainedintraoperatively.
Material
and
methods
AfterapprovalbytheReseachEthicsCommitteethroughthe Platform Brazil website, under the Certificate of Presenta-tionforEthicalAssessment(CertificadodeApresentac¸ãopara Apreciac¸ão Ética [CAAE])No.39346814.4.0000.0020, 100MRI scansanddatafromsurgeriesperformedbetween2012and 2014werecollectedandreviewedforthisretrospective, longi-tudinal,epidemiologicalstudy.
Inclusion criteria comprised skeletally mature patients withcompleteACLinjuryandnohistoryofpreviousligament or degenerative injuries. Exclusion criteria were: previous surgery, ligamentous laxity, chronic use of steroids, and dysplasia of the intercondylar notch (width of the distal femur/condylarfossa<0.2).
Aftersubjectselectionaccordingtoinclusionandexclusion criteria,44patientswereeligibleforthestudy.
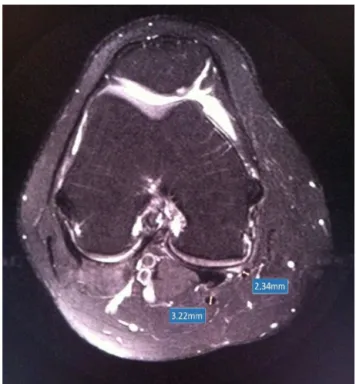
Fig.1–Measurementofdiameterofthesemitendinosus andgracilistendons.
attheirlargestdiameterintheaxialplane,consideringthe medialepicondyleofthefemurasthecutofflevel(Fig.1).
Duringsurgery,tendonswereremovedbystandardfashion techniquethroughaclosedtenotomy.Graftwaspreparedas usual:thegracilisandsemitendinosustendonswerefolded, formingaquadruplegraft.Thepreparedgrafthadits diame-termeasuredbeforedrillingthebonetunnelsinthetibiaand femur.Thesedatawererecordedatthesurgicalreportofthe patients.
Statisticalanalysis
Toevaluatetheassociationbetweenvariables,Pearson’s cor-relationcoefficientwasestimated.Theassessmentoftheuse ofthegracilisandsemitendinosusvariablesaspredictorsof graftdiameterwasmadethroughsimpleandmultiplelinear regressionmodels;toassesstheassociationofthesumofthe gracilisandsemitendinosuswiththeprobabilitythatthegraft diameterwasgreaterthan8mm,alogisticregressionmodel wasadjusted.Wald’stestwasusedtoassessthesignificance ofthecoefficients.
Regardingthesumofthegracilisandsemitendinosusfor determining a cutoff point associated with graft diameter (≤8mmor>8mm),aROCcurvewasadjusted.p-values<0.05 wereconsideredtobestatisticallysignificant.
DatawereanalyzedwithIBMSPSSv.20.0.
Results
Ofthe44patientsstudied,33weremale(75%)and11female (25%).Agerangedfrom 11to54 years,withamean of31.8 years.
Table1–Graftdiameter.
Graftdiameter n %
6 1 2.3
7 3 6.8
8 24 54.5
9 14 31.8
10 2 4.5
Total 44 100
MeandiameterofthegracilistendononMRIwas2.17mm, rangingfrom 1.45 to2.76mm, whilemeandiameter ofthe semitendinosuswas2.96,rangingfrom2.52to3.73mm.
During surgery,mean sizeofgrafts usedforACL recon-structionwas8.3mm,rangingfrom6to10 mm(Table1).
Fig.2showsthescatterplotgraphofthesemitendinosus and gracilisvariables,highlightingthe differenceof coordi-natesaccordingtothediameterofthegraft.
Datacorrelation
Gracilis×graftdiameter
Pearson’scorrelationcoefficientwasestimatedtobe0.59,and the test resultwas statistically significant (p<0.001). Thus, therewasasignificantcorrelationbetweenthegracilisand graftdiameter.Fig.3presentsthescatterplotofbothvariables. Eachpointcorrespondstoonecase.
Semitendinosus×graftdiameter
Pearson’scorrelationcoefficientwasestimatedtobe0.59,and the test resultwas statistically significant (p<0.001). Thus, there was asignificant correlation betweenthe semitendi-nosusandgraftdiameter.Fig.4presentsthescatterplotof bothvariables.Eachpointcorrespondstoonecase.
Sumofgracilis+semitendinosus×graftdiameter
Pearson’scorrelationcoefficientwasestimatedtobe0.74,and the test resultwas statistically significant (p<0.001). Thus, therewasasignificantcorrelationbetweenthesumof gra-cilis+semitendinosusandgraftdiameter.Fig.5presentsthe scatterplotofbothvariables.Eachpointcorrespondstoone case.
2 2.2 2.4 2.6 2.8 3 3.2 3.4 3.6 3.8 4
2.9 2.7 2.5 2.3 2.1 1.9 1.7 1.5 1.3
Semitendinosus
Gracilis
Diam 6 Diam 7 Diam 8 Diam 9 Diam 10
Table2–Gracilis+semitendinosusasapredictorofgraftdiameter.
Diameterestimatedbythemodel Diameterobservedinthesample
6 7 8 9 10
n % n % n % n % n %
6 0 0% 0 0% 0 0% 0 0% 0 0%
7 1 100% 1 33.3% 2 8.3% 0 0% 0 0%
8 0 0% 2 66.7% 19 79.2% 6 42.9% 0 0%
9 0 0% 0 0% 3 12.5% 8 57.1% 1 50%
10 0 0% 0 0% 0 0% 0 0% 1 50%
Total 1 100% 3 100% 24 100% 14 100% 2 100%
3.0 2.8 2.6 2.4 2.2 2.0 1.8 1.6 1.4 1.2
Gracilis 5
6 7 8 9 10 11
Intra-operative graft
Pearson’s correlation coeficiente: 0.59 (P<.001)
Fig.3–Gracilis×graftdiameter.
Pearson’scorrelationcoefficientforbothtendonsshowed amoderatepositivecorrelationpower,whichindicatesa ten-dencythatthe largerthediameter ofthe patients’tendon, thegreaterthe finaldiameterofthe graftobtainedforACL reconstruction.
Assessmentofthequalityofthesumof
gracilis+semitendinosusasapredictorofgraftdiameter Toevaluatethesumofgracilis+semitendinosusasa predic-torofgraft diameter,asimplelinearregressionmodelwas
3.8 3.6 3.4 3.2 3.0 2.8 2.6 2.4 2.2 2.0
Semitendinosus 5
6 7 8 9 10 11
Intra-operative graft
Pearson’s correlation coeficiente: 0.59 (P<.001)
Fig.4– Semitendinosus×graftdiameter.
adjusted, and the sum was considered as an explanatory variable (independent)andthe diameterofthegraft asthe responsevariable(dependent).Theadjustedmodelwas:
Estimated diameter=2.618+1.107 (gracilis+ semitendinosus).
Theestimateddiameterforeachsinglevalueofthesum ofgracilis+semitendinosusshouldberoundedtothenearest integer.Forexample,foraparticularcasewhosesumof gra-cilis+semitendinosusisequalto6.51,theestimatedvalueof thediameterwillbe:
Estimateddiameter=2.618+1.107×6.51=9.82.
Theresultdiametertobeconsideredisequalto10. Basedon the study sample,Table2 presentsthe scores obtainedwiththemodelforeachparticulargraftdiameter.
Asaresultofinterest,thedeterminationcoefficientwas 55%.Thus,itwasestimatedthat55%ofthediameter varia-tionswereexplainedbythegracilis+semitendinosus.
Assessmentofthequalityofthesumof
gracilis+semitendinosusasapredictorofgraftdiameter ≤8mmor>8mm
The analysis presented below aimed to evaluate whether thesumofgracilis+semitendinosuswoulddiscriminatewell betweengraftdiameter≤8mmor>8mm.
Alogisticregressionmodelwasadjusted,consideringthe sumofgracilis+semitendinosusastheexplanatoryvariable
6.6 6.4 6.2 6.0 5.8 5.6 5.4 5.2 5.0 4.8 4.6 4.4 4.2 4.0 3.8
Gracilis+Semitendinosus 5.5
6.0 6.5 7.0 7.5 8.0 8.5 9.0 9.5 10.0 10.5
Intra-operative graft
Pearson’s correlation coeficiente: 0.74 (P<.001)
Fig.5–Sumofgracilis+semitendinosus×diameterofthe
Table3–Probabilityofgraftdiameter.
Gracilis+semitendinous Probabilityofgraftdiameter
greaterthan8mm
3.5 0.001
4 0.005
4.5 0.035
5 0.201
5.5 0.632
6 0.922
6.5 0.988
7 0.998
andthediameterofthegraft(≤8mmor>8mm)asthe
depend-entvariable.Thenullhypothesisthatthereisnoassociation betweenthesumgracilis+semitendinosusandtheprobability thatthegraftdiameteris>8mmwastestedagainstthe alter-nativehypothesisthatthereissuchanassociation.Thetest resultindicatedtherejectionofthenullhypothesis(p=0.001) andindicatedthatthesumofgracilis+semitendinosus sig-nificantlyinfluencestheprobabilitythatthegraftdiameteris >8mm.
Table3and Fig.6presentthe valuesofthe sumof gra-cilis+semitendinosusandtherespectiveprobabilitythatthe graftdiameteris>8mm,estimatedbytheadjustedmodel.
Determinationofacutoffpointforthesumof gracilis+semitendinosusthatisassociatedwithgraft diameter≤8mmor>8mm(ROCcurve)
A ROC curve was adjusted for the sum of gra-cilis+semitendinosus and considered the diameter of the graft(≤8mmor>8mm).Theareaunderthecurvewas0.87, withstatisticalsignificance(p<0.001).Thisindicatesthatthe curve fit is good and the sum of gracilis+semitendinosus discriminateswellbetweendiameter≤8mmor>8mm.
The optimal cutoff point for the sum of gra-cilis+semitendinosus was equal to 5.28, with sensitivity of75%andspecificityof85.7%.Table4presentstheseresults. Sensitivity: probability that the sum of gra-cilis+semitendinosus is >5.28 if the graft diameter is >8mm.
0.0 0.2 0.4 0.6 0.8 1.0
Probability of graft diamete
r>
8
4
3.5 4.5 5 5.5
Gracilis+Semitendinosus
6 6.5 7
Fig.6– Probabilityofgraftdiameter.
Table4–Sensitivityandspecificityaccordingtothe cutoffpoint.
Gracilis+semitendinosus Graftdiameter(mm)
≤8 >8
≤5.28 24 4
85.7%(specif) 25%
>5.28 4 12
14.3% 75%(sensit)
Total 28 16
Specificity: probability that the sum of gra-cilis+semitendinosus is ≤5.28 if the graft diameter is
≤8mm.
Fig.7showstheadjustedROCcurve.
Fig.8presentsthesensitivityandspecificityvaluesfor var-iousvaluesofthesumofgracilis+semitendinosus.
Discussion
Inthisstudy,asignificantcorrelationwasobservedbetween themeasurementsofthediameterofthetendonsonMRIand thesizeobtainedinsurgery.
Nostudieswereretrievedintheliteratureinwhich mea-surementswere madein asimilarway, i.e., measuringthe tendons ofthe semitendinosusand gracilisattheirlargest diameterintheaxialplanewiththecutofflevelatthemedial femoralepicondyle.
Beyzadeogluetal.1observedstatisticalsignificanceinthe measurementofthecross-sectionalareaoftheflexortendons measuredattwolevelsonMRIandgraftsizeobtained intra-operativelyin51patients.Thediameterswerealsomeasured atthesetwolevels. However,nosignificantcorrelationwas observed.
Inasimilarstudy,Bickeletal.19observedasignificant cor-relationbetweenthesumofthesemitendinosusandgracilis areas measuredonMRIwithvaluesabove18mm2 and the
achievementofasuitable-sizedgraftin88%ofcases.
1.0
0.8
0.6
0.4
0.2
0.0
0.6 0.4
0.2 0.0
1-specificity
Sensitivity
1.0 0.8
0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0
6.4 6.2 6.0 5.8 5.6 5.4 5.2 5.0 4.8 4.6 4.4 4.2 4.0 3.8
Sensitivity/specificity
Gracilis+Semitendinosus
Sensitivity
Specificity
5.28
Fig.8–Sensitivityandspecificityforvariousvaluesofthe sumofgracilis+semitendinosus.
In another study, Wernecke et al.16 examined the area ofthe tendonsof34 patientson MRIand recommended a 10mm2-areaforthe gracilistendonand a17mm2-area for
thesemitendinosustendontoobtainasuitablesized graft, consideringaquadruplegraft.
Hamadaetal.18measuredthesemitendinosusareaatMRI in79patientsanddemonstratedthat,whentheareaislarger than11mm2,agraftgreaterthanorequalto7mmisachieved
duringsurgeryin89%ofcases.
Differently,Yasumotoetal.20showedthatpredictionofthe graftsizeispossiblebyexaminingthree-dimensional com-putedtomographyin28patients.
Otherstudieshaveattemptedtopredictthechanceof fail-ure in ACL reconstruction using data suchas gender, age, weight, height,and bone massindex (BMI). These studies, in general, have shown that eutrophic (>50kg) and short (>140–147cm)womenaremorelikelytohavegraftssmaller than7mm.9,13,15
Magnussenetal.10analyzedgraftsizeandageofpatients aspredictors ofearly revisionACL reconstruction. Authors demonstratedthattheuseofgraftssmallerthanorequalto 8mmandpatientsyoungerthan20yearsareassociatedwith higherratesofrevisionsurgery.
Inthepresentstudy,wedemonstratedthatpredictionof thegraftsizethatwillbeobtainedforACLreconstructionis possiblebymeasuringthediameterintheaxialplanewiththe cutofflevelatthemedialfemoralcondyle.
Throughmeasurementsand theproposedalgorithm, an estimateddiameterof2.618+1.107(gracilis+semitendinosus) canindicatetheapproximategraftsize.
Anothermethodtoassesswhetherthegraftwillhavean appropriatesizeissummingthediametersofthetendons.If sumofgracilis+semitendinosusisgreaterthan5.28mm,the probabilityofobtainingagraftgreaterthan8mmis75%.
Probably,withagreaternumberofcases,especiallythose withgraftssmallerthanorequalto7,resultswillbeevenmore accuratetopredictgraftdiameter.
Conclusion
Thisstudydemonstratedthatmeasuringthediameterofthe gracilisandsemitendinosustendonsonpreoperativeMRIis asimpleandeffectivemethodtopredictthefinalsizeofthe grafttobeusedinACLreconstructionsurgery.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.BeyzadeogluT,AkgunU,TasdelenN,KarahanM.Prediction ofsemitendinosusandgracilisautograftsizesforACL reconstruction.KneeSurgSportsTraumatolArthrosc. 2012;20(7):1293–7.
2.KupczikF,SchiavonMEG,SbrissiaB,FávaroRC,ValérioR. Enxertoidealparaligamentocruzadoanterior:correlacãoem ressonânciamagnéticaentreLCA,isquiotibiais,tendão patelaretendãoquadríceps.RevBrasOrtop.2013;48(5):441–7. 3.KweonC,LedermanES,ChhabraA.Anatomyand
biomechanicsofthecruciateligamentsandtheirsurgical implications.In:FanelliGC,editor.Themultipleligament injuredknee.NewYork:Springer-Verlag;2013.p.17–27. 4.StaeubliHU,AdamO,BeckerW,BurgkartR.Anteriorcruciate
ligamentandintercondylarnotchinthecoronaloblique plane:anatomycomplementedbymagneticresonance imagingincruciateligament-intactknees.Arthroscopy. 1999;15(4):349–59.
5.DuthonVB,BareaC,AbrassartS,FaselJH,FritschyD, MénétreyJ.Anatomyoftheanteriorcruciateligament.Knee SurgSportsTraumatolArthrosc.2006;14(3):204–13.
6.TsukadaH,IshibashiY,TsudaE,FukudaA,TohS.Anatomical analysisoftheanteriorcruciateligamentfemoralandtibial footprints.JOrthopSci.2008;13(2):122–9.
7.AraujoP,vanEckCF,TorabiM,FuFH.Howtooptimizetheuse ofMRIinanatomicACLreconstruction.KneeSurgSports TraumatolArthrosc.2013;21(7):1495–501.
8.GirgisFG,MarshallJL,MonajemA.Thecruciateligamentsof thekneejoint.Anatomical,functionalandexperimental analysis.ClinOrthopRelatRes.1975;106:216–31. 9.TremeG,DiduchDR,BillanteMJ,MillerMD,HartJM.
Hamstringgraftsizeprediction:aprospectiveclinical evaluation.AmJSportsMed.2008;36(11):2204–9. 10.MagnussenRA,LawrenceJT,WestRL,TothAP,TaylorDC,
GarrettWE.Graftsizeandpatientagearepredictorsofearly revisionafteranteriorcruciateligamentreconstructionwith hamstringautograft.Arthroscopy.2012;28(4):526–31. 11.DwyerT,WhelanDB,KhoshbinA,WassersteinD,DoldA,
ChahalJ,etal.Thesizingofhamstringgraftsforanterior cruciatereconstruction:intra-andinter-observerreliability. KneeSurgSportsTraumatolArthrosc.2015;23(4):1197–200. 12.ConteEJ,HyattAE,GattCJJr,DhawanA.Hamstringautograft
sizecanbepredictedandisapotentialriskfactorforanterior cruciateligamentreconstructionfailure.Arthroscopy. 2014;30(7):882–90.
13.TumanJM,DiduchDR,RubinoLJ,BaumfeldJA,NguyenHS, HartJM.Predictorsforhamstringgraftdiameterinanterior cruciateligamentreconstruction.AmJSportsMed. 2007;35(11):1945–9.
15.MaCB,KeifaE,DunnW,FuFH,HarnerCD.Canpre-operative measurespredictquadruplehamstringgraftdiameter?Knee. 2010;17(1):81–3.
16.WerneckeG,HarrisIA,HouangMT,SeetoBG,ChenDB, MacDessiSJ.Usingmagneticresonanceimagingtopredict adequategraftdiametersforautologoushamstring double-bundleanteriorcruciateligamentreconstruction. Arthroscopy.2011;27(8):1055–9.
17.NakayamaY,ShiraiY,NaritaT,MoriA,KobayashiK.The accuracyofMRIinassessinggraftintegrityafteranterior cruciateligamentreconstruction.JNipponMedSch. 2001;68(1):45–9.
18.HamadaM,ShinoK,MitsuokaT,AbeN,HoribeS. Cross-sectionalareameasurementofthesemitendinosus
tendonforanteriorcruciateligamentreconstruction. Arthroscopy.1998;14(7):696–701.
19.BickelBA,FowlerTT,MowbrayJG,AdlerB,KlingeleK,Phillips G.Preoperativemagneticresonanceimagingcross-sectional areaforthemeasurementofhamstringautograftdiameter forreconstructionoftheadolescentanteriorcruciate ligament.Arthroscopy.2008;24(12):1336–41.