SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Influence
of
proximal
femur
fractures
in
the
autonomy
and
mortality
of
elderly
patients
submitted
to
osteosynthesis
with
cephalomedullary
nail
夽
Rodrigo
Souto
Borges
Petros
∗,
Paula
Emília
Valente
Ferreira,
Rafael
Souto
Borges
Petros
CentroOrtopédicoTraumatológicoTijuca,HospitalTijutrauma,RiodeJaneiro,RJ,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received30November2016 Accepted26January2017 Availableonline26August2017
Keywords:
Hipfractures Femoralfractures Independentliving Ambulation Elderly
a
b
s
t
r
a
c
t
Objective:Todeterminetheautonomyandmortalityofelderlypatientssubmittedto proxi-malfemoralosteosynthesiswithcephalomedullarynailafterhipfracture.
Methods:Retrospectivestudywith61patientswithproximalfemoralfracturessubmittedto cephalomedullarynailosteosynthesis.Theauthorsanalyzedthemedicalrecordsand col-lectedinformationfromthepreoperativeperiod.Patientswerequestionedregardingpain, postoperativeautonomy,anddegreeofsatisfaction.Thetotalnumberofdeathswasverified. Theresultswerethencorrelated.
Results:Themeanagewas84years,predominantlyfemale(82%).Inthepostoperative eval-uation,45%ofthepatientspresentedworsenedlevelsofautonomy.Themajorityofpatients presentedmildpain(61%)ontheVASscale.Themortalityratewas24.6%,andthemean timeofpreoperativehospitalizationwasthreedays.Thefactorsthatpresentedstatistical significanceregardingpostoperativeautonomywerethetimeelapsedfromthetraumauntil themomentofsurgery,ASAscore,fracturestability,andpreviousfunctionalstatusofthe patients.Themortalityratewasassociatedwiththreemainfactors:advancedage,ASA score,andpreoperativehospitalizationtime.
Conclusion: Thepatient’spreviousautonomypositivelyinfluencedthefunctionaloutcome andpostoperativerecovery.Unstablefracturespresentedworseresultsforpainand ambu-lationinafollow-upof27months.Hipfractureisariskfactorassociatedwithmortalityand decreasedindependenceinpatientsover65yearsofage.
©2017PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeOrtopedia eTraumatologia.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedatHospitalTijutrauma,CentroOrtopédicoTraumatológicoTijuca,RiodeJaneiro,RJ,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](R.S.Petros).
http://dx.doi.org/10.1016/j.rboe.2017.08.014
Influência
das
fraturas
do
fêmur
proximal
na
autonomia
e
mortalidade
dos
pacientes
idosos
submetidos
a
osteossíntese
com
haste
cefalomedular
Palavras-chave:
Fraturasdoquadril Fraturasdofêmur Vidaindependente Deambulac¸ão Idoso
r
e
s
u
m
o
Objetivo: Determinara autonomiaeamortalidadedepacientesidososapósfraturado quadrilsubmetidosaosteossíntesedofêmurproximalcomhastecefalomedular.
Métodos: Estudoretrospectivocom61pacientescomfraturadofêmurproximalsubmetidos aosteossíntesecomhastecefalomedular.Osprontuáriosforamanalisadoseosregistros clínicosdopré-operatórioforamcoletados.Ospacientesforamreavaliadoseperguntados emrelac¸ãoador,autonomiapós-operatóriaegraudesatisfac¸ão.Foiverificadoonúmero totaldeóbitos.Osresultadosforamentãocorrelacionados.
Resultados: Amédiadeidadefoide84anos,compredominânciadosexofeminino(82%). Na avaliac¸ão pós-operatória, 45% dos pacientes apresentaram pioria em seu nível de autonomia.A maioriados pacientesapresentoudor leve(61%)pelaescalaEVA.Ataxa de mortalidadeencontradafoi de24,6%eotempomédiodeinternac¸ão pré-operatória foi detrêsdias.Osfatoresqueapresentaramsignificânciaestatísticaquantoà autono-miapós-operatóriaforamotempodecorridodotraumaatéomomentodacirurgia,escore ASA,estabilidadedafraturaeestadofuncionalpréviodopaciente.Ataxademortalidade foiassociadaatrêsfatoresprincipais:idadeavanc¸ada,escoreASAetempodeinternac¸ão pré-operatória.
Conclusão:Aautonomiapréviadopacienteinfluencioupositivamenteoresultadofuncional earecuperac¸ãopós-operatória.Fraturasinstáveisapresentarampioresresultadosparador edeambulac¸ãoemumseguimentode27meses.Afraturadoquadriléumfatorderisco associadoàmortalidadeediminuic¸ãodaindependênciaempacientesacimade65anos.
©2017PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileirade OrtopediaeTraumatologia.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Theincidenceofproximalfemoralfractureshasincreased sig-nificantlyinthelastdecadesandisexpectedtodoublewithin thenext25years,duetoincreasinglifeexpectancy.Olderage andassociatedcomorbiditiesare responsible forhigh mor-bidity and mortality, as well as higher costs oftreatment and hospitalization.1 Among proximal femoral fractures,
the transtrochantericfracture is animportantgroup, since theyare commonandusuallyaffectdebilitatedandelderly patients.2,3Thesefracturesaredefinedasthoseoccurringin
theareaextendingfromtheextracapsularregionofthebase ofthe femoral neckto a proximalregion along the minor trochanter.4
Thistypeoffractureiscommonintheelderlypopulation duetoosteoporosis,andismainlyassociatedwithlow-energy trauma,suchasfallfromtheirownheight.Itisestimatedthat nineoutoftentrochantericfracturesoccurinindividualsolder than65years.5,6
Hip fracture is a devastating injury in elderly patients, affectingtheirphysical,mental,functional,andsocial func-tion.Itreflectstheagingprocessofthepopulation,andhas permanentconsequenceson patientsurvivaland indepen-dence.
Surgical stabilization isthe option of choiceto manage trochantericfractures,regardlessofdeviationtypeorpattern. Thegoalofsurgicaltreatmentistoachievestablereduction
andfixation,allowingearlyactiveandpassivemobilization. Sinceelderlyindividualsarenotalwaysabletowalkwithout placing some load on the fractured limb, due to the pre-existing conditions,fracturestabilizationmustbesufficient toallowacertainloadtoleratedbythepatient.7
Studies demonstrate that up to 50% of patients with proximal femoralfractures diewithin the first sixmonths after trauma, and that many patients submitted to sur-gical treatment do not regain their baseline function and independence.8
Thisstudy aimedto determinetheautonomy and mor-tality ofelderly patientswho underwent proximalfemoral osteosynthesiswithcephalomedullarynailafterhipfracture.
Methods
Alongitudinal,retrospective,anddescriptivestudywas per-formedwith61patientswithproximalfemoralfracturewho underwentosteosynthesiswithcephalomedullarynailfrom March 2012to March2014, at the Hospitalde Ortopedia e Traumatologia,RiodeJaneiro,Tijutrauma.
Patients’medicalrecordswereanalyzedandinformation fromthepre-operativeclinicalrecords(clinicalevolutionand surgicalrisk)wascollected.
(ASA)score;andpre-traumaautonomy,dividedintofive walk-ingpatterns:(1) Walksoutsidehomecommunity distances withouthelp;(2)Walksoutsidehomecommunitydistances withhelp; (3) Walkshousehold distanceswithout help; (4) Walks household distances with help; (5) Non-ambulatory orwheelchairuser.Patientswithincompletemedicalcharts wereexcludedfromthesample.
Aftercollection ofcomplete preoperative data, patients wereinterviewedandunderwentclinicalevaluationtoassess painthroughavisualanalogscale(VAS),postoperative walk-ingstatus,anddegreeofsatisfaction.Atfollow-up,thetotal numberofdeathsaftersurgicaltreatmentwasusedto deter-mine the mortality rate. Patients who did not attend the intervieworwhowerelostfollow-upwereexcluded.
Datacollectedinthepre-andpostoperativeperiodswere then correlated with mortality and with influence on the patients’autonomy.
Forstatisticalanalysisoftheresults,tableswithabsolute and relative frequencydistribution were used. The associ-ationswere testedbyPearson’schi-squaredtestorFisher’s exacttest.NormalitywasassessedbytheShapiro–Wilktest, andcontinuousvariableswereassessedbyStudent’st-testor ANOVA.
Results
Themeanageofthepatientswas84years(±7.2),rangingfrom 67to97.Themalegrouppresentedaslightlyhighermeanage thanthefemalegroup(86[±8.0]yearsvs.83[±7.0], respec-tively,withoutstatisticalsignificance[p=0.260]).Lateralityof theaffectedhipwassimilar(50.8%and49.2%,respectively).
Asignificant difference wasobserved in the prevalence betweensex(p<0.001);asmostcases(82.0%)werefemale,that is,onaverage,surgicalproceduresforproximalfemoral frac-turewereperformed4.5timesmoreofteninwomenthanin men(Fig.1).
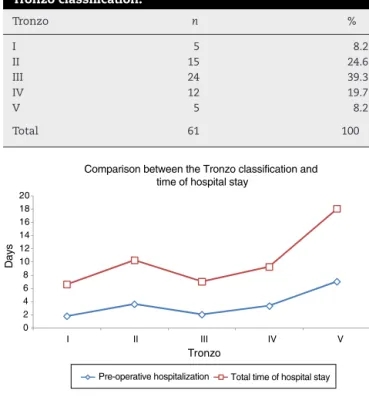
Regardingfractureclassification,24 patients(39.3%) pre-sentedTronzo typeIII, whiletypeIIwasobservedin24.6% (Table1).
Meanhospitalizationtimewas9days,rangingfrom2to 27.Meanhospitalizationtimebeforesurgerywas3days,
ran-Female 82% p < 0.0001 Males
18%
Fig.1–Frequencybysexoftheelderlysubmittedto surgicaltreatmentwithtranstrochantericfracture.
Table1–Correlationbetweenoperatedpatientsandthe Tronzoclassification.
Tronzo n %
I 5 8.2
II 15 24.6
III 24 39.3
IV 12 19.7
V 5 8.2
Total 61 100
0 2 4 6 8 10 12 14 16 18 20
V IV
III II
I
Days
Tronzo
Comparison between the Tronzo classification and time of hospital stay
Pre-operative hospitalization Total time of hospital stay
Fig.2–ComparisonbetweentheTronzoclassificationand hospitalizationtime.
gingfrom1to14.PatientsclassifiedasTronzotypeVhadthe highestmeanpre-operativehospitalization:7days(p=0.0047) (Table2andFig.2).
Inthepreoperativeassessment,21patientswereableto walk outside homeforcommunitydistanceswithout help. Aftersurgery,15patients(71.4%)maintainedthiscondition and33.3%worsenedtheirwalkingstatus.Ofthepatientswho wereabletowalkoutsidetheirhomeforcommunitydistances withhelp,six(50%)maintainedtheirconditionand50% wors-ened.Ofthe10patientswhowereabletowalkforhousehold distanceswithouthelp,44.4%maintainedtheirconditionand 55.6%worsened. Ofthe patientswhowere abletowalkfor householddistanceswithhelp,60.0%maintainedtheir con-ditionand40.0%worsened.Therefore,whencomparingthe pre-andpost-operativegeneralambulationstatus,45%ofthe patientspresentedadecreaseintheirleveloffunctional inde-pendence(Table3).TheVASscalewasappliedaftersurgery and mostpatients (60.9%)presentedmildpainwhile37.0% presentedmoderate pain. Onlyone patient(2.2%) reported severepain.Whenaskedaboutthedegreeofsatisfaction,90% ofthepatientsweresatisfiedwiththeresultofthesurgery;the remaining10%weredissatisfiedwithnotbeingabletowalk orwithlivinginnursinghomes,astheydidnotregaintheir previousindependence.
Patients with a moresevere Tronzo score had a higher meanVAS,butthedifferencewasnotstatisticallysignificant (p=0.057).
Table2–ComparisonbetweentheTronzoclassificationandmeantimeofhospitalstay.
Tronzo Meanpre-operativehospitalization p Meantotaltimeofhospitalstay p
I 1.8 0.0047 6.6 0.0020
II 3.6 10.3
III 2.0 7.0
IV 3.3 9.3
V 7.0 18.0
Total 3.1 9.1
Table3–Comparisonbetweenpre-andpost-operative walkingstatus.
Walkingstatus Evaluation
Pre-operative Post-operative
n % n %
Walksoutsidehomefor communitydistances withouthelp
21 45.7 15 32.6
Walksoutsidehomefor communitydistances withhelp
6 13 8 17.4
Walksforhousehold distanceswithouthelp
9 19.6 3 6.5
Walksforhousehold distanceswithhelp
10 21.7 13 28.3
Non-ambulatory, wheelchairuser
0 0 7 15.2
Total 46 100 46 100
0 2 4 6 8 10 12
Moderate or severe Mild
Days
EVA
Comparison between level of pain (VAS) and time of hospital stay
Pre-operative hospitalization Total time of hospital stay
Fig.3–Comparisonbetweenlevelofpain(VAS)and hospitalizationtime.
scale (p=0.016), aswastotal hospitalizationtime (p=0.026;
Fig.3).
Fifty-eightpatients(95.1%)hadatleastonepreoperative comorbidity.Onlythreepatients (4.9%)had nopre-existing disease.
The five most common co-morbidities were: SAH (39 patients; 63.9%), dyslipidemia(14 patients, 22.9%),diabetes (10patients,16.4%),cardiopathy(sevenpatients,11.5%),and hypothyroidism(sevenpatients,11.5%).
The mortality rate found in the study was 24.6% (15 deaths). Three factors were significantly associated with highermortalityinthesepatients:advancedage,ASAscore, andpreoperativehospitalizationtime(Table4).Meanageof the patients who died was 87.6 years,versus 82.5 ofthose patientswhowerealive(p=0.016).PatientsclassifiedasASAIII
Table4–Factorsassociatedwithhighermortalityrate.
Variable Alive
n=46
Death
n=15
p
Age–mean(±SD) 82.5(±6.7) 87.6(±7.5) 0.16
Gender–n(%)
Male 7(63.3%) 4(36.4%) 0.810 Female 39(78.0%) 11(22.0%)
Tronzo–n(%)
Stable 16(80.0%) 4(20.0%) 0.561 Unstable 30(73.2%) 11(26.8%)
ASA–n(%)
IandII 26(86.7%) 4(13.3%) 0.45 IIIandIV 20(64.5%) 11(35.5%)
Preoperativehospitalization–n(%)
Upto48h 30(85.7%) 5(14.3%) 0.30 Over48h 16(61.5%) 10(38.5%)
Associatedlesion,n(%)
Zeroto3 35(81.4%) 8(18.6%) 0.093 Over3h 11(61.1%) 7(38.8%)
Totaltimeofhospitalstay–n(%)
Upto7days 25(78.1%) 7(21.9%) 0.605 Over7days 21(72.4%) 8(27.6%)
orIVpresentedahighermortalityratethanthoseclassifiedas ASAIorII:35.5%versus13.3%,respectively.Regardingthe pre-operativehospitalizationtime,themortalityrateofpatients whowereoperatedonwithin48hofthefracturewas14.3%.In patientswhowereoperatedonafterover48hofthefracture, themortalityrateincreasedto38.5%.
Factors suchas Tronzoclassification,gender, numberof associateddiseases,andtotalhospitalizationtimewerenot associatedwithmortality.
Discussion
Transtrochantericfemoralfracturesarethemostfrequently operatedfracturetype,andpresentthehighestpostoperative mortalityrate;theyhavebecomeapublichealthcareissue, duetothehighcostoftreatmentandthedifficultyof recover-ingpostoperativefunctionalindependence.4
Theepidemiologicalprofileoftheindividualsinthepresent sample was not much different from those observed in Brazilian and internationalstudies.In the present study,a predominanceoffemaleswasobserved,ata4.5:1ratio;their mean age was 84 years.Comparing withBrazilianstudies, HungriaNetoetal.2foundapredominanceofwomeninthe
proportionof2:1andameanageof78.2years;Ramalhoetal.9
Inthepresentstudy,weobservedthatthedegreeof auton-omydecreasedaftersurgicaltreatment.8Nonetheless,55%of
thepatientsrecoveredtheirfunctionallevel.Asimilarfinding wasobservedbyHerreraetal.10intheirworkwith250patients
treatedwithcephalomedullarynail,inwhichapproximately 50%recoveredtheirpreviouswalkingstatusafteroneyear.
Patients’ previous autonomy positively influenced the functional outcome and the postoperative recovery. We observedthat71.4%ofpatientswhowereabletowalk out-sidehomeforcommunitydistanceswithouthelpmaintained theirlevelaftersurgery.Thisdemonstratesthatmore physi-callyindependentpatientspresentbetterresults.Zuckerman etal.11,12 observedthatthegroupofpatientswiththebest
pre-fracturescorerecoveredalmost100%oftheirfunctional capacity.
Regarding pain intensity after surgical treatment of transtrochanteric fractures, most operated patients (60%) had mildpain; similar datawere retrieved inthe Brazilian literature.13
Themortalityratein thepresent study was 24.6%,ata meanfollow-upof27months.Inastudywith1448patients, Rossoetal.14foundamortalityrateof18.8%inoneyearof
follow-up,whileDousaetal.,15inastudywith4280patients,
observeda30%deathrate.
Cooperetal.16statedthattheconsequencesofahip
frac-tureincludeprematuredeath(around20%inoneyear),lossof function(in30%),inabilitytowalkindependently(40%),and lossofatleastoneindependentdailyactivity(in80%ofthe patientstreated).
Some factors were statisticallysignificant formortality, suchastimeelapsedfromtraumatosurgery,ASAscore, frac-turestability,andageatthetimeoftrauma.
Inthepresentstudy,patientswithpreoperative hospital-izationtime greater than 48h had a 38.5% mortality rate, whilepatientswho underwent surgical treatmentin up to 48hhadalowerrate,14.3%.Regardingthetimeofsurgical delay,Hamlet et al.17 demonstrated that patients operated
withinthefirst 24hofadmissionhad lowermortalitythan thoseoperatedafter24h,regardlessofthepreoperativeASA score.Thehighermortalityrateassociatedwithsurgicaldelay demonstratestheimportanceoftheearlytreatmentofthese fractures,whicharenowtreatedasorthopedicemergencies. Somefactorsunderminetheimprovementofthistreatment, suchasovercrowdingofpublichospitals,bureaucracyfor sur-gical authorization, availability ofthe necessary materials, andavailabilityofmedicalstaff.
Anotherfactorthatwasstatisticallysignificantfor mortal-itywastheASAscore.Onlyfourdeaths(6.5%)wereobserved inpatientsclassifiedasASAIandII,versus11(18%)inpatients classifiedasASAIIIandIV.Micheletal.18demonstratedthat
patients classified as ASA III or IV had a nearly nine-fold greaterriskofdeathinthefirstpostoperativeyearthanthose classifiedasASAIorII(p<0.001).
Conclusion
Patient’spreviousautonomypositivelyinfluencedfunctional outcomeandpostoperativerecovery.
Inafollow-upof27months,unstablefracturespresented worseresultsforpainandwalkingstatus.
Hipfractureisariskfactorassociatedwithmortalityand decreased autonomyinpatients agedover 65 years.These fractures are devastatinginjuriesthatshould betreatedas orthopedicemergencies.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.BorgerRA,LeiteFA,AraújoRP,PereiraTFN,QueirozRD. Avaliac¸ãoprospectivadaevoluc¸ãoclínica,radiográficae funcionaldotratamentodasfraturastrocantéricasinstáveis dofêmurcomhastecefalomedular.RevBrasOrtop. 2011;46(4):380–9.
2.HungriaNetoJS,DiasCR,AlmeidaJDB.Características epidemiológicasecausasdafraturadoterc¸oproximaldo fêmuremidosos.RevBrasOrtop.2011;46(6):660–7.
3.RochaMA,CarvalhoWS,ZanquetaC,LemosSC.Estudo epidemiológicoretrospectivodasfraturasdofêmurproximal tratadosnoHospitalEscoladaFaculdadedeMedicinado TriânguloMineiro.RevBrasOrtop.2001;36(8):311–6.
4.RockwoodCA,GreenDP.Fraturasintertrocantéricas.In: BucholzRW,Court-BrownCM,HeckmanJD,TornettaP3rd, editors.FraturasemadultosdeRockwood&Green.SãoPaulo: Monelo;2013.p.1597–640.
5.ParkerMJ,HandollHH.Intramedullarynailsforextracapsular hipfracturesinadults.CochraneDatabaseSystRev.
2009;(3):CD004961.
6.KaplanK,MiyamotoR,LevineBR,EgolKA,ZuckermanJD. Surgicalmanagementofhipfractures:anevidence-based reviewoftheliteratureII.Intertrochantericfractures.JAm AcadOrthopSurg.2008;16(11):665–73.
7.GuimarãesJAM,GuimarãesACA,FrancoJS.Avaliac¸ãodo empregodahastefemoralcurtanafraturatrocantérica instáveldofêmur.RevBrasOrtop.2008;43(9):406–17.
8.BeckerC,FleischerS,HackA,HindererJ,HornA,ScheibleS, etal.Disabilitiesandhandicapsduetohipfracturesinthe elderly.ZGerontolGeriatr.1999;32(5):312–7.
9.RamalhoAC,Lazaretti-CastroM,HauacheO,VieiraJG,Takata E,CafalliF,etal.Osteoporoticfracturesofproximalfemur: clinicalandepidemiologicalfeaturesinapopulationofthe cityofSãoPaulo.SãoPauloMedJ.2001;119(2):48–53.
10.HerreraA,DomingoLJ,CalvoA,MartinezA,CuencaJ. Comparativestudyoftrochantericfracturestreatedwiththe Gammanailortheproximalfemoralnail.IntOrthop. 2002;26(6):365–9.
11.ZuckermanJD,KovalKJ,AharonoffGB,SkovronML.A functionalrecoveryscoreforelderlyhipfracturepatients:II. Validityandreliability.JOrthopTrauma.2000;14(1):26–30.
12.ZuckermanJD,KovalKennethJ,AharonoffGinaB,HiebertR, SkovronML.Afunctionalrecoveryscoreforelderlyhip fracturepatients:IDevelopment.JOrthopTrauma. 2000;14(1):20–5.
13.LimaAL,AzevedoFilhoAJ,AmaralNP,FranklinCE,Giordano V.Tratamentodasfraturasintertrocanterianascomplacae parafusodeslizante.RevBrasOrtop.2003;38(5):271–80.
15.DousaP,CechO,WeissingerM,DzupaV.Trochantericfemoral fractures.ActaChirOrthopTraumatolCech.2013;80(1):15–26.
16.CooperC.Thecripplingconsequencesoffracturesandtheir impactonqualityoflife.AmJMed.1997;103(2A):17S–9S, 12S–17S;discussion.
17.HamletWP,LiebermanJR,FreedmanEL,DoreyFI,FletcherA, JohnsonEE.Influenceofhealthstatusandthetimingof
surgeryonmortalityinhipfracturepatients.AmJOrthop. 1997;26(9):621–7.