SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
Magnetic
resonance
imaging
without
contrast
as
a
diagnostic
method
for
partial
injury
of
the
long
head
of
the
biceps
tendon
夽
Alexandre
Tadeu
do
Nascimento
∗,
Gustavo
Kogake
Claudio
HospitalOrthoservice,GrupodeOmbroeCotovelo,SãoJosédosCampos,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received12November2015 Accepted7January2016
Availableonline20December2016
Keywords:
Sensitivityandspecificity Rotatorcuff
Magneticresonanceimaging
a
b
s
t
r
a
c
t
Objective:Toevaluate theuseofmagneticresonanceimaging(MRI)without contrastas adiagnosticmethodofpartiallesionsofthelongheadofthebiceps,usingarthroscopic surgeryasthegoldstandard.
Methods:WeevaluateddatafromMRIandarthroscopicsurgicalfindingsofpatientsoperated duetorotatorcuffandSLAPinjuries.MRIwithoutcontrastofatleast1.5T,witharadiologist report,wasusedasacriterionforthedetectionoflongheadofthebicepsinjury.Allcases wereoperatedbythesamesurgeonatthishospital.
Results:Thisstudyevaluateddatafrom965patients,311women(32%)and654men(68%), withameanageof45years,whounderwentarthroscopicsurgeryforrotatorcuffandSLAP repairfromSeptember2012toSeptember2015.Overall,thesensitivityandspecificityof MRIwas0.22(CI:0.17–0.26)and0.98(CI:0.96–0.99),respectively.
Conclusions:MRIhasalowsensitivityandhighspecificityfordetectionofpartialtearsofthe longheadofthebicepstendon.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Avaliac¸ão
da
ressonância
magnética
sem
contraste
como
método
para
diagnóstico
de
lesões
parciais
do
tendão
da
cabec¸a
longa
do
bíceps
Palavras-chave:
Sensibilidadeeespecificidade Manguitorotador
Imagemporressonânciamagnética
r
e
s
u
m
o
Objetivo:Avaliararessonânciamagnética(RM)semcontrastecomométododiagnósticoda lesãoparcialdacabec¸alongadobícepscomousodacirurgiaartroscópicacomopadrão ouro.
夽
StudyconductedattheHospitalOrthoservice,GrupodeOmbroeCotovelo,SãoJosédosCampos,SP,Brazil. ∗ Correspondingauthor.
E-mails:[email protected],[email protected](A.T.Nascimento).
http://dx.doi.org/10.1016/j.rboe.2016.12.003
Métodos: ForamavaliadosdadosdeRMeachadoscirúrgicosartroscópicosdepacientes operadosdevidoàlesãodomanguitorotadoreàlesãodoaltodolabrumdeanteriorpara pos-terior(doinglêssuperiorlabralanteriortoposteriorSLAP).Foiusadocomocritériodedetecc¸ão delesãodacabec¸alongadobícepsressonânciamagnéticasemcontrastedenomínimo 1,5Tesla,comlaudoderadiologistas.Todososcasosforamoperadosporumúnicocirurgião emnossohospital.
Resultados: Oestudoavalioudadosde965pacientes,311mulheres(32%)e654homens (68%),commédiade45anos,quesesubmeteramacirurgiaartroscópicaparareparodo manguitorotadoredaSLAP,entresetembrode2012esetembrode2015.Deformageral, asensibilidadeeaespecificidadedaRMfora,de0,22(IC:0,17a0,26)e0,98(IC:0,96a0,99), respectivamente.
Conclusões: ARMtembaixasensibilidadeealtaespecificidadeparadetecc¸ãoderoturas parciaisdotendãodacabec¸alongadobíceps.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Injuriesofthelongheadofthebicepstendonarecommon inpatientswithshoulderpain;surgeryisrequiredin approx-imatelyhalfofcases.Pathologicalchangesofthelonghead ofthebicepstendon includetenosynovitis, partialrupture, completerupture,subluxation,anddislocation.1,2
Althoughinmostcasesthelesionofthelongheadofthe bicepsispartofasyndromeorisassociatedwithother con-ditions,itisnotuncommontoidentifyitasthesolecauseof shoulderpain.3–5
Magneticresonanceimaging(MRI)isroutinelyusedasa methodtoassesscasesofshoulderpainanddiagnose rota-torcuffinjuryandinjuriesofthelongheadofthebiceps.The literatureontheeffectivenessofMRIwithoutcontrast con-sistsofsmallcaseseriesthatexaminedbicepsinjury,butasa secondaryobjective.1,6Thereareonlyfourstudiesthat
specif-icallyexaminedthe validityofMRIwithout contrastinthe detectionofpartialinjuriesofthelongheadofthebiceps ten-donastheprimary goal,noneofwhich wereconductedin Brazil.3,7–9
ThisstudyaimedtoassesstheuseofMRIasadiagnostic methodforpartialruptureofthelongheadofthebiceps ten-don.Arthroscopicsurgerywasadoptedasthegoldstandard (Fig.1).
Material
and
methods
Datafrom965patientsoperatedatasinglecenterbya sin-glesurgeonwereretrospectivelyevaluated.DatafromtheMRI reportofpatientswhowouldundergoarthroscopicsurgeryfor rotatorcuffrepairorSLAPlesionswererecorded,withspecial attentiontothedescriptionoftheconditionsofthelonghead ofthebiceps.Afterarthroscopy,dataonthelongheadofthe bicepswererecordedincasesofpartialruptureofitsfibers.
Inclusioncriteriacomprisedpatientswithadiagnosisof rotatorcuff injuryorSLAP injury, who hadundergone MRI withoutcontrastofatleast1.5Tesla,witharadiologistreport, andwhohadundergonearthroscopicshouldersurgery.
PatientswithMRIoflessthan1.5Tesla,withadiagnosisof instabilityoftheglenohumeraljoint,withcompleteruptureof thelongheadbiceps,andthosewhohadundergoneprevious surgery,inwhichtenotomyortenodesisofthelongheadofthe bicepswasperformed,wereexcludedfromthestudy.Casesof previoussurgerythatdidnotapproachthelongheadofbiceps werenotexcluded.
Arthroscopictreatment
Allsurgicalprocedureswereperformedbythesamesurgeon, withpatientundergeneralanesthesiaandnerveblock,inthe beachchairposition.Bothglenohumeraljointand subacro-mialspacewereexamined,whichallowedfortheassessment oftheglenoidlabrum,rotatorcuff,andlongheadofthebiceps. Thelongheadofthebicepstendonwasdirectlyvisualizedand inspectedfortendinitisandpartialortotalrupture.Onlythe examsinwhichtherewaspartialruptureofthefibersofthe longheadofthebicepstendonwereconsideredaspositive.
Statisticalanalysis
Surgicalfindingswererecordedin2×2tablesastrueandfalse positivesandtrueandfalsenegativesforpartialruptureofthe bicepstendon.Tableswerecreatedtodeterminesensitivity, specificity,predictivevalues,likelihoodratio,andoddsratio, whichwerecalculatedbyExcel.A95%confidenceintervalwas consideredfortheanalysisofalldata.Pearson’scorrelation coefficient was usedto assess the correlationbetween the severityoftheconditionandthepresenceofpartialdamage, throughExcel.Valuesbetween0and0.3wereconsideredasa weakcorrelation;between0.3and0.6,moderatecorrelation; andgreaterthan 0.6,strongcorrelation.Toassessthis rela-tionship,theMann–WhitneytestwasalsousedintheMinitab program.
Results
Fig.1–Examplesofpartiallesionofthelongheadofthebicepsseenonarthroscopy.
Table1–EffectivenessofMRIforthediagnosisoflesionsofthelongheadofthebiceps.
NoIOlesion IOlesion Total
NoMRIlesion 615 263 878
MRIlesion 14 73 87
Total 629 336 965
Sensitivity 22% CI(0.17–0.26)*
Specificity 98% CI(0.96–0.99)*
Accuracy 71% CI(0.68–0.74)*
Positivepredictivevalue 84% CI(0.74–0.91)*
Negativepredictivevalue 70% CI(0.67–0.73)*
Positivelikelihoodratio 9.8 CI(5.6–17.0)*
Negativelikelihoodratio 0.8 CI(0.76–0.85)*
Diagnosticoddsratio 12.2 CI(6.8–22.0)*
IO,intraoperative;MRI,magneticresonanceimaging. ∗ 95%confidenceinterval.
arthroscopicsurgeryforrotatorcuffinjuryrepairandSLAP fromSeptember2012toSeptember2015.Theresultsobtained fromtheassessmentofallpatientstogetherwerecompiled inTable1.Theprevalenceoflesionsofthelongheadofthe bicepswas0.35(CI:0.32–0.38).Patientsweredividedintofour groups,dependingonthedisorderconcernedandthe sever-ityoftheinjury:SLAPinjury(Table2);partialrotatorcufftear (Table3);rotatorcufftear<3cm(Table4);androtatorcufftear >3cm(Table5).
The prevalenceof complete rotator cuff tears was 33% (319/965)throughoutthesample,with53%partialrotatorcuff
tears(513/965)and14%SLAPlesions(133/965).Ofthecomplete tears,7%(70of965)werelargerthan3cmand26%(249of965) weresmallerthan3cm.Theprevalenceofpartiallesionofthe longheadofthebicepswas9%(12of133)inSLAPinjuries,28% (144of513)inpartialsupraspinatuslesions,48%(119of249)in completelesionsofthesupraspinatussmallerthan3cm,and 87%(61of70)inlesionsgreaterthan3cm.Pearson’scoefficient showedamoderatecorrelation(0.38)betweentheseverityof theinjuryandthepresenceofpartialinjuriesofthelonghead ofthebiceps.TheMann–Whitneytestshowedastatistically significantvalueforthiscorrelation,withp<0.0001.
Table2–EffectivenessofMRIforthediagnosisoflesionsofthelongheadofthebiceps,whenassociatedwithSLAP lesions.
NoIOlesion IOlesion Total
NoMRIlesion 117 9 126
MRIlesion 4 3 7
Total 121 12 133
Sensitivity 25% CI(0.08–0.53)*
Specificity 97% CI(0.92–0.98)*
Accuracy 90% CI(0.85–0.95)*
Positivepredictivevalue 43% CI(0.11–0.79)*
Negativepredictivevalue 93% CI(0.86–0.96)*
Positivelikelihoodratio 7.56 CI(1.9–29.9)*
Negativelikelihoodratio 0.78 CI(0.56–1.08)*
Diagnosticoddsratio 9.75 CI(1.9–50.4)*
IO,intraoperative;MRI,magneticresonanceimaging.
Table3–EffectivenessofMRIforthediagnosisoflesionsofthelongheadofthebiceps,whenassociatedwithpartial lesionofthesupraspinatustendon.
NoIOlesion IOlesion Total
NoMRIlesion 364 110 474
MRIlesion 5 34 39
Total 369 144 513
Sensitivity 24% CI(0.17–0.31)*
Specificity 99% CI(0.97–0.99)*
Accuracy 78% CI(0.74–0.82)*
Positivepredictivevalue 87% CI(0.72–0.95)*
Negativepredictivevalue 77% CI(0.73–0.80)*
Positivelikelihoodratio 17.4 CI(6.9–43.7)*
Negativelikelihoodratio 0.77 CI(0.7–0.85)*
Diagnosticoddsratio 22.5 CI(8.6–58.9)*
IO,intraoperative;MRI,magneticresonanceimaging. ∗ 95%confidenceinterval.
Table4–EffectivenessofMRIforthediagnosisoflesionsofthelongheadofthebiceps,whenassociatedwithcomplete lesionofthesupraspinatustendon<3cm.
NoIOlesion IOlesion Total
NoMRIlesion 125 90 215
MRIlesion 5 29 34
Total 130 119 249
Sensitivity 24% CI(0.17–0.32)*
Specificity 96% CI(0.91–0.98)*
Accuracy 62% CI(0.56–0.68)*
Positivepredictivevalue 85% CI(0.68–0.94)*
Negativepredictivevalue 58% CI(0.51–0.64)*
Positivelikelihoodratio 6.34 CI(2.53–15.8)*
Negativelikelihoodratio 0.79 CI(0.70–0.87)*
Diagnosticoddsratio 8.05 CI(3.0–21.6)*
IO,intraoperative;MRI,magneticresonanceimaging.
∗ 95%confidenceinterval.
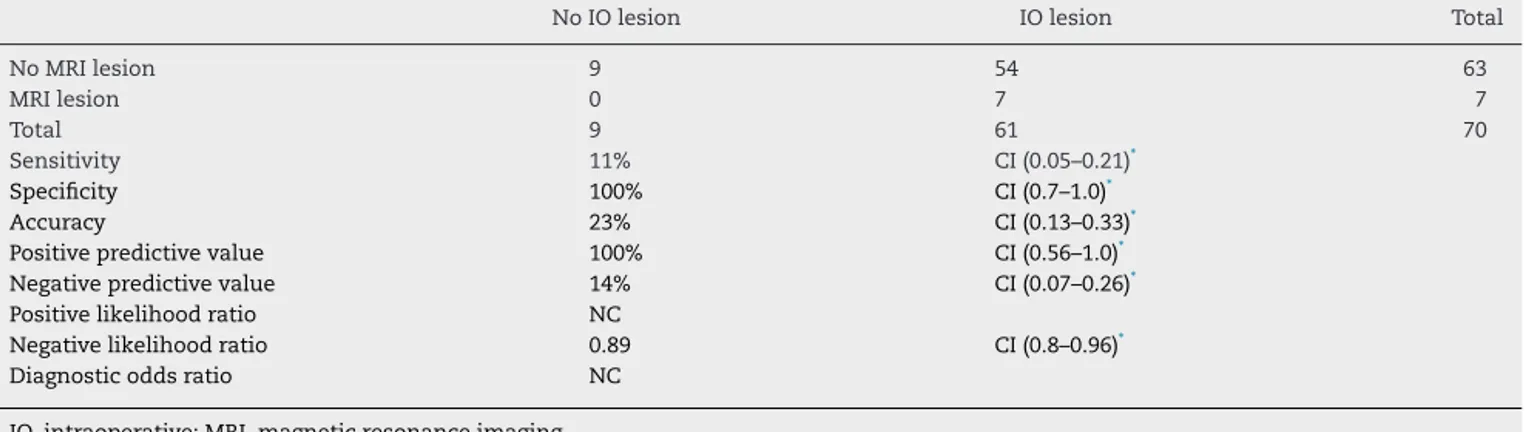
Table5–EffectivenessofMRIforthediagnosisoflesionsofthelongheadofthebiceps,whenassociatedwithcomplete lesionofthesupraspinatustendon>3cm.
NoIOlesion IOlesion Total
NoMRIlesion 9 54 63
MRIlesion 0 7 7
Total 9 61 70
Sensitivity 11% CI(0.05–0.21)*
Specificity 100% CI(0.7–1.0)*
Accuracy 23% CI(0.13–0.33)*
Positivepredictivevalue 100% CI(0.56–1.0)*
Negativepredictivevalue 14% CI(0.07–0.26)*
Positivelikelihoodratio NC
Negativelikelihoodratio 0.89 CI(0.8–0.96)*
Diagnosticoddsratio NC
IO,intraoperative;MRI,magneticresonanceimaging. ∗ 95%confidenceinterval.
Discussion
Intheliterature,studiesthatassessimagingmethodsforthe diagnosis ofpartial lesions ofthe long head ofthe biceps are rare. Almost all studies evaluatethe accuracyofthese tests only for complete injuries of this tendon. Literature
reviewretrievedonlyfourstudiesthatspecificallyexamined validity ofMRIwithout contrast inthe detectionofpartial damageto the long head ofthe biceps tendonas primary goal.3,7–9
amongstudiesreportinglowersensitivityandhigher speci-ficityofMRIindetectingpathologiesofthelongheadofthe biceps.7 Intheirstudy,Houtzetal.10 observedlow
sensitiv-ity,which rangedfrom 7%to33%,versus specificityvalues rangingfrom 95%to100% inthe31 casesofalterationsof the long head ofthe biceps out of 104 casesevaluated by MRIwithoutcontrast,regardlessoftheradiologists’placeof work(communityvs.academia).Nourissatetal.11addressed
onlytendinopathy inthe intra-articularportionofthelong headofbicepsandreportedasensitivityof43%andalower specificityvalue(75%).Bealletal.,3withasamplesizeof111
patients,reportedsensitivityandspecificityof52%and86%, respectively,fortotalorpartialrupturesofthelongheadofthe biceps,withaprevalenceof21%(23of111).Inpartialruptures ofthelong headofthe biceps,previousstudiesare consis-tentwiththelowsensitivityobservedinthepresentstudy.7,11
Mohtadietal.,1whoexaminedthelongheadofthebicepsin
aprospectivestudyof58patients,observedaprevalenceof partiallesionsof19%,withsensitivityandspecificityof50% and70%,respectively.Dubrowetal.7reportedasensitivityof
28%andspecificityof84%forthedetectionofpartialrupture ofthelongheadofthebiceps.Mohtadietal.1reported
sen-sitivityof0%andaspecificityof94%forfull-thicknessbiceps tendontear.
PartialrupturesremainachallengefordiagnosisbyMRI withoutcontrastduetoseveralreasons.Thelongheadofthe bicepsissubjecttoanMRIartifactthatoccursinthecranial portionoftheintertuberculargroove,whichissurroundedby collagenandappearshyperintense,andthuscanbemistaken forapathologicalchange.12
Theanatomyoftherotatorintervaliscomplex,androtator cufftearsmayhindertheinterpretationofthelongheadofthe bicepsduetofluidthatextendstotheregion.Anotherfactoris thatpositioningthepatientwiththearmininternalrotation increasesthedifficultyofassessingthetendon.
In the present study, the reduced sensitivity values in patientswithrotatorcufftearslargerthan3cmindicatethat themostseriousinjuriesprobablyadddifficulty to diagno-sisofinjuriesofthelongheadofthebiceps.Intheirstudy, Razmajouetal.9foundresultssimilartothoseofthepresent
study,demonstratingthattheseverityoftherotatorcuffinjury decreasesthesensitivityoftheMRItodetectthebicepsinjury. Inthepresentstudy,rotatorcuffinjuriesthatappearedmore severeattheMRIpresentedlowersensitivity;inthesecases, theprevalenceofpartialrupturesofthelongheadofthebiceps presentsitshighestvalue.Therefore,asalsoshowninother studies,theseverityoftherotatorcuffinjury(retraction of thetendon,muscleatrophy,andfatinfiltration)mayresultin underestimationofthebicepsinjuryandcontributetolower sensitivity.13
Someconsiderationsshouldbemadeinrelationshiptothe presentstudy.Asitwasaretrospectivestudy,itpresentsthe inherentshortcomingsofthistypeofstudy.Anotherissueis thefactthatthescanswereinterpretedbyradiologistsfrom the community,who were notnecessarilytrained to inter-pretmusculoskeletalMRIs;nonetheless,somestudies have failed to identifydifferences in MRI interpretation by aca-demicandcommunityradiologists.10Asapositiveaspect,this
study had asignificant sampleof965patients; tothe best
oftheauthors’knowledge,thatisthelargestsampleinthe subject.1–14
Conclusion
MRIwithoutcontrasthaslowsensitivityandhighspecificity forthe detection ofpartiallesions ofthelong head ofthe bicepstendon.Inpartialrotatorcuffinjuries,complete small-and-mediumlesionssmallerthan3cm,andinSLAPlesions, MRIsensitivityisalittlebetter,butstillfarfromoptimal.The highertheseverityoftherotatorcuffinjury,thelowerthe sen-sitivityofMRIforthediagnosisofpartialruptureofthelong headofthebicepstendon.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.MohtadiNG,VelletAD,ClarkML,HollinsheadRM,Sasyniuk TM,FickGH,etal.Aprospective,double-blindcomparisonof magneticresonanceimagingandarthroscopyinthe evaluationofpatientspresentingwithshoulderpain.J ShoulderElbowSurg.2004;13(3):258–65.
2.MurthiAM,VosburghCL,NeviaserTJ.Theincidenceof pathologicchangesofthelongheadofthebicepstendon.J ShoulderElbowSurg.2000;9(5):382–5.
3.BeallDP,WilliamsonEE,LyJQ,AdkinsMC,EmeryRL,JonesTP, etal.Associationofbicepstendontearswithrotatorcuff abnormalities:degreeofcorrelationwithtearsoftheanterior andsuperiorportionsoftherotatorcuff.AmJRoentgenol. 2003;180(3):633–9.
4.CervillaV,SchweitzerME,HoC,MottaA,KerrR,ResnickD. Medialdislocationofthebicepsbrachiitendon:appearance atMRimaging.Radiology.1991;180(2):523–6.
5.ChanTW,DalinkaMK,KneelandJB,ChervrotA.Biceps tendondislocation:evaluationwithMRimaging.Radiology. 1991;179(3):649–52.
6.HalmaJJ,EshuisR,KrebbersYM,WeitsT,deGastA. Interdisciplinaryinter-observeragreementandaccuracyof MRimagingoftheshoulderwitharthroscopiccorrelation. ArchOrthopTraumaSurg.2012;132(3):311–20.
7.DubrowSA,StreitJJ,ShishaniY,RobbinMR,GobezieR. Diagnosticaccuracyindetectingtearsintheproximalbiceps tendonusingstandardnonenhancingshoulderMRI.Open AccessJSportsMed.2014;5:81–7.
8.SpritzerCE,CollinsAJ,CoopermanA,SpeerKP.Assessment ofinstabilityofthelongheadofthebicepstendonbyMRI. SkeletalRadiol.2001;30(4):199–207.
9.RazmjouH,Fournier-GosselinS,ChristakisM,PenningsA, ElMaraghyA,HoltbyR.Accuracyofmagneticresonance imagingindetectingbicepspathologyinpatientswithrotator cuffdisorders:comparisonwitharthroscopy.JShoulder ElbowSurg.2016;25(1):38–44.
10.HoutzCG,SchwartzbergRS,BarryJA,ReussBL,ShoulderPapa L.MRIaccuracyinthecommunitysetting.JShoulderElbow Surg.2011;20(4):537–42.
12.EricksonSJ,CoxIH,HydeJS,CarreraGF,StrandtJA,Estkowski LD.EffectoftendonorientationonMRimagingsignal intensity:amanifestationofthemagicanglephenomenon. Radiology.1991;181(2):389–92.
13.ChenCH,HsuKY,ChenWJ,ShihCH.Incidenceand severityofbicepslongheadtendonlesioninpatientswith
completerotatorcufftears.JTrauma.2005;58(6): 1189–93.