Arq Neuropsiquiat r 2004;62(4):1092-1094
1Psychiat rist ; Coordinat or of t he Cent er f or Alzheimer’s Disease and Relat ed Disorders, Psychiat ry Inst it ut e, Federal Universit y of Rio de Janeiro, Brazil (CDA/IPUB-UFRJ), Associat e Prof essor of St at e Universit y of Rio de Janeiro; 2Neurologist , CDA/IPUB-UFRJ; 3Psychologist , CDA/IPUB-UFRJ; 4Neuroradiologist , Clínica M ult i-imagem e Ressonância, Rio de Janeiro, Brazil; 5Associat e Prof essor of Psychiat ry, Federal Universit y of Pelot as & Cat holic Universit y of Pelot as, Brazil; Clinical Research Physician, Eli Lilly, Brazil; 6Coordenador do Set or de Neurologia do Comport ament o do Inst it ut o de Neurologia Deolindo Cout o da Universidade Federal do Rio de Janeiro.
Received 20 February 2004, received in f inal f orm 2 M ay 2004. Accept ed 14 July 2004.
Dr. Jerson Laks - Avenida N. S. Copacabana 749/802 - 22050-000 Rio de Janeiro RJ - Brazil. Email: jlaks@cent roin.com.br
FUNCTIONAL AND M OTOR RESPONSE TO LOW
DOSE OLANZAPINE IN HUNTINGTON’S DISEASE
Case report
Jerson Laks
1, M arlos Rocha
2, Claudia Capit ão
3, Romeu Côrt es Domingues
4,
Giovanna Ladeia
4, M aurício Lima
5, Eliasz Engelhardt
6ABSTRACT - Previous report s on t he use of olanzapine in Hunt ingt on’s disease (HD) used doses ranging f rom 10-30 mg. We report a case of HD w it h marked delusions and behavioral impairment assessed by t he Unif ied Hunt ingt on’s Disease Rat ing Scale at baseline and f our mont hs lat er t reat ed w it h a low dose of olanzapine. The patient improved in motor, psychiatric and activity of daily living symptoms after four months of t reat ment . The response t o a low dose of olanzapine in HD may be an indicat or of eff icacy in similar cases. Furt her randomized cont rolled t rials can properly assess t hese f indings.
KEY WORDS: Hunt ingt on’s disease, olanzapine, behavioral abnormalit ies, f unct ional capacit y.
Resposta funcional e motora a doses baixas de olanzapina na doença de Huntington: relato de caso
RESUM O - Relat os de casos sobre o uso de olanzapina na doença de Hunt ingt on (DH) usaram doses var-iando de 10-30 mg. Est e é um relat o de caso de DH avaliado pela Unif ied Hunt ingt on Rat ing Scale no iní-cio e quat ro meses depois com uma dose baixa de olanzapina. A pacient e melhorou dos sint omas mot ores, psiquiát ricos e nas at ividades de vida diária após os quat ro meses de t rat ament o. A respost a a baixas dos-es de olanzapina na DH pode ser um indicador de ef icácia em casos similardos-es. M ais dos-est udos cont rolados randomizados podem avaliar apropriadament e esses achados.
PALAVRAS-CHAVE: doença de huntington, olanzapina, transtornos de comportamento, capacidade funcional.
Hunt ingt on’s disease (HD) is a heredodegener-at ive disorder of t he cent ral nervous syst em, t rans-mit t ed as dominant aut osomic inherit ance w it h a 100% penet rance. It is caused by a t hree nucleot ide basis (CAG) repet it ion at t he IT15 gene, w hich re-sides in the short arm of chromosome 41-2. HD is
cha-ract erized by insidious onset of neurological man-if est at ions including choreic movement s, dysar-thria, dysphagia, ideomotor and eyelid apraxia, pos-t ural inspos-t abilipos-t y, dyspos-t onia, dysf uncpos-t ion of eye move-ment s and rarely myoclonus. Incont inence of uri-nary and anal sphinct ers (common in t he t erminal st age of HD), aut onomic dysf unct ion including hy-perhydrosis, and pressure labilit y are ot her signs and sympt oms of t he disease. Seizures may occur
in 3% of adult HD pat ient s. Neuropsychiat ric signs and sympt oms may occur bef ore, during or af t er neurological manif est at ions. They are present in 35 t o 73% , and a w ide range of dist urbances are reported: affective, behavioral, personality changes w hich include depression, bipolar disorder, man-ic episodes, agitation, impulsiveness, aggressiveness. Cognit ive sympt oms are present in all HD pat ient s at some stage of the disease, characterized by a sub-cort ical dement ia prof ile3. The neuroimage show s
Arq Neuropsiquiat r 2004;62(4) 1093
Neurolept ic drugs are t he mainst ay t herapy in HD f or cont rolling mot or and psychiat ric dist urban-ces. Olanzapine is a dopaminergic–serot onergic antagonist, and has been suggested as an alternati-ve t herapy f or HD4-8.
We report a case of HD t reat ed w it h low dose olanzapine regarding it s mot or and f unct ional res-ponse as assessed by t he Unif ied Hunt ingt on´s Di-sease Rat ing Scale (UHDRS)9. The UHDRS is a prot
o-col by w hich pat ient s are evaluat ed on a series of crit eria, each of t hem receiving a score f rom 0 (nor-mal) t o 4 (incapacit at ed). M ot or signs and symp-t oms on UHDRS include chorea and rigidisymp-t y, balan-ce, eye movement , and abilit y t o w alk; t he beha-vioral section of the scale includes frequency and se-verit y of depression, irrit abilit y, and disrupt ive/ ina-ppropriate behavior; whereas functional UHDRS in-cludes t he abilit y t o perf orm act ivit ies of daily living such as preparing a meal, w alking around f amiliar places, or moving f rom one chair t o anot her.
The f amily and t he pat ient signed an inf ormed consent t o permit t his case report .
CASE
A f ort y-nine year-old Caucasian f emale st art ed t o have obsessive w orries about dirt and compulsive clean-ing in her house t w o years ago. Hypersexualit y and per-secut ory delusions (st range people in her house) devel-oped six mont hs lat er. At t his t ime, t he f amily not iced t he emergence of involunt ary movement s aff ect ing t he f ace and t he ext remit ies t hat quickly became generali-zed, w it h int erf erence in t he act ivit ies of t he daily liv-ing. The pat ient ´s f at her and t hree brot hers present ed choreic movement s as t he f irst clinical f eat ure, w it h bet -t er preserva-t ion of cogni-t ion.
Neurologic examination, laborat ory test ing and mag-net ic resonance imaging of t he brain (M RI) w ere perf or-med init ially. The UHDRS w as perf oror-med at baseline
and repeat ed f our mont hs lat er. The neurologic exam-inat ion show ed f ace and limb choreif orm movement s more apparent w hen w alking, mot or impersist ence signs, slow and dysmet ric saccades and choreif orm gait . The laborat ory t est ing (complet e blood count w it h blood smear, elect rolyt es, liver and t hyroid f unct ion pro-f ile, lipid propro-f ile, sediment at ion rat e, glucose, syphilis se-rology) w as normal. M RI show ed bilat eral caudat e at ro-phy and w idening of cort ical sulci.
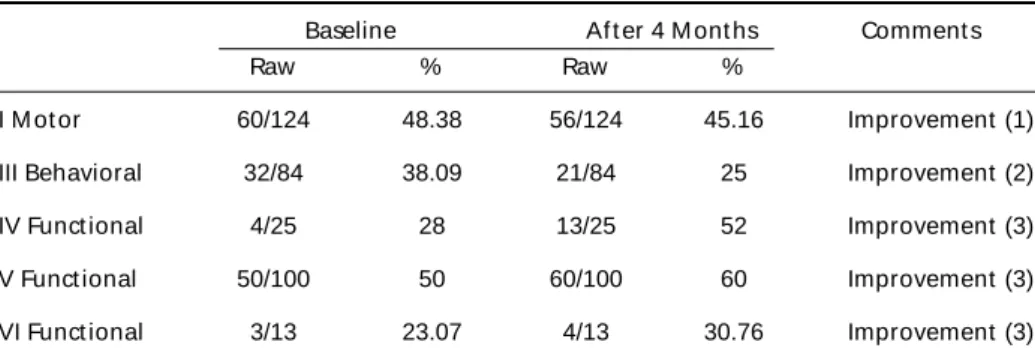
Olanzapine 2.5 mg/day w as prescribed and main-t ained f or 4 consecumain-t ive monmain-t hs. The UHDRS scores be-f ore and 4 mont hs abe-f t er prescript ion obe-f olanzapine are show n in Table 1.
The pat ient developed slight (+/4+) bilat eral ankle edema at t he second mont h t hat remained st able unt il t he f ourt h mont h. No ot her side ef f ect s w ere observed.
DISCUSSION
There are eight report s4-11describing t he use of
olanzapine in HD, and only t hree report s using t he UHDRS for assessment5-7,10. Also, the studies and case
report s published so f ar have dealt w it h eit her t he mot or, f unct ional or behavioral sympt oms4,5,7,8,11.
They have all show n improvement in mot or and behavioral UHDRS subscales w it h high doses of olanzapine and good long t erm t olerabilit y5,6, 8.
There are t w o report s using olanzapine in com-binat ion w it h a second drug. Dipple4used
olanza-pine (5 mg/d) and lof epramide (140 mg/d) during six mont hs, w it h improvement document ed on Quant if ied Neurological Exam12. Grove et al.11 used
olanzapine (5 mg/day) and valproic acid (1500 mg/ day) in t w o HD pat ient s, w it h improvement of t he psychiat ric manif est at ions.
In Brazil, Et chebehere et al.13described one HD
pat ient w hose brain SPECT imaging w as perf ormed bef ore and af t er f ive days of olanzapine (10 mg/d).
Table 1. UHDRS score bef ore and af t er olanzapine.
Baseline Af t er 4 M ont hs Comment s
Raw % Raw %
I M ot or 60/124 48.38 56/124 45.16 Improvement (1)
III Behavioral 32/84 38.09 21/84 25 Improvement (2)
IV Funct ional 4/25 28 13/25 52 Improvement (3)
V Funct ional 50/100 50 60/100 60 Improvement (3)
VI Funct ional 3/13 23.07 4/13 30.76 Improvement (3)
1094 Arq Neuropsiquiat r 2004;62(4)
improvement s in t his case report , t hese dif f eren-ces f rom baseline t o endpoint assessment s (af t er 4 mont hs) did not reach convent ional level of st a-t isa-t ical signif icance. How ever, a-t he response show n t o a low dose olanzapine t reat ment in HD may be considered an indicat or of possible eff icacy of olan-zapine in HD; f urt her st udies (randomized cont ro-lled t rials) can properly assess t hese f indings.
REFERENCES
1. Gusella JF, Wexler NS, Connealy PM, et al. A polymorphic DNA mark-er genetically linked to Huntington’s disease. Nature 1983;306:234. 2. Gilliam TC, Tanzi RE, Haines JL, et al. Localization of the Huntington’s
disease gene to a small segment of chromosome 4 flanked by D4S10 and the telomere. Cell 1987;50:565.
3. Cummings JL. Subcortical dementia. New York / Oxford, Oxford Univ Press, 1990.
4. Dipple HC. The use of olanzapine for movement disorder in Huntington’s disease: a first case report. J Neurol Neurosurg Psychiatry 1999;67:123-124. 5. Squitieri F, Cannella M, Piorcellini A, et al. Short-term effects of olan-zapine in Huntington’s disease. Neuropsychiatry Neuropsychol Behav Neurol 2001;14:69-72.
6. Bonelli RM, Niederwieser G, Tribl GG, et al. High-dose olanzapine in Huntington’s disease. Int Clin Psychopharmacol 2002;17:91-93. 7. Paleacu D, Anca M, Giladi N. Olanzapine in Huntington’s disease.
Acta Neurol Scand 2002;105:441-444.
8. Jiménez-Jiménez FJ, Toledo M, Puertas I, et al. La olanzapina mejora el corea en pacientes con enfermedad de Huntington. Rev Neurol 2002;35:524-525.
9. Huntington Study Group. Unified Huntington’s disease Rating Scale: reliability and consistency. Mov Disord 1996;11:136-142.
10. Bonelli RM, Mahnert FA, Niederwieser G. Olanzapine for Huntington disease: an open label study. Clin Neuropharmachol 2002;25:263-265. 11. Grove VE Jr, Quintanilla J, DeVaney GT. Improvement of Huntington’s disease with olanzapine and valproate. N Engl J Med 2000;343:973-974. 12. Folstein SE, Jensen B, Leigh RJ, et al. The measurement of abnormal movement: methods developed for Huntington’s disease. Neurobehav Toxicol Teratol 1983;5:605-609.
13. Etchebehere EC, Lima MC, Passos W, et al. Brain SPECT imaging in Huntington’s disease before and after therapy with olanzapine: case report. Arq Neuropsiquiatr 1999;57:863-866.
No assessment of clinical response w as described. We t reat ed our pat ient w it h 2.5 mg/d of olanza-pine, w hile in ot her st udies t he dose ranged f rom 5 mg/d t o 30 mg/d.
We evaluat ed t hree clust ers of t he disease as assessed by t he UHDRS.This report show s t he im-provement of mot or, f unct ional and behavioral sympt oms t o a low dose of olanzapine.
Our patient was treated for 4 consecutive months w hereas t he ot her report s describe a range f rom t w o w eeks t o 36 mont hs of medicat ion. She impro-ved in t he mot or scale f or t ongue prot rusion, f in-ger t aps, Luria’s sequence, and gait . The act ivit ies of daily living w ere resumed. She st art ed t o t ake t he medicat ion on her ow n, dress, bat he, and use t he t oilet w it hout help. The behavioral subscale show ed a marked improvement , w it h t he cont rol of obsessions, compulsions, and delusions. Bilat eral ankle edema w as observed at t he f ourt h mont h, as t he only adverse ef f ect .
Three st udies/case report s t hat used t he UHDRS had higher severit y scores on mot or and behavioral scales at baseline w hen compared t o our pat i-ent5,6,10. Anot her report7show ed less severit y scores
t han ours on mot or and behavioral scales but also used olanzapine in higher dose (10 mg). On the oth-er hand, only one case report6used all t he subscales
of t he UHDRS as in our case, alt hough t heir pat ient had no psychiatric symptoms. The other studies
ver-if ied only mot or subscale10 or mot or and
behav-ioral subscales5, 7.