ABSTRACT
Long- t erm effect s of vert ical bone augm ent at ion:
a syst em at ic review
Johan Anton Jochum KEESTRA
1,2, Obada BARRY
3, Lianne DE JONG
4*HUKDUG:$+/
31- Ordentall, Rotterdam, Netherlands.
2- Praktijk voor Parodontologie en Implantologie, Tilburg, Netherlands.
3- Universität Bonn, Poliklinik für Chirurgische Zahn-, Mund- und Kieferheilkunde, Bonn, Germany. 4- Dental Clinics Zuiderterras, Rotterdam, Netherlands.
&RUUHVSRQGLQJDGGUHVV Gerhard Wahl - Department of Oral Surgery, University of Bonn, Welschnonnenstraße 17, 53117 - Bonn, Germany - Fax: +49 228 287 22653 - e-mail: [email protected]
6XEPLWWHG$XJXVW0RGL¿FDWLRQ2FWREHU$FFHSWHG2FWREHU
E
xt ract ion, periodont it is, or t raum a can cause a reduct ion on t he alveolar ridge. This
FRXOGUHVXOWLQDQLQVXI¿FLHQWDOYHRODUERQHZLGWKDQGKHLJKW'LIIHUHQWWHFKQLTXHVRI
vert ical bone augm ent at ion are described in lit erat ure. However, nowadays t here is not
enough evidence against lat eral augm ent at ion procedures t o verify if t hese t echniques are
st able over a long period of t im e. Obj ect ive: This review analyses t he different t echniques
t hat are used t o vert ically augm ent t he bone and evaluat e if t hese t echniques are st able
over a long period of t im e. Mat erial and Met hods: The MEDLI NE- PubMed dat abase was
searched from it s earliest records unt il Decem ber 22, 2014. The following search t erm was
used: Alveolar Ridge augm ent at ion [ MESH] . Several j ournals were hand searched and som e
aut hors were cont act ed for addit ional inform at ion. The prim ary out com e m easure t hat was
analyzed was m arginal bone level change around dent al im plant s in t he augm ent ed sit es,
and t he secondary out com es were survival and success rat es of dent al im plant s placed
in t he augm ent ed sit es. Result s: The search yielded 203 abst ract s. Ult im at ely, 90 art icles
were select ed, describing 51 st udies m eet ing t he eligibilit y crit eria. The m arginal bone level
change for t he inlay t echnique and vert ical guided bone regenerat ion are in agreem ent
wit h t he success crit eria. Alveolar dist ract ion showed m ore m arginal bone level change
DIWHUWKH¿UVW\HDURIORDGLQJDQGIRUWKHLQOD\WHFKQLTXHYHU\IHZVWXGLHVZHUHDYDLODEOH
Conclusions: Based on t he available dat a in t he current exist ing st udies wit h a follow- up
period of at least 4 t o 5 years, one can sum m arize t hat t here seem s t o be a t rend t hat t he
onlay t echnique, alveolar dist ract ion, and vert ical guided bone regenerat ion are st able for
at least 4 t o 5 years.
Ke yw or ds:
Alveolar ridge augm ent at ion. Dent al im plant s. At rophy. Alveolar bone loss.
Bone subst it ut es.
I N TROD UCTI ON
Sin ce Br ån em ar k in t r od u ced a n ew d en t al
t r eat m ent , a m achined t it anium im plant , a new
t r eat m ent opt ion becam e available
3. I f t her e is
su f f icien t b on e q u an t it y an d q u alit y, a d en t al
im plant could be a predict able t reat m ent opt ion.
I n lit erat ur e, a sur v ival rat e ov er 95% in
non-com pr om ised pat ien t s is r epor t ed
3 2. Th er efor e,
dent al im plant s have becom e a reliable t reat m ent
opt ion for pat ient s m issing one or m ult iple t eet h.
However, unfavourable condit ions of t he alveolar
bone due t o periodont it is, ext ract ion, or t raum a
provoke decrease in t he alveolar ridge due t o bone
at rophy. Such bone at rophy could cause challenging
int erarch relat ionship in vert ical, t ransverse, and
sagit t al planes, which m ay cause incorrect dent al
im plant placem ent from a funct ional and aest het ic
point of view
19.
To provide adequat e bone volum e and t o assure
an adequat e aest het ic result , bone augm ent at ion
p r oced u r es ar e so m et i m es a p r er eq u i si t e f or
successful dent al im plant t r eat m ent . Ther e ar e
different t echniques t o augm ent t he bone, such as:
widt h of t he alveolar bone. The graft is im m obilised
wit h dent al im plant s, screws, or plat es
52.
2. I nlay graft ing. A part of t he alveolar ridge is
surgically separat ed and a graft m at erial is placed
bet ween t he t wo sect ions
52.
3. Ridge expansion. A part of t he alveolar ridge
is longit udinally split t o widen t he ridge and allow
placem ent of a graft , an oral im plant , or bot h
35.
4. Dist ract ion ost eogenesis. A gradual, cont rolled
displacem ent of a surgically prepared fract ure. The
t wo bone fragm ent s are slowly pulled apart , and
new bone will arise in t he gap
26.
5. Guided bone regenerat ion ( GBR) . A space is
m aint ained by a barrier m em brane, which will be
¿OOHGZLWKQHZERQH
67.
Different m aterials can be used for augm entation:
1. Aut ogenous bone graft . This bone graft is
t aken fr om t he sam e pat ient in an adj acent or
rem ot e sit e. This m at erial is considered t o be t he
“ gold st andard”, while it is biologically com pat ible
and provides a scaffold for new bone form at ion
77.
2. Allograft . This bone graft is harvest ed from
hum an cadavers and processed by m et hods such
as freezing or dem ineralising and freezing
67.
3. Xenograft . This is a graft m at erial derived
from anim als, usually bovine bone. I t is processed
t o com plet ely rem ove t he organic com ponent
13.
4. Alloplast ic graft . This bone graft is a synt het ic
bon e su bst it u t e m ade u p of bioact iv e glass or
calcium phosphat es
112.
5 . Ost e o i n d u ct i v e m a t e r i a l . Th i s m a t e r i a l
st im ulat es t he ost eoprogenit or cells t o different iat e
int o ost eoblast s and accelerat e new bone form at ion.
The m ost com m on are bone m orphogenet ic prot eins
( BMPs) , plat elet rich plasm a ( PRP) , and leukocyt e
SODWHOHWULFK¿EULQ/35)
33.
Each t y pe of augm ent at ion m at er ial m ay be
used com bined wit h a variet y of different surgical
t echniques.
The rat ionale for t he use of a v er t ical bone
augm ent at ion is t o im prove t he vert ical dim ension of
t he bone. I f t he use of a vert ical bone augm ent at ion
t echnique is needed, t he clinician needs t o decide
which t echnique and which m at erial should be used
t o vert ically augm ent t he bone. When t he vert ical
bone augm ent at ion is successful, one can proceed
for dent al im plant placem ent . The aim of t his review
is t o analyze t he success, survival rat es of dent al
im plan t s, an d t h e m ar gin al bon e lev el ch an ge
around dent al im plant s placed in t he augm ent ed
ar ea. Mar ginal bone level change is m ost oft en
cont rolled t hrough x- rays in t he m aint enance phase
t o dem onst rat e and secure im plant success.
M ATERI AL AN D M ETH OD S
Th e f ollow in g an aly sis w as p er f or m ed in a
differ ent way accor ding t o t he guidelines of t he
Cochrane Collaborat ion and t he principles of t he
PRI SMA ( Preferred Report ing I t em s for Syst em ic
Rev iew s an d Met a- An aly ses) st at em en t f or a
syst em at ic review
46,69.
Focu se d qu e st ion ( PI CO)
We f ocu sed on t h e f ollow in g qu est ion : “ Do
v er t ical b on e au g m en t at ion h av e a lon g - t er m
predict able st abilit y?”.
Se a r ch st r a t e gy
The MEDLI NE- PubMed dat abase was searched
from it s earliest records unt il Decem ber 22, 2014.
Th e f ollow in g sear ch t er m w as u sed: Alv eolar
Ridge augm ent at ion [ MESH] . I n addit ion, a m anual
search was carried out concerning issues from t he
past 10 year s of t he follow ing j our nals: Clinical
I m plant Dent ist ry and Relat ed Research, Clinical
Oral I m plant s Research, European Journal of Oral
I m p lan t olog y, I m p lan t Den t ist r y, I n t er n at ion al
Jo u r n a l o f Or a l a n d Ma x i l l o f a ci a l I m p l a n t s,
I n t er n at ion al Jou r n al of Or al an d Max illof acial
Surgery, Journal of Oral I m plant ology, Journal of
Oral and Maxillofacial Surgery, Journal of Clinical
Per iodont ology, Jour nal of Per iodont al Resear ch,
and t he Journal of Periodont ology.
St u dy in clu sion a n d e x clu sion cr it e r ia
The select ion pr ocess was per for m ed by t w o
m asked reviewers ( OB and JK) . The st udies were
an aly zed accor d in g t o t h e f ollow in g in clu sion
crit eria:
1. All st udies in which at least 10 pat ient s were
t reat ed and had a follow- up of at least 12 m ont hs.
2 . Pat ien t s p r esen t in g d ef icien t ed en t u lou s
ridges caused by at rophy, periodont al disease, and
t raum a were considered.
3 . Th e f ollow in g su r g ical p r oced u r es w er e
consider ed: onlay bone graft s, split - r idge/ r idge
ex pan sion t ech n iqu es/ in lay t ech n iqu e ( v er t ical
direct ion) , alveolar dist ract ion ost eogenesis, and
guided bone regenerat ion procedures.
4 . Ar t icles r elat ed t o d en t al im p lan t s w er e
considered for inclusion.
5 . No sp eci f i c d en t al i m p l an t sy st em w as
excluded.
6 . No sp eci f i c au g m en t at i o n m at er i al w as
excluded.
7. Only st udies in t he English language were
included.
The following exclusion crit eria were used:
1 . Pa t i e n t s w i t h b o n e d e f e ct s ca u se d b y
congenit al m alform at ions, aft er ablat ion of t um ors,
or ost eoradionecrosis.
2 . Th e f ollow in g su r g ical p r oced u r es w er e
e x cl u d e d : si n u s f l o o r e l e v a t i o n b y a l a t e r a l
approach, Le Fort I ost eot om y wit h int erposit ional
t ech n iqu es, an d cor r ect ion of deh iscen ces an d
fenest rat ions.
3. Duplicat ed st udies.
Ou t com e va r ia ble s
The prim ary out com e was: m arginal bone level
change around dent al im plant s in t he augm ent ed
sit es. The following recall m om ent s were not ed:
b aselin e ( p lacem en t of t h e f in al cr ow n , st ar t
loading) , year 1, 2, 3, 4, and 5 of loading. The
secondar y out com es w er e sur v ival and success
rat es of dent al im plant s placed in t he augm ent ed
sit es. I m plant survival was evaluat ed using Sim onis,
et al.
97( 2010) , being im plant rem oval t he survival
cr it er ion. I m plant success w as evaluat ed using
Albrekt sson, et al.
5( 2012) , and t he success crit eria
w er e absence of per sist ent pain or dysest hesia,
absence of peri- im plant infect ion wit h suppurat ion,
absence of m obilit y, absence of cont inuous
im plant radiolucency, less t han 1.5 m m of
peri-LPSODQW ERQH UHVRUSWLRQ GXULQJ WKH ¿UVW \HDU RI
funct ion, and less t han 0.2 m m in subsequent years.
D a t a e x t r a ct ion
The t it le and abst ract of st udies wit h pot ent ial
r el ev a n ce f o r t h e r ev i ew w er e o b t a i n ed a n d
screened independent ly by t wo m asked reviewers
( OB and JK) . St udies w it hout abst ract , but w it h
a t it le suggest ing relevance t o t he subj ect of t he
review, were select ed for full t ext screening. The
select ed full- t ext art icles were independent ly read
in det ail t o verify whet her t hey passed t he inclusion/
exclusion crit eria. The references of t he full t ext
art icles were screened for any relevant addit ional
DUWLFOHV6WXGLHVWKDWIXO¿OOHGDOOWKHVHOHFWLRQFULWHULD
were processed for dat a ext ract ion. Discrepancies
r egar din g t h e in clu sion or ex clu sion of st u dies
were resolved by discussion bet ween t he reviewers
( OB and JK) . The ext ract ed dat a included: year of
publicat ion, design of t he st udy, num ber of pat ient s
per
st udy ar m , defect t y pe, sur gical pr ocedur e,
donor sit e, num ber of dent al im plant s, t im ing of
im plant s, follow- up t im e, prim ary out com e m easure
DW EDVHOLQH SODFHPHQW RI WKH ¿QDO FURZQ VWDUW
loading) , year 1, 2, 3, 4, and 5 of loading, and
secondary out com es m easures. The qualit y of t he
YDULRXV VWXGLHV ZHUH QRW FRQVLGHUHG LQ WKH ¿QDO
an aly sis, t h er efor e, n o qu alit y assessm en t h as
been done.
St a t ist ica l a n a lyse s
Dat a of t he included st udies were ext ract ed and
insert ed int o a dat abase. Mean values and st andard
dev iat ions w er e ex t ract ed fr om t he dat a. I f no
st andard deviat ion was available, it was recalculat ed
E\WKHIRUPXOD6( 6'¥QZKHUHn
is t he sam ple
size. When m ean follow- up period was used, it was
recalculat ed, if possible, for every year; if not , t he
QHDUHVWIXOO\HDUZDVXVHG,IWKHUHZHUHLQVXI¿FLHQW
dat a available, t he cor r esponding aut hor s w er e
cont act ed for addit ional dat a. The available dat a
were recalculat ed in order t o present t he dat a like
m arginal bone level change at baseline ( placem ent
RIWKH¿QDOFURZQVWDUWORDGLQJ\HDU
and 5 of loading, and t he lat est available dat a for
survival and success rat es were not ed. The dat a
of t his review was st at ist ically analyzed using t he
program SPSS 21.0 ( I BM Corp. Released 2012. I BM
SPSS St at ist ics for Windows, Version 21.0. Arm onk,
NY: I BM Corp.) .
RESULTS
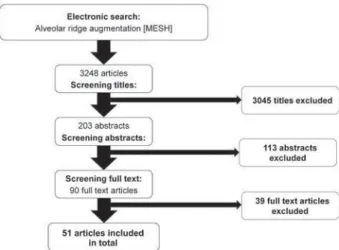
The init ial sear ch r esult ed in a t ot al of 3248
ar t icles ( Fig u r e 1 ) . Af t er scr een in g t h e t it les,
203 abst ract s were included for furt her analysis.
Analysis of t he abst ract s result ed in 90 pot ent ial
art icles. I n t he t hird phase, t he full- t ext art icles of
t he rem aining 90 art icles were evaluat ed, of which
39 art icles
2,8,9,12,14,18,23,24,27,28,30,39,41,44,45,48,49,51,56,59,60,62, 6 4 , 6 8 , 7 3 , 7 5 , 8 4 , 8 9 , 9 0 , 9 2 - 9 4 , 9 8 , 1 0 2 , 1 0 3 , 1 0 7 , 1 0 8 , 1 1 1 , 1 1 3did n ot pass
t he inclusion cr it er ia ( Figur e 2) . A scr eening of
t he reference list s of t he full t ext art icles did not
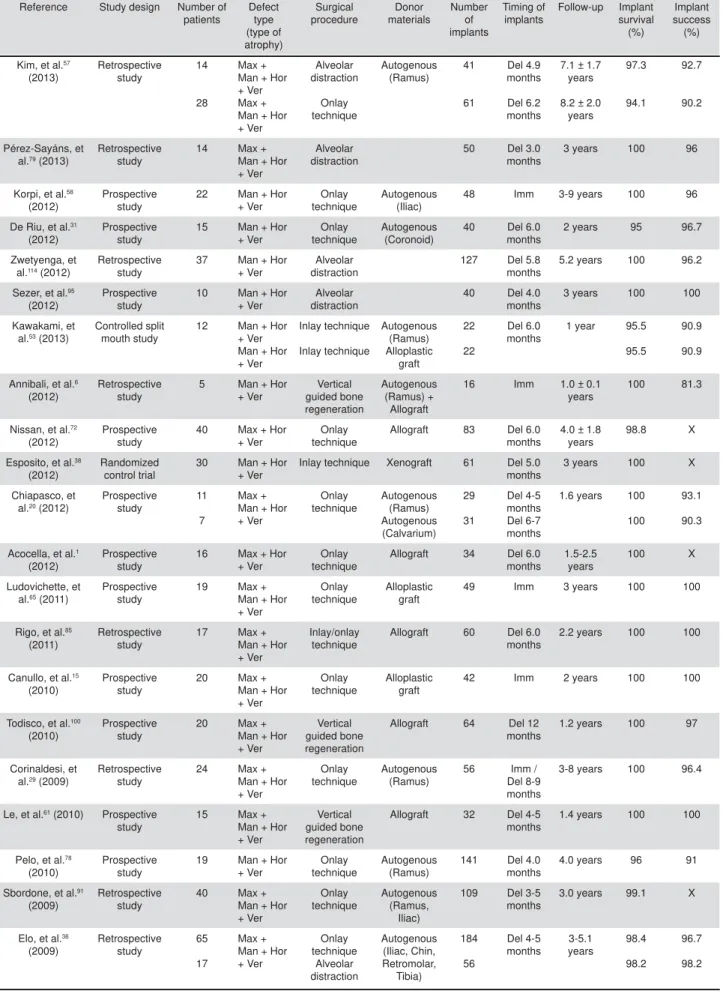
r esult in any addit ional ar t icles. I n Table 1, t he
m ain charact erist ics of t he 51 included st udies are
su m m ar ized
1 , 6 , 7 , 1 0 , 1 5 , 1 6 , 2 0 - 2 2 , 2 5 , 2 9 , 3 1 , 3 4 , 3 6 - 3 8 , 4 0 , 4 2 , 4 3 , 5 0 , 5 3 , 5 5 , 57,58,61,63,65,66,70- 72,74,78- 86,91,95,96,99,100,104- 106,109,110,114. Only
t he t reat m ent groups of int erest are represent ed.
For v er t ical bon e au gm en t at ion , f ou r dif f er en t
t ech n iq u es w er e u sed an d t h e r esu lt s w ill b e
present ed separat ely. I n Table 2, t he charact erist ics
of t he different vert ical augm ent at ion t echniques
are present ed.
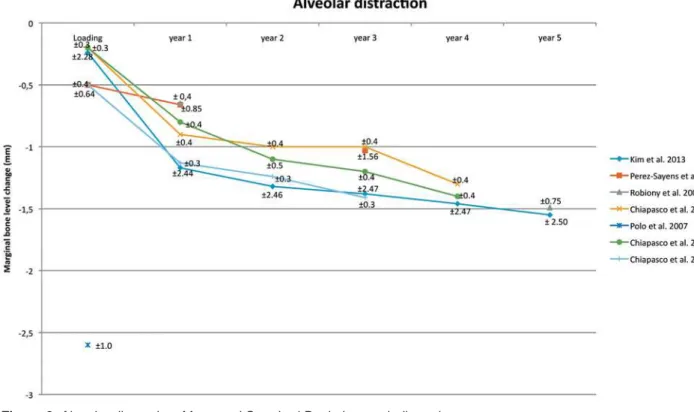
Alve ola r dist r a ct ion ( Ta ble 1 , Figu r e 3 )
T h e 5 1 i n c l u d e d a r t i c l e s p r o v i d e d 1 7
st udies
10,21,22,25,36,37,40,43,50,57,79,81- 83,95,104,114wit h alveolar
dist ract ion, and one st udy
86used a com binat ion
of t he inlay t echnique and alv eolar dist ract ion.
Eight st udies w er e r et r ospect ive w hile 10 w er e
prospect ive. A t ot al of 333 pat ient s wit h a vert ical
resorpt ion of part ially or t ot ally edent ulous alveolar
ridges were t reat ed wit h int raoral int raosseous or
ext raosseous devices. Twelve pat ient s were t reat ed
wit h a com binat ion of inlay t echnique and vert ical
dist ract ion. I n t ot al, 1011 dent al im plant s w er e
placed aft er 3 t o 6 m ont hs, and t he m ean was 3.8
m ont hs aft er t he com plet ion of t he dist ract ion. Aft er
t he st art of loading, t he follow- up ranged from 1 t o
7.1 years and t he m ean was 2.9 years. The survival
rat es for t he dent al im plant s in alveolar dist ract ed
bone ranged from 88 t o 100% and t he m ean was
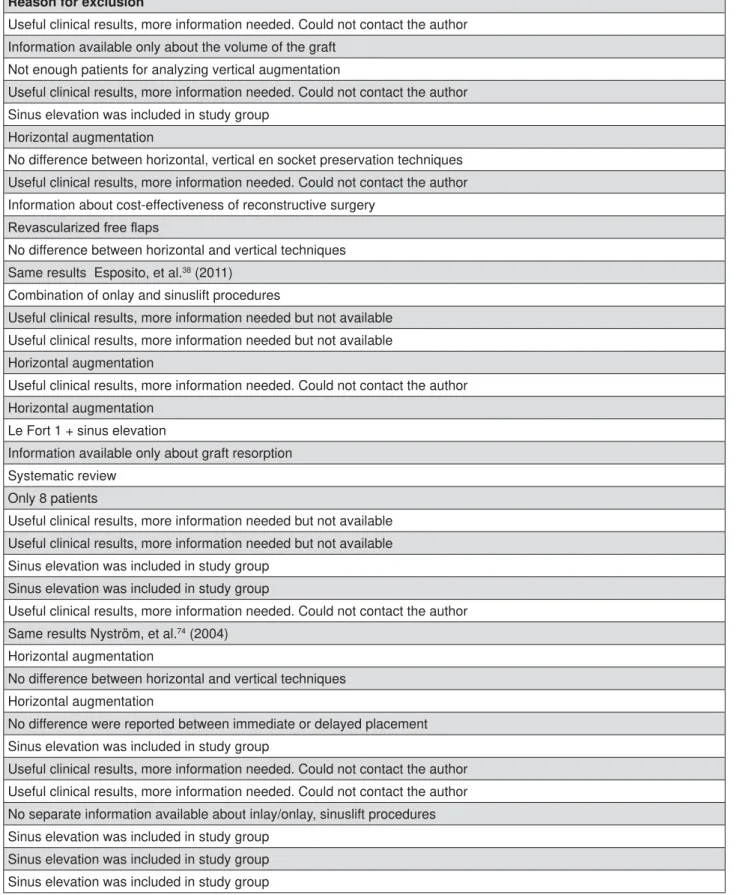
Reason for exclusion
Useful clinical results, more information needed. Could not contact the author
Information available only about the volume of the graft
Not enough patients for analyzing vertical augmentation
Useful clinical results, more information needed. Could not contact the author
Sinus elevation was included in study group
Horizontal augmentation
No difference between horizontal, vertical en socket preservation techniques
Useful clinical results, more information needed. Could not contact the author
Information about cost-effectiveness of reconstructive surgery
5HYDVFXODUL]HGIUHHÀDSV
No difference between horizontal and vertical techniques
Same results Esposito, et al.
38(2011)
Combination of onlay and sinuslift procedures
Useful clinical results, more information needed but not available
Useful clinical results, more information needed but not available
Horizontal augmentation
Useful clinical results, more information needed. Could not contact the author
Horizontal augmentation
Le Fort 1 + sinus elevation
Information available only about graft resorption
Systematic review
Only 8 patients
Useful clinical results, more information needed but not available
Useful clinical results, more information needed but not available
Sinus elevation was included in study group
Sinus elevation was included in study group
Useful clinical results, more information needed. Could not contact the author
Same results Nyström, et al.
74(2004)
Horizontal augmentation
No difference between horizontal and vertical techniques
Horizontal augmentation
No difference were reported between immediate or delayed placement
Sinus elevation was included in study group
Useful clinical results, more information needed. Could not contact the author
Useful clinical results, more information needed. Could not contact the author
No separate information available about inlay/onlay, sinuslift procedures
Sinus elevation was included in study group
Sinus elevation was included in study group
Sinus elevation was included in study group
Reference Study design Number of patients Defect type (type of atrophy) Surgical procedure Donor materials Number of implants Timing of implants Follow-up Implant survival (%) Implant success (%)
Kim, et al.57 (2013) Retrospective study 14 28 Max + Man + Hor + Ver Max + Man + Hor + Ver Alveolar distraction Onlay technique Autogenous (Ramus) 41 61 Del 4.9 months Del 6.2 months
7.1 ± 1.7 years
8.2 ± 2.0 years 97.3 94.1 92.7 90.2 Pérez-Sayáns, et al.79 (2013)
Retrospective study
14 Max + Man + Hor + Ver
Alveolar distraction
50 Del 3.0 months
3 years 100 96
Korpi, et al.58 (2012)
Prospective study
22 Man + Hor + Ver
Onlay technique
Autogenous (Iliac)
48 Imm 3-9 years 100 96
De Riu, et al.31 (2012)
Prospective study
15 Man + Hor + Ver
Onlay technique
Autogenous (Coronoid)
40 Del 6.0 months
2 years 95 96.7
Zwetyenga, et al.114 (2012)
Retrospective study
37 Man + Hor + Ver
Alveolar distraction
127 Del 5.8 months
5.2 years 100 96.2
Sezer, et al.95 (2012)
Prospective study
10 Man + Hor + Ver
Alveolar distraction
40 Del 4.0 months
3 years 100 100
Kawakami, et al.53 (2013)
Controlled split mouth study
12 Man + Hor + Ver Man + Hor + Ver Inlay technique Inlay technique Autogenous (Ramus) Alloplastic graft 22 22 Del 6.0 months
1 year 95.5
95.5
90.9
90.9
Annibali, et al.6 (2012)
Retrospective study
5 Man + Hor + Ver Vertical guided bone regeneration Autogenous (Ramus) + Allograft
16 Imm 1.0 ± 0.1 years
100 81.3
Nissan, et al.72 (2012)
Prospective study
40 Max + Hor + Ver
Onlay technique
Allograft 83 Del 6.0 months
4.0 ± 1.8 years
98.8 X
Esposito, et al.38 (2012)
Randomized control trial
30 Man + Hor + Ver
Inlay technique Xenograft 61 Del 5.0 months
3 years 100 X
Chiapasco, et al.20 (2012)
Prospective study
11
7
Max + Man + Hor + Ver Onlay technique Autogenous (Ramus) Autogenous (Calvarium) 29 31 Del 4-5 months Del 6-7 months
1.6 years 100
100
93.1
90.3
Acocella, et al.1 (2012)
Prospective study
16 Max + Hor + Ver
Onlay technique
Allograft 34 Del 6.0 months
1.5-2.5 years
100 X
Ludovichette, et al.65 (2011)
Prospective study
19 Max + Man + Hor + Ver
Onlay technique
Alloplastic graft
49 Imm 3 years 100 100
Rigo, et al.85 (2011)
Retrospective study
17 Max + Man + Hor + Ver
Inlay/onlay technique
Allograft 60 Del 6.0 months
2.2 years 100 100
Canullo, et al.15 (2010)
Prospective study
20 Max + Man + Hor + Ver
Onlay technique
Alloplastic graft
42 Imm 2 years 100 100
Todisco, et al.100 (2010)
Prospective study
20 Max + Man + Hor + Ver
Vertical guided bone regeneration
Allograft 64 Del 12 months
1.2 years 100 97
Corinaldesi, et al.29 (2009)
Retrospective study
24 Max + Man + Hor + Ver
Onlay technique
Autogenous (Ramus)
56 Imm / Del 8-9 months
3-8 years 100 96.4
Le, et al.61 (2010) Prospective study
15 Max + Man + Hor + Ver
Vertical guided bone regeneration
Allograft 32 Del 4-5 months
1.4 years 100 100
Pelo, et al.78 (2010)
Prospective study
19 Man + Hor + Ver
Onlay technique
Autogenous (Ramus)
141 Del 4.0 months
4.0 years 96 91
Sbordone, et al.91 (2009)
Retrospective study
40 Max + Man + Hor + Ver Onlay technique Autogenous (Ramus, Iliac)
109 Del 3-5 months
3.0 years 99.1 X
Elo, et al.36 (2009) Retrospective study 65 17 Max + Man + Hor + Ver Onlay technique Alveolar distraction Autogenous (Iliac, Chin, Retromolar, Tibia) 184 56 Del 4-5 months 3-5.1 years 98.4 98.2 96.7 98.2
Table 1-
Characteristics of the 51 studies included
Reference Study design Number of patients Defect type (type of atrophy) Surgical procedure Donor materials Number of implants Timing of implants Follow-up Implant survival (%) Implant success (%)
Ettl, et al.40 (2010)
Retrospective study
30 Max + Man + Hor + Ver
Alveolar distraction
82 Del 4.5 months
4.2 years 95.1 X
Nissan, et al.71 (2011)
Prospective study
31 Max + Hor + Ver
Onlay technique
Allograft 63 Del 6.0 months
2.8 ± 1.3 years
98.1 X
Felice, et al.42 (2009)
Prospective study
10 10
Man + Hor + Ver Inlay technique Onlay technique Autogenous (Iliac) 20 23 Del 3-4 months
1.5 years 100 100
90 86.9
Nissan, et al.70 (2011)
Prospective study
21 Man + Hor + Ver
Onlay technique
Allograft 85 Del 6.0 months
3.1 ± 1.4 years
95.1 X
Urban, et al.105 (2009)
Retrospective study
28 Max + Man + Hor + Ver Vertical guided bone regeneration Autogenous (Ramus, Chin)
54 Del 6-9 months
2.8 years 100 94.7
Carinci, et al.16 (2009)
Retrospective study
21 Man + Hor + Ver
Onlay technique
Allograft 63 Del 6.0 months
1.7 years 96.8 X
Robiony, et al.86 (2008)
Prospective study
12 Man + Hor + Ver Alveolar distraction + Inlay technique Autogenous (Iliac)
47 Del 6.0 months
5 years 97.9 91.5
Pieri, et al.80 (2008)
Prospective study
16 Max + Man + Hor + Ver Vertical guided bone regeneration Autogenous (Ramus) +Xenograft
44 Del 8-9 months
2 years 100 93.1
Bianchi, et al.10 (2008)
Prospective study
5
6
Man + Hor + Ver Inlay technique Alveolar distraction Autogenous (Iliac) 21 16 Del 3-4 months Del 4-5 months 1.8 years 2.5 years 100 100 95.2 93.7 Chiapasco, et al.25 (2007)
Prospective study
8
9
Man + Hor + Ver Onlay technique Alveolar distraction Autogenous (Ramus) 19 21 Del 4-5 months Del 3 months
2-4 years 100
100
89.5
94.7
Uckan, et al.104 (2007)
Retrospective study
21 Max + Man + Hor + Ver
Alveolar distraction
42 Del 3-4 month
2.7 years 88 X
Polo, et al.81 (2007)
Prospective study
10 Man + Hor + Ver
Alveolar distraction
34 Del 3-4 months
1.0 ± 0.3 years
100 X
Levin, et al.63 (2007)
Retrospective study
50 Max + Man + Hor + Ver Onlay technique Autogenous (Ramus, Iliac)
129 Del 4-6 months
2.0 ± 0.9 years
96.9 91.9
Smolka, et al.99 (2006)
Prospective study
10 Man + Hor + Ver
Onlay technique
Autogenous (Calvarium)
20 Del 6.0 months
2.5 years 95 X
Enislidis, et al.37 (2005)
Retrospective study
32 Man + Hor + Ver
Alveolar distraction
94 Del 3-5 months
3.0 years 95.7 X
van der Meij, et al.106 (2005)
Retrospective study
17 Man + Hor + Ver
Onlay technique
Autogenous (Calvarium)
34 Imm 4.3 years 88.2 88.2
Nyström, et al.74 (2004)
Retrospective study
30 Max + Hor + Ver
Onlay technique
Autogenous (Iliac)
177 Imm 10 years 72,8 X
Chiapasco, et al.21 (2004)
Prospective study
37 Max + Man + Hor + Ver
Alveolar distraction
138 Del 3 months
2.8 years 100 94.2
Chiapasco, et al.22 (2004)
Prospective study
5
10
Max + Man + Hor + Ver Vertical guided bone regeneration Alveolar distraction Autogenous (Ramus) 12 34 Del 6-7 months Del 3-4 months
1-3 years 100
100
75
94.1
Raghoebar, et al.83 (2002)
Prospective study
10 Man + Hor + Ver
Alveolar distraction
20 Del 2-3 months
0.9 years 95 X
Jensen, et al.50 (2002)
Prospective study
28 Max + Man + Hor + Ver
Alveolar distraction
84 Del 3-4 months
1-4.4 years
90.4 X
Rachmiel, et al.82 (2001)
Retrospective study
14 Max + Man + Hor + Ver
Alveolar distraction
23 Del 2-3 months
0.5-1.7 years
95.7 X
Continue in the next page
97.1% . Unfort unat ely, only nine st udies evaluat ed
t he im plant success rat e. This ranged from 92.7 t o
100.0% , and t he m ean was 95.5% .
Only seven st udies
21,22,25,57,79,81,86out of t he 17
w hich used alv eolar dist ract ion as a t r eat m ent
present ed t he m arginal bone level change in t heir
result s. The m arginal bone level change is shown in
Figure 3. Only four st udies present ed t he result s for
a follow- up period of 4 or 5 years. At baseline, t he
m arginal bone level change is around - 0.20 – - 0.50
m m , 1
styear of loading - 0.65 – - 1.17 m m , 2
ndyear
of loading - 1.00 – - 1.32 m m , 3
rdyear of loading
- 1.00 – - 1.41 m m , 4
t hyear of loading - 1.30 – - 1.46
m m , and 5
t hyear of loading - 1.49 – 1.55 m m .
I n la y t e ch n iqu e ( Ta ble 1 , Figu r e 4 )
T h e 5 1 a r t i c l e s i n c l u d e d p r o v i d e d f o u r
st udies
10,38,42,53wit h inlay t echnique, and one st udy
85used a com binat ion of onlay and inlay t echniques. Of
t hese, t wo were prospect ive st udies; one, a a split
m out h st udy; and one, a random ized clinical t rial.
A t ot al of 57 pat ient s wit h a vert ical resorpt ion of
part ially or t ot ally edent ulous alveolar ridges were
t reat ed wit h t he inlay t echnique. Sevent een pat ient s
were t reat ed wit h a com binat ion of onlay and inlay
t echniques. Three different donor m at erials for t he
bone where used: aut ogenous ( iliac
10,42, ram us
53) ,
xenograft s
38, and alloplast ic graft s
53. I n t ot al, 206
dent al im plant s were placed aft er 3 t o 6 m ont hs,
and t he m ean was 4.6 m ont hs aft er t he healing
of t he inlay t echnique. Aft er t he st art of loading,
t he follow- up ranged from 1 t o 3 years, and t he
m ean was 1.7 years. Survival rat es for t he dent al
im plant s in bone from t he inlay t echnique ranged
from 95.9 t o 100.0% , and t he m ean was 98.5% .
Un f or t u n at ely, on ly f ou r st u dies ev alu at ed t h e
im plant success rat e, which ranged from 90.9 t o
100.0% , and t he m ean was 93.4% .
Only t hree st udies
38,42,53out of t he four which
used t he inlay t echnique present ed t he m arginal
bone level change in t heir result s. The m arginal
b on e lev el ch an g e is sh ow n in Fig u r e 4 . On e
st udy
53has different t reat m ent groups, t herefore,
LWLVVKRZQWZLFHLQWKH¿JXUH1RQHRIWKHVWXGLHV
show ed a long- t er m follow- up. At baseline, t he
m arginal bone level change is around - 0.71 – - 1.21
m m , 1
styear of loading - 0.90 – - 1.65 m m , and 3
rdyear of loading - 2.43 m m .
Reference Study design Number of patients Defect type (type of atrophy) Surgical procedure Donor materials Number of implants Timing of implants Follow-up Implant survival (%) Implant success (%)
Simion, et al.96 (2001) Retrospective study 6 11 32 Max + Man + Hor + Ver Vertical guided bone regeneration Allograft Autogenous (Ramus, Chin) 17 26 82 Imm 5.3 years 3.3 years 2.5 years 94.1 100 100 94.1 96.1 100
Gaggl, et al.43 (2000)
Prospective study
34 Max + Man + Hor + Ver
Alveolar distraction
62 Imm 1 year 96 X
Keller, et al.55 (1999)
Retrospective study
28 4
Max + Hor + Ver Onlay technique Autogenous (Iliac) 183 21 Imm Del 4-6 months
5.6 years 86.3 91
X
Verhoeven, et al.109 (1997)
Prospective study
13 Man + Hor + Ver
Onlay technique
Autogenous (Iliac)
72 Imm 2.4 ± 0.9 years
100 X
McGrath, et al.66 (1996)
Retrospective study
18 Man + Hor + Ver
Onlay technique
Autogenous (Iliac)
36 Imm 1.4 years 91.6 91.6
Vermeeren, et al.110 (1996)
Retrospective study
31 Man + Hor + Ver
Onlay technique
Autogenous (Iliac)
78 Imm 5 years 89.7 X
Astrand, et al.7 (1996)
Retrospective study
17 Max + Hor + Ver
Onlay technique
Autogenous (Iliac)
92 Imm 3-5 y 75 X
Donovan et al.34 (1994)
Retrospective study
24 Max + Man + Hor + Ver Onlay technique Autogenous (Calvarium) 43 50 Imm Del 6-8 months 1.5 years 2.6 years 97.7 86 X X
Table 1-
Continuation
Alveolar distraction
,QOD\WHFKQLTXH
2QOD\WHFKQLTXH
Vertical guided bone
regeneration
Patients (n)
345
74
700
138
Implants (n)
1011
206
2155
347
Survival rate (%)
97.1
98.5
94.7
99.3
Success rate (%)
95.5
93.4
93.2
90.7
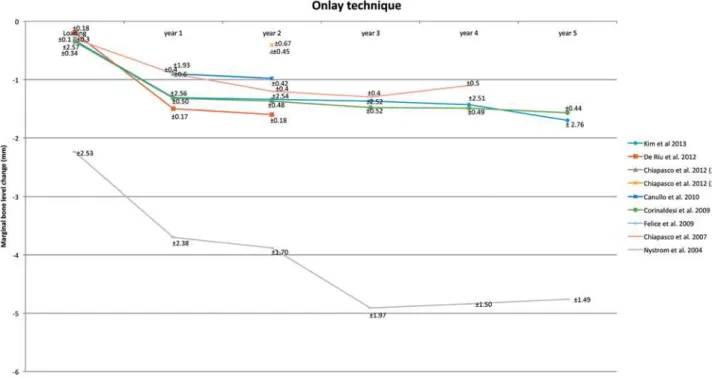
On la y t e ch n iqu e ( Ta ble 1 , Figu r e 5 )
T h e 5 1 a r t i c l e s i n c l u d e d p r o v i d e d 2 7
s t u d i e s
1 , 7 , 1 5 , 1 6 , 2 0 , 2 5 , 2 9 , 3 3 , 3 5 , 4 1 , 5 4 , 5 6 , 5 7 , 6 2 , 6 4 , 6 5 , 6 9 - 7 1 , 73, 77, 85, 91, 99, 106, 109, 110w it h onlay t echnique, and one
st u dy
8 4u sed a com bin at ion of in lay an d on lay
t echniques. Thir t een st udies w er e r et r ospect ive
while 14 were prospect ive. A t ot al of 683 pat ient s
w it h a v er t ical r esor pt ion of par t ially or t ot ally
edent ulous alveolar ridges were t reat ed wit h t he
onlay t echnique. Sevent een pat ient s were t reat ed
wit h a com binat ion of onlay and inlay t echniques.
Three different donor m at erials for t he bone where
u sed : au t o g en o u s ( i l i ac
7 , 3 6 , 4 2 , 5 5 , 5 8 , 6 3 , 6 6 , 7 4 , 9 1 , 1 0 9 , 1 1 0,
ram us
20,25,29,36,57,78, calvarium
20,34,99,106, chin
36, t ibia
36,
and coronoid
31) , allograft s
1,16,70- 72,85, and alloplast ic
graft s
15. I n t ot al, 910 dent al im plant s were placed
im m ediat ely, 1245 dent al im plant s w er e placed
aft er 3 t o 9 m ont hs, and t he m ean was 5.5 m ont hs
Figure 3-
Alveolar distraction. Mean and Standard Deviation are indicated
aft er t he healing of t he onlay t echnique. Aft er t he
st art of loading, t he follow- up ranged from 1.4 t o
10 years, and t he m ean was 3.5 years. Survival
rat es for t he dent al im plant s in bone from t he onlay
t echnique ranged from 72.8 t o 100.0% , and t he
m ean was 94.7% . Unfort unat ely, only 14 st udies
evaluat ed t he im plant success rat e, which ranged
from 86.9 t o 100.0% , and t he m ean was 93.2% .
Only eight st udies
15,20,25,29,31,42,57,74out of t he 27
w hich used t he onlay t echnique as a t r eat m ent
present ed t he m arginal bone level change in t heir
result s. The m arginal bone level change is shown
in Figure 5. One st udy
20has different t reat m ent
JURXSVWKHUHIRUHLWLVVKRZQWZLFHLQWKH¿JXUH
Only four st udies present ed t he result s for a
follow-up period of 4 or 5 years. At baseline, t he m arginal
bone level change is around - 0.30 – - 2.24 m m ,
1
styear of loading - 0.85 – - 3.70 m m , 2
ndyear of
Figure 5-
Onlay technique. Mean and Standard Deviation are indicated
loading - 0.41 – - 3.88 m m , 3
rdyear of loading - 1.30
– - 4.91 m m , 4
t hyear of loading - 1.10 – - 4.84 m m ,
and 5
t hyear of loading - 1.57 – - 4.76 m m .
V e r t ica l gu ide d bon e r e ge n e r a t ion ( Ta ble
1 , Figu r e 6 )
Th e 5 1 a r t i cl e s i n cl u d e d p r o v i d e d se v e n
s t u d i e s
6 , 2 2 , 6 1 , 8 0 , 9 6 , 1 0 0 , 1 0 5w i t h v e r t i c a l b o n e
r egenerat ion. Thr ee st udies w er e r et r ospect iv e
while 4 were prospect ive. A t ot al of 138 pat ient s
w it h a v er t ical r esor pt ion of par t ially or t ot ally
edent ulous alveolar ridges were t reat ed wit h vert ical
guided bone r egenerat ion. Tw o differ ent donor
m at er ials for t he bone w er e used: aut ogenous
( r am u s
2 2 , 9 6 , 1 0 5an d ch in
9 6 , 1 0 5) an d allogr af t s
6 1 , 1 0 0.
Moreover, com binat ions of different donor m at erials
for t he bone w ere used - aut ogenous+ allograft
6and aut ogenous+ xenograft
80. I n t ot al, 141 dent al
im plan t s w er e placed im m ediat ely, 2 0 6 den t al
im plant s were placed aft er 4 t o 12 m ont hs, and
t he m ean w as 7. 8 m ont hs aft er t he healing of
t he vert ical bone regenerat ion. Aft er t he st art of
loading, t he follow- up ranged from 1.0 t o 5.3 years,
and t he m ean was 2.4 years. The survival rat es for
t he dent al im plant s in bone from t he vert ical bone
regenerat ion ranged from 94.1 t o 100.0% , and t he
m ean was 99.3% . The im plant success rat e ranged
from 75.0 t o 100.0% , and t he m ean was 90.7% .
All t he seven st udies
6,22,61,80,96,100,105which used
vert ical bone regenerat ion as a t reat m ent present ed
t he m arginal bone level change in t heir result s.
The m arginal bone level change is shown in Figure
5. One st udy
96has differ ent t r eat m ent gr oups,
WKHUHIRUHLWLVVKRZQWKUHHWLPHVLQWKH¿JXUH2QO\
t wo st udies present ed t he result s for a follow- up
period of 5 years. At baseline, t he m arginal bone
level change is around 0.41 – - 1.29 m m , 1
styear
of loading - 0.85 – - 2.64 m m , 2
ndyear of loading
- 1.35 – - 2.64 m m , 3
rdyear of loading - 1.27 – - 2.64
m m , 4
t hyear of loading - 1.00 – - 2.64 m m , and 5
t hyear of loading - 1.00 – - 2.86 m m .
D I SCUSSI ON
I n t he lit erat ur e, ev idence is available about
t h e st ab ilit y of v er t ical b on e au g m en t at ion . A
w ide range of differ ent t echniques was used t o
vert ically augm ent t he bone. This review t ried t o
syst em at ically evaluat e t he current evidence and
t o com par e t he differ ent v er t ical augm ent at ion
t echniques as w ell as t heir m ar ginal bone level
change on t he long- t erm . I n t ot al, 51 art icles could
be included, from which t he dat a were obt ained.
Only 21 art icles out of 51 cont ained inform at ion
about t he m arginal bone level change. Line graphs
wit h st andard deviat ion were used t o present t he
m arginal bone level change over a long period of
t im e.
Few art icles
4,5,17,101showing t he m arginal bone
lev el ch an g e ar ou n d a su ccessf u l im p lan t ar e
available in lit erat ure. I n order t o assess t he st abilit y
of an im plant in augm ent ed bone, it is im port ant
t o know t he m arginal bone level change around a
successful im plant in non- augm ent ed bone. The
m ost recent dat a about m arginal bone level change
around non- augm ent ed im plant s were discussed
at t he Thir d EAO consensus confer ence. I n t his
art icle, dat a of im plant s in an augm ent ed side were
collect ed and com pared wit h t he EAO consensus
conference conclusions.
Alve ola r dist r a ct ion
The analysis shows t hat t he im plant survival and
success rat es are com parable wit h dent al im plant s
which are placed in non- augm ent ed bone
4. The line
graph ( Figure 2) shows an overview of t he m arginal
ERQHOHYHOFKDQJHIRUWKH¿UVW\HDUV2QO\WKUHH
st udies present t he result s for a follow- up period of
4 or 5 years
21,57,81. Unfort unat ely, it was not possible
t o com bine t hose result s. The m arginal bone level
change bet ween abut m ent connect ion and 1
styear
of loading varies bet ween - 0.60 – - 0.97 m m . Aft er
t he 2
ndyear, it varies bet ween - 0.1 – - 0.3 m m ; aft er
t he 3
rdyear, bet ween - 0.06 – - 0.17 m m ; aft er t he
4
t hyear, bet ween 0 – - 0.2 m m ; and aft er t he 5
t hyear of loading it is - 0.09 m m . These dat a are in
agreem ent wit h t he present success crit eria for t he
1
styear of loading, which allows a m arginal bone
loss of 1- 1.5 m m
5,17. I n t he 2
nd, 3
rd, 4
t h, and 5
t hyear,
t he bone loss is, in m ost of t he st udies, m ore t han
0.1 m m . This could indicat e t hat t he r esor pt ion
rat e is m ore rapidly progressing com pared t o
non-augm ent ed bone.
Al v eo l a r d i st r a ct i o n i n i t i a t es n a t u r a l b o n e
form at ion bet ween t he dist ract ed segm ent and t he
basal bone. Therefore, t here is no need for bone
graft ing, but for a narrow ridge inst ead. For a narrow
ridge, a bone graft ing is bet t er t o use, since it can
r ebuild t he hor izont al and ver t ical com ponent s.
Alv eolar dist ract ion seem s t o be only indicat ed
for t he m andible because of t he pneum at isat ion
of t he sinus in t he m axilla. A disadvant age of t his
t echnique is t he early resorpt ion of t he dist ract ed
bone. I t is essent ial t o consider som e overcorrect ion
dur ing t r eat m ent planning for dir ect ly av oiding
surgical relapse and anot her surgical int ervent ion
for addit ional augm ent at ion. Alveolar dist ract ion
u n d er g oes a m or e act iv e r em od elin g p r ocess
b e ca u se o f t h e b e t t e r v a scu l a r i za t i o n w h e n
com pared t o a block graft
47. For t he long- t erm , t he
m arginal bone level change m ight be m ore st able.
I n la y t e ch n iqu e
line graph ( Figur e 3) show s an over view of t he
PDUJLQDOERQHOHYHOFKDQJHIRUWKH¿UVW\HDUV
Only one st udy
38present s a follow- up period of 3
years. Unfort unat ely, it was not possible t o draw
any conclusion.
The inlay t echnique is a t echnique in w hich
a new graft is placed bet w een t he cranial bone
segm ent and t he basal bone. The inlay t echnique
LQ WKH PD[LOOD LV XVXDOO\ VHHQ DV D VLQXV ÀRRU
au gm en t at ion . Th is par t is ex clu ded f r om t h is
r ev iew. For a n ar r ow r idge, a h or izon t al bon e
JUDIWLQJLVVRPHWLPHVQHHGHG$GLI¿FXOW\IRUWKH
inlay t echnique is t he m anagem ent of soft t issues.
7KHVRIWWLVVXHVQHHGWRPDLQWDLQVXI¿FLHQWEORRG
su pply t o t h e bon e segm en t w h ich is cr an ially
displaced. The risk of wound dehiscence could arise
when t here is t oo m uch t ension aft er wound closure.
Unfort unat ely, no long- t erm follow- up st udies are
available. Th er efor e, a com par ison w it h den t al
im plant s in non- augm ent ed bone is not possible.
On la y t e ch n iqu e
The analysis shows t hat im plant survival and
success rat es are com parable wit h dent al im plant s
which are placed in non- augm ent ed bone. The line
graph ( Figure 4) shows an overview of t he m arginal
ERQHOHYHOFKDQJHIRUWKH¿UVW\HDUV2QO\IRXU
st udies present t he result s for a follow- up period
of 4 or 5 years
25,29,57,74. Unfort unat ely, it was not
possible t o com bine t hose result s. The m arginal
bone level change bet ween abut m ent connect ion
and 1
styear of loading varies bet ween - 0.60 – - 1.46
m m ; aft er t he 2
ndyear, bet ween - 0.03 – 0.30 m m ;
aft er t he 3
r dyear, bet w een - 0. 03 – - 1. 03 m m ;
aft er t he 4
t hyear, bet ween 0.2 – - 0.06 m m ; and
aft er t he 5
t hyear of loading, bet ween 0.08 – - 0.27
m m . These dat a are in agreem ent wit h t he present
success crit eria for t he 1
styear of loading, which
allows a m arginal bone loss of 1- 1.5 m m , and of 0.1
m m for t he 2
nd, 3
rd, 4
t h, and 5
t hyear
5,17. However,
one st udy
74show ed m ore m arginal bone loss in
com parison wit h ot hers
25,29,57.
The onlay t echnique is done m ost ly w it h an
au t ogen ou s bon e gr aft . Befor e t h e y ear 2 0 0 0 ,
m ost im plant s were im m ediat ely placed t oget her
wit h t he bone graft s. The im plant s were used t o
secure t he graft . The capacit y and volum e of t he
bon e gr af t s ar e v ar iable bet w een t h e st u dies.
These differences could be explained by different
follow- up periods, t im ing of im plant s placem ent ,
different sit es, and different bone graft ing m at erial.
2YHUDOO WKH UHVRUSWLRQ UDWH LV KLJKHU LQ WKH ¿UVW
year, but st abilizes aft er it . The aut ogenous bone
graft is st ill t he m ost fr equent ly used graft for
t he onlay t echnique. I t is a r ecom m endat ion t o
use cort icocancellous bone inst ead of part iculat ed
bone graft s. I deally, over sized graft s should be
har vest ed t o m aint ain enough volum e aft er t he
LQLWLDO UHVRUSWLRQ SKDVH 7KH PDMRU GLI¿FXOW\ IRU
t he onlay t echnique is t he m anagem ent of t he soft
t issues t o m aint ain a full wound closure. For t he
long- t erm , it seem s t hat t he m arginal bone level
change is com parable wit h dent al im plant s in
non-augm ent ed bone.
V e r t ica l gu ide d bon e r e ge n e r a t ion
The analysis show s t hat t he im plant sur vival
is com parable w her eas t he success rat e is not
com parable wit h dent al im plant s which are placed
in non- augm ent ed bone. The line graph ( Figur e
5) shows an overview of t he m arginal bone level
FKDQJH IRU WKH ¿UVW \HDUV 2QO\ WZR VWXGLHV
pr esent t he r esult s for a follow - up per iod of 5
y ear s
9 6 , 1 0 5. Un f or t u n at ely, on ce ag ain it is n ot
possible t o com bine t hose result s. The m arginal
bone level change bet ween abut m ent connect ion
and 1
styear of loading varies bet ween - 1.01 – - 1.86
m m ; aft er t he 2
ndyear, bet ween 0.05 – - 0.02 m m ;
aft er t he 3
rdyear, bet ween 0.11 – - 0.06 m m ; aft er
t he 4
t hyear, bet ween 0.27 – - 0.02 m m ; and aft er
t he 5
t hyear of loading, bet ween 0 – - 0.22 m m .
These dat a ar e in agr eem ent w it h t he pr esent
success crit eria for t he 1
styear of loading, which
DOORZVDPDUJLQDOERQHORVVGXULQJWKH¿UVW\HDURI
1- 1.5 m m , and of 0.1 m m for t he 2
nd, 3
rd, 4
t h, and
5
t hyear
5,17. However, one st udy
96has a different
am ount of dent al im plant s dur ing t he follow- up
SHULRGZKLFKFRXOGLQÀXHQFHWKHRXWFRPH
Ver t i cal g u i d ed b o n e r eg en er at i o n i m p l i es
t h a t t h e r e g e n e r a t i o n o f o sse o u s d e f e ct s i s
p r e d i ct a b l y a t t a i n a b l e v i a t h e a p p l i ca t i o n o f
o c c l u s i v e m e m b r a n e s , w h i c h m e c h a n i c a l l y
ex clu d e n on - ost eog en ic cell p op u lat ion s f r om
t he sur r ounding soft t issues. I n t he past ,
non-resorbable m em branes were used, but nowadays
resorbable m em branes are com m on. The defect
LVDOZD\V¿OOHGZLWKSDUWLFXODWHDXWRJHQRXVERQH
and som et im es m ixed wit h xenograft or allograft .
Wound dehiscence is oft en seen as a com plicat ion.
Therefore, it is im port ant t o get as lit t le t ract ion on
t he wound as possible. For t he long- t erm , it seem s
t hat t he m arginal bone level loss is com parable wit h
dent al im plant s in non augm ent ed bone.
I n t h e lit er at u r e, a lot of d if f er en t cr it er ia
is u sed t o det er m in e t h e su r v ival an d su ccess
rat es of dent al im plant s. The lack of universally
accept ed success crit eria m akes t he int erpret at ion
DQG FRPSDULVRQ RI WKH GDWD UHDOO\ GLI¿FXOW
76. I n
addit ion, a st at ist ical problem is perceived. There
is a discrepancy in report ed out com es when t he
prim ary unit of analysis is t he pat ient inst ead of
t h e den t al im plan t
8 7 , 8 8. Th er ef or e, t h e decision
Som e new guidelines were proposed in t he VI I I
European Workshop on Periodont ology. A successful
dent al im plant has t o m eet crit eria concerning t issue
physiology ( osseoint egrat ion) , funct ion ( chewing) ,
absence of pain, and user sat isfact ion
1017KH¿UVW
crit eria for m arginal bone loss exist since 1986
5.
This review shows t hat t he m arginal bone loss aft er
DEXWPHQWFRQQHFWLRQDQGWKH¿UVW\HDURIORDGLQJ
var ies bet w een 1. 0 and 1. 5 m m . This is called
saucerisat ion, and is caused by t he est ablishm ent
of t he biological widt h. Recent st udies allow a m ean
PDUJLQDOERQHORVVRIPPLQWKH¿UVW\HDURI
loading, and an annual of 0.1 m m bone loss can
be expect ed in t he following years
17. The crit eria
are divided int o t hree dom ains t hat are im port ant
for ident ify ing t he success of a dent al im plant .
Th ese dom ain s ar e: pat ien t - r epor t ed ou t com e
m easures ( healt h- relat ed qualit y of live and general
sat isfact ion) , peri- im plant healt h ( m arginal bone
level, bleeding on probing, and probing dept h) , and
im plant - suppor t ed r est orat ions ( longevit y of t he
rest orat ion, funct ion/ occlusion relat ed out com es,
and t echnical com plicat ions)
101.
To give a com plet e overview about t he different
t echniques, ever y t y pe of graft ing m at er ial was
included. Depending on t he graft ing m at erial used,
a different resorpt ion occurs. That is why t he result s
are present ed in graphs and t ables, which facilit at es
t he decision of clinicians regarding what t ype of
gr aft in g m at er ial m u st be u sed. No dist in ct ion
is m ade bet w een t he differ ent durat ions of t he
follow- up period, even t hough t here was a wide
range of it . The follow- up period needs t o be of at
least one year. These different lengt hs of follow- up
periods are included in t he calculat ions. However,
an im plant success rat e of 100% aft er one year
cannot be com pared wit h a success rat e aft er 10
years. Furt herm ore, different follow- up periods per
pat ient in a st udy are pooled t oget her. This could
lead t o a com plet e different out com e. This review
is designed t o give a com plet e overview, t hus, t he
clinician can decide what t he best t reat m ent is.
Aft er analysis of t he art icles about vert ical bone
augm ent at ion, t he m ain conclusion w as t hat a
wide range of different t echniques and m at erials
were used, and also different pat ient groups, st udy
design s, an t ibiot ic pr escr ipt ion s, an d follow - u p
r egim es. Because of t his, no m et a- analysis was
conduct ed, for once a m et a- analysis is perform ed,
it causes a bias.
Anot her lim it at ion of t his review is t hat it was
not possible t o separat e t he dat a for single t oot h
gap, m ult iple m issing t eet h, or an edent ulous ridge
in t he different art icles used. These different clinical
sit uat ions were m ost ly pooled t oget her; t herefore,
LWZDVKDUGWRDQDO\]HDVSHFL¿FWHFKQLTXHIRUD
VSHFL¿F FOLQLFDO FRQGLWLRQ )RU PRVW GHIHFW DQG
especially in t he at rophic j aws, t he descript ion of t he
seize of t he defect was hardly present , which was
also a t opic in t he last I TI Consensus Conference
11.
%DVHG RQ RXU SUHYLRXV ¿QGLQJV LW LV KDUG WR
st at e which vert ical bone augm ent at ion is t he best
t o u se. How ev er, w h en on ly con sider in g t h ose
vert ical bone augm ent at ion t echniques for which
st udies exist wit h a follow- up period of at least 4 t o
5 years, t here seem s t o be a t rend t hat t he onlay
t echnique, alveolar dist ract ion, and vert ical guided
bone regenerat ion are st able for at least 4 t o 5
years. Since it was not possible t o carry out m et
a-analyt ic procedures, a conclusion about st abilit y is
QRWMXVWL¿HGEXWDWUHQGLVVWLOOYLVLEOH+RZHYHU
IXUWKHUUHVHDUFKLVQHFHVVDU\WRFODULI\WKLV¿QGLQJ
More st udies t hat follow t he m arginal bone level
change for a longer period are necessary, in addit ion
t o bet t er descript ion and ridge m easurem ent s of t he
clinical sit uat ion before and aft er t he augm ent at ion
procedure. This will enable a bet t er int erpret at ion
of t he result s and allow t he clinician t o conclude
ZKLFKVSHFL¿FDXJPHQWDWLRQLVUHFRPPHQGHGDQG
in which clinical sit uat ion.
ACKN OW LED GEM EN TS
Th is p ap er h as b een p r ep ar ed w it h ou t an y
sou r ces of in st it u t ion al, p r iv at e, or cor p or at e
f in an cial su p p or t , an d t h er e ar e n o p ot en t ial
FRQÀLFWVRILQWHUHVW
REFEREN CES
1- Acocella A, Bert olai R, Ellis E 3rd, Nissan J, Sacco R. Maxillary alveolar ridge reconst ruct ion wit h m onocort ical fresh- frozen bone block s: a clinical, hist ological and hist om or phom et r ic st udy. J Craniom axillofac Surg. 2012; 40: 525- 33.
2- Adell R, Lekholm U, Gröndahl K, Brånem ark PI , Lindst röm J, Jacobsson M. Reconst r uct ion of sever ely r esor bed edent ulous
PD[LOODHXVLQJRVVHRLQWHJUDWHG¿[WXUHVLQLPPHGLDWHDXWRJHQRXV
bone graft s. I nt J Oral Maxillofac I m plant s. 1990; 5: 233- 46. 3- Adell R, Lekholm U, Rockler B, Brånem ark PI . A 15- year st udy of osseoint egrat ed im plant s in t he t reat m ent of t he edent ulous j aw. I nt J Oral Surg. 1981; 10: 387- 416.
4- Albrekt sson T, Donos N, Working Group 1. I m plant survival and com plicat ions. The Third EAO consensus conference 2012. Clin Oral I m plant s Res. 2012; 23: 63- 5.
5- Albrekt sson T, Zarb G, Wort hingt on P, Eriksson AR. The
long-WHUP HI¿FDF\ RI FXUUHQWO\ XVHG GHQWDO LPSODQWV D UHYLHZ DQG
pr oposed cr it er ia of success. I nt J Oral Max illofac I m plant s. 1986; 1: 11- 25.
6- Annibali S, Bignozzi I , Sam m art ino G, La Monaca G, Crist alli MP. Hor izon t al an d v er t ical r idge au gm en t at ion in localized
DOYHRODUGH¿FLHQWVLWHVDUHWURVSHFWLYHFDVHVHULHV,PSODQW'HQW
2012; 21: 175- 85.
7- Ast rand P, Nord PG, Branem ark PI . Tit anium im plant s and onlay bone graft t o t he at rophic edent ulous m axilla: a 3-year longit udinal st udy. I nt J Oral Maxillofac Surg. 1996; 25: 25- 9.
10- Bianchi A, Felice P, Lizio G, Marchet t i C. Alveolar dist ract ion ost eogenesis versus inlay bone graft ing in post erior m andibular at rophy: a prospect ive st udy. Oral Surg Oral Med Oral Pat hol Oral Radiol Endod. 2008; 105: 282- 92.
11- Bornst ein MM, Al- Nawas B, Kuchler U, Tahm aseb A. Consensus st at em en t s an d r ecom m en ded clin ical pr ocedu r es r egar din g cont em porar y sur gical and radiographic t echniques in im plant dent ist ry. I nt J Oral Maxillofac I m plant s. 2014; 29: 78- 82. 1 2 - Br av i F, Br u sch i GB, Fer r i n i F. A 1 0 - y ear m u l t i cen t er r et r ospect ive clinical st udy of 1715 im plant s placed w it h t he ed en t u l o u s r i d g e ex p an si o n t ech n i q u e. I n t J Per i o d o n t i cs Rest orat ive Dent . 2007; 27: 557- 65.
13- Browaeys H, Bouvry P, De Bruyn H. A lit erat ure review on biom at erials in sinus augm ent at ion procedures. Clin I m plant Dent Relat Res. 2007; 9: 166- 77.
14- Buser D, I ngim arsson S, Dula K, Lussi A, Hirt HP, Belser UC. Long- t erm st abilit y of osseoint egrat ed im plant s in augm ent ed bone: a 5- year prospect ive st udy in part ially edent ulous pat ient s. I nt J Periodont ics Rest orat ive Dent . 2002; 22: 109- 17.
15- Canullo L, Sist i A. Early im plant loading aft er vert ical ridge augm ent at ion ( VRA) using e- PTFE t it anium - reinforced m em brane and nano- st ruct ured hydroxyapat it e: 2- year prospect ive st udy. Eur J Oral I m plant ol. 2010; 3: 59- 69.
16- Carinci F, Brunelli G, Zollino I , Franco M, Viscioni A, Rigo L, et al. Mandibles graft ed wit h fresh- frozen bone: an evaluat ion of im plant out com e. I m plant Dent . 2009; 18: 86- 95.
17- Cecchinat o D, Bengazi F, Blasi G, Bot t icelli D, Cardarelli I , Gualini F. Bone level alt erat ions at im plant s placed in t he post erior segm ent s of t he dent it ion: out com e of subm erged/ non- subm erged healing. A 5- year m ult icent er, random ized, cont rolled clinical t rial. Clin Oral I m plant s Res. 2008; 19: 429- 31.
18- Chiapasco M, Abat i S, Rom eo E, Vogel G. Clinical out com e of aut ogenous bone blocks or guided bone regenerat ion wit h e- PTFE m em branes for t he reconst ruct ion of narrow edent ulous ridges. Clin Oral I m plant s Res. 1999; 10: 278- 88.
19- Chiapasco M, Casent ini P, Zaniboni M. Bone augm ent at ion procedures in im plant dent ist ry. I nt J Oral Maxillofac I m plant s. 2009; 24: 237- 59.
20- Chiapasco M, Casent ini P, Zaniboni M, Corsi E. Evaluat ion of peri- im plant bone resorpt ion around St raum ann Bone Level im plant s placed in areas reconst ruct ed wit h aut ogenous vert ical onlay bone graft s. Clin Oral I m plant s Res. 2012; 23: 1012- 21. 2 1 - Ch iap asco M, Con solo U, Bian ch i A, Ron ch i P. Alv eolar
GLVWUDFWLRQRVWHRJHQHVLVIRUWKHFRUUHFWLRQRIYHUWLFDOO\GH¿FLHQW
edent ulous ridges: a m ult icent er prospect ive st udy on hum ans. I nt J Oral Maxillofac I m plant s. 2004; 19: 399- 407.
22- Chiapasco M, Rom eo E, Casent ini P, Rim ondini L. Alveolar dist ract ion ost eogenesis vs. vert ical guided bone regenerat ion
IRU WKH FRUUHFWLRQ RI YHUWLFDOO\ GH¿FLHQW HGHQWXORXV ULGJHV D
1- 3- year prospect ive st udy on hum ans. Clin Oral I m plant s Res. 2004; 15: 82- 95.
23- Chiapasco M, Rom eo E, Coggiola A, Brusat i R. Long- t erm
RXWFRPHRIGHQWDOLPSODQWVSODFHGLQUHYDVFXODUL]HG¿EXODIUHH ÀDSVXVHGIRUWKHUHFRQVWUXFWLRQRIPD[LOORPDQGLEXODUGHIHFWV
due t o ext rem e at rophy. Clin Oral I m plant s Res. 2011; 22: 83- 91. 24- Chiapasco M, Zaniboni M, Boisco M. Augm ent at ion procedures
IRU WKH UHKDELOLWDWLRQ RI GH¿FLHQW HGHQWXORXV ULGJHV ZLWK RUDO
im plant s. Clin Oral I m plant s Res. 2006; 17: 136- 59.
25- Chiapasco M, Zaniboni M, Rim ondini L. Aut ogenous onlay bone graft s vs. alveolar dist ract ion ost eogenesis for t he correct ion of
YHUWLFDOO\GH¿FLHQWHGHQWXORXVULGJHVD\HDUSURVSHFWLYHVWXG\
on hum ans. Clin Oral I m plant s Res. 2007; 18: 432- 40.
26- Chin M. Dist ract ion ost eogenesis for dent al im plant s. At las Oral Maxillofac Surg Clin Nort h Am . 1999; 7: 41- 63.
27- Cordaro L, Torsello F, Accorsi Ribeiro C, Liberat ore M, Mirisola d i Tor r esan t o V. I n lay - on lay g r af t in g f or t h r ee- d im en sion al reconst ruct ion of t he post erior at rophic m axilla wit h m andibular bone. I nt J Oral Maxillofac Surg. 2010; 39: 350- 7.
28- Cordaro L, Torsello F, Miuccio MT, di Torresant o VM, Eliopoulos D. Mandibular bone harvest ing for alveolar reconst ruct ion and im plan t placem en t : su bj ect iv e an d obj ect iv e cr oss- sect ion al evaluat ion of donor and recipient sit e up t o 4 years. Clin Oral I m plant s Res. 2011; 22: 1320- 6.
29- Corinaldesi G, Pieri F, Sapigni L, Marchet t i C. Evaluat ion of survival and success rat es of dent al im plant s placed at t he t im e of or aft er alveolar ridge augm ent at ion wit h an aut ogenous m andibular bone graft and t it anium m esh: a 3- t o 8- year ret rospect ive st udy. I nt J Oral Maxillofac I m plant s. 2009; 24: 1119- 28.
30- Dahlin C, Johansson A. I liac crest aut ogenous bone graft v er sus alloplast ic graft and guided bone r egenerat ion in t he reconst ruct ion of at rophic m axillae: a 5- year ret rospect ive st udy on cost- effect iveness and clinical out com e. Clin I m plant Dent Relat Res. 2011; 13: 305- 10.
31- De Riu G, Meloni MS, Pisano M, Baj A, Tullio A. Mandibular coronoid process graft ing for alveolar ridge defect s. Oral Surg Oral Med Oral Pat hol Oral Radiol. 2012; 114: 430- 6.
32- Den Hart og L, Slat er JJ, Vissink A, Meij er HJ, Raghoebar GM. Treat m ent out com e of im m ediat e, early and convent ional single-t oosingle-t h im plansingle-t s in single-t he aessingle-t hesingle-t ic zone: a sy ssingle-t em asingle-t ic r ev iew single-t o survival, bone level, soft- t issue, aest het ics and pat ient sat isfact ion. J Clin Periodont ol. 2008; 35: 1073- 86.
3 3 - Din op ou los H, Dim it r iou R, Gian n ou d is PV. Bon e g r af t subst it ut es: What are t he opt ions? Surgeon. 2012; 10: 230- 9. 3 4 - Don ov an MG, Dick er son NC, Han son LJ, Gu st af son RB. Maxillary and m andibular reconst ruct ion using calvarial bone graft s and Branem ark im plant s: a prelim inary report . J Oral Maxillofac Surg. 1994; 52: 588- 94.
35- Elian N, Jalbout Z, Ehrlich B, Classi A, Cho SC, Al- Kaht ani F, et al. A t wo- st age full- arch ridge expansion t echnique: review of t he lit erat ure and clinical guidelines. I m plant Dent . 2008; 17: 16- 23. 36- Elo JA, Herford AS, Boyne PJ. I m plant success in dist ract ed bone ver sus aut ogenous bone- graft ed sit es. J Oral I m plant ol. 2009; 35: 181- 4.
37- Enislidis G, Fock N, Millesi- Schobel G, Klug C, Wit t wer G, Yerit K, et al. Analysis of com plicat ions following alveolar dist ract ion ost eogenesis and im plant placem ent in t he part ially edent ulous m andible. Oral Sur g Oral Med Oral Pat hol Oral Radiol Endod. 2005; 100: 25- 30.
38- Esposit o M, Cannizarro G, Soardi E, Pellegrino G, Pist illi R, Felice P. A 3- year post- loading report of a random ised cont rolled t rial on t he rehabilit at ion of post erior at rophic m andibles: short im plant s or longer im plant s in vert ically augm ent ed bone? Eur J Oral I m plant ol. 2011; 4: 301- 11.
39- Esposit o M, Pellegrino G, Pist illi R, Felice P. Rehabilit at ion of post erior at rophic edent ulous j aws: prost heses support ed by 5 m m short im plant s or by longer im plant s in augm ent ed bone? One- year result s from a pilot random ised clinical t rial. Eur J Oral I m plant ol. 2011; 4: 21- 30.
40- Et t l T, Gerlach T, Schüsselbauer T, Gosau M, Reichert TE, Dr iem el O. Bon e r esor p t ion an d com p licat ion s in alv eolar dist ract ion ost eogenesis. Clin Oral I nvest ig. 2010; 14: 481- 9. 41- Felice P, Pellegrino G, Checchi L, Pist illi R, Esposit o M. Vert ical augm ent at ion w it h int er posit ional block s of anor ganic bov ine bone v s. 7- m m - long im plant s in post er ior m andibles: 1- year r esult s of a random ized clinical t r ial. Clin Oral I m plant s Res. 2010; 21: 1394- 403.