REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
In
vitro
comparison
of
epidural
bacteria
filters
permeability
and
screening
scanning
electron
microscopy
Aysin
Sener
a,
Yuksel
Erkin
b,
Alper
Sener
c,∗,
Aydin
Tasdogen
b,
Esra
Dokumaci
d,e,
Zahide
Elar
baAnesthesiologyandReanimationDepartment,CanakkaleGovermentHospital,Canakkale,Turkey bAnesthesiologyandReanimationDepartment,DokuzEylulUniversity,FacultyofMedicine,Izmir,Turkey cInfectiousDiseaseDepartment,OnsekizMartUniversity,FacultyofMedicine,Canakkale,Turkey
dMetallurgyandMaterialEngineeringDepartment,DokuzEylulUniversity,FacultyofEngineering,Izmir,Turkey eDepartmentofMaterialScience,DokuzEylulUniversity,FacultyofEngineering,Izmir,Turkey
Received11July2013;accepted15August2013 Availableonline11November2013
KEYWORDS
Bacteriafilter; Staphylococcus aureus; Pseudomonas aeruginosa; Scanningelectron microscope
Abstract
Backgroundandobjectives: Epidural catheter bacteria filters are barriers in the patient-controlledanalgesia/anaesthesiaforpreventingcontaminationattheepiduralinsertionsite. Theefficiencyofthesefiltersvariesaccordingtoporesizesandmaterials.
Method: Thebacterialadhesioncapabilityofthetwofilterswasmeasuredinvitroexperiment. AdhesioncapacitiesforstandardStaphylococcusaureus(ATCC25923)andPseudomonas aeru-ginosa(ATCC27853)strainsofthetwodifferentfilters(PortexandRusch)whichhavethesame poresizewereexamined.Bacterialsuspensionof0.5Mc Farlandwasplacedinthe patient-controlledanalgesiapump,wasfilteredataspeedof5mL/h.incontinuous infusionfor48h andaccumulatedinbottle.Thetwofilterswerecompared withcolonycountsofbacteriain thefiltersandbottles.Atthesametime,thefiltersandadheredbacteriaweremonitoredby scanningelectronmicroscope.
Results:ElectronmicroscopicexaminationoffiltersshowedthatthePortexfilterhada gran-ular and theRusch filter fibrillary structure.Colony counting fromthe catheterand bottle showedthatbothofthefiltershavesignificantbacterialadhesioncapability(p<0.001).After thebacteriasuspensioninfusion,colonycountingsshowedthatthePortexfilterwasmore effi-cient(p<0.001).TherewasnotanydifferencebetweenS.aureusandP.aeruginosabacteria adhesion.IntheSEMmonitoringaftertheinfusion,itwasphysicallyshownthatthebacteria wereadheredefficientlybybothofthefilters.
∗Correspondingauthor.
E-mail:[email protected](A.Sener).
Conclusion:Thegranular structuredfilterwasfound statisticallyandsignificantlymore suc-cessfulthanthefibrial.Althoughtheporesizesofthefiltersweresame---ofwhichstructural differencesshownbySEMwerethesame---itwouldnotberighttoattributethechangesin theefficienciestoonlystructuraldifferences.Usingmicrobiologicalandphysicalproofswith regardtoefficiencyatthesametimehasbeenanotherimportantaspectofthisexperiment. ©2013SociedadeBrasileiradeAnestesiologia.PublishedbyElsevier EditoraLtda.Allrights reserved.
PALAVRAS-CHAVE
Filtroantibacteriano; Staphylococcus aureus; Pseudomonas aeruginosa; Microscópio eletrônicode varredura
Comparac¸ãoinvitrodapermeabilidadedefiltrosepiduraisantibacterianosetriagem pormicroscopiaeletrônicadevarredura
Resumo
Justificativaeobjetivos: Osfiltrosantibacterianosparacateterepiduralsãobarreirasda anal-gesia/anestesia controlada pelopaciente para evitar a contaminac¸ão do local de inserc¸ão epidural.Aeficáciadessesfiltrosvariadeacordocomomaterialetamanhodosporos.
Método: A capacidade deaderência bacterianados doisfiltros foimedida em experimento
invitro.AvaliamosacapacidadedeaderênciadascepaspadrãodeStaphylococcusaureus(ATCC 25923)ePseudomonasaeruginosa(ATCC27853)dedoisfiltrosdiferentes(PortexeRusch),mas comporosdomesmotamanho.Umasuspensãobacterianagrau0,5deMcFarlandfoicolocadana bombadeanalgesiacontroladapelopacienteefiltradaaumavelocidadede5mL/heminfusão contínuapor48heacumuladaemfrasco.Osdoisfiltrosforamcomparadoscomcontagensde colôniasdebactériasnosfiltrosefrascos.Aomesmotempo,osfiltroseasbactériasaderidas forammonitoradoscommicroscópioeletrônicodevarredura.
Resultados: Oexame dosfiltrospormicroscópicoeletrônicomostrou queaestruturado fil-troPortexeragranuladaeadofiltroRuschfibrilar.Acontagemdecolôniasdocateteredo frascomostrouqueambososfiltrospossuíamumacapacidadedeadesãobacterianasignificativa (p<0,001).Apósainfusãodasuspensãobacteriana,ascontagensdecolôniasmostraramqueo filtroPortexfoimaiseficiente(p<0.001).Nãohouvequalquerdiferenc¸aentreasadesõesde bactériasS.aureuseP.aeruginosa.Namonitorac¸ãoporMEVapósainfusão,ficoufisicamente evidentequeasbactériasforamaderidasdemodoeficazporambososfiltros.
Conclusão:Ofiltrocomestruturagranularfoiestatísticaesignificativamentemaisbem suce-didoqueofiltrocomestruturafibrilar.Emboraotamanhodosporosdosfiltrosfosseigual ----asdiferenc¸as estruturais mostradaspeloMEV eramsemelhantes ----,nãoseria justoatribuir asalterac¸õesdeeficiênciaapenasàsdiferenc¸asestruturais.Ousoaomesmotempodeprovas microbiológicasefísicasparaavaliaraeficáciafoioutroaspectoimportantedesteexperimento. ©2013SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Bacteriafilter
LocalanaesthesiawasimplementedbyJamesLeonard Corn-ingin1885forthefirsttimeinabyinjectingcocaineinto theepiduralsitesofdogs.
Due to the fact that the local analgesia/anaesthesia decreases postoperative mortality and morbidity, its administration has increased. The increased analge-sia/anaesthesia has brought up new problems. These primaryproblems are cardio toxicity, hypotension, motor block,andtranspositionofthecatheter.
Localanalgesia/anaesthesia infectionhasbeen seen at ratesof 0.5---5.4%.1,3,4It hasbeensuggested topay
atten-tiontosterilisationtopreventinfectionaswell asplacing filtersin the catheters.1---4 For thispurpose, newtypes of
catheters and filters began to be used.1 The filters were
usedfor preventingparticulatesincludingglass,etc. from
entering the epidural/spinalsite and the development of infection.Theintendedpurposeofusingfilterstodayisto preventcontaminationduringtheadministrationofbolusat theepiduralsite.
Inthe practiceofanaesthesia,therearemany contro-versialissuessuchaswhethertheadministrationshouldbe forashort-termorlong-term,careservicesofthepatients shouldbeprovidedinthehospitalsorat home,whattype of catheter is the most suitable for patients, what types ofanalgesicsorcombinationsshouldbeadministeredtothe patients,andwhatshouldbethechangeperiodofthe bacte-riafilters.Theimportanceofthebacteriafilterhasalways beenneglectedamongalltheseproblemsandhasnotbeen totallystudied.Duetothefactthatcosteffectiveanalyses inthehealthcarefieldhavegainedimportanceinthe21st century,theefficiencyandnecessityofthebacteriafilters arenowbeingdiscussed.
anaesthesia/analgesia(PCA),wereencountered.The dura-tionof stayof theepiduralcatheter,thecondition of the catheter administration space, the characteristics of the material of which the catheter wasmade, the asepsis of thepersonwhoperformerstheadministrationandhis/her following proper antisepsis procedures, his/her personal experiencesandskillshavebeenindicatedtobeimportant factorscontributingtotheriskofinfection.1,2,7,10Thereisno
markeddifferencebetweentheinfectionandcolonisation levelsaccordingtothecathetertypesadministeredtoday. Thefactorsaffectingtheriskofinfectionare7---13:
A Patientfactors
1. Ageofthepatient(>65yearsand<2years)
2. Existenceofa chronicdisease(malignancy,diabetes mellitus,chronicrenalfailure)
3. Anatomicconditionoftheadministrationarea (surger-ies,trauma history, instrumentation history, chronic degenerativedisease)
4. Existenceofanotherinfectioncentre(Haematogenous spread)
B Factorsoftheadministrators
1. Notfollowingtheproceduresofasepsis
2. Notcleaningtheadministrationareaoftheskin prop-erly
3. Traumaticadministration(haematoma) C Factorsofcatheter
1. Non-existenceofthebacteriafilter
2. Characteristicsofthebacteriafilter(Membrane sur-facespaceandthematerialofwhichitismade) There aretwobacteriafiltersaccording tothe struc-turesofthefiltermaterials;
1. Polyvinylchloride 2. Celluloseacetate
3. Durationofstayofthecatheter D Factorsoftheactivemicroorganism
1. Capacityofadhesiontothebacteriafilter(makinga biofilm)
2. Resistancetothesanitisersandantiseptics 3. Takingpartintheflora-colonisation
Purpose
Comparing the Staphylococcus aureus and Pseudomonas aureginosabacteriaadhesioncapacitiesofthetwodifferent bacteria filters Portex® (Smiths-Medical, USA) and Rusch®
(Melsungen, Germany) that are commonly used in daily practicewithaninvitrotestingapparatusand demonstrat-ingthevisualadhesionofthebacteriabythefiltersystem withscanningelectronmicroscopy.
Materials
and
methods
Bacteriologicalmethodandtestingapparatus
Theresearcherwhowasgoingtopreparethetesting appara-tusworesterilisedclothes.Therubbertopoftheemptyand sterile1000ccbottleswascleanedwithasterilisedbatticon twice.18Goftuohysyringewasplacedintothetopofthe bottle.Thecatheterwasputintothesyringeandthesyringe was removed. Catheter was located in the 9cm distance frombottle.Afilterwasattachedonthetip.Inthisstudy,
Table1 Summaryofthedifferencesbetweenthefilters.
Catheter Surface space
Pore material
Filtermaterial
Portex® 4.91cm2 Circular Polyvinylchloride Rusch® 5.0cm2 String Celluloseacetate
Portex® (Smiths-Medical, USA) which has 0.2
m of pore
aperture and Rusch® (Melsungen, Germany) flat catheter
filterswereused.The differences betweenthe filters are explainedinTable1.
Experimentgroups
GROUP1:Portexfilter10×
S.aureus0.5Mfc(105cfu/mL)-250ccnormalsaline GROUP1Control:Portexfilter10×
Nobacteria-250ccnormalsaline
GROUP2:Portexfilter10×
P.aeruginosa0.5Mfc(105cfu/mL)-250ccnormalsaline GROUP2Control:Portexfilter10×
Nobacteria-250ccnormalsaline
GROUP3:Ruschfilter10×
S.aureus0.5Mfc(105cfu/mL)-250ccnormalsaline GROUP3Control:Ruschfilter10×
Nobacteria-250ccnormalsaline
GROUP4:Ruschfilter10×
P.aeruginosa0.5Mfc(105cfu/mL)-250ccnormalsaline GROUP4Control:Ruschfilter10×
Nobacteria-250ccnormalsaline
The bacteria used in the study are clinical standard strains; Staphylococcus aureus (ATCC 25923) and Pseu-domonasaeruginosa (ATCC 27853).Bothbacterial suspen-sionswerepreparedinthesterilisedsalineserumwithoptic density of 0.5 Mc Farland (105cfu/mL) and in the 250mL
ofsalineseruminasterilisedarea.Thetipofthepumpset wasattachedtothefilter.Thesuspensionwhichwasfiltered for48hinacontinuousinfusionof5mL/hbyusingthePCA (PatientControlledAnalgesia)equipmentwasaccumulated inthesyringe.
Bacterialisolationandidentificationweredonefromthe pumping site in aerobic conditions of 37◦C after 16---24h
incubation. The number of the colony was examined to checkif therewas any decrease.After infusion, bacteria filterswerecleanedwithsterilenormalsalineandbacterial isolationandidentificationwasalsoperformedforcleaning solution.Bacterial adheration to filters andproportion of thebacteriaheldbyfilterswerecompared.
Electronmicroscopicscreening
Intheelectronmicroscopicscreening,SEM(scanning elec-tron microscope) JEOL-JSM-6060 model was used. The examplesweredried witha methodof critical-point dry-ingandtheywerecoveredbyGold-Palladiumand‘Sputter CoaterPoloran’method.Imagesweretakeninthe15---20kV rangeandphotographicenlargementsof30×,250×,500×, 1000×,2500×and5000×weretakenandsaved.
thebacteriaadheredinthefilters,SEMscreening,whichis interpretedasthegoldstandard,wasdone.
Statisticalanalysis
Afterthetwodifferentbacteriasuspensionswerefiltered, thebacteriaadhesionlevelsofthefilterswerecomparedby meansofManWhitneyU,whichisanonparametrictestby usingSPSS10.0andthevaluesunderp<0.05wereaccepted asstatisticallysignificant.
Results
The fibrillary (Rusch-Fig. 1) and granular (Portex-Fig. 2) structures of the bacteria filters were monitored by SEM beforethebacterialinfusion.Aftertheinfusionof suspen-sions,theadhesionsoftheS.aureus(Figs.3and4)andP. aeruginosa(Figs.5and6)weremonitoredvisuallybySEM.
Asaresultofthecomparisonofthecolonycountsfrom thecatheterandbottle,itwasconfirmedthatbothofthe epiduralfiltersdemonstratedbacteriaadhesioncapacityat asignificantlevel(p<0.001)(Tables2and3).
Figure 1 SEM-Rusch Flat Filter; Fibrillary structure 1000×
magnification-beforebacterialinfusion.
Figure2 SEM-Portex Flat Filter; Granular structure 5000×
magnification,beforebacterialinfusion.
Figure3 SEM-PortexFlatFilter,Staphylococcusaureus5000×
magnification,afterbacterialinfusion.
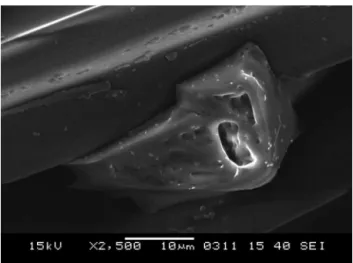
Figure4 SEM-Rusch FlatFilter,S.aureus2500× magnifica-tion,afterbacterialinfusion.
Figure 5 SEM-Rusch Flat Filter, Pseudomonas aeruginosa
Figure6 SEM-PortexFlatFilter,P.aeruginosa2500× magni-fication,afterbacterialinfusion.
When thetwodifferentcatheterfilterswerecompared with each other, there was not any significant difference (Table4).
Whenthecolonycountsfromthebottleswerecompared afterthe bacterialsuspension infusion, it wasshown that thePortex®filteradherestomuchmorebacteria(p<0.001)
anditismoreefficient.
Nodifferencewasobservedinthefilteradhesionofthe S.aureusandP.aeruginosabacteria.
Discussion
Twodifferentbacteriafilterswhich areusedwidely inthe marketwerecomparedaccording totheirefficiencyinan invitrostudy.Asimilarstudyintheliteraturewasexamined by De Cicco etal. for long-term paincontrol in epidural administrations about the efficiencyof bacteria filters as invivoandtheefficiencywasfoundtobeacceptable.2The
Table 2 Comparison of the colony counting from the
catheterandbottleafterinfusion.
X±SD Significance
Rusch-catheter 190,000.0±284,604.9894 MWU=9000
p<0.001 Rusch-bottle 22,600.0±40,958.5156
Table 3 Comparison of the colony counting from the
catheterandbottleafterinfusion.
X±SD Significance
Portex-catheter 91,000.0±28,460.4889 MWU=.500
p<0.001 Portex-bottle 1243.0±3101.7882
Table4 ComparisonofbacterialcolonycountingofPortex
andRuschfilters.
X±SD Significance
Rusch 190,000.0±284,604.9894 MWU=40.500
p>0.05 Portex 91,000.0±28,460.4889
main subject of the discussion onthis topicstarted with questioning whether there is a necessity to use bacteria filtersinshort-termepiduralcatheteradministrations.14 In
fact,thefirstinterpretationintheliteraturewasbroughtup byAbouleishandAmorteguiin1977withtheclaimswhether bacteriafiltersarenecessaryinepiduralanaesthesiawhich isespecially usedfor labour.15 In thefollowing years,the
fact that there were various numbers in the frequency ofcomplicationssuchasbacterialmeningitisandepidural abscessinlong-termepiduralcatheterisationcauseda num-berof researchersand clinicianstobe unclearabout this issue.16---21
Thisstudyisalsocrucialforhavingaroughideawhether bacteriafiltersshouldbeadministeredinshort-term(48h) labouranalgesiapracticallyandscientifically.Whenwe eval-uatedtwodifferentbacteriafiltersindependently,wefound theminvitroefficient.Bothofthefiltersadheredbacteria efficiently and sufficiently(Tables 2 and3). However, we needtoaddthatalthoughthereisnotsignificantdifference betweenthemstatistically,thenumberofcolonythatPortex filteradhereistentimesmorethanthenumberofcolony thattheRuschfilteradhere(Table4).Inthe enumeration (symbolisestheepiduralsite invivo) of coloniesthat was experimentedinthebottlesinbothtestingapparatus,the permeabilityof Portex bacteria filterwas observed tobe less(Table3).Accordingtoourstudy,theefficiencyofthe Portexfilterishigher.
The bacteria used in our study are standard clinical strainsandtheyarethemostfrequentbacteriaamongGram positiveandGramnegativebacteria;S.aureusandP. aeru-ginosawhichwecome acrossashospitalinfections.Inthe pilotstudy,itwasdeterminedthattheadhesioncapacityof thefiltersin differentconcentrations didnot change. For thisreason,the experimentalgroupin whichthebacteria usedinintense concentration(1 McFarland) wasremoved fromthestudy.
With the purposeof demonstrating the bacteria adhe-sionphysically,SEMscreeningwastakeninthestudy.Inthe screeningwhichwastakenbeforethebacteriainfusion,the bacteriafilters werefound tobe significantly differentin structures.ItwasmonitoredthatRuschfiltershadfibrillary structure(Fig.1)andPortexfiltershadamoreconcentrated granularstructure(Fig.2).Thefactthattheirphysical struc-turesweredemonstratedtobedifferentexplainsthe statis-ticallysignificantdifferenceinthebacteriologicalanalyses. Therearenootherstudiesinliteraturewherethe bacteri-ologicalanalysissupported theSEMimages.The studyhas alsobeenbeneficialwithregardtothefactthatSEMimages and visual demonstration of the bacteria adhesion by fil-tersweredemonstratedatthesametime(Figs.3---6).The factthatthebacteriaadhesionwasobservedphysicallyalso showsthesuccessofthetestingapparatus.
Themostimportantproblemweencounteredduringthe SEMscreeningwasthefactthatsomeimagescouldnotbe takenclearlysincethebacteriaweresensitivetothe>10kV electronflow.
Thattherewasnocontaminationinthesynchronised con-trolgroupofeach infusion inthetesting apparatusshows thatweworkedinsterilisedconditions.Thiswasconfirmed byarandomSEMscreening.
evaluatedthecontaminationriskinlong-termbacteriafilter usageandfoundthattheywereopentothecontamination riskathigherlevelsthanothermaterialsintheinvitrostudy heperformed.2IntheretrospectivestudiesthatLowandhis
colleaguesperformed inthe followingyears,theyshowed thattheinfectionlevelswerelowinepiduralanalgesia(for labour-short-term)inwidepatientseries.4Forthisreason,
someepiduralanalgesiacathetersetsareputonthemarket withoutbacteriafilters.Inourinvitrostudy,itwasindicated thatthebacteriainhighdensitywereadheredbythefilters. Inpractice,however,thisnumberofbacteriaatthisdensity cannotbeusedinlong-termanalgesicadministrations.This studyasamodelopensthenecessityofthebacteriafilters inshort-termepiduralcatheterisationwhencosteffective analysisprioritisedupfordiscussion.
Especiallyin the long-termepidural analgesia adminis-trationsoncancerpatients,itisamusttousethebacteria filtersduetothefactthatthedurationistoolongand pro-moterassociateddiseaseofthepatient.WallaceandDuPen whoworked in this field a lothad the same results from hisresearch.1,8 Anotherexceptionof thiscase isshort-or
long-termepiduraladministrationsthatwillbeperformedin childhood.Intheirstudy,Woodandhiscolleaguesconcluded thatabacteriafiltershouldnecessarilybeusedinall epidu-raladministrationwhichwillbeperformedonchildren.7We
evaluatedtheefficiencyof bacteriafiltersintwobacteria basiswithaninvitrotestingapparatusandcomparedtheir differences.Accordingtoourhypothesis,granularfilterwas supposedtobestatisticallyandsignificantlymoresuccessful inadhesionofdensebacteriasuspensionthantheoneswith fibriaandwecametothisconclusion.Thisexperimentisa firstmicrobiologicaland physical proofregarding the effi-ciencyofthebacteriafiltersandalsothefirststudyinthe literaturethatitwillbeused.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Wallace M,Yaksh TL. Long-term spinal analgesic delivery: a reviewofpreclinicandclinicalliterature.RegionalAnaesthPain Med.2000;25:117---57.
2.DeCiccoM,MatovicM,CastellaniGT,etal.Time-dependent efficacyofbacterialfiltersandinfectionriskinlong-term epidu-ralcatheterization.Anesthesiology.1995;82:765---71.
3.KehletH,HolteK.Effectofpostoperativeanalgesiaonsurgical outcome.BrJAnaesth.2001;87:62---7.
4.Low SHJ. Survey of epidural analgesia management in gen-eralintensivecareunitsinEngland.ActaAnaesthesiolScand. 2002;46:799---805.
7.Wood CE, Goresky GV, Klassen KA, Kuwahara B, Neil SG. Complications of continuous epidural infusions for post-operative analgesia in children. Can J Anaesth. 1994 July;41(7):613---20.
8.DuPen.Complicationsofneuraxialinfusionincancerpatients. S. Oncology (Williston Park). 1999 May;13 (5 Suppl 2): 45---51.
9.GrewalS,Hocking G,Wildsmith JA.Epidural abscesses.Br J Anaesth.2006Mar;96(3):292---302.Epub2006Jan23.
10.Kindler CH, Seeberger MD, Staender SE. Epidural abscess complicating epidural anesthesia and analgesia. An analysis of the literature. Acta Anaesthesiol Scand. 1998 Jul;42(6): 614---20.
11.HayekMS,PaigeB,GirgisG,etal.Tunneledepiduralcatheter infectionsinnoncancer pain: increased riskin patientswith neuropathicpain/complexregionalpainsyndrome.ClinJPain. 2006;22(1):82---9.
12.PeugesDA,CarrDB,HopkinsCC.Infectiouscomplications asso-ciated with temporary epidural catheters. Clin Infect Dis. 1994;19:970---2.
13.ByresK,AxelrodP,MichaelS,etal.Infectionscomplicating tun-neledintraspinalcathetersystemsusedtotreatchronicpain. ClinInfectDis.1995;21:403---8.
14.Abouleish E, Amortegui AJ. Correspondence: milipore fil-ters are not necessary for epidural block. Anesthesiology. 1981;55(5):604.
15.Abouleish E, Amortegui AJ, Taylor FH. Are bacterial filters neededincontinuousepiduralanalgesiaforobstetrics. Anes-thesiology.1977;46(5):351---4.
16.SmittPS,TsafkaA,TengVan-deZandeF,etal.Outcomeand complications of epidural analgesia in patients with cancer pain.Cancer.1998;83:2015---22.
17.Kaushal M, Narayan S, Aggarwal R, et al. In vitro use of bacterial filters for prevention of infection. Indian Pediatr. 2004;41:1133---7.
18.DupenSL,PetersonDG,WilliamsA,BogosianAJ.Infection dur-ingchronicepiduralcatheterization:diagnosisandtreatment. Anesthesiology.1990;73:905---9.
19.Phillips JM, Stedeford JC, Hartsilver E, Roberts C. Epidu-ralabscesscomplicatinginsertionofepidural catheters.BrJ Anaesth.2002;89(5):778---82.
20.SimpsonRS,MacintyrePE,ShawD,etal.Epiduralcathetertip cultures:resultsofa4-yearauditandimplicationsforclinical practice.RegAnesthPainMed.2000;25(4):360---7.