w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Original
article
Descriptive
study
of
the
prevalence
of
anemia,
hypertension,
diabetes
and
quality
of
life
in
a
randomly
selected
population
of
elderly
subjects
from
São
Paulo
Jacqueline
Lacerda
a,
Matheus
Rodrigues
Lopes
b,
Douglas
Patriota
Ferreira
a,
Fernando
Luiz
Affonso
Fonseca
a,
Patricia
Favaro
a,∗ aUniversidadeFederaldeSãoPaulo(Unifesp),Diadema,SP,BrazilbUniversidadeEstadualdeCampinas(Unicamp),Campinas,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received17February2016 Accepted19March2016 Availableonline14April2016
Keywords:
Anemia Elderly
Erythrocyteindices Personalfunctionalstatus Non-psychoticmentaldisorders
a
b
s
t
r
a
c
t
Background:Therapidincreaseintheagedpopulationhasresultedinagrowingnumberof casesofchronicdiseases.Thisincreaseisanimportantdemographicchangethatlow-and middle-incomecountrieshavetofaceandposesanewchallengetohealthservices.Oneof thefirststepstoformulatepublicpoliciesistounderstandtherealityofeachcountry’saging population.Thisstudydescribestheprevalenceofanemia,hypertensionanddiabetesand theoverallhealthstatusinpre-elderlyandelderlysubjectsenrolledintwoprimaryhealth careclinics,EldoradoandPiraporinha,inthecityofDiadema,SãoPaulo.
Method:Across-sectionalstudywasconductedwith373participants.Clinicaldatawere collectedfrompatientchartsandthedegreeofdisabilityandcommonmentaldisorders,as wellasdemographicdatawereobtainedbyinterviews.
Results:Theprevalenceofanemiawasapproximately11%andhypertensionwas70%and 81%inEldoradoandPiraporinha,respectively.Thefrequencyofdiabeteswas52%in Eldo-rado and30%in Piraporinha. The subjectsofboth health care clinicsreported having difficultiesinsomeoftheirdailyphysicalandinstrumentalactivities,withphysical symp-tomsandemotionaldisorders.
Conclusion: Anemia,hypertensionanddiabetesareprevalentinthestudiedpopulation,and patientsshoweddegreesofdependencyandimpairedhealthstatus.
©2016Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mails:[email protected],[email protected](P.Favaro). http://dx.doi.org/10.1016/j.bjhh.2016.03.005
Introduction
Increasesin theproportion ofolderpeople are auniversal phenomenon.Theforecastforthisolderpopulation(>65year old)for2100,acrossthe globe, ismorethan triple the cur-rentnumber.1Thisdemographicchangeisaconsequenceof
socioeconomicgrowthandincreasingprosperity,resultingin ahigheraveragelifeexpectancy.2However,thisagingofthe
populationhasanimpactonhealthcaresystems,inpartdue totheincreaseinthenumberofpeoplewithchronicdiseases.3
Lifeexpectancyishigherindevelopedcountrieshowever theabsolutenumberofolderadultsisconcentratedin devel-opingcountries.4Inthepast50years,Brazil,thefifthlargest
country inthe world, has experienceda demographic rev-olution. Accordingto the Braziliancensusdepartment,the InstitutoBrasileiradeGeografiaeEstatística,theaveragelife expectancyinBrazilhadreached73yearsin2009(76.5and 69 years forwomenand men, respectively).5 Nevertheless,
thecorrespondingrateofsocioeconomicgrowthand improve-mentinhealthcarehasnotkeptupwiththisrapidrateof agingoftheBrazilianpopulation.6 Thus,understandingthe
Brazilianrealityofthisagingpopulationcouldhelpimplement localhealthpoliciesandinterventionsbasedondiversities.
Theaimofthisstudywastoevaluatetheprevalenceof ane-mia,hypertensionanddiabetesandtocorrelatetheseissues withtheoverallhealthstatusinpre-elderly(50–59years)and elderlypatients(age≥60years)enrolledintwoprimarycare
clinics.
Method
Studydesign
Thisisacross-sectionalobservationalstudycarriedoutattwo primaryreferralcentersforelderlycare,Eldoradoand Pira-porinha.BothclinicsareinthecityofDiadema,whichalong withother cities, belongs to theconurbation ofSãoPaulo. TheEldoradoclinicislocatedintheoutskirtsofthecityand thePiraporinhaclinicislocatedinamoreprivilegedarea,in thecitycenter,conferringdifferentgeographiccontextstothe clinics.
Participants
Thisstudyincluded373participantswithclinicaldatabeing collected between November 2012 and April 2013. All pre-elderlyandelderlymaleandfemaleindividuals(50yearsor older)ofthetwoclinicswereinvitedtoparticipateinthestudy. Subjectswho didnotliveinDiademaandindividuals who refusedtoparticipateinthestudy wereexcluded fromthe study,aswerethosewhowereunabletoanswerthequestions duetodeafness,blindness,orwithdifficultiestounderstand. Asimplerandomsamplingmethodwasused.Inorderto cal-culatethesamplesize,theelderlypopulationofDiademawas consideredtobeapproximately4%ofthetotalpopulation,5
thus using a 95% confidence level and 5%sampling error, theminimumsamplesizerequiredwas280subjects.7Allthe
individualswhoparticipatedinthestudyprovidedinformed writtenconsent.TheEthicsCommitteeoftheUniversidade
FederaldeSão Paulo(Unifesp)approvedthestudy protocol (#142.778).
Diagnosisofanemia,hypertensionanddiabetes
Diagnosesofanemia,highbloodpressureanddiabetes mel-lituswerebasedonclinicalcharts,wheneveravailable.The diagnosesforanemiaanddiabeteswerebasedontheresults from automated hematology and biochemistry analyzers, respectively.AnemiawasdefinedaccordingtoWorldHealth Organizationcriteria8asahemoglobinlevel<13g/dLinmen
or<12g/dLinwomen.Thediagnosisofdiabeteswasdefined based onthe currentAmerican DiabetesAssociation(ADA) guidelines,which includeafastingplasma glucoselevelof
≥7.0mmol/L (126mg/dL).9 Hypertension was defined as a
consistent (three or more readings by the physician dur-ing a medical appointment) systolic blood pressure (SBP)
≥140mmHgoradiastolicbloodpressure(DBP)≥90mmHg.10
Procedure
One hundred and seven subjects agreed to complete the Brazilian OlderAmericans ResourcesAnd Services Multidi-mensionalFunctionalAssessmentQuestionnaire(BOMFAQ)7,8
andtheSelf-ReportingQuestionnaire(SRQ-20)9,10;both
inter-views were carried out in person by trained students. Demographicdataregardingthenumberofyearsof school-ingandincomewerealsoobtained.TheBOMFAQconsistsof 15questionsaboutactivitiesofdailyliving(ADL),dividedinto twosub-scales;eightphysicalADL(PADL),andseven instru-mentalADL(IADL).ThePADLincludedgettingintoandoutof bed,eating,combingthehair,walkingonflatsurfaces,having abath/shower,gettingdressed,gettingtothetoiletintimeand cuttingtoenails.TheIADLincludedclimbingstairs(oneflight), takingmedicinesontime,walkingclosetohome,shopping, preparingmeals,gettingoffbusesandcleaningthehouse.11
Thesubjects’responsestotheBOMFAQwereanalyzed accord-ingtotwocriteria:withorwithoutdifficultytocompletethe task.
Statisticalanalysis
Allstatisticaldataanalyseswereperformedusingthe Statis-ticalPackagefortheSocialSciences(SPSS,version21.0;IBM Corp.,2012).TheStudent’st-test,thechi-squaretest,andthe Pearsoncorrelationcoefficientwithalevelofsignificanceof 5%anda95%confidenceinterval(95%CI)wereusedfordata analysis.Atwo-tailedp-value<0.05wasconsidered statisti-callysignificant.
Results
Studypopulation
Table1–Clinicalcharacteristicsofsubjects.
Characteristic Eldorado Piraporinha p-Valuea
Age(years)–mean(range) 61(50–93) 62(50–101) 0.377
Pre-elderly–n(%) 40(41.7) 115(41.5) –
Elderly–n(%) 56(58.3) 162(58.5) –
Gender–n(%)
Male 36(37.5) 105(37.9) 0.943
Female 60(62.5) 172(62.1)
Peripheralbloodparameters–mean(range)
Erythrocytes(×1012L) 4.63(2.41–5.8) 4.63(3.00–6.79 0.401
Hematocrit(%) 41.3(27.2–51.1) 41.1(25.1–60.9) 0.504
Hemoglobin(g/dL) 13.9(9.2–17.8) 13.7(8.2–20.8) 0.559
Totalleukocytes(×109/L) 6.85(2.6–11.9) 6.1(0.8–16.2) 0.460
Meancorpuscularvolume 89.4(65.6–112.9) 89.4(59.6–101.4) 0.702
MCH(pg/cell) 30.1(20.3–38.2) 30.3(18.5–36.8) 0.249
MCHC(g/dL) 33.6(30.9–36.6) 33.8(13.0–39.5) 0.461
RDW(%) 13.1(10.7–27.0) 12.8(10.1–17.9) 0.151
Platelets(×109/L) 228(130–654) 234(81–454) 0.316
Fastingplasmaglucose 117.8(67–376) 106.14(43–432) 0.06
MCH:meancorpuscularhemoglobin;MCHC:meancorpuscularhemoglobinconcentration;RDW:redcelldistributionwidth. a Student’st-testwasusedforquantitativevariablesandtheChi-squaretestforcategoricalvariables.
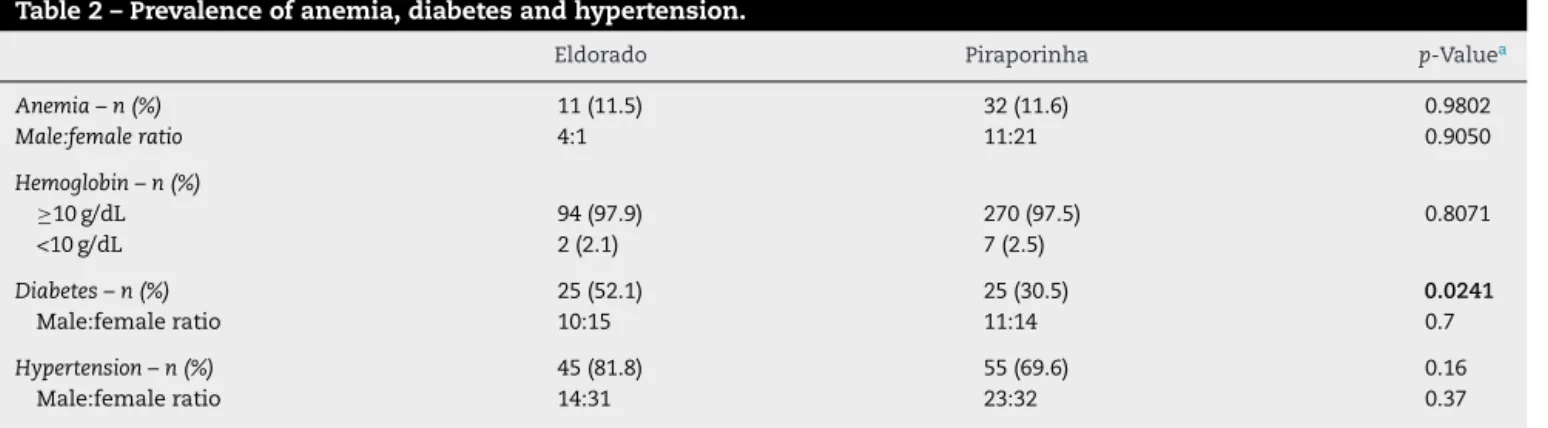
Prevalenceofanemia,diabetesandhypertension
The prevalence of anemia in the studied population was approximately11%formenandwomeninbothhealthcare clinics with hemoglobin <10g/dL being found in approxi-mately2%ofthesubjects(Table2).
Approximately 52% of the subjects had diabetes in the Eldoradohealthcareclinicwhichwasasignificantlyhigher frequencywhencomparedtoPiraporinha,wherenearly30% ofthesubjectswerediabetic(p-value=0.0241;Table2).
The frequencies of hypertension were similar in both clinics(70%inEldoradoand81%inPiraporinha)withno sta-tisticallysignificantdifferencebetweengenders(Table2).
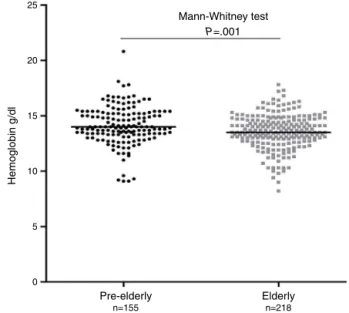
Hemoglobinvaluesandage
The Pearson correlation coefficient demonstrated that hemoglobin levels were inversely associated with age
(Figure1).Inaddition,hemoglobinvaluesweresignificantly lowerintheelderlywhencomparedwiththepre-elderlygroup (Figure2).
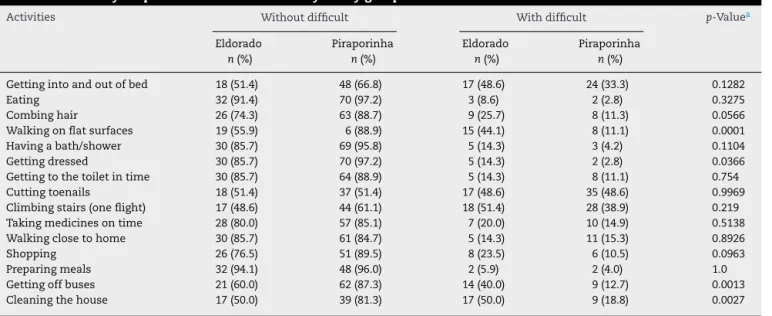
Assessmentofthedegreeofdependencyandcommon
mentaldisorders
Onehundred andsevensubjectswere assessedusingboth the BOMFAQ and the SRQ-20 instruments to evaluate the degreeofdisability andcommon mentaldisorders, respec-tively. Table 3 shows the sociodemographic data of the sample.
Whenthesubjectswereevaluatedaccordingtotheirlevel ofindependence,thesubjectsfromtheEldoradohealthcare clinicgenerallyreportedhavingmoredifficultiesintwoPADL andtwoIADL;walkingonflatsurfaces(44.1%),gettingdressed (14.2%),gettingoffbuses(40%)andcleaningthehouse(50%) (Table4).Subjectsfrom Eldoradoalsopresentedwithmore
Table2–Prevalenceofanemia,diabetesandhypertension.
Eldorado Piraporinha p-Valuea
Anemia–n(%) 11(11.5) 32(11.6) 0.9802
Male:femaleratio 4:1 11:21 0.9050
Hemoglobin–n(%)
≥10g/dL 94(97.9) 270(97.5) 0.8071
<10g/dL 2(2.1) 7(2.5)
Diabetes–n(%) 25(52.1) 25(30.5) 0.0241
Male:femaleratio 10:15 11:14 0.7
Hypertension–n(%) 45(81.8) 55(69.6) 0.16
Male:femaleratio 14:31 23:32 0.37
25
20
15
10
5
0
50 60 70 80
Age (years; n=373)
Hemoglobin (g/dL)
Pearson’s correlation P<.0001 r=–0.2551
90 100 110
Figure1–Correlationofhemoglobinvalues(g/dL)withage (years).
physicalsymptomsandemotionaldisorderswhencompared withPiraporinhasubjects(Table5).
Discussion
Thisstudy revealedthatapproximately 11%ofthesubjects of50yearsofageandolderpresentedanemiaaccordingto WHOcriteriainbothhealthcareclinics.Thelowprevalence ofanemiainourcohortcorroboratesotherstudiesthatalso assessedtheprevalenceofanemiaamongfree-livingelderly people;Guralniketal.presenteddataregardingaNorth Amer-icanpopulation,12Saliveetal.reportedontheEpidemiologic
StudyoftheElderly(EPESE)13andInelmenetal.describeddata
inarepresentativeItalianpopulation.14Inthecurrentstudy,
theanemiawasmildinthemajorityoftheanemicsubjects. In this cohort, normocyticanemia was the most common typeofanemia(between54.5%and70%),whichisconsistent withaBrazilianstudythatstudiedfree-livingelderly individ-ualsinsouthernBrazil.15Anemiaofinflammatoryresponseis
mostoftendescribedasanormocyticnormochromicanemia
25
20
15
10
5
0
n=155 Pre-elderly
Mann-Whitney test
Hemoglobin g/dl
P=.001
Elderly n=218
Figure2–Distributionofhemoglobinvalues(g/dL)in pre-elderlyandelderlygroups(horizontallinesindicate medians).
and isusuallymild.16 Theriskfactors linkedtothe
major-ity ofchronicdiseases,suchasdiabetes,havebeen shown toincreaseinflammation,17andinthisstudy,therewerehigh
frequenciesofbothdiabetesandhypertension.Despitehaving observed anegativecorrelationbetween hemoglobinlevels andage,withlowerhemoglobinvaluesintheelderlywhen comparedtothepre-elderlygroup,itisnotbelievedthatthese valuesareduetoage.Thereisabodyofevidencethatsuggests that mostcasesofanemia inolderpeopleare duetopoor healthandshouldpromptfurtherinvestigationsinthe clin-icalpractice,evenwhenthepersonhasnoapparentclinical disease.12,18
Withregardtothehighprevalenceofhypertensioninthe current cohort, the literatureshows that theprevalenceof hypertensionincreaseswithageinadults19andcanreacha
Table3–Sociodemographiccharacteristics.
Eldorado
n(%)
Piraporinha
n(%)
p-Valuea
Gender
Male 5(14.3) 23(31.9)
Female 30(85.7) 49(68.1) 0.05
Education(years)
None 4(11.4) 8(11.1) 0.3
1–3 25(71.4) 38(52.8)
4–7 2(5.7) 10(13.9)
8+ 4(11.5) 16(22.2)
Monthlyincome(R$)b
0–723 15(44.1) 21(30) 0.15
724–2172 19(55.9) 44(62.9)
2173+ 0 5(7.1)
a Chi-squaretest.
b DuringtheperiodofdatacollectiontheminimumBrazilianwagewasapproximatelyR$724.00,andUS$1.00wasapproximatelyequaltoR$
Table4–Difficultyforperform15activitiesofdailylifebygroup.
Activities Withoutdifficult Withdifficult p-Valuea
Eldorado n(%)
Piraporinha n(%)
Eldorado n(%)
Piraporinha n(%)
Gettingintoandoutofbed 18(51.4) 48(66.8) 17(48.6) 24(33.3) 0.1282
Eating 32(91.4) 70(97.2) 3(8.6) 2(2.8) 0.3275
Combinghair 26(74.3) 63(88.7) 9(25.7) 8(11.3) 0.0566
Walkingonflatsurfaces 19(55.9) 6(88.9) 15(44.1) 8(11.1) 0.0001
Havingabath/shower 30(85.7) 69(95.8) 5(14.3) 3(4.2) 0.1104
Gettingdressed 30(85.7) 70(97.2) 5(14.3) 2(2.8) 0.0366
Gettingtothetoiletintime 30(85.7) 64(88.9) 5(14.3) 8(11.1) 0.754
Cuttingtoenails 18(51.4) 37(51.4) 17(48.6) 35(48.6) 0.9969
Climbingstairs(oneflight) 17(48.6) 44(61.1) 18(51.4) 28(38.9) 0.219
Takingmedicinesontime 28(80.0) 57(85.1) 7(20.0) 10(14.9) 0.5138
Walkingclosetohome 30(85.7) 61(84.7) 5(14.3) 11(15.3) 0.8926
Shopping 26(76.5) 51(89.5) 8(23.5) 6(10.5) 0.0963
Preparingmeals 32(94.1) 48(96.0) 2(5.9) 2(4.0) 1.0
Gettingoffbuses 21(60.0) 62(87.3) 14(40.0) 9(12.7) 0.0013
Cleaningthehouse 17(50.0) 39(81.3) 17(50.0) 9(18.8) 0.0027
a Chi-squaretest.Statisticallysignificancewasdefinedasp-values<0.05.
prevalenceashighas80%.20–23Itisimportanttopointoutthat
hypertensionisindependentlyassociatedwithcardiovascular diseasesintheelderly.
Thisstudyfocusedonadescriptionofthe prevalenceof diseasesrelatedtoelderlyindividualsandtheirqualityoflife. Althoughtherewerenosocialanddemographicdifferences, thestudywasperformedintwocontrastingareasofDiadema. WhilethePiraporinhaclinicislocatedinamoreprivileged area,inthecity center,theEldoradoclinicislocatedinthe pooreroutskirts.Thesubjectsthatliveintheoutskirtshad
significantlylower scoresfortwo PADLandtwo IADLthan thesubjectswholivedinthecitycenter.Subjectsfrom Eldo-radoalsopresentedasignificantlyhigherprevalenceofminor psychiatricdisorders,when comparedtothesubjectsfrom Piraporinha.Moreover,theprevalenceofdiabeteswasmuch higherintheEldoradohealthcareclinic.Theliteratureshows thattheincidenceofdepressionandimpairedcognitive func-tionincreasesinelderlyindividualswithdiabetes.24Moreover,
depressioninelderlypatientswithdiabetesisastrong predic-torofhospitalizationanddeath25;anxietyandstressinthe
Table5–ResultsoftheSRQ-20questionnairebygroup.
Yes No p-Valuea
Eldorado n(%)
Piraporinha n(%)
Eldorado n(%)
Piraporinha n(%)
1.Headaches 12(34.3) 9(12.5) 23(65.7) 63(87.5) 0.0078
2.Poorappetite 14(40.0) 13(18.1) 21(60.0) 59(81.9) 0.0142
3.Sleepingbadly 15(42.9) 29(40.3) 20(57.1) 43(59.7) 0.7992
4.Easilyfrightened 17(48.6) 18(25.0) 18(51.4) 54(75.0) 0.0148
5.Handsshake 9(25.7) 9(12.5) 26(74.3) 63(87.5) 0.0865
6.Feelingnervous,tenseorworried 26(74.3) 41(56.9) 9(25.7) 31(43.1) 0.082
7.Poordigestion 12(34.3) 17(23.6) 23(65.1) 55(76.4) 0.2438
8.Troublethinkingclearly 15(42.9) 8(11.1) 23(57.14) 64(88.9) 0.0002
9.Feelingunhappy 24(68.6) 32(44.4) 11(31.4) 40(55.6) 0.0191
10.Cryingmorethanusual 12(32.3) 19(26.4) 23(65.7) 53(73.6) 0.3982
11.Difficultyinenjoyingdailyactivities 14(40.0) 21(29.17) 21(60.0) 51(70.8) 0.2625
12.Difficultyinmakingdecisions 14(40.0) 21(38.9) 21(60.0) 51(70.8) 0.9121
13.Dailysufferingatwork 11(31.4) 15(20.8) 24(68.6) 57(79.2) 0.2306
14.Unabletoplayausefulroleinlife 14(40.0) 14(19.4) 21(60.0) 58(80.6) 0.0232
15.Lostinterestinthings 20(57.1) 26(36.1) 15(42.9) 46(63.9) 0.0392
16.Feelingthatyouareaworthlessperson 8(22.9) 6(8.3) 27(77.1) 66(91.7) 0.063 17.Thoughtsofendingyourlifehavebeenon
yourmind
6(17.1) 6(8.3) 27(77.1) 66(91.7) 0.2008
18.Feelingtiredallthetime 14(41.2) 16(22.2) 20(58.8) 56(77.8) 0.0432
19.Uncomfortablefeelingsinyourstomach 15(42.9) 23(30.6) 20(57.1) 50(69.4) 0.2094
20.Easilytired 17(48.6) 23(31.9) 18(51.4) 49(68.1) 0.0954
elderlyareimportanthealthissuesfrequentlyassociatedwith poorerphysicalandemotionalwell-being.26
Conclusion
Regardless of the location of the health care clinic, there areprevalencesofanemia,hypertensionanddiabetesinthe populationsofpre-elderlyandelderlyindividuals.Boththese groups showed degrees ofdependency and impairment of healthstatus.Ourfindingsmightaidpublichealthcare man-agersinthetargetingofstrategiestopromotebetterhealthin theagingpopulation.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
FundingforthisworkwasprovidedbyConselhoNacionalde DesenvolvimentoCientíficoeTecnológico(CNPq).Theauthors would like to thank Raquel Susana Foglio for the English review.
r
e
f
e
r
e
n
c
e
s
1. WorldPopulationProspects[WPP].The2010revision, highlightsandadvancetables.NewYork:Departmentof EconomicandSocialAffairsPD;2011.
2. TonelliM,RiellaMC.WorldKidneyDay2014:CKDandthe agingpopulation.AmJKidneyDis.2014;63(3):349–53. 3. MathersC,LoncarD.Updatedprojectionsofglobalmortality
andburdenofdisease,2002–2030:datasources,methodsand results.OrganizationWH;2006.
4. HoltzC.Globalhealthcare:issuesandpolicies.Sudbury,MA: Jones&Bartlett;2008.
5. Searchnationalhouseholdsample;2010.Availablefrom: http://www.ibge.gov.br/censo2010/primeirosdados divulgados/index.php[cited2014].
6. PalloniA,PeláezM.Historyandnatureofthestudy.In:Lebrão ML,DuarteYA,editors.KNOW–healthwellnessandaging: theSABEprojectinthemunicipalityofSãoPaulo–aninitial approach.Brasília:PanAmericanHealth;2003.p.15–32. 7. LaboratóriodeEpidemiologiaeEstatística–LEE.Available
from:http://www.lee.dante.br/pesquisa.html;2000[cited 17.02.16].
8. Nutritionalanaemias.ReportofaWHOscientificgroup. WorldHealthOrganTechRepSer.1968;405:5–37.
9. AmericanDiabetesAssociation.Standardsofmedicalcarein diabetes–2010.DiabetesCare.2010;33Suppl.1:S11–61. 10.ChobanianAV,BakrisGL,BlackHR,CushmanWC,GreenLA,
IzzoJLJr,etal.TheSeventhReportoftheJointNational
CommitteeonPrevention,Detection,Evaluation,and TreatmentofHighBloodPressure:theJNC7report.JAMA. 2003;289(19):2560–72.
11.FriedLP,FerrucciL,DarerJ,WilliamsonJD,AndersonG. Untanglingtheconceptsofdisability,frailty,andcomorbidity: implicationsforimprovedtargetingandcare.JGerontolA: BiolSciMedSci.2004;59(3):255–63.
12.GuralnikJM,EisenstaedtRS,FerrucciL,KleinHG,Woodman RC.Prevalenceofanemiainpersons65yearsandolderinthe UnitedStates:evidenceforahighrateofunexplained anemia.Blood.2004;104(8):2263–8.
13.SaliveME,Cornoni-HuntleyJ,GuralnikJM,PhillipsCL, WallaceRB,OstfeldAM,etal.Anemiaandhemoglobinlevels inolderpersons:relationshipwithage,gender,andhealth status.JAmGeriatrSoc.1992;40(5):489–96.
14.InelmenEM,D’AlessioM,GattoMR,BaggioMB,JimenezG, BizzottoMG,etal.Descriptiveanalysisoftheprevalenceof anemiainarandomlyselectedsampleofelderlypeople livingathome:someresultsofanItalianmulticentricstudy. Aging(Milano).1994;6(2):81–9.
15.SgnaolinV,EngroffP,ElyLS,SchneiderRH,SchwankeCH, GomesI,etal.Hematologicalparametersandprevalenceof anemiaamongfree-livingelderlyinsouthBrazil.RevBras HematolHemoter.2013;35(2):115–8.
16.RoyCN.Anemiaofinflammation.HematolAmSocHematol EducProgram.2010;2010:276–80.
17.PrasadS,SungB,AggarwalBB.Age-associatedchronic diseasesrequireage-oldmedicine:roleofchronic inflammation.PrevMed.2012;54Suppl.:S29–37.
18.IzaksGJ,WestendorpRG,KnookDL.Thedefinitionofanemia inolderpersons.JAMA.1999;281(18):1714–7.
19.RodriguezBL,LabartheDR,HuangB,Lopez-GomezJ.Riseof bloodpressurewithage.Newevidenceofpopulation differences.Hypertension.1994;24(6):779–85.
20.AronowWS,FlegJL,PepineCJ,ArtinianNT,BakrisG,Brown AS,etal.ACCF/AHA2011expertconsensusdocumenton hypertensionintheelderly:areportoftheAmericanCollege ofCardiologyFoundationTaskForceonClinicalExpert ConsensusDocuments.Circulation.2011;123(21):2434–506. 21.BurtVL,WheltonP,RoccellaEJ,BrownC,CutlerJA,HigginsM,
etal.PrevalenceofhypertensionintheUSadultpopulation. ResultsfromtheThirdNationalHealthandNutrition ExaminationSurvey,1988–1991.Hypertension. 1995;25(3):305–13.
22.OstchegaY,DillonCF,HughesJP,CarrollM,YoonS.Trendsin hypertensionprevalence,awareness,treatment,andcontrol inolderU.S.adults:datafromtheNationalHealthand NutritionExaminationSurvey1988to2004.JAmGeriatrSoc. 2007;55(7):1056–65.
23.EganBM,ZhaoY,AxonRN.UStrendsinprevalence, awareness,treatment,andcontrolofhypertension, 1988–2008.JAMA.2010;303(20):2043–50.
24.MeneillyGS,TessierD.Diabetesinelderlyadults.JGerontol A:BiolSciMedSci.2001;56(1):M5–13.
25.RosenthalMJ,FajardoM,GilmoreS,MorleyJE,NaliboffBD. Hospitalizationandmortalityofdiabetesinolderadults.A 3-yearprospectivestudy.DiabetesCare.1998;21(2):231–5. 26.BlazerDG.Depressioninlatelife:reviewandcommentary.J